
Abstract
Introduction:
The relationship between smoking and mortality in patients on hemodialysis is controversial. Earlier studies showed that the insertion/deletion (I/D) polymorphism of the ACE gene might have an effect on mortality. The aim of this study was to test the impact of smoking on survival and whether this association was influenced by ACE gene I/D polymorphism in patients on maintenance hemodialysis.
Participants and methods:
In this prospective, multicenter cohort study we analyzed 709 prevalent patients on maintenance hemodialysis. Patients were allocated into groups based on their smoking habit. Outcome data were collected during the 144-month follow-up period. Outcomes of current smokers and lifelong non-smokers were compared. In order to control for interactions between predictor variables, we also identified 160 matched pairs for further sub-analysis.
Results:
The vast majority of patients (67%) were non-smokers, followed by current smokers (22.2%) and ex-smokers (9.8%). Smoking had no impact on survival in the matched pair analysis (p = 0.99). After adjustment for ACE I/D polymorphism and other co-variates, smoking had no effect on survival.
Conclusion:
Our data suggest that smoking has no impact on survival; neither is it associated with ACE gene I/D polymorphism in hemodialysis patients.
Keywords
Introduction
The survival of patients with end-stage renal disease (ESRD) on renal replacement therapy (RRT) has been improving over the past decade. However, the mortality rate is still high in this population compared to the general population and also to patients living with a less-severe degree of renal impairment. Therefore, identifying risk factors that could contribute to the progression of kidney disease and also development of comorbidities remains one of the priorities of the management of these patients. 1 Furthermore, concurrent presence of risk factors may aggravate their single harmful effect.
Several studies suggest that smoking is one of the modifiable risk factors that can accelerate the progression of chronic kidney disease (CKD). Potential mechanisms of this action include promotion of atherosclerosis in renal arteries, excessive formation of free radicals, higher activity of the sympathetic nervous system, and intrarenal hemodynamic changes and influencing the production of several cytokines in the renal interstitium. These could lead to tubular dysfunction, interstitial fibrosis, and glomerulosclerosis, and accelerate progression of CKD.2–5
Nicotine as a significant part of smoke resulted in activation of inflammatory mediators in the rat model of glomerular injury, whose results could be one explanation of kidney injury by smoke. 6 Based on the available evidence, nicotine seems to be one of the responsible deleterious factors in a progression of CKD because of its several biological and renal effects including mesangial and glomerular cell proliferation, fibronectin production, inflammation, oxidative stress and reducing number of podocytes. Interestingly, however, some studies showed a protective effect of nicotine in certain conditions. 7
The association between smoking and accelerated progression of CKD has been demonstrated in patients with various etiologies of kidney disease.8–10 Furthermore, graft survival after kidney transplantation was significantly better in non-smokers compared to patients who smoked. 11
According to a recently published meta-analysis, smoking was associated with a significant increase in all-cause mortality in dialyzed patients. However, not all of the examined studies showed a significant association between smoking and mortality. 12 Soon after this meta-analysis, a post hoc analysis of the Hemodialysis (HEMO) study appeared giving additional evidence on this topic. Comparing data of patients who were current smokers to those of patients who never smoked, the results showed that smokers had significantly greater infection-related and all-cause mortality, and this group also had higher cardiovascular, infection-related and all-cause hospitalization rates during a two-year follow-up. 13 The reason for the particular focus on smoking is not only because it has a considerable impact on renal damage, cardiovascular comorbidities, carcinogenesis and eventually patient survival, but it is definitely a modifiable risk factor. 14 Furthermore, there is evidence that smoking cessation is beneficial for renal function. In patients with type 2 diabetes, smoking cessation could ameliorate the progression of CKD.15,16 Also, in patients with immunoglobulin (Ig)A nephropathy, smoking status and the number of cigarettes smoked were significant predictors for progression of kidney disease. 17
In our previous study, we showed that angiotensin I converting enzyme (ACE) gene insertion/deletion (I/D) polymorphism was associated with mortality in hemodialyzed patients. Patients with the D/D genotype had an inferior outcome, compared to patients with the I/D or I/I genotype. We also showed that ACE inhibitor therapy, as a strong remediable factor in the renin angiotensin aldosterone system (RAAS), can mitigate the deleterious effect of the D/D genotype on survival. 18 In a more recent study, authors found an association between ACE gene I/D polymorphism and development of end-stage renal disease (ESRD). Patients with I/D or D/D genotypes had higher risk for progression of CKD to ESRD than patients with the I/I genotype. The distribution of genotypes between patients with ESRD and healthy controls was significantly different. In ESRD patients, the D allele was detected more frequently. Furthermore, the authors claimed that interaction of the gene polymorphism and smoking can enhance the development of ESRD because smokers with the D/D genotype followed by the I/D genotype showed inferior outcome for disease progression compared to patients with the I/I genotype. 19 In contrast, in an earlier study, the authors did not find any association between ACE gene I/D polymorphism and smoking status. 20 Despite a considerable amount of evidence about the harmful effect of smoking on the progression of renal disease of various etiologies and its impact on mortality, there are still conflicting data about the association between smoking and survival in patients on hemodialysis.
We hypothesized that this inconsistency in the literature could be explained by a potential interaction between smoking and ACE I/D polymorphism on survival in this population. Therefore, the aim of this study was to test the impact of ACE I/D polymorphism on the association between smoking and survival in patients with ESRD on hemodialysis.
Participants and methods
All data for the current retrospective analysis were extracted from the database of the B. Braun Avitum Hungary-DialGene Study. This was a cross-sectional genetic study that was conducted in the dialysis units of the B. Braun Avitum Hungary CPLC Dialysis Network. The contributors to the study are listed in the acknowledgment of this article. Data collection started in 11 dialysis centers of the B. Braun Avitum Hungary CPLC Dialysis Network in 1997.
Inclusion criteria were more than 90 days on dialysis at the time of cross-sectional data collection and written informed consent to the study. A total of 746 patients were eligible for baseline data collection. During the follow-up period of 12 years, only outcome data were collected. Thirty-seven patients had an incomplete data set; they were therefore excluded from the analysis.
Patients were assigned to three groups according to their smoking status: “current smokers,” “ex-smokers” and “non-smokers,” who never smoked habitually. For further analysis, we excluded patients in the “ex-smokers” groups.
Because of the significant differences in baseline parameters between the patient groups, we identified 160 matched pairs based on smoking status (smokers and non-smokers) in order to explore the impact of smoking on survival. Matching variables were gender, age (⩽ 10 years difference), time on dialysis at baseline (according to the following categories: less than 12 months, 12–35 months, 36–59 months, more than 60 months) and diabetes mellitus. Variables were compared using the paired t-test and McNemar test. Kaplan-Meier estimate with log-rank test was used in this sub-cohort of patients to compare survival of patients who smoked vs never smoked.
In addition, Cox proportional hazard models were created to examine the effect of smoking and ACE I/D polymorphism on survival in the whole study cohort. Since a significant association was found between age and smoking status, the Cox models were stratified by age groups (18–44 years, 45–64 and ⩾ 65 years). All multivariate models were adjusted for age, gender and diabetes.
Continuous variables were presented with mean ± standard deviation (SD) and categorical variables with absolute and relative frequencies (%). Differences in characteristics of groups were compared with the use of analyses of variance (ANOVA) (comparisons of group Tukey-test) or Kruskal-Wallis and Mann-Whitney test for continuous variables, chi-square test for categorical variables. A p value less than 0.05 was considered statistically significant. Statistical analyses were performed using STATISTICA v.10 software (Tulsa, OK, USA).
Results
Baseline characteristics of all patients in the study and also in groups according to their smoking status are presented in Table 1. A total of 709 patients were enrolled in the analysis. The majority of the patients were non-smokers (n = 480), followed by current smokers (n = 159) and ex-smokers (n = 70). The mean age was 54.9±15.5 years and current smokers were younger than ex-smokers and non-smokers (p < 0.001 for each). The proportion of male gender was 53.2%. Males were more prevalent in the current and ex-smoker groups, but female patients were more prevalent among non-smokers. There were significantly more male patients, who were also significantly younger, in the current smokers group.
Baseline characteristics of dialyzed patients by smoking habit.

PKD: polycystic kidney disease; ESRD: end-stage renal disease; ACE: angiotensin I converting enzyme; I: insertion; D: deletion.
The most frequent cause of ESRD in the whole cohort was glomerulonephritis (28.9%), followed by tubulointerstitial disease (24.2%).
Glomerulonephritis was the most prevalent cause of ESRD in the current smoker and ex-smoker groups, whereas tubulointerstitial disease was more prevalent in patients who never smoked. The prevalence of diabetes was 16.5% in the whole cohort and it was the least prevalent in current smokers.
The duration of dialysis treatment (dialysis vintage) before the cross-sectional data collection was 23.8 (interquartile range, IQR: 11.2–47.1) months. Dialysis vintage and distribution of ACE gene I/D genotypes were well balanced among the three groups. There were no associations between ACE gene I/D polymorphism or allele frequency and smoking status (Table 1). Similarly, when patients were re-allocated into aggregated groups (current smokers plus ex-smokers vs non-smokers or current smokers vs non-smokers plus ex-smokers), we did not find any associations between ACE gene polymorphism or allele frequency and smoking habit (data not shown).
In the matched pair analysis, mean age was 48.0±14.8 years in the smoker group and 48.9±13.8 years in the non-smoker patients (p = 0.64); the proportion of male patients (71.9%), the prevalence of diabetes (7.5%) and also dialysis vintage (36.1±34.1 vs 37.8±35.4 months; p = 0.97) were similar. There were no differences in the distributions of ACE gene I/D genotypes (p = 0.27) between the two groups. The 12-year cumulative mortality was also similar (50.0% vs 51.9%; p = 0.80) in the two groups. The mean survival time was also similar in the two groups: 93.6±3.8 months (95% confidence interval (CI): 86.1–101.1) and 93.7±4.1 months (95% CI: 85.7–101.7) for non-smokers and smokers, respectively. In the Kaplan-Meier analysis, there was no survival difference between patients who smoked or never-smoked (log-rank test: p = 0.99) (Figure 1).
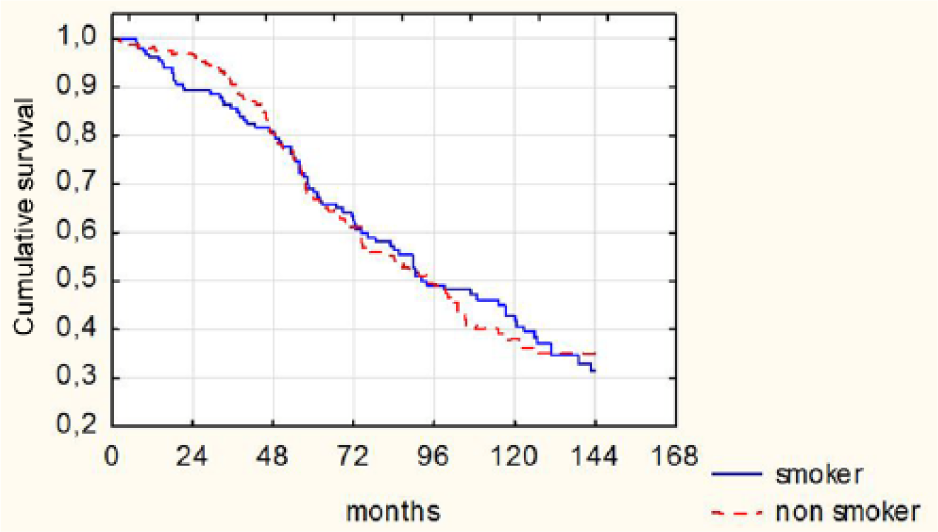
Kaplan-Meier survival estimates for smoker and non-smoker patients, based on the matched pair analysis (log-rank test: p = 0.99).
The multivariate Cox regression models were stratified to three age groups and further adjusted for age, gender and diabetes, as described. Neither smoking nor ACE I/D polymorphism proved to be a significant predictor of mortality (Table 2). Additional multivariate models created for comparing current-smokers vs ex-smokers showed similar results (data not shown).
Multivariate Cox proportional hazards model for survival in hemodialyzed patients with different age groups.

Adjusted for age and gender. HR: hazard ratio; CI: confidence interval; I: insertion; D: deletion.
Discussion
In this multicenter, retrospective cohort study, we analyzed the potential effect of ACE I/D polymorphism on the association between smoking and survival among chronic hemodialysis patients. We found that irrespective of ACE gene I/D polymorphism, smoking had no effect on mortality in our cohort of end-stage kidney disease patients on hemodialysis.
Our results concerning no relationship between smoking and survival in unselected hemodialysis patients are in contrast to the results of a recently published meta-analysis by Liebman et al. 12 and the post hoc analysis of the HEMO study data set. 13 There might be numerous reasons for this contradictory result. Among the 10 studies included in the above meta-analysis, only six reported significant associations between smoking and all-cause mortality and only two out of five between smoking and cardiovascular mortality. The heterogeneity of the results is remarkable. Interestingly, in studies in which smoking was the primary variable of interest, it was not associated with mortality, whereas in other studies, smoking as a covariable in multivariate models was a significant predictor of mortality. In these latter studies, significant associations between smoking and other predictor variables (such as age, gender and comorbidities) could have obscured the observed relationship. Particularly, age and gender were highly related to smoking in our analysis as well. In order to control for these correlations of predictor variables, we used the matched pair analysis in the study. In addition, patients with current acute medical conditions were generally excluded from the above studies, which could result in excluding high-risk patients and might lead to further biases. Our cohort was not selected in this regard and therefore we believe that it was more representative of the chronic hemodialysis population.
The low number of patients in our analysis could also explain why we failed to detect a very strong potential association between all-cause mortality and smoking. The above cited post hoc analysis of the HEMO study included more than 1800 patients, allowing the detection of a 44% greater adjusted risk (with 95% CI 1.16–1.79) of mortality in current smokers vs lifelong non-smokers. Although one could observe a trend for increased mortality in smokers aged between 45 and 64 years in our data set, our cohort did not allow the detection of a potential association of this magnitude with confidence.
The I/D polymorphism of the ACE gene was found to be an important mortality risk factor among patients on hemodialysis in a previous analysis. Although rarely examined, this polymorphism could also have an effect on associations between other predictors, such as smoking and mortality. We hypothesized that this polymorphism could stand behind the conflicting results regarding the association between smoking and mortality. Our current analysis failed to demonstrate this modifying effect.
Our study has some major limitations that could also bias the results. The cross-sectional nature of data collection did not allow for potential temporal changes in smoking habit. Consequently, we had to assume that this factor remained stable in time. However, some patients in our cohort might have started or stopped smoking during the follow-up period, and this could have reduced the mortality difference between the two patient groups.
The assessment of smoking habit was based on patient self-report. Although this adds some uncertainty to our variable of main interest, it could rather affect mis-classification between current and former smokers only. Since we decided to exclude former smokers from our analysis, this resulting potential bias was rather small, if any. It is very unlikely that lifelong non-smokers were reported as smokers or contrariwise.
The quantity of smoking was not assessed in our study, which could lead to great heterogeneity among our patients in the current smoker group. Consequently, it could lessen the mortality difference between the examined patient groups.
Conflicting results were reported about the associations between mortality and former smoking. Some authors found that there was no difference in mortality between these patients, whereas others found that smoking cessation even after one year resulted in a lower risk of mortality compared to current smokers. For clarity and to prevent mis-classification bias, we decided to exclude former smokers from our analysis.
Our cohort included only patients of Caucasian origin, and therefore our results might be difficult to generalize to patients of other races. ACE I and D allele frequencies might well be different in other races, as was shown among Han Chinese ESRD patients in a recent report by Yang et al. 19
Interestingly, the authors of this report found significant interaction between ACE I/D polymorphism and smoking habit. ESRD patients who ever smoked more likely had the D allele compared to patients who never smoked. We could not observe a similar association between ACE I/D polymorphism and smoking habit. This lack of association was reported in a representative cohort of Caucasian patients without kidney disease, as well.
We believe that the above limitations might explain to some extent why we did not observe a significant association between smoking and mortality in our cohort. However, our data clearly demonstrate that ACE I/D polymorphism has no impact on this potential association. Furthermore, we do not suggest that smoking has no impact on mortality in this population.
Footnotes
Acknowledgements
Contributors to the BBAVHU-DIALGENE study in the B. Braun Avitum Hungary CPLC Dialysis Network were: Zoltán Amma, MD, Attila Benke, MD, Béla Borbás, MD, Sándor Ferenczi, MD, Mária Hengsperger, MD, Szilvia Kazup, MD, Lajos Nagy, MD, József Németh, MD, Antal Rozinka, MD, Tamás Szabó, MD, Tamás Szelestei, MD, PhD, Eszter Tóth, MD, Gábor Varga, MD and Gábor Zakar, MD.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Hungarian Scientific Research Group (OTKA, TO23927/1997) and the B. Braun Avitum Hungary CPLC Dialysis Network.