
Abstract
Background:
Several reports suggest that the use of angiotensin receptor blockers (ARBs) is associated with lung cancer (LC) reduction. However, the results were contradictory.
Methods:
Four online databases were searched. The strength of the association between ARB and the risk of LC was measured by odds ratio (OR) and 95% confidence interval (CI). OR was analyzed by random-effects model.
Results:
Eight studies with 298000 subjects were included in this meta-analysis. Using of ARB was significantly associated with decreased LC risk (OR = 0.81; 95% CI 0.69–0.94; p = 0.005). In the subgroup analysis by race, Asians treated with ARB showed decreased LC risk (OR = 0.60; 95% CI 0.54–0.67; p < 0.00001). However, Caucasians treated with ARB did not show significantly decreased LC risk (OR = 0.90; 95% CI 0.79–1.02; p = 0.11). Subgroup analysis by duration of follow-up was conducted. The studies with less than 5 years showed significant result (OR = 0.79; 95% CI 0.64–0.97;p = 0.02). However, the studies with more than 5 years did not show significantly decreased LC risk (OR = 0.84; 95% CI 0.61–1.16; p = 0.29).
Conclusions:
This meta-analysis indicated that ARBs may be associated with decreased risk of LC.
Introduction
Lung cancer (LC) is a major cause of cancer death worldwide with 1 million deaths each year. 1 More than 80% of LC cases are of non-small cell lung cancer (NSCLC), 2 and it has been estimated that 51% of patients present with advanced disease at the time of diagnosis. 3 Although much progress has been made in optimizing the treatment of LC (including multidisciplinary therapy, targeted therapy, etc.), the 5-year overall survival rate remains about 15% for all stages. 1 Therefore, it is important to find new therapies which could prevent LC development.
The angiotensin I-converting enzyme (ACE) regulates angiotensin II (AngII), the active peptide of the renin–angiotensin system (RAS) that regulates blood pressure. ACE has also been associated with cell proliferation, angiogenesis, and inflammation. 4 The receptor of AngII, the AngII type1 receptor (AT1R) subtype, is expressed on tumor and endothelial cells, and is upregulated in many cancer tissues. Angiotensin receptor blockers (ARBs) are used as one of the first-choice drugs for patients with hypertension. Some studies reported that ARB user showed decreased LC risk. However, other studies could not confirm this result.5–12 Thus, the result is still controversial. We performed this meta-analysis to assess the relationship between ARB and LC risk.
Methods
Publication search
Two researchers independently performed a computerized search in four databases up to April 2015: PubMed, ISI Web of Knowledge, Chinese National Knowledge Infrastructure, and Wanfang. The search terms were “angiotensin receptor blocker” or ARB, “lung cancer or lung carcinoma or lung neoplasm” in various combinations, with no language limitation. The reference list of each relevant publication was also reviewed to ensure that all appropriate studies were included in the meta-analysis.
Study selection
The inclusion criteria were as follows: (1) the research was a case-control study or a cohort study; (2) the study investigated the association between ARB and LC risk; (3) sufficient published data about sample size, odds ratio (OR), and their 95% confidence interval (CI). Studies were excluded when they were: (1) a duplicate publication; (2) meta-analyses, letters, reviews, or editorial articles.
Data extraction
Two reviewers collected the data and reached a consensus on all items. The following items were extracted from each study if available: first author, year of publication, study design, ethnicity, age, gender, sample size, follow-up years, and covariates.
Qualitative assessment
Two authors completed the quality assessment independently. The Newcastle–Ottawa Scale (NOS) was used to evaluate the methodological quality, which scored studies by the selection of the study groups, the comparability of the groups, and the ascertainment of the outcome of interest. We considered a study awarded 0–3, 4–6, or 7–9 as a low-, moderate-, or high-quality study, respectively.
Statistical analysis
The strength of the association between ARB and the risk of LC was measured by OR and 95% CI. OR was analyzed by random-effects model. Heterogeneity was evaluated by an χ2-based Q statistic and was considered statistically significant when p < 0.10. The significance of the pooled OR was determined by the Z-test and was considered statistically when the p-value was less than 0.05. Subgroup analyses by ethnic groups and follow-up years (less than 5 years or not) were performed. Publication bias was analyzed by funnel plots and Egger’s test. All statistical tests were performed using the Revman 5.1 and STATA 11.0 software.
Results
Eligible studies
Eight studies with 298,000 subjects were included in this meta-analysis. Three studies were case-control studies and five studies were cohort studies. Three studies were conducted in Asian patients and four studies were performed in Caucasian patients. The median follow-up duration ranged from 2.9 to 7.8 years. The quality score ranged from 7 to 9, suggesting that the quality of the studies was good. The characteristics of included studies are showed in Table 1.
Characteristics of the included studies.

ACEI: angiotensin-converting enzyme inhibitor; BB: beta-blocker; BMI: body mass index; CCB: calcium channel blocker; NA: not available; NSAIDs: Non-steroidal anti-inflammatory drugs; DM: diabetes mellitus.
Quantitative data synthesis
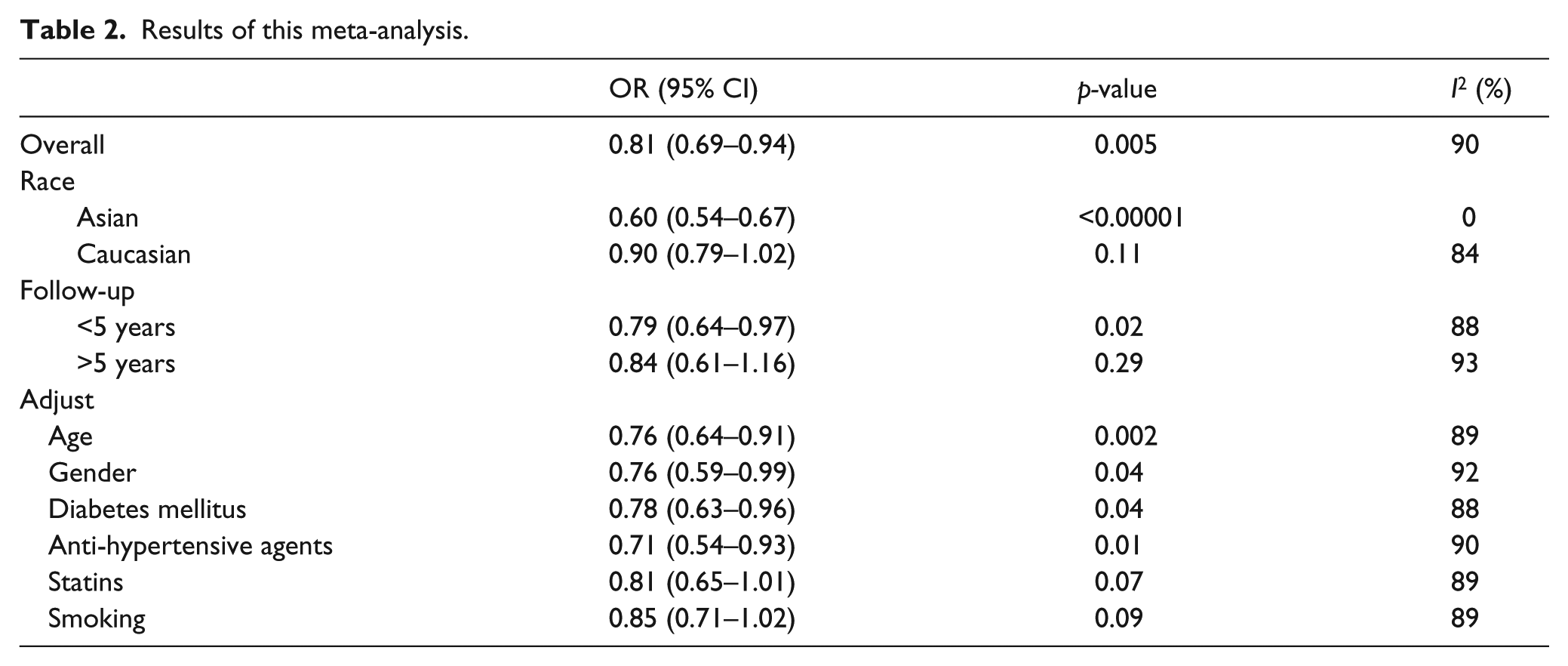
As shown in Figure 1, using of ARB was significantly associated with decreased LC risk (OR = 0.81; 95% CI 0.69–0.94; p = 0.005). In the subgroup analysis by race, Asians treated with ARB showed decreased LC risk (OR = 0.60; 95% CI 0.54–0.67; p < 0.00001; Figure 2). However, Caucasians treated with ARB did not show significantly decreased LC risk (OR = 0.90; 95% CI 0.79–1.02; p = 0.11; Figure 2). Subgroup analysis by duration of follow-up was conducted. As shown in Figure 3, the studies with less than 5 years’ duration showed significant result (OR = 0.79; 95% CI 0.64–0.97; p = 0.02). However, the studies of more than 5 years did not show significantly decreased LC risk (OR = 0.84; 95% CI 0.61–1.16; p = 0.29). When we limited the meta-analysis to studies that controlled for confounders such as age, sex, diabetes, coronary artery disease, and anti-hypertensive agents, a significant association between ARB use and decreased LC risk remained (Table 2). However, when we limited the meta-analysis to studies that controlled for statins or smoking, the result was changed (Table 2).
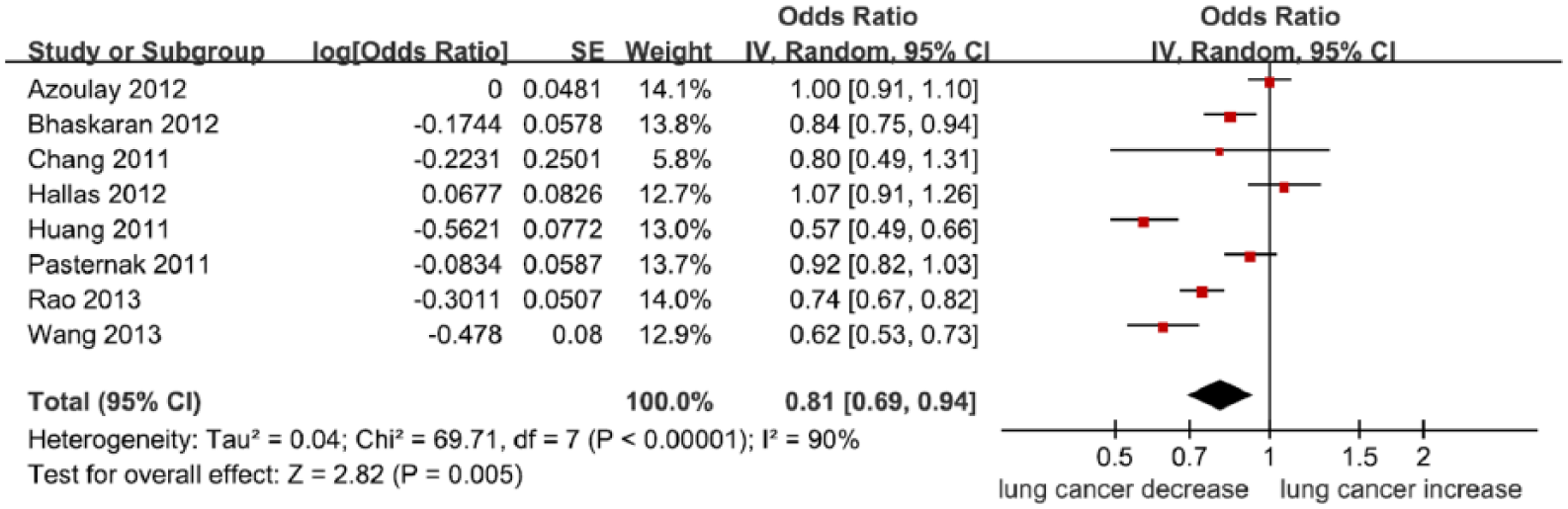
Meta-analysis of the association between ARBs and LC risk.

Subgroup analysis by race of the association between ARBs and LC risk.

Subgroup analysis by duration of follow-up of the association between ARBs and LC risk.
Results of this meta-analysis.
The funnel plot and Egger’s test were performed for the overall comparison. No obvious visual asymmetry was observed in funnel plots (Figure 4), and the p-value of the Egger’s test was greater than 0.05, indicating no statistical evidence for publication bias among studies.

Funnel plot for the association between ARBs and LC risk.
Discussion
The present meta-analysis of eight observational studies showed that the use of ARBs could decrease LC risk. This result suggested that ARBs might be a protective factor for LC. However, this protective value was only found in Asians and not in Caucasians. It was possible that different lifestyles, diets, and environments may account for this discrepancy. In addition, we found that this protective effect might decrease if the duration of follow-up is more than 5 years. This result indicated that time might modify the effect of ARB on LC risk. Furthermore, we observed that statin and smoking status could also modify the effect of ARB on LC risk.
RAS signaling has been shown to increase cell proliferation during malignancy, and ARBs are able to decrease pro-survival signaling by inhibiting anti-apoptotic molecules and suppressing caspase activity. 4 A previous study found that telmisartan could induce apoptosis via down-regulation of Bcl-2 and involvement of caspase-3 in human renal cancer cells. 13 Wilop and coworkers suggested that addition of ACEI or ARB to platinum-based first-line chemotherapy may contribute to prolonged survival in patients with advanced LC. 14 Inhibition of RAS could also improve the risk and survival of other cancers. Rao et al. found a small, but statistically significant, reduction in the incidence of clinically detected prostate cancer among patients assigned to receive ARB. 15 Babacan et al. suggested that the use of ACE inhibitors/ARBs may be effective in N3+ breast cancer patients. 16 Chen et al. indicated that administration of ACEIs/ARBs was independently associated with superior overall survival in patients with esophageal squamous cell carcinoma receiving oesophagectomy. 17
Our analysis has several limitations. First, all the included studies were observational investigations and cannot thus support any causality between the use of ARB and LC risk. Second, the lack of the original data of the eligible studies limited the evaluation of the effects of ARB on different populations, such as smokers and non-smokers. In addition, the subgroup analysis of statins was also not conducted. Third, although we performed an extensive review of the main electronic databases, we cannot be sure to have included all relevant studies.
Conclusion
In conclusion, this meta-analysis indicated that ARBs may be associated with decreased risk of LC. ABRs might be one of the chemoprophylactic drugs of LC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.