
Abstract
Objective:
The effect of dual renin–angiotensin system (RAS) inhibition in heart failure (HF) is still controversial. Systematic reviews have shown that dual RAS blockade may reduce mortality and hospitalizations, yet it has been associated with the increased risk of renal dysfunction (RD). Surprisingly, although RD in patients with HF is frequent, the effect of combining RAS inhibitors in HF patients with RD has never been studied in a meta-analysis.
Methods:
A systematic review and meta-analysis of randomized clinical trials involving HF patients with RD who received dual blockade analyzing death, cardiovascular (CV) death or HF hospitalization, and adverse events.
Results:
Out of 2258 screened articles, 12 studies were included (34,131 patients). Compared with monotherapy, dual RAS inhibition reduced hazard ratio of death to 0.94 (p=0.07) and significantly reduced CV death or HF hospitalization to 0.89 (p=0.0006) in all individuals, and to 0.86 (p=0.005) in patients with RD and to 0.91 (p=0.04) without RD. Nevertheless, dual RAS blockade significantly increased the risk of renal impairment (40%), hyperkalemia (44%), and hypotension (42%), although discontinuation of treatment occurs only in 3.68% versus 2.19% (p=0.00001).
Conclusions:
Dual RAS inhibition therapy reduces the risk of CV death or HF hospitalization. However, cautions monitoring for specific adverse events may be warranted.
Introduction
Heart failure (HF) is a public health burden affecting about 23 million people worldwide. 1 Among adults, prevalence and incidence rates for HF are, respectively, 1–2% and 5–10% per 1000 persons per year.2,3 In the USA and Europe, HF is a concerning cause of morbid-mortality and, despite the fact that evidence-based treatment improves survival of patients with HF, death and hospitalization rates remain high.4,5 HF is also commonly associated with other comorbidities such as chronic kidney disease (CKD),6-8 with the prevalence of CKD in patients with HF ranging from 32% to 51%.7,9,10 In addition, the presence of CKD is a predictor of poor prognosis in HF, and the risk of mortality is inversely proportional to estimated glomerular filtration rate (eGFR). 11
Blockade of the renin–angiotensin system (RAS) with angiotensin-converting enzyme inhibitors (ACEIs), angiotensin II receptor blockers (ARBs) or aliskiren have been widely used to treat HF for over 20 years, decreasing rates of cardiovascular death and HF hospitalization by 26%.12,13 Nonetheless, it is interesting to note that because of the presence of alternative RAS pathways, the blockade of the RAS is not absolute when using a single drug. 14 To overcome this problem, several studies have investigated whether the combination of RAS inhibitors can improve HF outcomes.11,15-18
To date, only two systematic reviews have examined the effect of dual versus single-drug RAS inhibition on morbidity and mortality in patients with HF.19,20 Analyzing eight studies that included 18,061 patients, Kuenzli et al. 20 concluded that dual drug therapy with ACEIs and ARBs reduces HF hospitalizations. In another meta-analysis, dual RAS blockade in HF patients reduces HF hospitalizations although it did not improve all-cause or cardiovascular mortality. 19
Both of these reviews concluded that dual therapy was associated with hyperkalemia, hypotension, and renal impairment, suggesting that their benefits do not overcome their risks. Notwithstanding, this conclusion has been criticized since they do not recognize that HF hospitalization is a clinically relevant outcome, and its decrease represents an improvement of the quality of life. Moreover, efficacy and safety parameters were examined in heterogeneous studies that included patients with normal renal function and others with renal failure in hemodialysis. 21
In order to address the role of dual RAS blockade on HF patients with and without kidney disease, we carried out for the first time a systematic review and meta-analysis that evaluate the effect of dual drug therapy (ARBs and ACEIs, or aliskiren and ACEIs/ARBs) on the risk of all-cause death, CV death or HF hospitalization, and other adverse events in HF patients with and without renal dysfunction (RD).
Methods
This systematic review adhered to the Cochrane Collaboration methodology 22 and was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Checklist. 23 We registered this study on PROSPERO (registration number, CRD42015029351).
Information sources and search strategy
A specific search was developed for each of the following bibliographic databases using terms such as medical subject headings and keywords, as described in Supplementary Table S1; the Cochrane Library CENTRAL, Embase, LILACS, PubMed and Web of Science. The selection was supplemented with the inclusion of two clinical trial registry databases, ICTRP (WHO International Clinical Trials Registry Platform) and NCT (number of clinical trials, deposit in the clinicaltrials.gov site); and two databases of gray literature, Google Scholar and Open Grey, as well as handsearching through the reference lists of identified articles which were included in the first phase. The search encompassed articles published until 4 January 2018.
Study selection
We included randomized clinical trials that investigated dual RAS blockade in HF and analyzed a subgroup of patients with RD, which was defined as eGFR <60 ml/min/1.73m2. The studies should contain at least one outcome measurement for inclusion. Article selection was then carried out in two stages by two independent reviewers. The studies that did not meet the inclusion criteria were excluded with appropriate justification (Figure 1). In the absence of a consensus between the two authors, a third reviewer (FARN) acted as a mediator to reach a final decision.

Flow diagram of literature search and selection criteria adapted from PRISMA.
Risk of bias and data collection
The Cochrane Collaboration’s tool for assessing risk of bias in randomized studies was applied. Information regarding the protocols of previously published studies was accessed to evaluate the risk of bias. In the absence of any data, we attempted to contact authors responsible for these studies, and one of them provided numerical data. All data collected were checked by the second author (AGM) and reviewed by the third reviewer (FARN).
Summary measures
All analyses were performed using the RevMan 5.3 software. 22 For time-to-event outcomes (death, CV death, and HF hospitalization), log hazard ratios (HRs) and standard errors were calculated using the generic inverse variance method with a fixed-effect model. Analyses of the relative risk (RR) of adverse event outcomes were conducted using the Cochran–Mantel–Haenszel method with a random-effect model since we pooled different adverse events in the same graphic analysis. Statistical significance was defined as p<0.05 and results were reported with 95% confidence intervals (CIs).
Results
Study selection and study characteristics
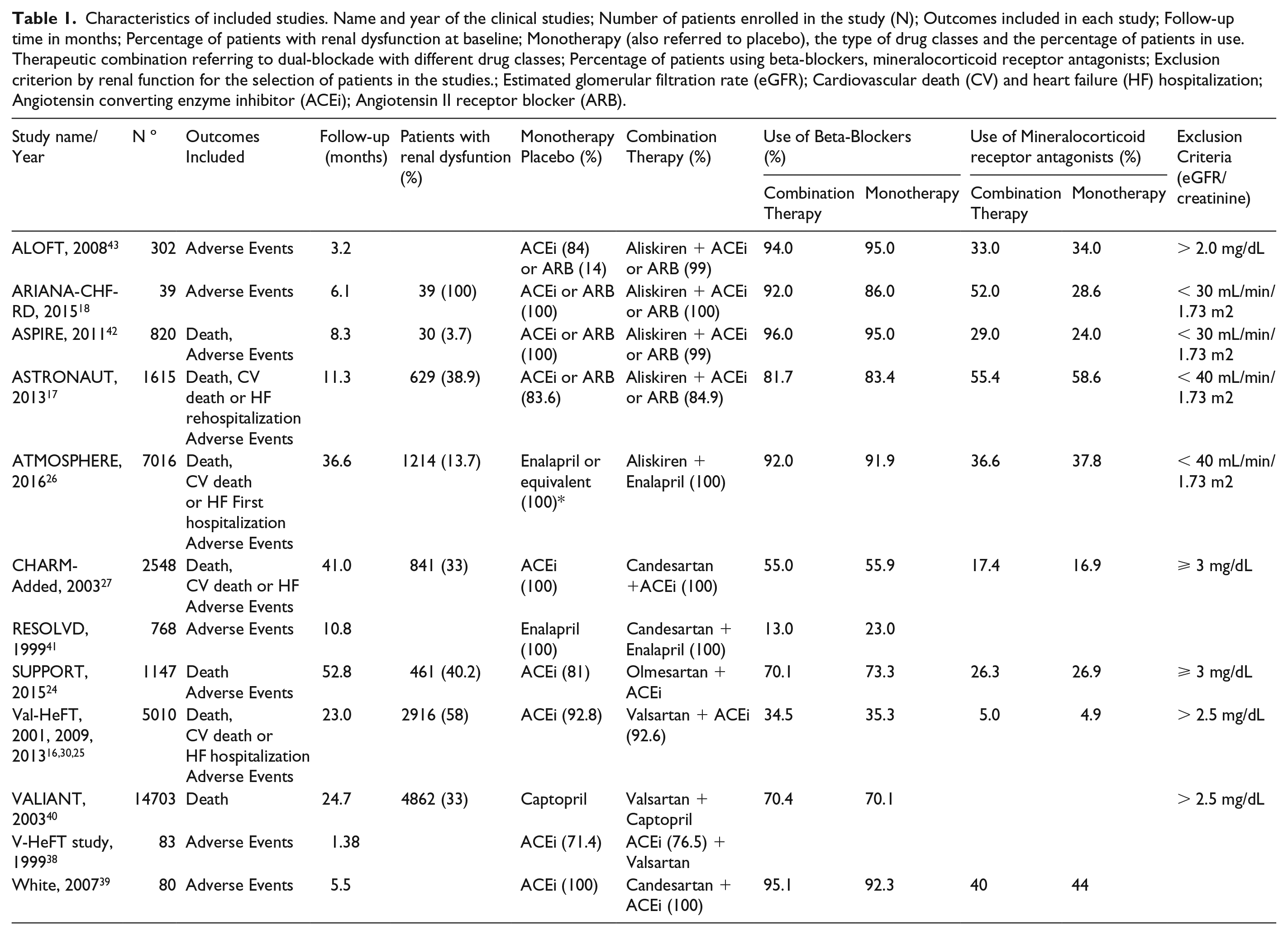
We identified 2258 articles in the searched databases (Figure 1). Articles that did not meet the selection criteria were excluded (Supplementary Table S2). We included 14 articles from 12 studies (Table 1). All of them were included in our review and also selected for quantitative analysis. Almost all studies were randomized double-blind clinical trials, except for the SUPPORT trial, which was randomized open-label blinded endpoint. 24
Characteristics of included studies. Name and year of the clinical studies; Number of patients enrolled in the study (N); Outcomes included in each study; Follow-up time in months; Percentage of patients with renal dysfunction at baseline; Monotherapy (also referred to placebo), the type of drug classes and the percentage of patients in use. Therapeutic combination referring to dual-blockade with different drug classes; Percentage of patients using beta-blockers, mineralocorticoid receptor antagonists; Exclusion criterion by renal function for the selection of patients in the studies.; Estimated glomerular filtration rate (eGFR); Cardiovascular death (CV) and heart failure (HF) hospitalization; Angiotensin converting enzyme inhibitor (ACEi); Angiotensin II receptor blocker (ARB).
We first performed a meta-analysis of patients with HF independently of the renal functions on death, CV death or HF hospitalization and adverse events such as renal impairment, hyperkalemia, and hypotension, besides the discontinuation of the therapy. Some studies did not have group data comparing outcomes between patients with and without RD.
Risk of bias
A graph and summary of study quality are presented in supplementary Figure S1. To evaluate the quality of evidence and strength of recommendations, we used the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) (Supplementary Table S3). Our result suggests that the vast majority of the studies were graded as having a low risk of bias.
Death
Initially, we performed a meta-analysis examining rates of death among the overall HF population. We observed that, in comparison with monotherapy, combined RAS inhibition had a trend toward a lower death rate, though this difference was not significant (p=0.07; Figure 2(a)). Subsequently, we compared death rates between patients with RD (eGFR <60 ml/min/1.73m2) and without RD (eGFR ⩾60 ml/min/1.73m2) in only the Val-HeFT 25 and ATMOSPHERE 26 studies. This analysis did not reveal a significant difference in death rates between patients with and without RD, and the total effect was not significant (HR, 0.94; 95% CI, 0.86–1.02; p=0.16; Figure 2(b)).

(a) Meta-analysis of death with the total shows HR 0.94 (0.89, 1.00–1.01), the heterogeneity test: Chi2=5.83, df=6 (p=0.44); I2=0%; Test for overall treatment effect: Z=1.82 (p=0.07). (b) Meta-analysis of death with the subgroups according to the estimated glomerular filtration rate (eGFR).The total shows the HR 0.94 (0.86–1.02), the heterogeneity test: Chi2=1.24, df=3 (p=0.74); I2=0%; Test for overall treatment effect: Z=1.41 (p=0.16); Test for difference between subgroups: Chi2=1.07, df=1 (p=0.30); I2=6.9%.
CV death and hospitalization due to HF
The studies ASTRONAUT, 17 ATMOSPHERE, 26 CHARM-Added, 27 and Val-HeFT 25 reported the results for the outcome of CV death or HF hospitalization. However, only ASTRONAUT, 17 ATMOSPHERE, 26 and Val-HeFT 25 stratify patients by eGFR.
Our meta-analysis demonstrated that, when compared with monotherapy, dual blockade reduced the risk of CV death or HF hospitalization by 12% (p<0.0001) (Figure 3(a)). Interestingly, the benefit of a dual blockade was similar between patients with and without RD (11%; p=0.0006). Specifically, the risk of CV death or HF hospitalization in patients with and without RD was decreased by 14% and 9%, respectively (test for subgroup differences, p=0.44). Furthermore, tests for heterogeneity in our meta-analysis suggested adequate homogeneity between the included studies (Chi2=7.43; df=5; p=0.19; I²=33%).

(a) Meta-analysis of cardiovascular (CV) death or heart failure (HF) hospitalization. The total shows the HR 0.88 (0.83–0.93), the heterogeneity test; Chi2=3.23, df=3, (p=0.36); I²=7%; Test for overall treatment effect: Z=4.41 (p<0.0001); (b) Meta- analysis of cardiovascular (CV) death or heart failure (HF) hospitalization with the subgroups accordings to eGFR. The total shows the HR 0.89 (0.83–0.95), the heterogeneity test; Chi2=0.59, df=1, (p=0.44); I²=0%. The name and year of the studies are presented followed by weight of each study and the hazard ratio (HR) with 95% confidence interval (CI).
Adverse events and discontinuation of therapy
We found that, in contrast to monotherapy, dual blockade increased the risk of adverse events by 40% overall (40% for renal impairment, 44% for hyperkalemia, and 42% for hypotension) (Figure 4(a)). Furthermore, treatment discontinuation following the occurrence of adverse events was described in 3.68% of patients undergoing dual blockade and 2.19% of patients receiving monotherapy. In terms of RR, the risk of adverse events in patients undergoing dual RAS blockade significantly increased to 1.72 overall (1.66 for renal impairment, 2.21 for hyperkalemia, and 1.55 for hypotension) (p<0.00001) (Figure 4(b)).

(a) Meta-analysis of adverse events and (b) discontinuation of treatment by renal impairment, hyperkalemia, and hypotension. (a) The total shows RR 1.40 (1.29–1.52), the heterogeneity test: Tau2=0.01; Chi2=23.68, df=16, (p=0.24); I²=26%; Test for overall treatment effect: Z=8.23 (p<0.00001). Test for difference between subgroups: Chi2=0.04, df=2, (p=0.98); I²=0%. (b) The total shows RR 1.72 (1.48–1.99), the difference between subgroups: Tau2=0.02; Chi2=24.18, df=18, (p=0.15); I²=26%; Test for overall treatment effect: Z=7.11 (p<0.00001). Test for difference between subgroups: Chi2=1.69, df=2, (p=0.43); I²=0%. The graph shows the name and year of the studies followed by the number of events and the total number of participants, comparing dual blockade versus monotherapy with the total number of participants, weight admitted to the study, relative risk (RR) with 95% confidence interval (CI).
Discussion
Summary of evidence
RAS blockade has a key role in the treatment of HF. RAS inhibition can be achieved with a single-drug therapy using ACEIs, ARBs, or aliskiren. More effective RAS inhibition can also be achieved with the combination of two or more of these drugs, which inhibits alternative pathways of angiotensin II generation.14,28 Nevertheless, combination therapy increases the risk of some adverse events,19,20,29 and raises the concern of whether the risks overcome its benefits. Although 30–40% of patients with HF have RD, the impact of dual RAS inhibition on these patients has not yet, to our knowledge, been investigated. Here, we describe the first meta-analysis examining the effect of dual RAS blockade in HF patients with and without RD.
We selected 12 studies in our review.17,18,26,30 Among these studies, eight investigated dual blockade with a combination of ARBs and ACEIs, and four with aliskiren and ACEIs/ARBs.
Our meta-analysis found that, in relation to monotherapy, dual blockade did not reduce death in the overall population, though there was a trend toward combination therapy being beneficial (p=0.07) (Figure 2(a)). While this result is similar to former meta-analyses,19,20 it must be observed that these previous meta-analyses did not include results from the ATMOSPHERE 26 and ASTRONAUT 17 studies, in which dual RAS blockade was carried out with aliskiren.
We also compared the effect of dual RAS inhibition on death rates between patients with and without RD. Our results demonstrated that rates of death did not significantly differ within these groups (p=0.16) (Figure 2(b)). It should be noted that we did not include the other studies in this analysis because the results comparing outcomes between those with and without RD still have not been published.
To further investigate whether dual RAS blockade can have a positive impact on patients with HF, we then examined rates of CV death or HF hospitalization. Our results demonstrated that, in comparison to monotherapy, dual RAS blockade significantly reduced the risk of CV death or HF hospitalization by 12% (p<0.0001) in the overall population (Figure 3(a)). Interestingly, combining RAS inhibitors was also observed to have favorable outcomes in patients both with and without RD, reducing hazard ratios by 14% and 9%, respectively, in these patient groups (Figure 3(b)). In other words, the beneficial effect of dual RAS blockade did not differ according to eGFR.
Our meta-analysis provides some insights into the controversy surrounding the effect of dual RAS blockade in the treatment of patients with HF. While the Val-HeFT study found that combination therapy was beneficial, 16 the ASTRONAUT 17 and ATMOSPHERE 26 studies did not. The explanation for these discrepancies is not clear. Factors that may have influenced the results of these studies include the lower percentages of patients using beta-blockers (34.5%) and mineralocorticoid receptor antagonists (5%) in the Val-HeFT study (Table 1) than in the ASTRONAUT (81.7% and 55.4%, respectively) and ATMOSPHERE (92.0% and 36.6%, respectively) studies.16,17,26,31 However, the effect of dual RAS blockade in reducing CV death and HF hospitalization cannot be attributed to sample size weighting differences in the aforementioned studies. The sample size weighting of the RD patient subgroup in the Val-HeFT 25 study (22.7%) was larger than those in the ASTRONAUT 17 (5.2%) and ATMOSPHERE 26 (13.8%) studies. In contrast, the sample size weighting of patients without RD was smaller in the Val-HeFT 25 (19.5%) than in the ATMOSPHERE 26 (32.6%) study (Figure 3(b)).
Interestingly, the CHARM-Added study, which investigated dual blockade with an ARB (candesartan) and ACEIs in patients with HF, also found a benefit in terms of CV death or HF hospitalization (HR, 0.85; 95% CI, 0.75–0.96; p=0.01). 27 Among patients whose treatment consisted of candesartan combined with ACEIs, 55% were also using a beta-blocker and 17.4% a mineralocorticoid receptor antagonist at baseline. Furthermore, 33% of the patients had an eGFR <60ml/min/1.73m2. Unfortunately, results from this study comparing outcomes between patients with and without RD were neither published nor available 15 for analysis stratified by eGFR.
The observation of favorable results in the Val-HeFT16,25,30 and CHARM-Added15,27 studies—where dual RAS blockade was achieved with ARBs and ACEIs, and unfavorable results in the ASTRONAUT 17 and ATMOSPHERE 26 studies were identified, and whereby aliskiren was added—may suggest pharmacological differences in the RAS inhibition pathway. Both ARBs and ACEIs elevate the levels of angiotensin(1-7), the product of angiotensin I and II degradation. 32 On the other hand, aliskiren blocks RAS upstream and therefore does not increase (but may rather even decrease) the concentration of this peptide. Since angiotensin(1-7) antagonizes the deleterious actions of angiotensin II, favoring vasodilation and anti-proliferative actions, which have been shown to be cardioprotective in animal models, this may account for why favorable results were seen in the Val-HeFT 25 and CHARM-Added 27 studies but not in ASTRONAUT 17 and ATMOSPHERE. 26
To investigate this possibility, we performed a multiple treatment meta-analysis comparing studies in the literature that achieved dual blockade with ARBs and ACEIs and those that used aliskiren. We found an 11% reduction in the risk of CV death or HF hospitalization in patients treated with dual blockade instead of monotherapy (p=0.0007) (Supplementary Figure S2). On the other hand, we did not observe a significant difference among those treated with ARBs plus ACEIs and those treated with aliskiren plus ACEIs/ARBs. It is important to mention that this analysis was not the main objective of the present study.
The use of dual RAS blockade was also not favorable in terms of adverse events (Figure 4). Our meta-analysis of adverse events following combination therapy (Figure 4(a)) showed that compared with monotherapy, dual blockade increased the risk of renal impairment, hyperkalemia, and hypotension by 40%, 44%, and 42%, respectively. In addition, discontinuation due to adverse events (Figure 3(b)) also demonstrated that combination therapy led to a 4.82% (vs. 3.05% with monotherapy) rate of discontinuation due to renal impairment, 3.20% (vs. 1.41%) due to hyperkalemia, and 2.72% (vs. 1.78%) due to hypotension. These results clearly demonstrate that dual blockade therapy increases the risk of adverse events. Notwithstanding, considering that our other results suggest that combined therapy reduces the risk of CV death or HF hospitalization, we recommend that its cost-benefit ratio be evaluated for each patient since the above adverse effects can be monitored with routine exams in most patients.
A new option for RAS blockade in selected HF patients with reduced ejection fraction (NYHA class II or III) has also been recently investigated with the novel angiotensin-neprilysin inhibitor LCZ696 (Sacubitril and Valsartan). 33 This study found that LCZ696 was more effective than enalapril in terms of death and HF hospitalization, as the former reduces the risk of death from cardiovascular causes or HF hospitalization by 20% 33 . Importantly, outcomes were similar between patients with an eGFR <60 ml/min/1.73m2 and those with an eGFR ⩾60 ml/min/1.73m2.33,34 In acutely decompensated HF patients, the PIONEER-HF 35 study demonstrated that sacubitril-valsartan therapy significantly reduced N-terminal pro–B-type natriuretic peptide (NT-proBNP) concentration when compared with enalapril therapy without causing decreasing kidney function, symptomatic hypotension, and angioedema. However, this study follows the patients during only 8 weeks and data concerning hospitalization and cardiovascular mortality were still not available. New clinical trials addressing these questions are in course, such as PARADISE-MI 31 among others. Although the combination of ACEI and LCZ696 is not plausible, since it increases the risk of angioedema, as observed with Omapatrilat (combination of a neprilysin inhibitor with an ACEI), 36 we cannot rule out the association between LCZ696 and aliskiren, in spite of the fact that hypotension should be a concern.
Quality assessment
Our meta-analysis was mostly graded as having a low risk of bias (Supplemetary Figure S1). GRADE evaluation results ranged from moderate to high, according to the outcomes analyzed (Supplemetary Table S3). Together, these evaluations did not reveal any important biases that could affect the interpretation of our meta-analysis results. 37
It should be noted that the Val-HeFT 25 study was assessed as having a high risk of bias in the selective reporting domain. However, this was due to the lack of pre-specification in the protocol regarding CV death or HF hospitalization outcomes. 25 We, therefore, cannot discard this study result, since its protocol was established within the analysis of death outcomes and morbid events. In addition, despite some differences among the studies, the main clinical characteristics of the patients were similar.
Limitations
First, there were a small number of studies available that presented data of eGFR in HF trials. Second, the data extracted for meta-analysis by eGFR were obtained from subgroups in randomized clinical trials involving patients with HF. Most of the studies did not evaluate the presence of proteinuria and normal eGFRs. Last, there was variation in the average follow-up period among the studies, which ranged from 1.38 to 52.8 months (Table 1). The V-HeFT study, 1999, 38 had the shortest follow-up of 1.38 months, while the SUPPORT study had the longest follow-up period of 52.8 months.17,18,24,26
Conclusions
The present meta-analysis demonstrates that compared with monotherapy, dual RAS blockade in patients with HF and kidney dysfunction reduces the risk of CV death or HF hospitalization by 12%. Furthermore, this benefit remains in patients both with and without renal disease. Even though the combination of RAS inhibition drugs increases the risk of adverse events such as hypotension, hyperkalemia, and renal impairment, only a small percentage of patients need to discontinue treatment due to these events.
This meta-analysis contributes to the discussion of whether dual RAS blockade in patients with HF and RD should be recommended. Clinicians might be aware that dual RAS blockade displays a potential benefit and may not be categorically contraindicated in HF patients, and should evaluate the cost-benefit ratio of dual therapy for each patient.
Supplemental Material
Figure_S1_-_Risk_of_bias – Supplemental material for Effects of dual blockade in heart failure and renal dysfunction: Systematic review and meta-analysis
Supplemental material, Figure_S1_-_Risk_of_bias for Effects of dual blockade in heart failure and renal dysfunction: Systematic review and meta-analysis by Alessandra Rodrigues Silva, Alexandre Goes Martini, Graziela De Luca Canto, Eliete Neves da Silva Guerra and Francisco de Assis Rocha Neves in Journal of the Renin-Angiotensin-Aldosterone System
Supplemental Material
Figure_S2_-_ARB_vs_Aliskiren – Supplemental material for Effects of dual blockade in heart failure and renal dysfunction: Systematic review and meta-analysis
Supplemental material, Figure_S2_-_ARB_vs_Aliskiren for Effects of dual blockade in heart failure and renal dysfunction: Systematic review and meta-analysis by Alessandra Rodrigues Silva, Alexandre Goes Martini, Graziela De Luca Canto, Eliete Neves da Silva Guerra and Francisco de Assis Rocha Neves in Journal of the Renin-Angiotensin-Aldosterone System
Supplemental Material
supplemantary_material – Supplemental material for Effects of dual blockade in heart failure and renal dysfunction: Systematic review and meta-analysis
Supplemental material, supplemantary_material for Effects of dual blockade in heart failure and renal dysfunction: Systematic review and meta-analysis by Alessandra Rodrigues Silva, Alexandre Goes Martini, Graziela De Luca Canto, Eliete Neves da Silva Guerra and Francisco de Assis Rocha Neves in Journal of the Renin-Angiotensin-Aldosterone System
Footnotes
Acknowledgements
The authors wish to thank Dr. Anastasia Lesogor and Dr. Tsushung A. Hua for sending the requested data of Val-HeFT study for the meta-analysis.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by Ministry of Education of Brazil, Coordenação de Aperfeiçoamento de Pessoal de Nıvel Superior (CAPES) and by Brazilian Research Council (Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq 309989/2014-0), to FARN. ARS was supported by a CAPES fellowship.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.