
Abstract
Introduction:
The captopril challenge test (CCT) is the major confirmatory test for primary aldosteronism (PA), and frequently carried out because of its convenience. However, it presents false-negative results with a certain probability, and as there are many criteria for CCT, it is not concluded yet which criteria to use.
Materials and methods:
A total of 71 PA patients were evaluated. We compared CCT-positive and CCT-negative patients in the following three criteria: plasma aldosterone/renin ratio (ARR) >200 after the CCT (criterion 1); plasma aldosterone concentration (PAC) >120 pg/ml after the CCT (criterion 2); and PAC suppression <30% of PAC before CCT (criterion 3).
Results:
The positive rate was 70.4%, 64.8% and 54.9% for criterion 1, criterion 2 and criterion 3, respectively. With criterion 1, the baseline plasma renin activity was lower, thus baseline ARR was higher in CCT-positive patients. With criterion 2, PAC was higher and estimated sodium intake and K were lower in CCT-positive patients. With criterion 3, K and PAC were lower in CCT-positive patients. Although it was not significant, in the patients with high sodium intake, the positive rate of criterion 1 was higher than that of the other criteria.
Conclusions:
ARR>200 is the valuable criterion for the diagnosis of PA.
Introduction
Primary aldosteronism (PA) is characterized by autonomous production of aldosterone from the adrenal glands that is not regulated by angiotensin II (Ang II) or plasma potassium concentrations. 1 PA is the leading cause of secondary hypertension, seen in 5–10% of patients with hypertension. 2 It is especially frequent in resistant hypertension and reported to account for 3.9% in stage 1 hypertension and 11.8% in stage 3 hypertension. 3
Aldosterone hypersecretion predicts the progression of hypertension in normotensive patients 4 and is the independent risk factor for mortality in heart failure patients. 5 Thus, PA patients are more prone to cardiovascular diseases, such as stroke, myocardial infarction and atrial fibrillation, and it is urgent to identify such patients promptly. 6
While the plasma aldosterone/renin ratio (ARR) is a simple method to identify PA patients 7 and is recommended as screening method in current guidelines,8–10 confirmatory tests are also recommended to diagnose PA.8–10 In the guideline from the Japanese Society of Hypertension (JSH), one of the following confirmatory tests must be used to diagnose PA: captopril challenge test (CCT), 11 upright furosemide loading test, saline loading test 12 or oral sodium loading test. 13 Similarly, in the guideline from the Japan Endocrine Society (JES), it is recommended that the definitive diagnosis be made when at least two of three confirmatory tests (CCT, upright furosemide loading test and saline loading test) are positive. Nevertheless, it has not yet been determined which confirmatory test is the best.
CCT was proposed to be useful in discriminating PA from essential hypertension (EH) in 1983. 14 It was reported to be as effective as the sodium loading test in confirming PA. 15 In Japan, the consensus statement published in 2016 recommends CCT as the first choice because of its convenience and safety. CCT raises the accuracy of definitive diagnosis when added to the measurement of ARR alone. 16
However, the CCT has false-negative results in some cases. Mulatero et al. noted that CCT might be misleading in confirming the diagnosis. 17 Because CCT is relatively safe and easily carried out in outpatients, physicians might rule out PA simply by the fact that the CCT is negative. Furthermore, although there are several criteria for CCT in guidelines, it is not assessed yet whether there are differences in the clinical features between CCT-positive patients and CCT-negative patients in various criteria.
Therefore, we compared and examined influencing factors for the differences between CCT-positive and CCT-negative patients in each criterion of CCT recommended in current guidelines to elucidate the points to note when we use these criteria for PA diagnosis.
Materials and methods
Participants and the CCT procedure
A total of 71 patients who were finally diagnosed with PA based on the guideline from JSH 10 in our hospital from 2011 to 2017 were included. In detail, all the patients fulfill ARR >200, plasma aldosterone concentration (PAC) >120 pg/ml, and at least one confirmatory testing other than CCT. Our study protocol was approved by the Ethics Committee of The Jikei University School of Medicine (No. 30-410), and informed consent was obtained from all patients participating in the study.
All antihypertensive agents except for calcium channel blockers and α-blockers were withdrawn at least 6 wk before the baseline blood sample, confirmatory testing and adrenal vein sampling (AVS). Baseline blood samples were taken one day after the patients remained in the recumbent position for at least 30 min. Baseline urine samples were obtained at the same time. All blood and urine samples were examined by SRL Inc. (Tokyo, Japan). All the patients who have visible adenoma with computed tomography (CT) underwent 1 mg dexamethasone suppressing test as previously described 18 and there were no patients who were diagnosed with subclinical Cushing’s syndrome or Cushing syndrome.
CCT was carried out on another day. All patients underwent CCT in the morning. The blood samples were obtained just before the patients received 50 mg of captopril at approximately 8:00 a.m. Then, 90 min after captopril administration, blood samples were again obtained, and before taking blood samples, patients remained in the recumbent position for at least 30 min.
The comparison of CCT criteria
In the guideline from JSH, a criterion for CCT is ARR >200 at 60 or 90 min after captopril administration. 10 In the guideline from JES, the three criteria for CCT are: ARR >200; PAC/active renin concentration ratio >40; and PAC >120 pg/ml at 60 or 90 min after captopril administration. 9 On the other hand, in the Endocrine Society clinical practice guideline, the value of PAC after the CCT (post PAC) remains elevated, not suppressed. More than 30% of the value of PAC before the CCT (pre PAC) is used as the criterion. 8 Therefore, each of the criteria was compared: ARR >200 (criterion 1); PAC >120 pg/ml (criterion 2); and post PAC >0.7 × pre PAC (criterion 3). The clinical features and the rates of a positive upright furosemide loading test and saline loading test were compared between the CCT-positive and CCT-negative groups using each criterion. In addition, we compared the characteristics of PA patients in accordance with the number of the positive results in various criteria for CCT; group 1: CCT positive in all the criteria; group 2: CCT positive in one or two criteria; group 3: CCT negative in all the criteria.
Procedures of confirmatory tests other than CCT for PA
The other confirmatory tests for PA were performed as described in JSH guideline. 10 In the upright furosemide loading test, plasma renin activity (PRA) <2.0 ng/ml/h at 2 h after furosemide infusion was considered a positive. In the saline loading test, PAC >60 pg/ml at 4 h after saline infusion was considered a positive result.
AVS
AVS was carried out on another day. Criteria for adequate catheterization were defined as an adrenal venous cortisol concentration after adrenocorticotropic hormone (ACTH) stimulation ⩾200 μg/dl and an adrenal venous cortisol concentration after ACTH stimulation ⩾5 times the cortisol concentration from the inferior vena cava, as described in the current guideline. 9 The adrenal venous blood aldosterone/cortisol (A/C) ratio after ACTH stimulation was calculated bilaterally. An adrenal PAC after ACTH stimulation ⩾14,000 pg/ml was defined as aldosterone hypersecretion. When it was present in each of the adrenal glands and if the lateralized ratio calculated as the adrenal vein A/C ratio on the high value side/low value side was ⩾4, and the contralateral ratio calculated as the adrenal vein A/C ratio on the low value side/high value side was <1, the patient was diagnosed as having unilateral hypersecretion. If the patient did not meet each of the requirements above, the patient was diagnosed as having bilateral hypersecretion.
Formula to estimate sodium and potassium excretion
The estimated amount of creatinine excreted per day was calculated by the formula (–2.04 × age (y) + 14.89 × body weight (kg) + 16.14 × height (cm) – 2244.45 mg/d), and then the estimated amount of sodium excreted per day was calculated as 21.98 × [(urinary sodium concentration/urinary creatinine concentration) × estimated creatinine excretion] 0.392. 19 Similarly, the estimated amount of potassium excreted per day was calculated as 7.59 × [(urinary potassium concentration/urinary creatinine concentration) × estimated creatinine excretion] 0.431. 19
Statistical analysis
Data are described as means ± standard deviation. P<0.05 was considered significant. The significance of differences between the CCT-positive and CCT-negative groups was assessed by the Mann–Whitney U test. The comparison between three groups in accordance with the number of the positive results was assessed by the Kruskal–Wallis test. The associations between parameters were analyzed by Pearson’s product moment correlation coefficient. One-way analysis of variance was used to compare the positive rate of each criterion.
Multivariable logistic regression models were employed to elucidate the factors contributing to the result of each criteria. Multivariate regression analyses were operated to identify the factors related to ARR value or PAC value after CCT.
All statistical analyses were performed with EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria). More precisely, it is a modified version of R commander designed to add statistical functions frequently used in biostatistics. 20
Results
A total of 71 patients were included. Their mean age was 50.3±10.4 y, and 69.0% of patients were male. Overall, 67.6% of patients received only calcium channel blockers before the CCT, and 2.8% received calcium channel blockers and α-blockers at the time of the CCT. The baseline values of PRA and PAC were 0.43±0.30 ng/ml/h and 229.0±189.4 pg/ml, respectively, and ARR was 911.3±1897.6. From CT, 38.0% of the patients had unilateral or bilateral adrenal adenomas. Unilateral hypersecretion was verified in 21.1% of patients. Estimated sodium excretion by day was 145.3±41.2 mEq/d. Of the 71 patients, 83.3% and 76.1% of them were positive on the upright furosemide loading test and saline loading test, respectively.
Subsequently, the positive rate for each of the diagnostic criteria of CCT was evaluated and found to be 70.4%, 64.8% and 54.9% for criterion 1, criterion 2 and criterion 3, respectively. The positive rate of each criterion was not different significantly (P=0.15).
For criterion 1, the patients with unilateral hypersecretion were more likely to be included in the CCT-positive group. Although there was no significant difference in PAC between the CCT-positive and CCT-negative groups, PRA was significantly lower, and thus ARR was significantly higher in the CCT-positive group. The estimated amount of sodium excretion and the serum adrenaline and noradrenaline concentrations were not different between the two groups (Table 1).
Comparison between captopril challenge test (CCT)-positive and CCT-negative patients using the criterion of aldosterone/renin ratio >200.

Also, for criterion 2, the patients with unilateral hypersecretion were more likely to be included in the CCT-positive group. Serum potassium concentration was significantly lower in the CCT-positive group, and estimated sodium and potassium excretion from urine were significantly lower in the CCT-positive group. Although there was no significant difference in ARR between the two groups, PAC was significantly higher in the CCT-positive group (Table 2).
Comparison between captopril challenge test (CCT)-positive and CCT-negative patients using the criterion plasma aldosterone concentration >120 pg/ml.

For criterion 3, the patients with unilateral hypersecretion were again more likely to be included in the CCT-positive group. Serum potassium concentration was significantly lower in the CCT-positive group, and serum noradrenaline concentration was significantly lower in the CCT-positive group. Although the difference was relatively small, PAC was significantly lower in the CCT-positive group (Table 3).
Comparison between captopril challenge test (CCT)-positive and CCT-negative patients using the criterion of post plasma aldosterone concentration (PAC) >0.7 × pre PAC.

The differences in the ARR and PAC values after the CCT between the unilateral and bilateral PA groups were evaluated. The values of both PAC and ARR after the CCT were similarly and significantly higher in unilateral PA (PAC 362.7±374.4 pg/ml versus 193.2±66.9 pg/ml, P<0.005; ARR 2203.9±3909.6 versus 565.0±424.5, P<0.005), which explain the reason that the patients of unilateral hypersecretion were much more included in the CCT-positive group in all the criteria. On the other hand, there was no significant difference in the ratio of PAC after the CCT to PAC before the CCT between unilateral hypersecretion and bilateral hypersecretion (0.79±0.15 versus 0.76±0.28, P=0.17). In the CCT-negative patients of each criteria, the patients with unilateral hypersecretion were 4.8%, 8.0% and 9.4%, respectively. There were no significant differences between the groups (P=0.83).
Since baseline ARR differed between the two groups for criterion 1 because of the PRA, factors related to PRA variation were further explored. While sodium intake has been found to be inversely related to the synthesis and release of renin, 21 in the present study, sodium intake estimated by urinary sodium excretion was not correlated with the PRA value (Figure 1(a)). Although urinary sodium excretion was also not correlated with ARR (Figure 1(b)), it was significantly and inversely correlated with PAC (Figure 1(c)).

Relationships between plasma renin activity (PRA), aldosterone/renin ratio (ARR) and plasma aldosterone concentration (PAC) with 24-h estimated sodium excretion. (a) There is no significant correlation between 24-h estimated sodium excretion and the baseline PRA value. (b) There is no significant correlation between 24-h estimated sodium excretion and the baseline ARR value. (c) PAC is inversely correlated with 24-h estimated sodium excretion.
We underwent logistic regression analysis to evaluate which factors influence the result of each CCT criteria. We included age, estimated glomerular filtration rate, serum potassium concentration, unilateral hypersecretion, estimated sodium excretion, baseline PRA and baseline PAC. For criterion 1, baseline PRA (odds ratio (OR) 0.0057 (95% confidence interval (CI) 0.00023–0.14), P=0.0015) and age (OR 0.92 (95% CI 0.86–0.98), P=0.016) remained as the contributing factors. For criterion 2, only baseline PAC (OR 1.010 (95% CI 1.00–1.02), P=0.02) remained as the contributing factor. For criterion 3, baseline PRA (OR 0.052 (95% CI 0.004–0.638), P=0.021) and age (OR 0.95 (95% CI 0.90–0.99), P=0.040) remained as the contributing factors.
Furthermore, univariate and multivariate regression analyses were performed to identify the causal factors for ARR after CCT, PAC after CCT, and decrement of PAC after CCT. Baseline PRA, baseline PAC, serum potassium concentration and unilateral hypersecretion were independent predictors of the ARR after CCT after adjusting for adrenal adenoma, serum creatinine concentration, serum sodium concentration, estimated sodium excretion and serum noradrenaline concentration (Table 4). Baseline PAC, serum potassium concentration and unilateral hypersecretion were independent predictors of the PAC after CCT after adjusting for serum creatinine concentration, and estimated sodium excretion (Table 5). There was no independent predictor for the decrement of PAC after CCT.
Univariate and multivariate regression analyses performed to identify the causal factors for aldosterone/renin ratio after captopril challenge test.

Univariate and multivariate regression analyses performed to identify the causal factors for plasma aldosterone concentration after captopril challenge test.

As it is postulated that estimated sodium excretion, almost equal to sodium intake, was considerably related to the result of CCT in criterion 2, we compared the positive rate of each criteria on the basis of estimated sodium excretion. In the patients whose estimated sodium intake was more than the median value (estimated sodium excretion ⩾143.47 mEq/d), the positive rate of criterion 2 and criterion 3 tended to be lower than criterion 1 (criterion 1: 66.7%, criterion 2: 50.0%, criterion 3: 50.0%; P=0.27). As a matter of fact, although the positive rate was not different due to sodium intake in criterion 1 (estimated sodium excretion ⩾143.47 : estimated sodium excretion <143.47 was 66.7% : 73.5%, P=0.54), and criterion 3 (estimated sodium excretion ⩾143.47 : estimated sodium excretion <143.47 was 50.0% : 61.8%, P=0.33), the positive rate was significantly lower in the patients with more sodium intake (estimated sodium excretion ⩾143.47 : estimated sodium excretion <143.47 was 50.0% : 79.4%, P<0.01).
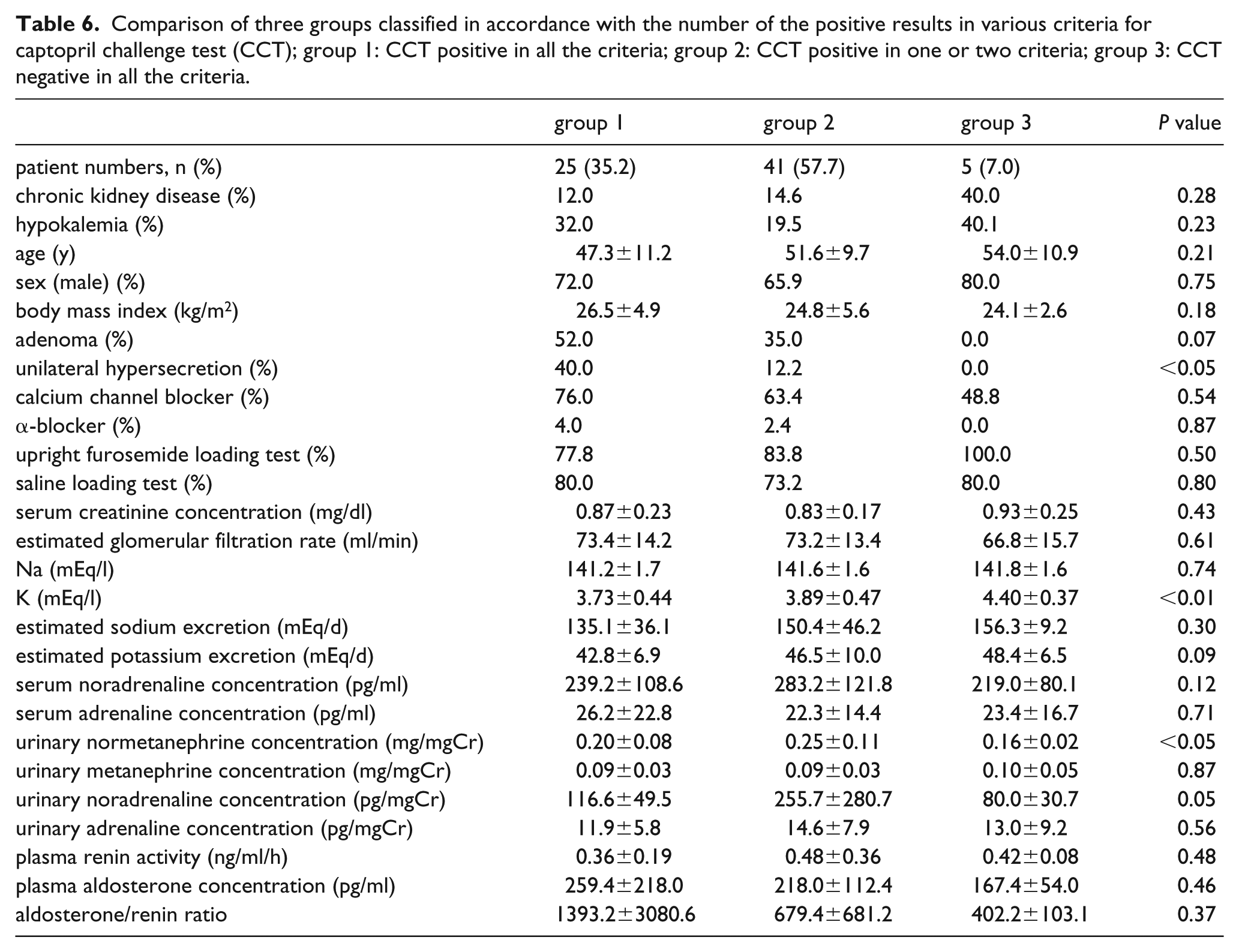
Besides, we compared the characteristics of PA patients in accordance with the number of the positive results in various criteria for CCT; group 1: CCT positive in all the criteria; group 2: CCT positive in one or two criteria; group 3: CCT negative in all the criteria (Table 6). Although PRA, PAC and ARR values were not different between the three groups, serum potassium concentration was significantly higher in group 3 than in group 1 and group 2. Furthermore, there were no patients with unilateral hypersecretion in group 3.
Comparison of three groups classified in accordance with the number of the positive results in various criteria for captopril challenge test (CCT); group 1: CCT positive in all the criteria; group 2: CCT positive in one or two criteria; group 3: CCT negative in all the criteria.
Discussion
The CCT is a confirmatory test that was first proposed in 1983, 14 and it has been broadly applied worldwide. The CCT raises the sensitivity and specificity from 95.4% and 28.3% when using the ARR value alone to 100% and 67.9%, respectively, 11 and various guidelines emphasize its usefulness for diagnosing PA. Guidelines that were recently published mention the use of confirmatory tests for PA,8–10 and the CCT is recommended preferentially because of its simplicity and safety. However, Mulatero et al. disputed the usability of the CCT because of the diversity in absorption efficiency for each patient. 17 Westerdahl et al. even argued that the ARR after the CCT is only marginally better than basal ARR measurement, so that it is almost no use administering the CCT for diagnostic confirmation. 22 Rossi et al. reported that, although the PAC values after the CCT and the saline loading test were equally helpful in PA diagnosis, the accuracy of the CCT was inferior to that of the saline loading test in patients with sodium intake less than 130 mEq/d because of renin-angiotensin system (RAS) activation. 23
Which criterion of the CCT is the best for diagnosing PA is also a matter of discussion. Naomi et al. reported first that ARR>200 after the CCT showed sufficient sensitivity (95%) and specificity (92%) in Japanese PA patients. 24 There are various reports about the thresholds for PAC after the CCT, 25 and a recent paper from Korea indicated that sensitivity and specificity of PAC >120 pg/ml after the CCT were 98% and 71.4%, respectively, 16 which meant that it showed enough reliability for PA diagnosis. Therefore, the Japanese guideline recommends using ARR>200 and PAC>120 pg/ml after the CCT as the criterion, 9 whereas the Endocrine Society clinical practice guideline recommends the use of the extent of PAC suppression. 8
Recently, two reports from China discussed which criterion is the most suitable for diagnosing PA after the CCT. Meng et al. advocated that, since the difference in the degree of PAC decline was relatively small (17.7% in EH versus 14.2% in PA), the PAC value after the CCT rather than the degree of PAC decline is better for PA diagnosis. 26 They indicated that the optimal cutoff value of PAC after the CCT was 16.7 ng/ml. Song et al. also alleged that the CCT is equally reliable for diagnosing PA with the fludrocortisone suppression test, and the area under the receiver operating characteristic curve of the CCT was higher for PAC after the CCT than for the PAC diminution rate after the CCT. 27 Nanba et al. reported that, at least for unilateral aldosterone-producing adenoma (APA) diagnosis, ARR after the CCT was as useful as PAC after the CCT. 28 As a matter of fact, ARR after the CCT was also reported to be helpful for differentiation of APA from EH and idiopathic hyperaldosteronism (IHA) at the threshold of ARR=422 (sensitivity 75.0%, specificity 81.0%). 29
For criterion 1, the ARR value was significantly higher in CCT-positive patients. As the PAC value was not different between the two groups, the PRA discrepancy is the main reason for this ARR dissimilarity. In general, PRA is suppressed in PA patients. PRA has been shown to be modulated by sodium intake, Ang II, the sympathetic nervous system (SNS), atrial natriuretic peptide and autacoids such as prostaglandins, nitric oxide and adenosine.21,30 We explored the relationship between PRA, PAC and estimated sodium excretion, and elucidated that, at least in our study, estimated sodium excretion was correlated not with PRA but with PAC. As sleep apnea syndrome is found to be associated with hyperaldosteronism, and leads to SNS activation,31,32 and renal sympathetic nerve activity is indicated to be the mediator of renin secretion, this coexisting disease might affect the PRA value. We evaluated the correlation between serum, urine noradrenaline concentration and PRA value, and found that PRA value was significantly correlated with serum noradrenaline value, but it was not correlated with urine noradrenaline value.
Although PRA is regulated by sodium intake change, in the stable state, PRA is reported to be not necessarily correlated with 24-h urine sodium excretion. 33 Furthermore, as we employed spot urine sodium measurements which do not take circadian changes in sodium excretion throughout the day and changes in diet into account to predict the estimated sodium excretion, 19 it might not reflect actual 24-h sodium excretion. 34 Therefore, it was not possible to rule out the effect of sodium intake from the spot urinary specimens alone. It is also difficult to evaluate the strength of SNS activation by a single index. Since all catecholamines released are ultimately excreted in urine, measurements of urinary catecholamine excretion and its metabolites might provide information about the strength of SNS activity. 35 However, it is indicated that the reproducibility of the measurements was relatively low. 36
Furthermore, circulating norepinephrine levels are only a minor fraction of the amount derived from sympathetic nerve terminals and might not reflect SNS activity.35,37 In fact, a current review emphasized that the measurement of plasma norepinephrine (or any other single measurement) cannot be taken as a sensitive or specific marker of overall sympathetic activity. 37 Hence, the influence of SNS activity on PRA dissimilarity cannot be discounted.
From these data, it is suggested that we should beware of both baseline PRA and baseline PAC when we select this criterion.
For criterion 2, estimated sodium excretion was significantly less in the CCT-positive group. Although it seems that this is in conflict with the report from Rossi et al., which indicated that false-negative results increase in patients with sodium intake less than 130 mEq/d because of PRA augmentation, 23 their report presumed ARR>300 to be CCT-positive, which might explain the reason for this deviation. Since sodium depletion activates the RAS in general, it might increase the PAC value and lead to CCT-positive results when the PAC value after the CCT is used as the criterion. In fact, although estimated sodium excretion was not correlated with PRA and ARR, it was inversely correlated with PAC.
On the other hand, although serum potassium concentration was significantly lower in the CCT-positive group, estimated potassium excretion in urine was also lower in the CCT-positive group. It is reported that 48% of the patients with APA and 17% of those with IHA had serum potassium concentrations under 3.5 mmol/l. 38 Hypokalemia can be caused either by a deficit of potassium intake or by excessive excretion of potassium in the urine and gastrointestinal tract 39 and in general, it is postulated that excessive aldosterone secretion leads to increased potassium excretion from the urine, which is indicated to be the main reason of hypokalemia in PA patients. 8 Therefore, it is incompatible with our data. We cannot elucidate the precise reason for this discrepancy, but it might be due to the lack of reliability with the formula to estimate the potassium ingestion only from a one-time urine sample because it is carried out at an arbitrary time in outpatient visits.
As estimated sodium excretion was significantly different between CCT-positive and CCT-negative patients in criterion 2 whereas there was no significant difference in criterion 1, we compared each criterion from the aspect of estimated sodium intake. Although it did not reach significance, the positive rate of CCT was relatively lower for the patients with high sodium intake in criterion 2 and criterion 3 than in criterion 1, and, actually, the positive rate of CCT was significantly lower in the patients with high sodium intake in criterion 2. Although the formula we adopted for the presumption of sodium intake is not validated enough, we demonstrated that sodium intake presumed by the formula in one day was significantly correlated with the sodium intake calculated in another day (data not shown). Hence, the estimated value was consistent to some extent. Therefore, we must consider the estimated amount of sodium ingestion particularly when we use this criterion for PA diagnosis.
For criterion 3, the PAC value was significantly lower in the CCT-positive group.
As the reduction rate of PAC is adopted in this criterion, the patients whose baseline PAC was high might tend to be included in the CCT-negative group. Furthermore, the serum potassium concentration was significantly lower in the CCT-positive group. Univariate and multivariate regression analyses revealed that decrement of PAC after CCT was not influenced by any variables we adopted in our study. It means that the result of criterion 3 was relatively independent of baseline status of PRA, PAC thus ARR. However, as the positive rate of this criterion was the lowest among all criteria, and about half of the PA patients are misdiagnosed with this criterion, we consider that this criterion is short of reliability.
In our study, the positive rate of criterion 1 was significantly higher than that for criterion 2. It seems different from a previous report which showed that the area under the curve (AUC) of ARR after CCT was lower than the AUC of PAC after CCT. 27 We speculated two reasons for this discrepancy. For the first, although we adopted PRA to calculate ARR, their study adopted plasma renin concentration (PRC) to calculate ARR. Although PRA is proposed to be correlated with PRC to some extent, there might be discrepancies in some cases. Besides, although their study did not present the baseline value of PRA, PAC or ARR, the PAC value before CCT in our study (215.7±110.7 pg/ml) was relatively lower than their study (29.5 ng/dl). Hence, the patients in our study tend to exhibit a negative result in the criterion based on the PAC value.
As unilateral forms of PA are able to be cured by unilateral adrenalectomy,40,41 a current guideline emphasizes the importance of discriminating unilateral hypersecretion from bilateral hypersecretion. 8 Therefore, it is exceedingly important not to overlook the patients with a unilateral form of PA. As patients with unilateral hypersecretion were significantly more included in the CCT-positive group in all the criteria, and the false-negative rate of CCT was not different significantly between the three criteria, these three criteria are equally useful from this perspective. Moreover, as there was no patient with unilateral hypersecretion in the group which presented a negative result in all the criteria, CCT might be a useful method to rule out the possibility of unilateral hypersecretion.
Conclusions
In the present study, it is suggested that although there are several criteria in CCT, we should evaluate baseline PAC level, PRA level and sodium intake beforehand, in order to make a precise examination of CCT. Furthermore, ARR >200 after the CCT seems to be the useful criterion, because it shows the highest positive rate and it is not influenced relatively by the amount of sodium intake. However, we must take into consideration that it is not always correct to ignore the possibility of PA simply because the CCT is negative, since 30% of PA patients exhibit a negative result even for this criterion.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.