
Abstract
Objectives:
We conducted a meta-analysis of published studies on the angiotensin-converting enzyme (ACE) gene insertion/deletion (I/D) polymorphism associated with the risk of chronic obstructive pulmonary disease, as well as with pulmonary function and circulating angiotensin-converting enzyme changes.
Methods:
A literature search, quality assessment and data extraction were completed independently and in duplicate.
Results:
A total of 16 articles were meta-analysed, including 12 articles (2113 patients and 8786 controls) for chronic obstructive pulmonary disease risk and eight articles (11,664 subjects) for pulmonary and circulating phenotypes. In overall and subgroup analyses, no significance was noted between the I/D polymorphism and chronic obstructive pulmonary disease risk under all genetic models (P>0.05), without heterogeneity or publication bias. Carriers of II, ID and II plus ID genotypes had significantly lower levels of circulating angiotensin-converting enzyme than those with the DD genotype (weighted mean difference −13.35, −8.13 and −10.74 U/L, respectively, P<0.001). For forced expiratory volume in one second (FEV1)/forced vital capacity, carriers of the DD genotype had marginally lower levels than those with the DD genotype (weighted mean difference –1.66, P=0.034). Furthermore in the case of FEV1 of 50% or greater of predicted FEV1, FEV1 was marginally lower in ID genotype carriers than DD genotype carriers (weighted mean difference −3.50, P=0.056).
Conclusions:
Our meta-analytical findings demonstrated that the ACE gene I/D polymorphism was not associated with the risk of chronic obstructive pulmonary disease.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is characterised by persistent respiratory symptoms and airflow limitation, and it has ranked as the third killer in the world as per the latest statistics.1,2 Although several modifiable risk factors such as cigarette smoking and exposure to ambient air pollution have been identified, there is substantial evidence for the contribution of a heritable component to COPD susceptibility. For instance, a twin study estimated that inherited genetic susceptibility contributed to 60% of COPD risk. 3 Genome-wide association studies have succeeded in showing convincingly that COPD is a multifactorial polygenic disease.4,5 Despite tremendous advances gained in heritable insights, it still remains a challenge to unlock the genetic basis of COPD, because of apparent inconsistency from underpowered individual studies.
It is widely recognised that the gene encoding angiotensin-converting enzyme (ACE) is a COPD susceptibility candidate.6–9 Low ACE activity was identified to play a beneficial role in the development of COPD. The genomic sequence of the ACE gene is polymorphic, and thereof an insertion/deletion (I/D) polymorphism (rs4646994) in intron 16 is found to be highly associated with the circulating ACE level. 10 In particular, carriers of the DD genotype of this polymorphism had higher cellular and circulating levels of ACE, as well as power/sprint performance related to those with the II genotype. 11 It is thus reasonable to hypothesise that the ACE gene I/D polymorphism is a promising candidate locus in susceptibility to COPD. In fact, the association of the ACE gene I/D polymorphism with COPD risk has been extensively studied in the medical literature, while the findings are inconsistent and inconclusive.6–9 A comprehensive evaluation of this inconsistency is obviously needed for such a conclusion to be drawn more firmly. To test this hypothesis and yield more information, we conducted a systematic meta-analysis of published data on the ACE gene I/D polymorphism in association with COPD. In addition, we attempted to interrogate the association of this polymorphism with pulmonary function and circulating ACE changes.
Methods
The conduct of this meta-analysis conformed to the guidelines of the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement. 12 The PRISMA checklist and flow diagram are presented in Supplementary Table 1 and Supplementary Figure 1, respectively.
Search strategy
We searched major online public databases including Medline/PubMed, EMBASE (Excerpta Medica database) and Web of Science for studies published before 25 August 2017. We used heading search strategy with the terms: (‘ACE’ or ‘angiotensin-converting enzyme’) and (‘COPD’ or ‘chronic obstructive pulmonary disease’) and (‘polymorphism’ or ‘SNP’ or ‘variant’ or ‘mutation’). We also checked the reference lists of identified reports for the other potentially relevant studies. The search strategy was completed by two authors (Guodong Xu and Guohui Fan). A final reference list was determined after combining search results and removing duplicated hits.
Selection criteria
Articles were included if the genotype or allele counts of the ACE gene I/D polymorphism were provided in both COPD patients and healthy controls, and if COPD was diagnosed by a standard method, and if the I/D polymorphism was genotyped by a validated method. Only articles published in the English language were included in this meta-analysis. An article was excluded if it was published in forms of conference abstract, letter to the editor, case reports or case series, or if it lacked the control group.
As per the selection criteria formulated above, two authors (Guodong Xu and Guohui Fan) independently assessed the eligibility of each potential article for inclusion, and the results were compared and disagreement was solved by consensus.
Data extraction
The following data were extracted into a uniform design table from each eligible study: the first author’s surname, year of publication, country where the study was conducted, race of the study population, study design, diagnosis of COPD, source of controls, age, gender, body mass index, forced expiratory volume in one second (FEV1), FEV1/FVC (forced vital capacity), smoking status, pack years of smoking, the number of subjects with different genotypes of the ACE gene I/D polymorphism in COPD patients and controls. Data abstracted by the two authors were checked for coherence, and any divergence was resolved by resorting to original context until a consensus was reached.
Statistical analysis
Statistical analyses were conducted using STATA/SE software (version 11.2 for Windows; Stata Corp, College Station, TX, USA).
The primary outcome was the weighted odds ratio (OR) with 95% confidence interval (CI) for different genotypes and alleles of the ACE gene I/D polymorphism in patients with COPD compared with controls. The second outcome of this meta-analysis was the discrepancies of FEV1 and circulating ACE between different genotypes, as expressed as weighted mean difference (WMD) with 95% CI. The summary OR and WMD were calculated with a fixed effects model. Heterogeneity was tested using the inconsistency index (I2) statistic (ranging from 0.0% to 100.0%), which is defined as the percentage of observed between-study variability that is due to heterogeneity rather than chance. If the I2 exceeds 50.0%, it indicates statistically significant heterogeneity.
Funnel plots were used to assess the probability of publication bias and the small study effect. If funnel shape was asymmetric inverted, it might suggest an association between the pooled estimate and study size (publication bias or small study bias). The Egger’s test was used to assess funnel asymmetry objectively.
Univariate random-effects meta-regressions with log-transformed ORs were used to assess potential confounding of some risk factors, including age, gender and proportion of smokers.
Results
Qualifying studies
Our initial search of three public databases identified 42 articles published in the English language, and only 16 of them were eligible for analysis.6–9, 13–24 There were 12 articles (12 studies including 2113 patients and 8786 controls) that incorporated data on the risk of the ACE gene I/D polymorphism for COPD, and eight articles (14 studies including 11,664 subjects) that incorporated data on the changes of either FEV1 or FEV1/FEV or circulating ACE across the genotypes of this polymorphism.
Baseline characteristics
The baseline characteristics of eligible studies are presented in both Table 1 and Supplementary Table 2.
Baseline characteristics of eligible studies for the association of ACE gene I/D polymorphism with COPD risk.

ACE: angiotensin-converting enzyme; BMI: body mass index; FEV1: forced expiratory volume in one second; FVC: forced vital capacity; DD: deletion/deletion genotype; ID: insertion/deletion; II: insertion/insertion genotype; n.a.: not available.
I/D polymorphism and COPD risk: overall analysis
The association of the ACE gene I/D polymorphism with COPD risk was examined under the allelic, homozygous genotypic and dominant models, respectively. Figure 1 shows the corresponding forest plots. Overall, no hint of statistical significance was noted between this polymorphism and COPD risk under all genetic models (P>0.05). There was no evidence of heterogeneity between studies (I2=0.0%, 0.0% and 10.4%, respectively). In addition, there was a low likelihood of publication bias (Egger’s test P=0.811, 0.994 and 0.894, respectively). The Begg’s funnel plot in Figure 2 seemed symmetrical, and no study was reported to be missing.

Forest plots of the angiotensin-converting enzyme (ACE) gene insertion/deletion (I/D) polymorphism in association with chronic obstructive pulmonary disease under allelic (the upper), homozygous genotypic (the middle) and dominant (the lower) models.
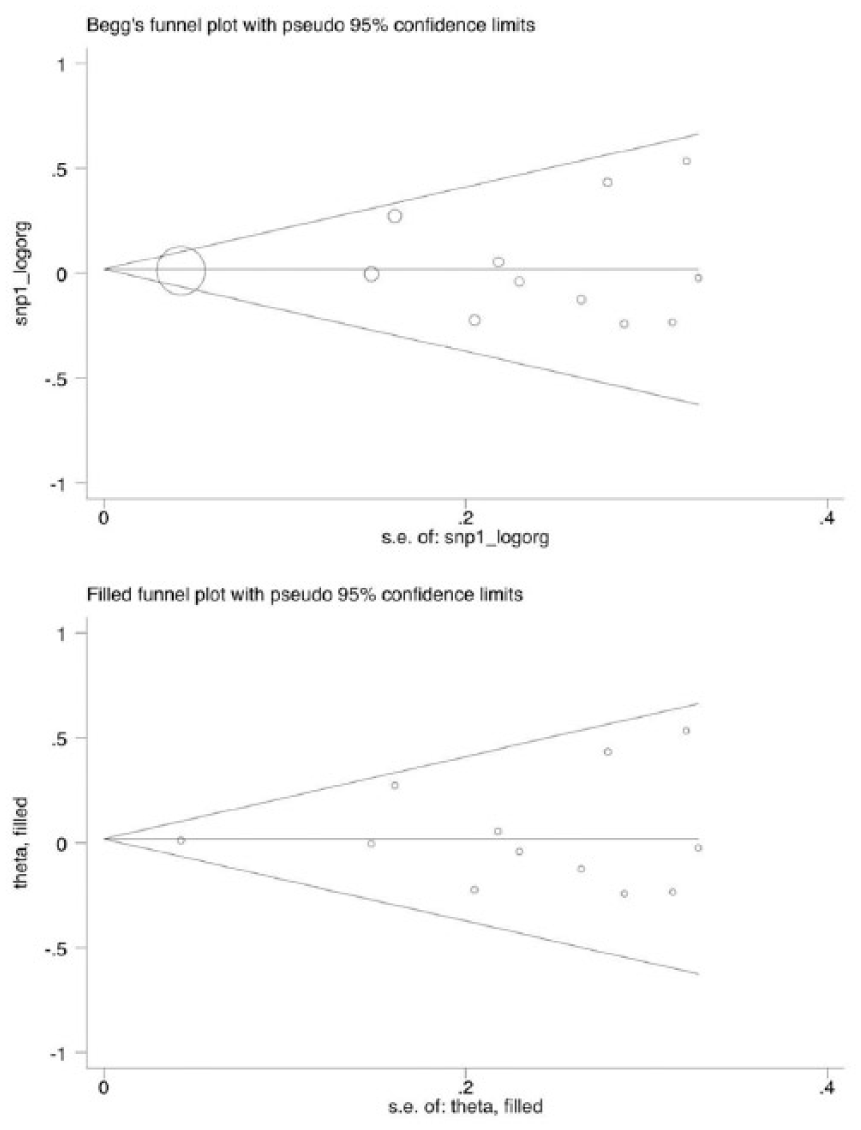
Begg’s and filled funnel plots of the angiotensin-converting enzyme (ACE) gene insertion/deletion (I/D) polymorphism in association with chronic obstruction pulmonary disease under the allelic model.
I/D polymorphism and COPD risk: subgroup analysis
Table 2 shows the subgroup analysis of the ACE gene I/D polymorphism in the prediction of COPD risk under the allelic, homozygous genotypic and dominant models, respectively. Factors under stratification included continent, race, study design, matched condition, COPD diagnosis, control source and sample size. Still, there was no detectable significance across all subgroups under all genetic models (P>0.05), and there was low evidence of heterogeneity for a majority of comparisons (I2<50%).
Subgroup analyses of ACE gene I/D polymorphisms in association with COPD.

ACE: angiotensin-converting enzyme; COPD: chronic obstructive pulmonary disease; OR: odds ratio; 95% CI: 95% confidence interval; I2: inconsistency index; I: insertion allele; D: deletion allele; DD: deletion/deletion genotype; ID: insertion/deletion; II: insertion/insertion genotype; II: insertion/insertion genotype; n.a.: not available.
I/D polymorphism and COPD risk: meta-regression analysis
Other sources of heterogeneity were explored through meta-regression analysis, including age, gender, smoking and pack years of smoking, and no factors exhibited a significant contribution (P>0.05).
I/D polymorphism and phenotypes: overall analysis
Table 3 shows the changes in FEV1, FEV1/FVC and circulating ACE across genotypes of the ACE gene I/D polymorphism. Carriers of the II genotype, ID genotype and the combination of II and ID genotypes had significantly lower levels of circulating ACE than those with the DD genotype (WMD −13.35, −8.13 and −10.74 U/L, respectively, all P<0.001). For FEV1/FVC, carriers of the ID genotype had a marginally lower level than those with the DD genotype (WMD −1.66, P=0.034). There was no evidence of heterogeneity and publication bias, as reflected by the I2 and Egger’s test, respectively.
Mean changes of FEV1, FEV1/FVC and circualting ACE between carriers of different genotypes of ACE gene I/D polymorphism.
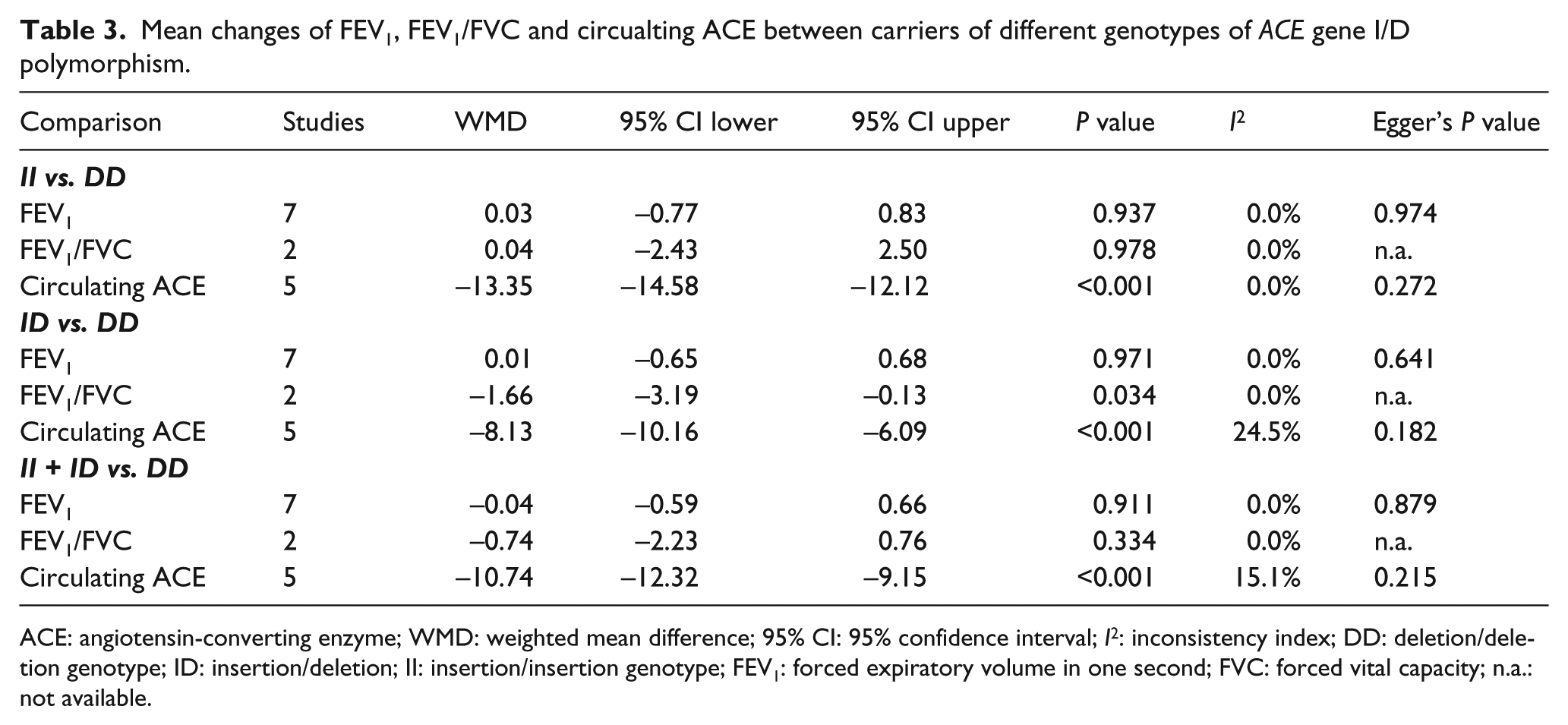
ACE: angiotensin-converting enzyme; WMD: weighted mean difference; 95% CI: 95% confidence interval; I2: inconsistency index; DD: deletion/deletion genotype; ID: insertion/deletion; II: insertion/insertion genotype; FEV1: forced expiratory volume in one second; FVC: forced vital capacity; n.a.: not available.
I/D polymorphism and phenotypes: subgroup analysis
Shown in Table 4 is the subgroup analysis of relevant phenotypes across genotypes of the ACE gene I/D polymorphism under various genetic models. According to the degree of FEV1/predicted FEV1 in DD genotype carriers, no significant association was found in COPD patients and controls, respectively. When FEV1 of 50% or greater predicted FEV1, FEV1 was marginally lower in the ID genotype carriers than the DD genotype carriers (WMD −1.73, P=0.056).
Subgroup analyses of FEV1/predicted FEV1 and circulating ACE between carriers of different genotypes of ACE gene I/D polymorphism.

ACE: angiotensin-converting enzyme; WMD: weighted mean difference; 95% CI: 95% confidence interval; DD: deletion/deletion genotype; ID: insertion/deletion; II: insertion/insertion genotype; FEV1: forced expiratory volume in one second; n.a.: not available.
In the case of circulating ACE, changes were consistently significant in both COPD patients and controls, and it was more obvious for the comparison of the II genotype with the DD genotype (WMD −14.03 U/L, P<0.001 in patients and WMD −13.12, P<0.001 in controls).
Discussion
This meta-analysis was designed to examine the association of the ACE gene I/D polymorphism with COPD risk. After a comprehensive analysis of 16 articles, our findings demonstrated that the ACE gene I/D polymorphism was not associated with the risk of COPD. In addition, we observed that the ID genotype carriers of this polymorphism tended to have reduced FEV1 (% predicted FEV1) in COPD patients with GOLD stages I–II. To our knowledge, this is the first meta-analytical report that has evaluated the association of the ACE gene I/D polymorphism with pulmonary function.
COPD is a complex multifactorial disease, and its development is thought to be largely under genetic control. A considerable number of genes and polymorphisms have been identified as susceptible candidates for COPD risk.25–27 The gene encoding ACE is one such candidate. ACE is a key element of the renin–angiotensin–aldosterone system, and its plasma levels are modulated by common defects of the gene. 28 In particular, the ACE gene I/D polymorphism has received great attention, as the D allele of this polymorphism correlated with a higher plasma ACE activity, the finding being further validated by our current analysis on different genetic models and diverse disease conditions. It has recently been increasingly recognised that the ACE gene I allele, interacting with the endothelial nitric oxide synthase (eNOS) gene 894G allele, can cause less vasoconstriction and increase vasodilation that may be advantageous in the improvement of COPD. 14 However, in the present meta-analysis, although the ACE gene I allele was associated with a slightly increased risk of COPD, there was no detectable significance under different genetic models of inheritance, even in various subgroups by many study characteristics. This association was robust and solid, as this meta-analysis is currently based on the largest number of eligible studies relative to previously published meta-analyses,29–31 and importantly our findings remain unperturbed by between-study heterogeneity and publication bias. On the other hand, it is widely recognised that the increased risk attributable to a single allele is small in genetically susceptible individuals, and such a small effect may also be exacerbated by locus heterogeneity across different ethnic/racial groups.6,8,18 Wide coverage of the genetic variability of the ACE gene and other COPD susceptibility genes is required to decipher the genetic basis of COPD.
In addition, our findings also dropped a hint of a probable contribution of the ACE gene I/D polymorphism to pulmonary function, as carriers of the ID genotype had a significantly lower level of FEV1/FVC than carriers of the DD genotype. Moreover, the ID genotype was associated with reduced FEV1 in COPD patients with GOLD stages I–II, while this reduction was non-significant in patients with GOLD stages III–IV. In view of limited studies in subgroup analysis, our findings gave rise to speculation that the ACE gene I/D polymorphism may serve as a predictive marker for the early development of COPD. We agree that further validation of our findings in large, well-designed studies is necessary.
Our analyses have several limitations. The first limitation was that our findings were based on cross-sectional observational data, which precluded comment on causality between circulating ACE and COPD risk. The second limitation lay in the analysis of only one polymorphism in the ACE gene. The third limitation was that we only retrieved articles published in the English language, as it is estimated that the exclusion of grey literature from meta-analysis may result in an overestimate of an association impact by an average of 12%. 32 The fourth limitation was although our analyses indicated low probabilities of heterogeneity and publication bias, we cannot fully exclude their potential confounding impact. The fifth limitation was that residual confounding due to unadjusted divergence in baseline characteristics of eligible studies cannot be completely assessed or ruled out using study-level data.
Taken together, our meta-analytical findings demonstrated that the ACE gene I/D polymorphism was not associated with the risk of COPD. Large-scale validation is necessary to confirm our findings. For practical reasons, a single well-designed study is warranted to interrogate gene–gene and gene–environment interactions further on the association of ACE gene multiple polymorphisms with COPD risk and related pulmonary phenotypes.
Supplemental Material
jraas-2018-0006-File004_Supplementary – Supplemental material for Association of angiotensin-converting enzyme gene I/D polymorphism with chronic obstructive pulmonary disease: a meta-analysis
Supplemental material, jraas-2018-0006-File004_Supplementary for Association of angiotensin-converting enzyme gene I/D polymorphism with chronic obstructive pulmonary disease: a meta-analysis by Guodong Xu, Guohui Fan, Yingtong Sun, Lili Yu, Sinan Wu and Wenquan Niu in Journal of the Renin-Angiotensin-Aldosterone System
Footnotes
Author contribution
WN planned and designed the study; GX and WN searched the literature, selected articles and abstracted data; GX, GF, YS and LY conducted the data preparation, quality control and data analyses; WN, GX and SW wrote and revised the manuscript.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.