
Abstract
Background:
Preeclampsia (PE) is a pregnancy-associated hypertensive disorder and a leading cause of maternal and neonatal morbidity and mortality. While its pathogenesis remains ill defined, several candidate genes for PE have been identified, but results remain inconclusive. We investigated the association of the angiotensinogen (AGT) gene variants M235T and T174M with PE, and we analyzed the contribution of both variants to the severity of PE.
Methods:
This case-control study enrolled 550 Tunisian pregnant women: 272 with PE, of whom 147 presented with mild, and 125 with severe PE, along with 278 unrelated age- and ethnically matched control women. AGT genotyping was performed by polymerase chain reaction-restriction fragment length polymorphism.
Results:
Significantly higher M235T minor allele frequency (MAF) was associated with increased risk of PE (p < 0.001). Decreased frequency of heterozygous T174M genotype carriers were found in control women (p = 0.015), suggesting a protective effect of this genotype (odds ratio (95% confidence interval) = 0.51 (0.29–0.89)). Two-locus haplotype analysis demonstrated MM and TT haplotypes to be negatively and positively associated with PE, respectively. MAF of M253T, but not T174M, was higher in the severe PE group, and carrying M235T or T174M minor allele was associated with increased body mass index (p < 0.001) among unselected PE women.
Conclusions:
AGT M235T and T174M variants contribute to an increased risk of developing PE, and for M235T to PE severity.
Introduction
Preeclampsia (PE) is a significant pregnancy complication characterized by hypertension and proteinuria, 1 affecting 2%–8% of all pregnancies worldwide. 2 PE is defined as systolic blood pressure (SBP) of ≥140 mmHg, and/or diastolic blood pressure (DBP) of ≥90 mmHg on at least two occasions separated by six hours, and following 20 weeks of amenorrhea combined with proteinuria. 3 PE is severe if SBP or DBP exceed 160 mmHg or 110 mmHg usually with abnormal proteinuria (at least 5 g/24 hours). 3 PE is multifactorial and is accompanied by maternal multi-organ dysfunction, fetal complications, and growth restriction, 4 and is considered a disease of theories. 5 The progression of PE is related to several factors, including abnormal placental development, trophoblast invasion, and remodeling of uterine spiral arteries, 6 along with dysregulated immunity, 7 placental ischemia, 8 oxidative stress 9 and thrombosis. 10
The renin-angiotensin-aldosterone (RAAS) system regulates BP, vascular tone, electrolyte balance and fluid homeostasis. 11 RAAS effects result from cleavage of angiotensinogen (AGT) by renin to angiotensin I, 12 which subsequently cleaves by angiotensin-converting enzyme (ACE) to (biologically active) angiotensin II (Ang II). 13 Ang II stimulates aldosterone synthesis, resulting in water retention and salt reabsorption in the renal tubes and systemic arteriolar vasoconstriction. 14 In addition, accumulating evidence highlights the contribution of extra-renal RAAS (brain, heart, ovary, placenta) in carrying out similar effects as renal RAAS.14,15 In particular, decidual spiral arteries show expression of AGT, renin, ACE and Ang II type 1 (AT1) receptors.16,17
During normal pregnancy, there is an increase in maternal blood volume, a decrease in total resistance and elevated plasma concentrations of renin, Ang II and aldosterone.16,18,19 This increase in the RAAS components, due to increased estrogen levels, mediates the expansion of extracellular and blood volumes typical for the normal adaptive mechanism of pregnancy. 15 In the placenta, all components of the RAAS are distributed and trophoblasts cells are rich in AT1 receptors and thus are responsive to the changes in Ang II concentrations. 18 Furthermore, it has also been shown that Ang II and aldosterone have a crucial role in placental development, and thus fetal perfusion. 20
In PE, the intravascular blood volume and cardiac output are reduced, while the total peripheral resistance is increased and the components of circulating RAAS are downregulated, including plasma renin activity, plasma Ang I, Ang II, Ang-(1–7) and aldosterone.19–21 PE is a multifactorial disease, and modifiable and non-modifiable risk factors contribute to its physiopathology, the latter including genetic susceptibility factors. 22 The AGT gene, located on chromosome 1 (1q42–43), encodes the precursor of all angiotensin peptides, and has been described as a candidate gene of hypertension 23 and PE.24,25 The AGT gene is polymorphic, and 1249 variants distributed between near gene (154), untranslated regions (76), exons (355) and intron (664) regions have been reported, of which M235T (rs699) and T174M (rs4762) have been the most investigated. These variants were associated with a rise in serum AGT levels in patients with essential hypertension, 26 leading to increased SBP and DBP, 27 and abnormal remodeling of the uterine spiral arteries, an early cause of PE. 28 Here we investigate the association of AGT M235T and T174M variants with PE among (North African) Tunisian Arab women, and correlate the impact of carrying the minor allele of these variants on the severity of PE.
Materials and methods
Study participants
From 1 May 2012, to 31 July 2014, 345 women with PE (mean age 31.3 ± 7.0 years), and 323 normotensive control women with normal pregnancy (mean age 30.5 ± 5.8 years) were recruited from the outpatient Obstetrics & Gynecology service of Fattouma Bourguiba University Hospital (Monastir, Central Tunisia), Farhat Hached University Hospital (Sousse, Central Tunisia), Taher Sfar University Hospital (Mahdia, Eastern Tunisia) and Gafsa Regional Hospital (Gafsa, Southern Tunisia). Inclusion criteria for cases were PE during natural pregnancy, which was defined as gravidic hypertension, and assessed as SBP >140 mmHg, DBP >90 mmHg, and/or rise in SBP >30 mm, or DBP >15 mmHg on at least two occasions six hours apart, following 20 weeks of gestation, and with evidence of marked proteinuria (> 300 mg/24 hours), or >2+ proteinuria as determined by the dipstick method.
Control women with no known personal or family history of PE were recruited from the same geographical area. Inclusion criteria for controls were uncomplicated pregnancy after 20 weeks of gestation, and negative proteinuria. Exclusion criteria for PE cases and control women were arterial hypertension, gestational hypertension, hemolysis, elevated liver enzymes, and low platelets syndrome and non-Arab origin. The investigation was approved by local ethics committees, and all participants were asked for, and provided written informed consent. Demographic data of participants and clinical characteristics of the patients are shown in Table 1.
Characteristics of study participants a .

Study participants comprised 272 PE cases and 278 control women.
Mean ± SD.
Number (percentage of individuals within group or subgroup).
Obesity defined by BMI greater than 30.
p < 0.05 (controls vs. All PE cases), fp < 0.05 (mild vs. severe PE cases), Student’s t-test (two tailed) for continuous variables, Pearson’s chi-square test for categorical variables.
PE: preeclampsia; BMI: body mass index; BP: blood pressure.
AGT genotyping
Peripheral venous blood samples were collected in ethylenediaminetetraacetic acid-containing vacutainer tubes. Plasma was recovered following centrifugation at 3000 revolutions per minute for 15 minutes, and stored in small aliquots at −20°C pending analysis. Genomic DNA was extracted by the salting-out method. 29 AGT genotyping was performed by polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP). Briefly, PCR was performed in a final-volume 15 µl containing genomic DNA (50 ng), 0.2 μM of forward and reverse primers, 0.2 mM deoxynucleotide mix (Invitrogen, Carlsbad, CA, USA) and 1 U GoTaqDNA polymerase (Promega, Madison, WI, USA). For M235T, the following primers were used: forward, 5’-CAgggTgCTgTC CAC ACT ggA CCC C-3’, and reverse, 5’- CCg TTT gTgCAgggCCTggCT CTC T-3’. For T174M, the following primers were used: forward, 5’-gATgCg CAC AAggTC CTg-3’, and reverse, 5’, CAg ggTgCTgTC CAC ACT ggCTCg C-3’. The 165 base pair (bp) M235T and 303 bp T174M amplicons were digested with Thermus thermophilus strain 111 Tth111I at 65°C or Nocardia corallina (NcoI) at 37°C, respectively (New England Biolabs, Ipswich, MA, USA). Digested fragments were separated by electrophoresis on 3% agarose gel, and yielded 141 bp + 24 bp for M235T, and 211 bp + 92 bp for T174M, respectively.
Statistical analysis
Statistics were performed by SPSS version 20 (SPSS, Chicago, IL, USA). Continuous data are presented as mean ± SD, and analyzed by Student t-test, while categorical data are presented as frequencies, and tested by χ2 test. Allele frequencies were calculated by the gene-counting method, and each polymorphism was tested for the Hardy–Weinberg equilibrium using Haploview 4.2 (www.broadinstitute.org/haploview). Calculation of the power for detecting association between AGT variants and PE was performed using the Genetic Power Calculator (http://pngu.mgh.harvard.edu/~purcell/cgi-bin/cc2k.cgi). The parameters used were number of PE cases and control women, genotypic relative risk for heterozygote (1/2) and homozygous minor allele (2/2), and minor allele frequency (MAF) for PE cases and control women for the two tested AGT single-nucleotide polymorphisms (SNPs), and assuming a 3.5% prevalence of PE. Assuming these parameters, the overall power (53.4%) was calculated as the average power of the two tested SNPs. Logistic regression analysis was performed to build nested prediction models of PE. The corresponding crude odds ratio (OR) and 95% confidence interval (95% CI) were calculated. For all analyses, statistical significance was considered at p < 0.05.
Results
Characteristics of study participants
Baseline and clinical characteristics of study participants are described in Table 1. The total number of study women was 550. First we compared the clinical characteristics of all PE cases (N = 272) to control pregnant women (N = 278). After that, we subdivided the PE cases into two groups (mild PE and severe PE form) and compared the severe PE (N = 147) to the mild PE form (N = 125).
While women with PE were matched to controls according to age and Cesarean section delivery, PE cases had a higher mean body mass index (BMI) than the control group (p < 0.001). Women with PE had significantly lower gestational age at blood sampling, and lower newborn weight. Accordingly BMI, regional origin, newborn weight, gestation age, and pregnancy status were selected as the covariates that were controlled for in subsequent analysis. Apart from SBP and DBP readings (p < 0.001), the characteristics of severe PE cases were compared to those of mild PE cases.
Association of AGT SNPs with PE
The AGT SNPs investigated were selected based on their MAF of >5% in Tunisians, and association with hypertension and adverse pregnancy complications, including PE. The allele distributions of the tested AGT SNPs between PE cases and control women are summarized in Table 2. The genotype distribution of M235T (p = 0.46) and T174M (p = 1.00) were in Hardy–Weinberg equilibrium among study women (Table 2). MAF of M235T (p = 5.0 × 10−4), but not T174M (p = 0.08), were significantly higher among PE cases than control women, which persisted after correcting for multiple comparisons. This translated into high risk of PE associated with M235T (OR (95% CI) = 1.63 (1.24–2.15)), but not T174M.
Distribution of AGT alleles in PE cases and control women.

Location on chromosome based on the Single Nucleotide Polymorphism database build 125.
aOR: adjusted OR, adjusted for body mass index, gestation, and baby weight.
AGT: angiotensinogen; PE: preeclampsia; SNP: single-nucleotide polymorphism; MAF: minor allele frequency; T: threonine; M: methionine; HWE: Hardy–Weinberg equilibrium; CI: confidence interval.
AGT genotypes
A significant difference in the distribution of M235T (p = 0.003) and T174M (p = 0.015) genotypes was seen between PE cases and healthy controls (Table 3). Taking a homozygous wild-type genotype as a reference (OR = 1.00), increased PE risk was seen with M235T, while T174M was associated with decreased risk of PE. This persisted after controlling for BMI, gestation age, and baby weight (Table 3). Stratification of PE cases into mild and severe PE (Table 4) resulted in the loss of M235T (p = 0.053) and T174M (p = 0.518) effects, demonstrating that neither variant was associated with altered PE severity (Table 4). However, these findings need to be evaluated with caution, given the relatively low power associated with M235T (76.9%) and T174M (29.9%), resulting in an overall power of 53.4%. Carrying either M235T or T174M minor alleles (1/2 + 2/2) was associated with increased BMI (p < 0.001) among unselected PE patients. On the other hand, carrying M235T and T174M minor alleles was not linked with BMI changes among subgroups of PE cases.
Association of AGT genotypes with PE.

Number (frequency).
aOR: adjusted OR, adjusted for body mass index, gestation, and baby weight.
AGT: angiotensinogen; PE: preeclampsia; SNP: single-nucleotide polymorphism; T: threonine; M: methionine; OR: odds ratio; CI: confidence interval.
Distribution of AGT alleles in mild type PE and severe PE.

Number (frequency),
aOR: adjusted OR, adjusted for body mass index, gestation, and baby weight.
AGT: angiotensinogen; PE: preeclampsia; SNP: single-nucleotide polymorphism; MAF: minor allele frequency; HWE: Hardy–Weinberg equilibrium; T: threonine; M: methionine; OR: odds ratio; CI: confidence interval.
Haploview analysis
Results from Table 5 demonstrated enrichment of threonine threonine (TT) and reduced frequency of methionine (M)T haplotypes among PE cases compared with control women, thereby assigning PE susceptibility and protective nature to these haplotypes, respectively. The negative association of MT haplotype (corrected p (pc) = 0.02) and positive association of TT haplotype (pc = 7.0 × 10−4) with PE persisted after correcting for multiple comparisons. On the other hand, none of the four two-locus haplotypes was associated with severity of PE, even before correcting for multiple comparisons (Table 5). This was evidenced by the comparable haplotype frequencies among severe versu mild PE cases.
Haplotype frequencies across AGT SNPs a in PE cases and control women.
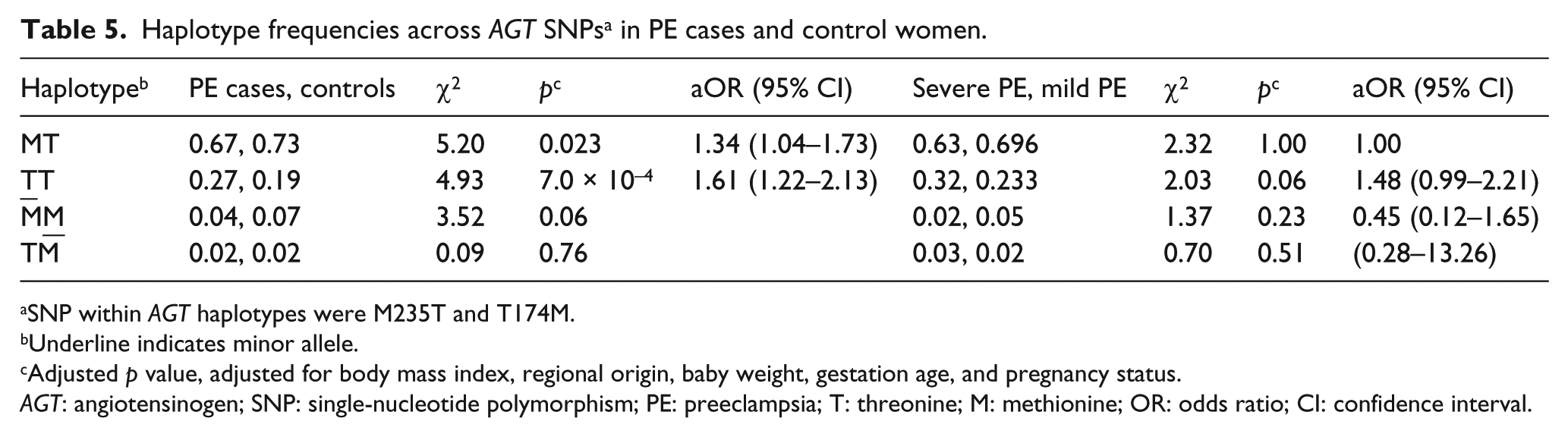
SNP within AGT haplotypes were M235T and T174M.
Underline indicates minor allele.
Adjusted p value, adjusted for body mass index, regional origin, baby weight, gestation age, and pregnancy status.
AGT: angiotensinogen; SNP: single-nucleotide polymorphism; PE: preeclampsia; T: threonine; M: methionine; OR: odds ratio; CI: confidence interval.
Discussion
Insofar as RAAS stimulation and increased levels of its components regulate physiologic hypervolemia during normal pregnancy, decreased RAAS activity resulting in vascular resistance was seen in women with PE. AGT, the precursor of angiotensin peptides, especially (vasoactive) Ang II, is key to vascular remodeling.30,31 Genetic association studies demonstrated a strong link between variation in the AGT gene and its gene expression, and altered plasma AGT levels. 32 AGT M235T and T174M were previously associated with altered susceptibility to vascular diseases, including hypertension, atherosclerosis and PE. 33 This is the first study that evaluates the contribution of these common SNPs to PE in (North African) Tunisian women.
The main finding of this study is that the M235T minor allele increases the risk of PE by almost three-fold. Haplotype analyses confirmed this association, as the 235T-T174 haplotype was positively associated with PE, which remained significant after controlling for potentially confounding variables. While T174M was not significantly associated with PE at the allele level, in partial agreement with two recent meta-analyses that reported that T174M is not associated with PE,34,35 a protective effect of T174M emerged when genotypes were examined. The association of M235T with PE was first reported for Caucasians in 1993, 36 and an earlier meta-analysis demonstrated significant association of M235T with PE, under dominant and recessive genetic models. 37 An ethnic contribution to M235T was suggested, exemplified by a meta-analysis involving 32 studies that reported an association of M235T with higher PE risk in Caucasians and Mongolians, but not in Black South Africans and African Americans. 34 Another meta-analysis involving 22 studies reported evidence of an association of M235T with PE in Caucasians, but not in Indian, Black South African, African American, and Asian populations. 38
Carrying AGT M235T and T174M minor alleles positively associated with BMI among unselected PE patients suggests gene-environment interaction in determining PE risk. A recent meta-analysis reported that increased BMI is associated with heightened risk of PE, suggesting that obesity constitutes a predictor of PE development. 39 Our results are in agreement with an earlier Japanese study that reported a positive association of M235T with visceral obesity in obese women, 40 and with morbid obesity in patients with type 2 diabetes mellitus (T2DM). 41 Obesity and hypertension are two parameters of metabolic syndrome; our result is favorable for the hypothesis that PE is considered a metabolic syndrome. In the Tunisian population, M235T has been investigated to be associated with atherosclerotic stroke 42 and T2DM, 43 and to affect the susceptibility to nephropathy in T2DM patients, 44 increased risk of heart failure and death. 45
We examined the prognostic role of M235T and T174M as determinants of the severity of PE by analyzing the effects of carrying the minor allele in mild versus severe PE women. There was a trend toward increased risk of severe PE in the presence of M235T, but it did not reach statistical significance (p = 0.053); no significance was noted in the case of T174M between both groups. Parallel studies that examined the contribution of M235T to PE severity did not find a significant association.46–48 A recent Iranian study reported that carrying the M235T minor allele with the −217A allele increased the risk of severe PE 2.23-fold. 49 Concerning AGT T174M, our study is the first to investigate the association of this variant with PE severity.
Mechanistically, the contribution of AGT M235T to PE was suggested earlier to be exacted at the level of local elevation of Ang II, and hence abnormal physiologic remodeling of the uterine spiral arteries. 28 Higher plasma AGT levels were seen in PE women carrying 235T/T or 235M/T compared to 235M/M genotypes, 36 which was associated with a parallel increase in Ang II production, and hence vascular tone and vascular hypertrophy. 50 When combined with AGT promoter –6G>A, carrying the AGT M235T minor allele was associated with augmented AGT expression. 32 Moreover, placental abruption because of defective spiral artery remodeling was associated with AGT M23T minor allele in 63% of women with PE, and 60% in intrauterine growth restriction compared with normal pregnancy.46–51 On the other hand, MAF of AGT T174M is lower in Tunisians and European, Asian, and African American populations, but was found to be at lower frequencies in PE cases than in control pregnant women. While no study addressed the impact of AGT T174M genotypes on plasma AGT levels in PE, it was shown that plasma AGT levels were significantly lower in women without a medical history of essential hypertension who were carriers of 174M/M or 174T/M rather than 174M/M genotypes. 52
The pathogenesis of PE results from the altered expression of angiogenic factors, including placental growth factor (PIGF), 53 and anti-angiogenic antagonists, like soluble fms-like tyrosine (sFlt1), 54 both of which are implicated in regulating placental vasculogenesis. 55 This carries the potential to offer major advances in the diagnosis and management of this obstetric complication even in early gestation.53,56,57 A recent study of a Chinese population showed that AGT M235T may contribute to altered PIGF and sFlt1 concentrations, with plasma sFlt1 levels higher and PIGF lower in PE patients carrying 235T/T compared with 235M/M genotypes. 58
To the best of our knowledge, this is the first study in North Africa that investigates the association of these SNPs with PE and its severity. The strengths of our study are the homogeneity of the population tested, which minimizes the problems of differences in genetic background inherent in gene-association studies, and that potential covariates were controlled for. Some potential limitations should be considered in our study. Our study population has a relatively small sample size in terms of PE manifestation, in particular when PE patient subgroups were analyzed separately, which affected overall study power. Further studies with larger samples are necessary to augment our findings. Another limitation is that we have used two missense SNPs located in the coding region, but we did not investigate polymorphisms –6G>A and –20A>A in the promoter region that are in linkage disequilibrium with AGT M235T and T174M, respectively. In conclusion, AGT M235T and T174M contribute to an increased risk of developing PE in Tunisians and to BMI excess in women with PE, and AGT M235T may predispose patients to severe PE.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.