
Abstract
Introduction:
Bilateral nephrectomy leads to a short-term reduction in blood pressure. This is mainly due to a sharp change in the circulating renin-angiotensin system (RAS), but data on the long-term outcomes of their clinical status and further changes in circulating RAS are rare.
Materials and methods:
We enrolled four Chinese patients who had both of their kidneys removed two (1), six (1) and eight (2) years prior to this study, respectively. Their clinical data were collected retrospectively and circulating RAS was evaluated by radioimmunoassay.
Results:
Hypotension after surgery occurred in two patients who suffered thrombosis of the arteriovenous fistula, but no life-threatening complications occurred. The average hemoglobin level was 103.3±12.3 g/l. Two patients without hemorrhage received intravenous erythropoietin (EPO) of 4500–8000 iu/week. Extremely low plasma renin activity (PRA) of 0.08±0.03 ng/ml (normal range 0.93–6.56 ng/ml) showed in the patients. Surprisingly, plasma angiotensin II concentration (71.37±8.28 pg/ml) and aldosterone level (0.17±0.02 ng/mlng/ml) were within the normal range.
Conclusions:
The four anephric individuals did not suffer life-threatening complications while their hypotension gradually subsided and their EPO dosage was relatively low. Although their PRA level was extremely low, they produced normal levels of angiotensin II and aldosterone in plasma, which indicates the kidney-independent mechanism of angiotensin II production likely compensated in the long term.
Introduction
Bilateral nephrectomy has been reported to be conducted in patients with end-stage renal disease (ESRD) to address various conditions, including drug-resistant hypertension, malignancy, and polycystic kidney disease. It leads to a short-term reduction in blood pressure (BP), mainly due to a sharp change in the circulating renin-angiotensin system (RAS), but data on the long-term outcomes of clinical status and further changes in circulating RAS are limited. In the present study we investigated the clinical life status of hemodialysis (HD) patients 2–8 years after bilateral nephrectomy to better understand the long-term prognosis of this procedure. In addition, we observed changes in BP and evaluated the levels of RAS components in circulation in anephric patients.
Materials and methods
Case series
Four cases with bilateral nephrectomy were identified among 304 patients on maintenance HD in our dialysis center in December 2016. These individuals had been dependent on HD with three sessions weekly for one to 15 years before bilateral nephrectomy, and continued maintenance HD thrice a week until the time of this study. They underwent unilateral nephrectomy twice, and had their second kidney removed two to six months after the first. Clinical and laboratory data were obtained by retrospective review of medical records, detailed in Table 1. Participants were seated for 30 minutes before blood samples for RAS component tests were taken from peripheral veins immediately before HD was started. Diet and medication were not altered for the two weeks prior to blood drawing. Blood was centrifuged immediately at 2500 g for 10 minutes at 4°C, and plasma was stored at −20°C. One patient (patient 4) who refused to give blood was excluded from the circulating RAS test.
Clinical and laboratory findings of anephric patients.

BP: blood pressure; EPO: erythropoietin; ESRD: end-stage renal disease; F: female; HGB: hemoglobin; iPTH: intact parathyroid hormone; iv: intravenous; M: male.
Circulating RAS evaluation
Plasma renin activity (PRA) was quantified using an iodine (125I) angiotensin I (Ang I) radioimmunoassay kit (Beijing North Institute of Biological Technology, China). In brief, 1 ml plasma, acquired from centrifugation of ethylenediaminetetraacetic acid tubes collected during blood draw, was mixed with 100 µl maleate buffer and 10 µl phenylmethylsulfonyl fluoride solution. Two aliquots of each sample were incubated for one hour at 4°C and 37°C, respectively, and then mixed with 100 ul (125I) Ang I and rabbit anti-Ang I antibody. After incubation for 16–24 hours at 2–8°C, 500 ul of donkey antirabbit immune separation reagent was added to each tube, and angiotensin II (Ang II) concentration was evaluated with radioactive assay of the precipitate compared with the standard control. PRA was calculated by subtraction of Ang I concentration at 4°C from Ang I concentration at 37°C.
Next, an Ang II assay was performed with an iodine (125I) Ang II radioimmunoassay kit (Beijing North Institute of Biological Technology) according to the manufacturer’s instructions. Briefly, based on the rule of competitive inhibition, 200 µl plasma or standard control and 200 µl tracer (125I-Ang II) were incubated for 16–24 hours with rabbit anti-Ang II antibody. Mixed with 500 µl of donkey antirabbit immune separation reagent, Ang II concentration was evaluated with radioactive assay of the precipitate compared with the standard control.
Plasma aldosterone concentration was measured by radioimmunoassay with an iodine (125I) aldosterone radioimmunoassay kit (Beijing North Institute of Biological Technology). A total of 100 µl plasma or standard control and 100 µl tracer (125I-aldosterone) was incubated for 16–24 hours with rabbit antialdosterone antibody. Mixed with 500 µl of donkey antirabbit immune separation reagent, the mixture was placed still for 15 minutes and then centrifuged at 3500 rpm for 15 minutes. Then a radioactive assay of the precipitate was performed. The aldosterone concentration of sample was calculated by comparison with the standard control.
Results
Clinical features
As shown in Table 1, the four anephric patients were all Chinese with ages ranging from 49 to 80 years old; three were female. The reasons for nephrectomy included size expansion of polycystic kidney disease (n = 1), cancer (n = 2), and pain due to hydronephrosis (n = 1). Malignant hypertension was not the main reason for nephrectomy in any patient. Nephrectomy was conducted two to eight years prior to this study. Hypotension after surgery occurred in patient 1 and patient 3, whose BPs before nephrectomy were below 140/90 mmHg without the use of antihypertensive drugs. They had hypotension mostly during dialysis, and in one of them this lasted for six years before BP rose again. Thrombosis of the arteriovenous fistula was noted in these two hypotensive patients, but no life-threatening complications such as cardiac infarction, severe dysrhythmia, cerebral infarction or pulmonary embolism resulted from the low BP. Patient 1 had her in situ thrombosis of fistula half a year after bilateral nephrectomy, and had further surgery to remove the thrombus. Patient 3 suffered the thrombosis of fistula twice about two years after kidney surgery and underwent surgery to remove the thrombus and repair the fistula.
Based on 48-hour BP monitoring during one dialysis cycle, the systolic blood pressures (SBPs) during dialysis and between dialysis of all four patients were at 90 mmHg or above, with the lowest SBP of 90 mmHg and diastolic blood pressure of 46 mmHg occurring during dialysis and at midnight, respectively. Patient 2 was the only case in whom severe hypertension recurred four years after nephrectomy. At present, his BP has not been well controlled despite antihypertensive therapy of six drugs including valsartan (80 mg/day), perindopril (8 mg/day), amlodipine (10 mg/day), nifedipine (120 mg/day), metoprolol (150 mg/day) and prazosin (3 mg/day). The average hemoglobin level was 103.3±12.3 g/l. Patients 2 and 4 experienced hemorrhage of the digestive tract, and thus were treated with high doses of erythropoietin (EPO). The other two patients who did not suffer hemorrhage received intravenous EPO doses of only 4500–8000 iu/week (Figure 1 and Table 1).

Blood pressure (BP) of the four cases over 48 hours including during dialysis and during dialysis interval. The first three data points for all patients were of the last 10 dialysis sessions. Other data points were collected from ambulatory BP monitoring.
RAS level in circulation
All three tested patients presented with extremely low PRAs of 0.08±0.03 ng/ml, compared with a normal range of 0.93–6.56 ng/ml (Table 2). However, their plasma Ang II concentration of 71.37±8.28 pg/ml and aldosterone level of 0.17±0.02 ng/ml were within normal limits.
Circulating RAS of anephric patients.
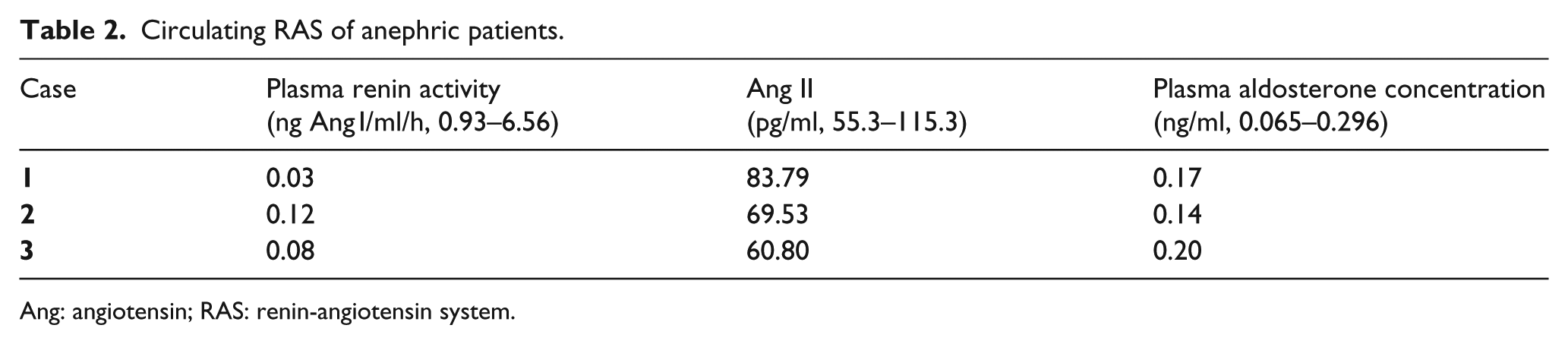
Ang: angiotensin; RAS: renin-angiotensin system.
Discussion
Bilateral nephrectomy is seldom conducted in ESRD patients on dialysis, with the most frequently reported reason for it being to treat drug-resistant hypertension. However, the four cases presented in our study had additional reasons to remove their kidneys, including polycystic kidney disease, malignancy and hydronephrosis. A decrease in BP after surgery is expected in patients with uncontrolled hypertension, but it becomes concerning in patients receiving the surgery for BP-independent reasons like the four patients in this study. As reported in the literature review in Table 3, there are limited data about the long-term clinical status of anephric patients. Therefore, we conducted our research to describe the overall clinical outcomes of bilateral nephrectomy for up to eight years after surgery. We also assessed circulating RAS components to understand the potential mechanism involved in changes in BP regulation after surgery.
Summary of published studies on the effects of bilateral nephrectomy (without simultaneous transplantation) on BP and circulating RAS in ESRD adults.

Ang: angiotensin; BP: blood pressure; ESRD: end-stage renal disease; h: hour; NA: not available; RAS: renin-angiotensin system.
In the literature review showed in Table 3, the majority of the reports indicated improvement of hypertension after nephrectomy. But they seldom mentioned low BP-related complications, and mainly focused on the recent effect of nephrectomy on BP with the longest observation period of only three years. Our results will fill in the blank of long-term assessment of clinical manifestation of this kind of patients.
In our research, a decrease in BP was observed in all four patients, indicating the definite effect of BP change of bilateral nephrectomy. Hypotension did occur soon after surgery in two patients whose BP was not high before. One of them lasted for six years before BP rose again, and the other did not show BP recovery within the limited observation time available. Thrombosis of the arteriovenous fistula happened in the period of low BP status. Fortunately, the fact that neither suffered life-threatening complications, such as cardiac infarction, severe arrhythmia, cerebral infarction or pulmonary embolism reduced our concern about severe side effects of bilateral nephrectomy to some extent. One case with severe hypertension before surgery developed extremely high BP again four years after nephrectomy, indicating that critical hypertension can recur after nephrectomy.
RAS is known to play a pivotal role in BP control and undergoes drastic change after bilateral nephrectomy. In a literature review, however, only three reports discussing circulating RAS activity in anephric patients were found in the PubMed database (Table 3). The three reports agree that PRA decreases after surgery, but opinions about the plasma concentration of Ang II are controversial. In our study, we detected plasma RAS level again to observe the precise change of it to better understand the mechanism of BP control. We observed that renin activity was extremely low in all three patients tested, even in one taking angiotensin-converting enzyme inhibitors and Ang II receptor blockers. Surprisingly, although PRA was much lower than normal as reported in the literature, plasma Ang II and aldosterone levels of all three patients were in the normal range, which paralleled a previous study. 1 We speculate that the disagreement among the other studies may be relevant to the distinct time of assessment. According to the report by Ferrario et al., the plasma Ang II of rats 48 hours after bilateral nephrectomy significantly dropped by 66%, 2 indicating that Ang II undergoes a prominent fall in plasma early after removal of renin from the kidneys.
The nonparallel change in circulating renin and Ang II in our findings provides further evidence that renal and plasma renin are not the only enzymes that catalyze the production of angiotensins, and there is a part of plasma angiotensin that is produced by extrarenal mechanisms. Because Ang II has been found to be released from diverse vascular tissue, the vascular system seems to be the best candidate responsible for this compensation mechanism.9,10 RAS components have been detected not only in the adipose tissue of humans and rodents but also in cultured adipocytes. Human adipocytes express angiotensinogen, renin, angiotensin-converting enzyme, Ang II type 1 receptor, and Ang II type 2 and Mas receptors.11–13 Adipose tissue may also produce RAS independently from circulating renin. Also, it has been reported in rats that cardiac tissue expression of renin significantly decreases along with the abolition of plasma renin after bilateral nephrectomy, but myocardial Ang II expression is upregulated, indicating a renin-independent mechanism was responsible for Ang II production. 8 Local RAS production has also been reported in the brain 14 and adrenal glands. 15 Therefore, it is possible that the cardiovascular system and other tissues may become potent producers of Ang II when the kidneys are removed. However, there has not been any direct evidence of this to date.
There is accumulating evidence that RAS takes part in erythropoiesis. Ang II is known to enhance erythropoiesis by acting as a growth factor for erythroid progenitors to increase red blood cells in cooperation with EPO and by stimulating EPO secretion. 16 It is noteworthy that recent studies have identified the expression of prorenin receptor (pRR), a specific receptor for renin and prorenin, in erythroid cells.17,18 Overexpression of pRR leads to partial negative regulation of erythropoiesis in chronic inflammation. 5 Therefore, we speculate that the extremely low levels of PRA in anephric patients may lead to an insufficient combination of pRR on erythroid cells with renin, contributing to the amelioration of anemia, but the exact conclusion requires further study.
Conclusion
In conclusion, two to eight years after surgery, the four anephric cases did not suffer life-threatening complications related to their hypotension, and their BP gradually recovered. Their PRAs were extremely low, but plasma levels of Ang II and aldosterone were normal, which indicates that the kidney-independent mechanism of Ang II production might play an important role in RAS regulation in the long term after removal of the kidneys.
Footnotes
Acknowledgements
The authors thank the team at Beijing North Institute of Biological Technology for the assessment of circulating RAS components.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the National Natural Scientific Foundation, China (81600547, 81170675 and 81200537) and the Beijing Municipal Science & Technology Commission (D131100004713002).