
Abstract
Objective:
The renin–angiotensin system gene has been implicated in the progression of colorectal cancer. Nevertheless, the details of that role remain controversial. We performed a meta-analysis to investigate the correlation between renin–angiotensin system gene polymorphisms and colorectal cancer.
Methods:
We retrieved relevant studies from PubMed and Embase. Subsequently, fixed or random-effects models were used to calculate pooled odds ratios (ORs) with 95% confidence intervals (CIs).
Results:
We identified six studies of the angiotensin-converting enzyme insertion/deletion (I/D) polymorphism, and two studies of the angiotensinogen M235T polymorphism. The angiotensin-converting enzyme I/D polymorphism did not significantly correlate with colorectal cancer risk in the total population (DD vs. II: OR 0.77, 95% CI 0.39–1.50; DI vs. II: OR 1.05, 95% CI 0.85–1.30; dominant model: OR 0.94, 95% CI 0.68–1.31; recessive model: OR 1.01, 95% CI 0.80–1.27). Similarly, the angiotensinogen M235T polymorphism was not associated with colorectal cancer risk (TT vs. MM: OR 1.38, 95% CI 0.52–3.67; TM vs. MM: OR 1.19, 95% CI 0.96–1.47; dominant model: OR 1.28, 95% CI 0.77–2.14; recessive model: OR 1.17, 95% CI 0.53–2.59).
Conclusion:
Our findings suggest that the angiotensin-converting enzyme I/D and angiotensinogen M235T polymorphisms are unlikely to correlate with colorectal cancer.
Introduction
Colorectal cancer (CRC) is the third most common malignancy worldwide, and is also among the five most common fatal malignancies. 1 Generally, CRC is not diagnosed until the advanced stages, thereby causing high morbidity and mortality rates. Smoking, excessive alcohol intake and high consumption of red meat have been identified as potential risk factors for CRC; nevertheless, the exact causes of CRC remain unclear.2,3 The fact that a significant portion of CRC patients is not exposed to any of these carcinogenic factors suggests that genetic susceptibility might also be involved in the pathogenesis. 4
The renin–angiotensin system (RAS), a hormonal signalling pathway, modulates cardiovascular homeostasis as well as blood pressure. 5 Briefly, renin releases 10 amino acids from angiotensinogen (AGT) to form Ang I and a large protein (des (Ang I) AGT). AGT and des (Ang I) AGT are thought to be non-inhibitory serpins that suppress angiogenesis. 6 Subsequently, two amino acids are removed from Ang I by ACE to generate Ang II. Ang II is the main active peptide of RAS, and could trigger angiogenesis as well as cell proliferation by way of the angiotensin II type 1 receptor (AGTR1). 7
We searched for electronic databases, and only two polymorphisms accord with the standards. The ACE gene, located on human chromosome 17q23, is composed of 26 exons and 25 introns. An insertion/deletion (I/D) polymorphism is commonly found in the ACE gene, characterised by the presence or absence of a 287 bp Alu repetitive sequence in intron 16. 8 In terms of ACE plasma levels, homozygotes for the D allele have the highest, followed by ID heterozygotes and homozygotes for the I allele. 9 The AGT gene, located on lq42-43, is composed of five exons. There is an association between the AGT gene M235T polymorphism and increased levels of AGT. To be specific, plasma AGT levels in individuals with 235TT homozygotes are 10% and 20% higher, respectively, than those with 235MM. 10
Previous studies have suggested that ACE I/D and AGT M235T polymorphisms are related to CRC risk by affecting RAS functions. Meta-analysis could not only overcome the problem of small size and inadequate statistical power of genetic studies of complex traits, but may suggest more reliable outcomes than can single case–control studies. 11 We conducted a meta-analysis of all eligible published case–control studies and evaluated the effect of two polymorphisms on CRC risk.
Materials and methods
Search strategy for identification of studies
This systematic review and meta-analysis were conducted according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines. We searched two electronic databases (MEDLINE, Google Scholar, CNKI and EMBASE) for all relevant studies with the following terms: ‘angiotensinogen/AGT’, ‘angiotensin-converting enzyme/ACE,’ ‘colorectal cancer/CRC’, ‘genetic polymorphism’ and ‘single nucleotide polymorphism’, restricted to articles written in English. We further manually searched studies according to the references of the original article. In cases of overlapping information, the publication with the most comprehensive data was chosen.
Inclusion criteria
The inclusion criteria were as follows: (a) assessment of RAS gene polymorphisms and CRC risk; (b) case–control studies; and (c) available genotype data. Exclusion criteria were as follows: (a) studies not concerning cancer; (b) reviews; (c) studies without accessible information; and (d) repeated research.
Data extraction
All relevant articles were reviewed and data were extracted by two independent investigators. A third investigator assessed controversial studies. A series of data was extracted from every paper, as follows: name of first author, region, number of cases and controls, year of publication, genotype frequencies in cases as well as controls, and evidence of Hardy–Weinberg equilibrium (HWE) in controls.
Quality assessment
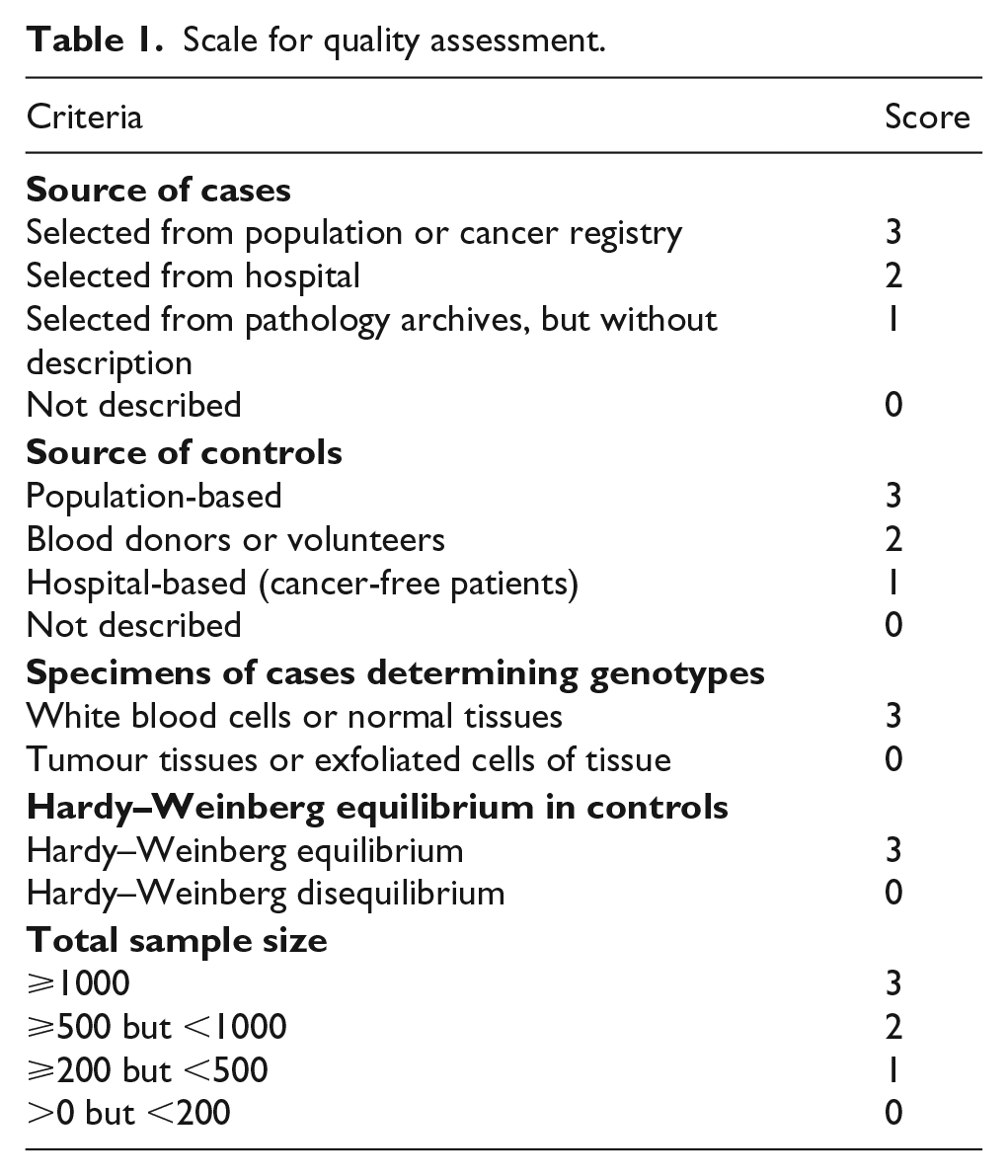
As shown in Table 1, we used quality assessments. 12 Briefly, the criteria included source of controls, representativeness of cases, CRC diagnosis, quality assessment of genotyping approaches, sample size as well as HWE, with a total score ranging from 0 to 15. Articles with scores less than 10 were considered ‘low quality’ and those with scores of 10 or greater were considered ‘high quality’.
Scale for quality assessment.
Statistical methods
Meta-analysis was performed using the meta-package of R 3.33 software. ORs with corresponding 95% CIs were employed to evaluate correlations of ACE I/D and AGT M235T polymorphisms with CRC risk using various comparisons, including homozygote (AA vs. aa), heterozygote (AA vs. Aa), dominant and recessive models between groups. The definition of the dominant model was Aa+aa versus AA, where ‘A’ and ‘a’ indicated major and minor alleles, respectively. The recessive model was defined as aa versus AA+Aa. We used the χ2 test to determine HWE for genotype distribution in the studies. The I2 statistic was used to analyse heterogeneity, with I2 greater than 50% suggesting heterogeneity. In the case of heterogeneity, a random effects model was used to calculate the pooled OR, otherwise the fixed effects model was employed. Result stability was determined using one-way sensitivity analysis. Every individual study was sequentially omitted to identify the effects of this specific study on the pooled OR. The diversity among the studies was examined using subgroup analyses stratified by race, sample size and quality assessment. Finally, funnel plots using Begg’s test and Egger’s tests were inspected to test for publication bias.
Results
Characteristics of studies
In total, 3760 relevant articles were retrieved. Finally, eight studies with complete text were enrolled in this meta-analysis in accordance with the inclusion and exclusion criteria.13–20 These enrolled studies were published between 2007 and 2017. The diagram of the selection process is shown in Figure 1. Briefly, these eight articles were written in English, with HWE tests performed on genotype distribution of the controls. None of the studies deviated from HWE except for Marques et al. 18 The quality score of every study was over 10 points except for Marques et al., 18 suggesting high quality. The features as well as methodological quality of the studies are summarised in Tables 2 and 4.

The flow diagram of included/excluded studies.
Characteristics of the included studies of ACE I/D polymorphism.

ACE: angiotensin-converting enzyme; I/D: insertion/deletion; HWE: Hardy–Weinberg equilibrium.
Meta-analysis
The major findings of ACE I/D polymorphism and CRC risk are displayed in Table 3. No significant correlation was found between the ACE I/D polymorphism and CRC risk if all eligible studies were pooled into one dataset (DD vs. II: OR 0.77, 95% CI 0.39–1.50; DI vs. II: OR 1.05, 95% CI 0.85–1.30; dominant model: OR 0.94, 95% CI 0.68–1.31; recessive model: OR 1.01, 95% CI 0.80–1.27). In subgroup analysis stratified by ethnicity, the ACE I/D polymorphism was not significantly correlated with CRC risk in either Asian or Caucasian populations (Figure 2). In subgroup analysis stratified by sample size, there was no significant relationship between sample size greater than 300 and sample size of 300 or less. Similarly, in subgroup analysis stratified by quality assessment, there was an insignificant relationship in high quality studies.
Summary ORs and 95% CI of ACE I/D polymorphism with cancer risk.

Number of comparisons.
OR: odds ratio; CI: confidence interval; ACE: angiotensin-converting enzyme; I/D: insertion/deletion; HWE: Hardy–Weinberg equilibrium.

Forest plot for meta-analysis of the association between the angiotensin-converting enzyme (ACE) insertion/deletion (I/D) polymorphism and colorectal cancer (CRC) risk in subgroup analysis under DD versus II.
The AGT M235T polymorphism did not significantly correlate with CRC risk in any genetic model (Figure 3 and Table 5, TT vs. MM: OR 1.38, 95% CI 0.52–3.67; TM vs. MM: OR 1.19, 95% CI 0.96–1.47; dominant model: OR 1.28, 95% CI 0.77–2.14; recessive model: OR 1.17, 95% CI 0.53–2.59).
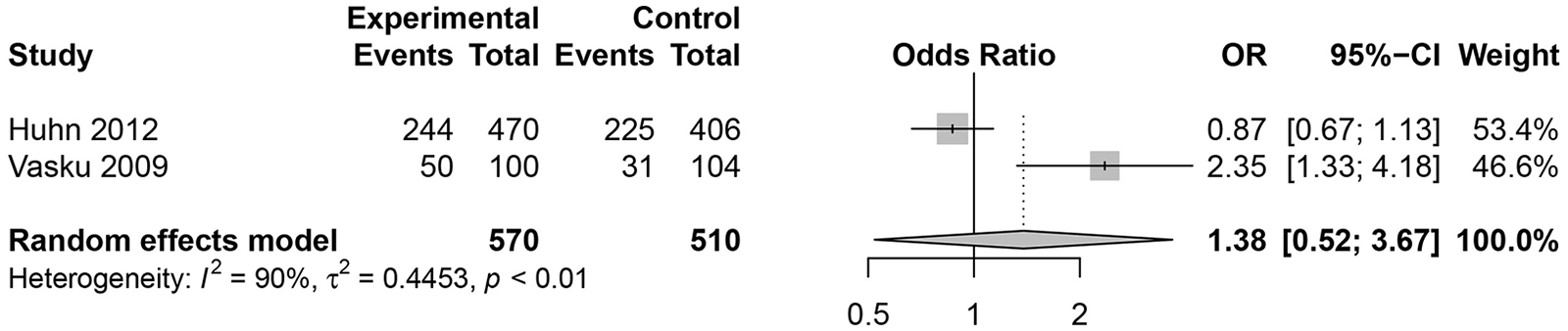
Forest plot for meta-analysis of the association between the angiotensinogen (AGT) M235T polymorphism and colorectal cancer (CRC) risk under TT versus MM.
Characteristics of the included studies of AGT M235T polymorphism.

AGT: angiotensinogen; HWE: Hardy–Weinberg equilibrium.
Summary ORs and 95% CI of AGT M235T polymorphism with cancer risk.

Number of comparisons.
OR: odds ratio; CI: confidence interval; AGT: angiotensinogen.
Publication bias
Sensitivity analysis was conducted to evaluate the stability of the results by deleting a single study at a time. No individual study significantly affected the pooled ORs. Begg’s and Egger’s funnel plots were generated to assess potential publication bias. The funnel plots were symmetrical, suggesting an absence of publication bias.
Discussion
CRC is the leading cause of cancer-related mortality in western countries, the incidence rate of which is also increasing in Asia. 21 Several lines of evidence suggest that CRC is caused by the complicated interplay between environmental and genetic factors. Despite the possible correlation of the RAS gene (ACE I/D as well as AGT M235T polymorphisms) with CRC, the specific association remains controversial. Many of these studies involve relatively small sample sizes, limiting the robustness of the results. To understand better the relationship of ACE I/D and AGT M235T polymorphisms to CRC risk, we conducted the present meta-analysis.
The correlation of RAS gene polymorphisms with CRC risk was quantitatively evaluated. We found no correlation between the ACE I/D polymorphism and CRC risk. In consideration of the possible effects of confounding factors, subgroup analysis was performed. Nevertheless, subgroup analysis stratified by ethnicity, sample size and quality assessment failed to reveal any correlation of this polymorphism with CRC susceptibility. The AGT M235T polymorphism was also not related to CRC risk in the general population. The robustness of these outcomes was further validated using sensitivity analysis and publication bias.
There are certain limitations in this meta-analysis. First, the number of studies and samples was relatively small. Second, this meta-analysis was performed according to unadjusted estimates. Therefore, to obtain an adjusted estimate, a more accurate analysis should be performed with accessible detailed individualised information. Third, there may be publication bias, because only published studies were included. Finally, the impacts of gene–gene and gene–environment interactions were not investigated.
In summary, we found that ACE I/D and AGT M235T polymorphisms might be not related to CRC risk. Because of the inaccessible relevant studies as well as limited evidence, large-scale studies with adequate methodological quality are urgently warranted.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.