
Abstract
Introduction:
Preeclampsia is a life-threatening disorder of pregnancy. The pathogenic mechanisms of preeclampsia remain uncertain. The aim of this study is to investigate the relation between urinary angiotensinogen (UAGT) levels, an indicator of local renin–angiotensin system (RAS) activity in the kidney, and blood pressure and urinary protein excretion in preeclampsia.
Materials and methods:
For this study, 90 women aged between 20–39 years were recruited. Spot urine samples were collected to measure urinary angiotensinogen/creatinine ratio (UAGT/UCre). Log(UAGT/UCre) was compared in pregnancies with and without preeclampsia and non-pregnant controls. Factors affecting log(UAGT/UCre) in pregnancies were also investigated.
Results:
In all pregnancies log(UAGT/UCre) levels were significantly higher than in non-pregnant controls (0.58±0.19 vs. 0.33±0.14, respectively, p=0.002). However, log(UAGT/UCre) levels in pregnancies with preeclampsia were slightly lower than in normal pregnancies (0.52±0.18 vs. 0.64±0.19, respectively, p=0.012). Log(UAGT/UCre) levels were correlated positively with blood pressure and proteinuria in pregnancies with preeclampsia. However, log(UAGT/UCre) levels were not correlated with age, height, body weight, gestational age, body mass index, and serum creatinine.
Conclusion:
This study showed that elevated local RAS activity in kidney was correlated with high blood pressure and proteinuria in preeclampsia. Local RAS activation in the kidneys may be one of the contributing factors in the development of preeclampsia.
Introduction
Preeclampsia is a life-threatening disorder of pregnancy that affects approximately 7% of pregnancies; it is characterized by hypertension and proteinuria, resulting in maternal and neonatal morbidity and mortality. 1 To date the underlying pathogenic mechanisms of preeclampsia remain uncertain. However, many clinical trials suggest alterations in renin–angiotensin system (RAS) components in the pathogenesis of preeclampsia.2-4 The regulation of the RAS in preeclampsia differs from that in healthy pregnancies. Although most circulating RAS components increase in an uncomplicated pregnancy, preeclamptic women have lower circulating levels of RAS components than normotensive pregnant women. 3 Preeclamptic women, however, show increased sensitivity to angiotensin II (ANG II) in their vascular system. 5 Recently emerging evidence suggests that local formation is of major significance in the regulation of RAS in many organs and tissues. Although every organ system in the body has elements of the RAS, the kidney is unique in having every component of the RAS, with compartmentalization in the tubular and interstitial networks as well as intracellular accumulation. 6 There is substantial evidence that ANG II present in renal tissues is generated locally from angiotensinogen (AGT) delivered to the kidney as well as from AGT locally produced by proximal tubule cells. However, most of the systemic AGT cannot pass through the glomerular basement membrane of the nephrons because of its high molecular weight. Since AGT is not filtered at the glomerulus, it is suggested that AGT that appears in the urine is of renal tubular origin. 7 Kobori et al. showed a positive correlation between urinary AGT and intrarenal ANG II levels in ANG II-dependent hypertensive rats. 8 Similarly, urinary AGT was significantly correlated with intrarenal AGT gene expression and ANG II immunoreactivity in patients with normotensive IgA nephropathy. 9 Recent evidence has also revealed that inappropriate activation of intrarenal RAS is an important contributor to the pathogenesis of hypertension and renal injury.10-12 We hypothesized that local RAS activation in the kidneys may have a role in the pathophysiological mechanisms for development of preeclampsia. Therefore in this study, we aimed to investigate the relationship between urinary AGT levels and proteinuria and blood pressure measurements in preeclamptic pregnancies.
Methods
Patients
In total, 90 women aged between 20–39 years (30 women with normotensive pregnancy, 30 women with newly diagnosed preeclampsia and 30 non-pregnant control female subjects) were recruited for the study. Power analysis showed that a total sample size of 90 patients gives a 90% probability of detecting a difference significant at the 15% level between angiotensinogen levels in study groups. Preeclampsia was defined as an office blood pressure of 140/90 mmHg or greater on two occasions more than 2 h apart, with a urinary protein concentration >300 mg/l collected at random or >300 mg/24 h after 20 weeks of gestation in a woman who was normotensive before pregnancy without pre-existing cardiovascular or renal disease. Mean gestational age of pregnancies with preeclampsia was 35.3±3.5 months. The 30 normotensive pregnant women were selected from pregnant women followed at our centers, according to inclusion criteria (gestation weeks greater than 20 weeks); and exclusion criteria ((i) history of preeclampsia in previous pregnancies; (ii) history of hypertension and kidney disease; (iii) history of cardiovascular diseases). Mean gestational age of women with normal pregnancies was 35.0±3.4 months. The control group, which consisted of normotensive non-pregnant women with similar ages and no history of preeclampsia or hypertension and/or kidney diseases and/or cardiovascular diseases, was recruited at the same time. The demographics (age, parity, history of hypertension and preeclampsia, gestation weeks) of all of the women were recorded at initiation of the study. Serum creatinine, albumin, and uric acid levels of women were obtained from medical records. The study protocol was approved by the Local Ethical Committees and written informed consent was obtained from each subject.
Measurements
Morning spot urine samples were collected from all women to measure urinary AGT, creatinine, and albumin levels. Collected 24 h urine was used for quantitation of daily urinary protein excretion. Urinary concentration of AGT was measured from 10 ml of urine sample with human AGT-ELISA kits (Uscn Life Science Inc., Wuhan, China) by a technician who was blinded to the patients’ data. All samples were measured in duplicate and the average value of two measurements was recorded for each patient. The intra-assay coefficient of variation (CV) was <10%, and inter-assay CV was <12%. The detection range of the assay was 0.312–20 ng/ml. The minimum detectable dose of the kit was typically less than 0.102 ng/ml. The urinary creatinine level was measured with Jaffe’s method. Urinary AGT/creatinine ratios (UAGT/UCre) were calculated and logarithmically transformed (log [UAGT/UCre]) to make normal distribution. Log(UAGT/UCre) levels were used for further analyses in this study. Urinary albumin and urinary protein levels were quantified with nephelometry (Immage 800; Beckman Coulter, USA) and an automated turbidimetric method using benzalkonium chloride, respectively, as routinely used in our practice. Systolic and diastolic blood pressure was measured three consecutive times using a sphygmomanometer after the patients had rested for at least 15 min; the mean of the lowest two readings was recorded. Blood pressure was measured three times a day in a supine position, and the means of values obtained 3 days before the initiation of anti-hypertensive treatment were recorded.
Statistical analysis
The SPSS program version 15.0 (SPSS Inc., Chicago, IL, USA) was used for analysis. Results are presented as means ± SDs and median [interquartile ranges] values. Kolmogorov–Smirnov and Levene’s tests were used for distribution and variance homogeneity. The parameters with a normal distribution were compared between groups by parametric tests such as the ANOVA test and t-tests. Parameters with non-normal distribution were compared between groups by non-parameteric tests such as Kruskall–Wallis and Mann–Whitney U test. Similarly, correlation analyses between parameters were made by Pearson’s or Spearman’s correlation tests depending on the distribution of data; a p-value of <0.05 was considered statistically significant.
Results
The demographic and laboratory data of the study population are presented in Table 1. There were no significant differences in demographic characteristics between non-pregnant controls, normotensive pregnancies and pregnancies with preeclampsia. Mean serum uric acid levels, serum creatinine, blood urea nitrogen and blood pressure measurements were lower in normal pregnancies than non-pregnant controls (Table 1). In pregnancies with preeclampsia, blood pressure levels, serum uric acid levels, and proteinuria/24 h were higher than in non-pregnant controls and normal pregnancies (Table 1).
The demographic data and laboratory parameters in study groups.
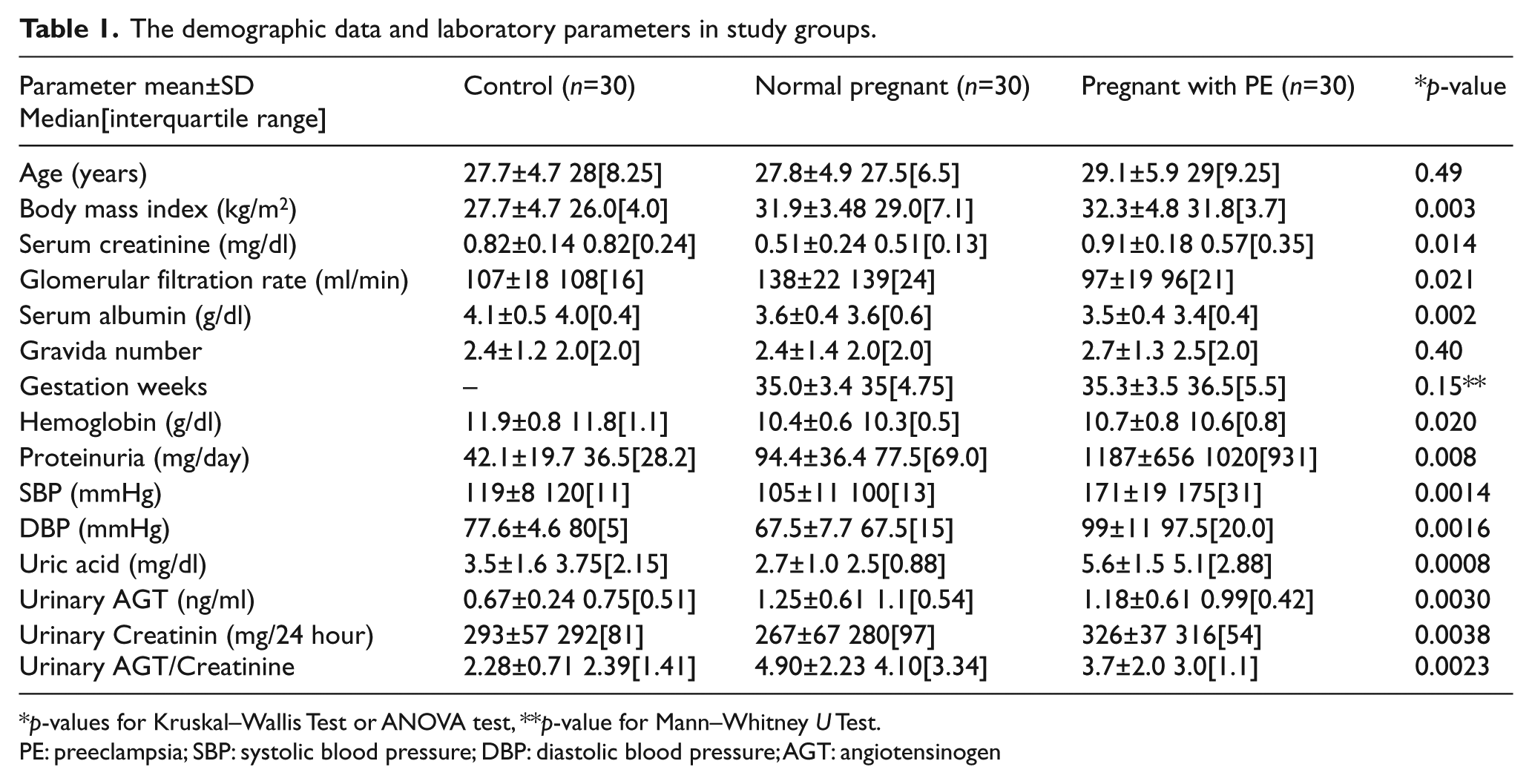
p-values for Kruskal–Wallis Test or ANOVA test, **p-value for Mann–Whitney U Test.
PE: preeclampsia; SBP: systolic blood pressure; DBP: diastolic blood pressure; AGT: angiotensinogen
In all pregnancies; log (UAGT/UCre) levels were significantly higher than in non-pregnant controls (0.58±0.19 vs. 0.33±0.14, respectively, p=0.002). However, log (UAGT/UCre) levels in pregnancies with preeclampsia were slightly lower than in normal pregnancies (0.52±0.18 vs. 0.64±0.19, respectively, p=0.012) (Figure 1).

Comparison of urinary angiotensinogen/creatinine levels (log[UAGT/UCRE]) between the study groups (p=0.0019).
Correlation analysis in pregnancies with preeclampsia showed that log (UAGT/UCre) levels were significantly correlated positively with systolic and diastolic blood pressure levels (p=0.005, r=0.49; p=0.003, r=0.53 respectively) (Figures 2 and 3). In addition, log (UAGT/UCre) levels were also associated with 24 h urinary protein excretion (r=0.42, p=0.001) in pregnancies with preeclampsia (Figure 4). However, log (UAGT/UCre) levels were not correlated with age, gestational age, body mass index, serum creatinine, blood urea nitrogen and uric acid levels.

Correlation between urinary angiotensinogen/creatinine levels (log[UAGT/UCre]) and systolic blood pressures in pregnancies with preeclampsia (p=0.005).

Correlation between urinary angiotensinogen/creatinine levels (log [UAGT/UCre]) and diastolic blood pressures in pregnancies with preeclampsia (p=0.003).
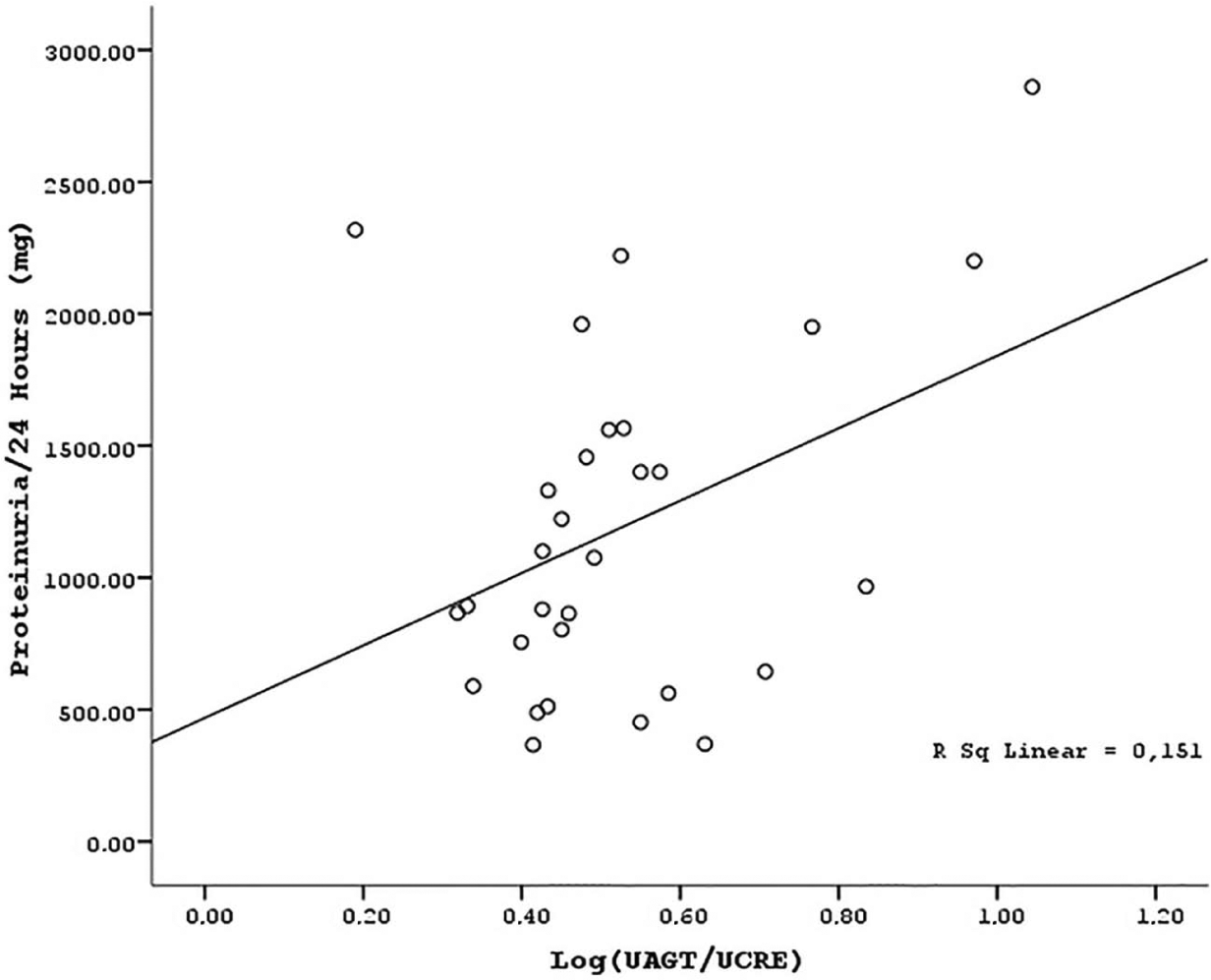
Correlation between urinary angiotensinogen/creatinine levels (log [UAGT/UCre]) and proteinuria (24 h) in pregnancies with preeclampsia (p=0.001).
Discussion
This study showed that local RAS activation in kidney reflected by urinary AGT levels is increased in pregnant women. In addition, urinary AGT levels seem to be associated with systolic and diastolic blood pressure levels and urinary protein excretion in pregnant women with preeclampsia.
Previous trials demonstrated that circulating AGT increases in an uncomplicated pregnancy, possibly resulting from an increase in estrogen levels which stimulates synthesis of AGT by the liver; however, local RAS activation was not well studied in pregnancies.2,3,13 An experimental histological study demonstrated that there is a significant increase in local kidney tissue AGT levels at mid-gestation. 14 To the best of our knowledge, our study was the first clinical study that demonstrated a significant increase in urinary AGT excretion in pregnancies. Although there are some hypothetical suggestions to explain the rise of AGT levels in kidney tissue, the mechanism is unclear. Our findings also showed that the augmentation of urinary AGT levels in women with uncomplicated pregnancy was not associated with a rise of systolic or diastolic blood pressure levels. This finding suggests that normal pregnant women are actually refractory to the local RAS component’s vasopressor effects. Previous studies in uncomplicated pregnancies showed that the presence of increased levels of progesterone and prostacyclins can decrease ANG II sensitivity. 5 This may explain the resistance to the vasopressor effects of local RAS activation in kidney.
This study showed that urinary AGT excretion is lower in women with preeclampsia than in normal pregnancies. However, urinary AGT levels in preeclamptic pregnancies were still higher than in non-pregnant controls. The regulation of the systemic RAS in preeclampsia differs from that in normal pregnancies. Studies have demonstrated that many of the components of the systemic RAS in women with preeclampsia are down-regulated, including AGT. 2 Studies showed that the changes observed in the local RAS are different from those in the circulation in preeclampsia.12,15,16 However, in recent work, Chen et al. found low urinary AGT levels, similar to systemic RAS components, in women with preeclampsia. 16 Our results also confirmed the study findings of Chen et al. In addition, the results demonstrated that urinary AGT levels were associated with systolic and diastolic blood pressure levels in pregnancies with preeclampsia. This finding suggests that activation of the local RAS in kidney may have role in the elevation of blood pressure in preeclampsia. Compared with normotensive patients, hypertensive patients had significantly higher urinary AGT levels.17,18
Kobori et al. also demonstrated a significant relationship between blood pressure levels and urinary AGT in some specific patient populations, such as in patients with chronic kidney disease and diabetes mellitus.19-23 To the best of our knowledge, our study is the first study confirming this association in women with preeclampsia. Previous studies showed that hypertension in preeclampsia is due primarily to marked vasoconstriction, because both cardiac output and arterial compliance are reduced. 24 As mentioned before, women with an uncomplicated pregnancy show a relative vascular insensitivity to ANG II. Preeclamptic women, however, show increased ANG II sensitivity in their adrenal cortex and vascular system.5,25 Explanations for the increased reactivity to ANG II include up-regulation of receptor sensitivity, synergy with circulating auto-antibodies agonistic to the ANG type 1 receptor, and decreases in the level of circulating ANG 1-7.26,27 Increases in insulin resistance and sympathetic nervous system tone also occur, and have been implicated in the vasoconstriction characteristic of preeclampsia. 28 One of the important findings of the present study was the significant positive correlation between urinary AGT and daily urinary protein excretion in women with preeclampsia. Previous studies in hypertensive or renal patients have demonstrated similarly that an increased urinary AGT level was correlated with proteinuria.20-23 Many experimental and clinical studies in chronic kidney disease models described possible mechanisms for development of proteinuria via the local RAS in kidney.9,10,20
Previous studies evaluating the pathogenesis of proteinuria in preeclampsia have demonstrated pathogenic mechanisms including down-regulation of podocyte expression of nephrin, increased endothelin and decreased vascular endothelial growth factor (VEGF), indicating a mechanism where the endothelium loses its fenestrations, an alteration which contributes to protein loss in the urine.29-32 Likewise, experimental models demonstrated that locally produced ANG II in the kidney may induce proteinuria via reduction of nephrin expression and podocyte injury and stimulated expression of some cytokines such as VEGF.33-35 These findings suggest that local RAS activation in kidney may contribute to the pathogenesis of proteinuria in women with preeclampsia. However, the study was cross-sectional, and therefore no causal conclusion could be drawn.
In summary, this study showed that elevated local AGT expression was correlated with blood pressure elevation and renal injury, presented by proteinuria, in women with preeclampsia. The significance of this observation is highlighted by understanding the possible role of the local RAS in the kidney during pregnancy. Large longitudinal studies are needed to definitively explain the role of the local RAS in the kidney on preeclampsia pathogenesis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.