
Abstract
Background:
Preventive medications for dialysis-requiring congestive heart failure (CHF) in non-dialysis Japanese patients with Stage 5 chronic kidney disease (CKD) are unknown. Our aim was to explore which CKD medication was associated with a reduced prevalence of dialysis-requiring CHF in non-dialysis Japanese patients with Stage 5 CKD.
Methods:
The present multicenter, retrospective, cross-sectional study examined the association between CKD medications and the prevalence of dialysis-requiring CHF in non-dialysis Japanese patients with Stage 5 CKD.
Results:
There were 1536 Japanese Stage 5 CKD patients who satisfied our inclusion criteria. We had 309 (20.1%) patients whom had developed dialysis-requiring CHF and 940 patients (60.8%) whom had been using angiotensin-II receptor blockers (ARBs) before initiating dialysis. In our multivariate analysis, only ARB use was significantly associated with a lower risk of CHF (Odds ratio (OR): 0.680, 95% confidence interval (CI): 0.516–0.897; p = 0.0064), of the CKD treatments examined in this study.
Conclusions:
We found that ARB use during the pre-dialysis period is associated with a lower prevalence of CHF in the non-dialysis Japanese patients with Stage 5 CKD, suggesting a possible prevention of dialysis-requiring CHF by ARBs, in non-dialysis Japanese patients with Stage 5 CKD.
Keywords
Introduction
The prevalence of chronic kidney disease (CKD) is estimated to be 8–16% worldwide, 1 and the risk of death or cardiovascular events increases with increasing CKD stages.1–4 In the early-to-moderate CKD stages, inhibition of the renin-angiotensin-aldosterone system has been shown to provide both renal and cardiac protection.5–10 Angiotensin-converting enzyme inhibitors (ACEIs) are used worldwide to treat hypertension, CKD, and cardiovascular disease.11–15 A recent meta-analysis has revealed that ACEIs reduce the incidence of all-cause mortality, cardiovascular mortality, and major cardiovascular events, including congestive heart failure (CHF) in early-to-moderate stage CKD and in patients with diabetes mellitus; although angiotensin-II receptor blocker (ARB) use do not reduce the incidence of these events, except for CHF. 16
Hsu et al. 26 report that ACEI, but not ARB, used effectively prevent mortality and end-stage renal disease progression, while ARB use only decreases hospitalization due to CHF; however, approximately 5–20% of patients cannot tolerate ACEIs, because of dry cough and the other adverse effects (e.g. angioedema, hypotension, hyperkalemia or renal dysfunction).17–20 Unfortunately, this persistent dry cough is highly prevalent in the East Asian populations21,22; therefore, many East Asian patients must be switched from ACEI to ARB, as an alternative treatment. Recently, Nishio et al. 23 reported 2 gene polymorphisms of angiotensin-converting enzyme deletion/insertion (ACE D/I) and bradykinin B2 receptor -58T/C contribute to the risk of ACEI-related cough in East Asians, but a negative association between the ACE I/D polymorphism and ACEI-related cough was observed in Caucasians. Thus, the effect of ARB should be clarified in Japanese CKD patients, which motivated us to explore the effect of ARBs in dialysis-requiring CHF in late-stage CKD patients in Japan.
To date, preventive effects of the medications used for CKD on patients with dialysis-requiring CHF is not well understood.24–26 In addition, few clinical reports focus on patients with Stage 5 CKD, which is defined by an estimated glomerular filtration rate (eGFR) of < 15 mL/min/1.73m2. A recent study reports that ACEI or ARB use in non-dialysis patients with Stage 5 CKD is associated with a reduced risk of long-term dialysis or death, 27 but no information was provided regarding dialysis-requiring CHF patients.
Among the uremic symptoms that require renal replacement therapy (RRT), CHF significantly predicts the incidence of cardiac events and mortality in end-stage kidney disease.28,29 Unfortunately, no effective preventative treatment for CHF has been definitively described for patients with Stage 5 CKD. Furthermore, the ability of ARB to prevent CHF (a major reason for initiating RRT) has not been assessed in patients with Stage 5 CKD. Thus, we evaluated the associations between various medications (including ACEI and ARB) and the prevalence of dialysis-requiring CHF in non-dialysis Japanese patients with Stage 5 CKD. Our objective was to explore which CKD medication would be associated with a reduced prevalence of dialysis-requiring CHF, in non-dialysis Japanese patients with Stage 5 CKD.
Methods
Study design
This study used a cross-sectional, observational multicenter design, and included 3447 Japanese patients across nine Japanese institutions, whom had initiated RRT between 1 January 2006 and 31 October 2013. All participating institutions belonged to the Japanese Study Group for Assessing Initiation of Renal Replacement Therapy (J-START), and these institutions served as the primary pre-dialysis source of information, for patients with end-stage kidney disease. All the J-START members are nephrologists who have been certified by the Japanese Society of Nephrology and the Japanese Society of Dialysis Therapy. We collected clinical information and hematological data at the institutional level, immediately before the patient’s first hemodialysis session, according to the J-START database sheet (Microsoft Excel). Each patient’s information was only labeled with the institution and patient number, to protect their privacy. This study was performed in accordance with the Declaration of Helsinki. The ethics committee for clinical research of Jikei University School of Medicine approved this study (permission number 25-343).
To explore the association between CKD medications and dialysis-requiring CHF, the following inclusion criteria were selected:
Only Japanese Stage 5 CKD patients who were followed up over 3 months and received a stable prescription > 3 months by a nephrologist, to exclude emergent initiation of dialysis, for AKI; and
Those with patient records with complete data, regarding the following factors: age, gender, presence of diabetic kidney disease, reasons (uremic symptoms) for initiating RRT, history of ischemic heart disease (IHD), duration of nephrologist follow-up, systolic and diastolic blood pressure, and laboratory data (hemoglobin, albumin, urea nitrogen, creatinine, sodium, potassium, chloride, corrected calcium, phosphorus, C-reactive protein (CRP) and intact parathyroid hormone (PTH).
As a result, 1911 patients were excluded from the analysis, due to having Stage 1–4 CKD (45 patients), being ⩽ 19 years old (3 patients), having an uncertain history of IHD (164 patients) and comorbidity (29 patients), having a follow-up period of < 3 months or of unknown length (819 patients), lack of data regarding medication use in the previous 3 months (254 patients) and insufficient laboratory data (624 patients). Therefore, among the 3474 patients whom we evaluated, there were 1536 Japanese patients satisfying our inclusion criteria whom were included in our analysis (Figure 1). Compared to the included patients, the excluded patients whom had < 3 months of nephrologist follow-up had a significantly higher prevalence of dialysis-requiring CHF (35.8% versus 20.1%; p < 0.0001), a lower prevalence of diabetic kidney disease (35.9% versus 43.3%; p = 0.0024), a lower frequency of ARB use (36.5% versus 60.8%; p < 0.0001), and higher levels of CRP (3.17 ± 4.96 mg/dL versus 1.27 ± 3.06 mg/dL; p < 0.0001). We observed no significant differences regarding age, gender, eGFR and history of IHD, when the included and excluded patients were compared.

Study flow chart.
The eGFR was calculated using the new Japanese equations, 30 for men (1) and for women (2):


We used a modified version of Framingham heart failure diagnostic criteria to confirm the diagnosis of CHF. 31 A diagnosis of CHF was made according to the presence of orthopnea, sudden weight gain and radiography findings (enlarged pulmonary vessels, alveolar edema and pleural effusion); and these findings were rapidly resolved after the first hemodialysis session.
We also collected information regarding the patients’ medication use before starting dialysis. The specific medications that we evaluated were erythropoietin receptor stimulating agents (ESAs), ACEIs, ARBs, calcium channel blockers (CCBs), loop diuretics, other anti-hypertensive agents (alpha-blockers and/or beta-blockers, and/or other hypertensive drugs), Vitamin D receptor activators (VDRAs), calcium carbonate (CaCO3) and AST-120 (Kureha Corporation, Tokyo, Japan) is an orally administered spherical carbon adsorbent that can adsorb various small molecule uremic toxins. 32
Variables
The primary outcome was the prevalence of CHF at dialysis initiation, and the predictor variable was the CKD medications used before dialysis initiation. We also selected the following explanatory variables: gender; age; comorbid diabetes mellitus; medical history of IHD; the nephrology follow-up period; systolic and diastolic blood pressure; use of ARBs, ACEIs, CCBs, other antihypertensive drugs, loop diuretics, ESAs, VDRAs, CaCO3, or AST-120; eGFR; serum uric acid; serum potassium; serum chloride; serum corrected calcium; serum phosphorus; serum intact PTH; serum albumin; and hemoglobin concentration.
Statistics
Statistical analyses were performed using JMP 9.0 (SAS Institute Inc., Cary, NC, USA). Data were expressed as the mean ± SD or number (percentage) of patients. Comparisons across the various groups were performed using the Pearson chi-squared test for categorical data and the Dunnett test for continuous data. All tests were two-tailed, and a p < 0.05 was considered statistically significant. Factors that were associated with CHF during the univariate analysis were subsequently included in a multivariate model. Multivariate logistic regression analyses were performed to identify the covariates that were associated with the development of dialysis-requiring CHF. Odds ratios (ORs) and 95% CIs were determined using univariate and multivariate logistic regression models for the factors that were significantly associated with CHF. We used Forrest plots to summarize the results of the logistic regression analysis, and Microsoft Excel to plot the 95% CI range on the log scale Forrest plots.
Results
Reasons for starting dialysis
Figure 2 shows the reasons (uremic symptoms) for initiating dialysis. Among the 1536 Japanese patients, 309 patients (20.1%) started RRT due to developing CHF, 230 patients (15.0%) started RRT due to gastro-intestinal symptoms, 198 patients (12.9%) started RRT due to uncontrollable edema, 77 patients (5.0%) started RRT due to other symptoms (anemia, neurological or other symptoms), and 722 patients (47.0%) underwent planned RRT (with no symptoms).

Reasons (uremic symptoms) for initiating dialysis in Japanese patients with Stage 5 CKD. Data are expressed as the percentage of the total study population.
Comparison of patients presenting with or without CHF
The patients’ characteristics and laboratory test results from immediately before starting dialysis are shown in Table 1, along with a comparison of patients with and without CHF. Compared to the patients without CHF, the patients whom presented with CHF were significantly older (66.7 ± 12.9 years, versus 68.9 ± 13.4 years; p = 0.0092), had a higher frequency of diabetic kidney disease (40.1% versus 55.3%; p < 0.0001), a higher frequency of a medical history of IHD (16.3% versus 28.5%; p < 0.0001), a lower diastolic blood pressure (77.6 ± 13.8 mmHg versus 75.3 ± 16.5 mmHg; p = 0.0123), and a shorter follow-up period (3.83 ± 3.73 years versus 3.14 ± 3.11 years; p = 0.0028).
Baseline characteristics and comparison of patients who presented with or without CHF.

Data are expressed as a number (%) of patients or the mean ± SD.
ACEI: angiotensin-converting enzyme inhibitor; BP: blood pressure; ARB: angiotensin-II receptor blocker; AST-120: an orally administered uremic toxins adsorbent32; CaCO3: calcium carbonate; CCB: calcium channel blocker; CHF: congestive heart failure; CRP: C-reactive protein; CTR: cardiothoracic ratio; eGFR: estimated glomerular filtration rate; ESA: erythropoietin receptor stimulating agent; IHD: ischemic heart disease; PTH: parathyroid hormone; VDRA: vitamin D receptor activator.
In addition, the patients who presented with CHF used loop diuretics significantly more frequently (66.5% versus 82.5%; p < 0.0001), and used ARBs (62.2% versus 56.0%; p = 0.0460), CaCO3 (36.3% versus 26.9%; p = 0.0019) and VDRAs (27.5% versus 17.8%; p = 0.0005) less frequently, when compared to the patients without CHF; however, we observed no significant associations between CHF development and the use of ACEIs, CCBs, ESAs, AST-120 or other hypertensive drugs.
The patients who started RRT due to CHF development also had significantly higher levels of CRP (0.94 ± 2.50 mg/dl versus 2.60 ± 4.43 mg/dl; p < 0.0001), eGFR (5.04 ± 1.77 mL/min/1.73m2 versus 5.84 ± 2.32 mL/min/1.73m2; p < 0.0001), uric acid (8.43 ± 2.18 g/dL versus 8.78 ± 2.43 g/dL; p = 0.0122), corrected calcium (8.51 ± 0.92 mg/L versus 8.67 ± 0.97 mg/L; p = 0.0062) and cardiothoracic ratio (CTR) (53.2 ± 6.1% versus 58.0 ± 6.7%; p < 0.0001), as well as significantly lower levels of hemoglobin (8.83 ± 1.47 g/dL versus 8.54 ± 1.51g/dL; p = 0.0023), serum creatinine (9.57 ± 3.18 mg/dL versus 8.54 ± 3.06 mg/dL; p < 0.0001), potassium (4.63 ± 0.82 mEq/L versus 4.50 ± 0.86 mEq/L; p = 0.0174), chloride (105.2 ± 6.0 mEq/L versus 104.0 ± 6.2 mEq/L; p = 0.0018) and serum albumin (3.30 ± 0.58 g/dL versus 3.03 ± 0.57 g/dL; p < 0.0001). There were no significant differences between the two groups, regarding gender, systolic blood pressure, urea nitrogen, sodium, phosphorus and intact PTH.
Association between various risk factors and the prevalence of CHF
As is shown in Table 2, univariate and multivariate-adjusted logistic regression analysis were used to assess the independent association between CHF development and medications or the other clinical parameters. The primary outcome was the prevalence of CHF at dialysis initiation, the predictor variable was ARB use, and the covariates were determined according to their univariate relationship or importance within the explanatory variables. In the univariate analysis, older age, shorter nephrologist follow-up, lower diastolic blood pressure, and higher levels of corrected calcium were risk factors for dialysis-requiring CHF, although they were not independent risk factors after the multivariate-adjusted logistic regression analysis. VDRA and CaCO3 use were also associated with dialysis-requiring CHF in the univariate model, although these associations disappeared after adjusting for intact PTH, corrected calcium and the nephrologist follow-up period.
The association between various risk factors and the prevalence of CHF in non-dialysis Japanese patients with Stage 5 CKD.
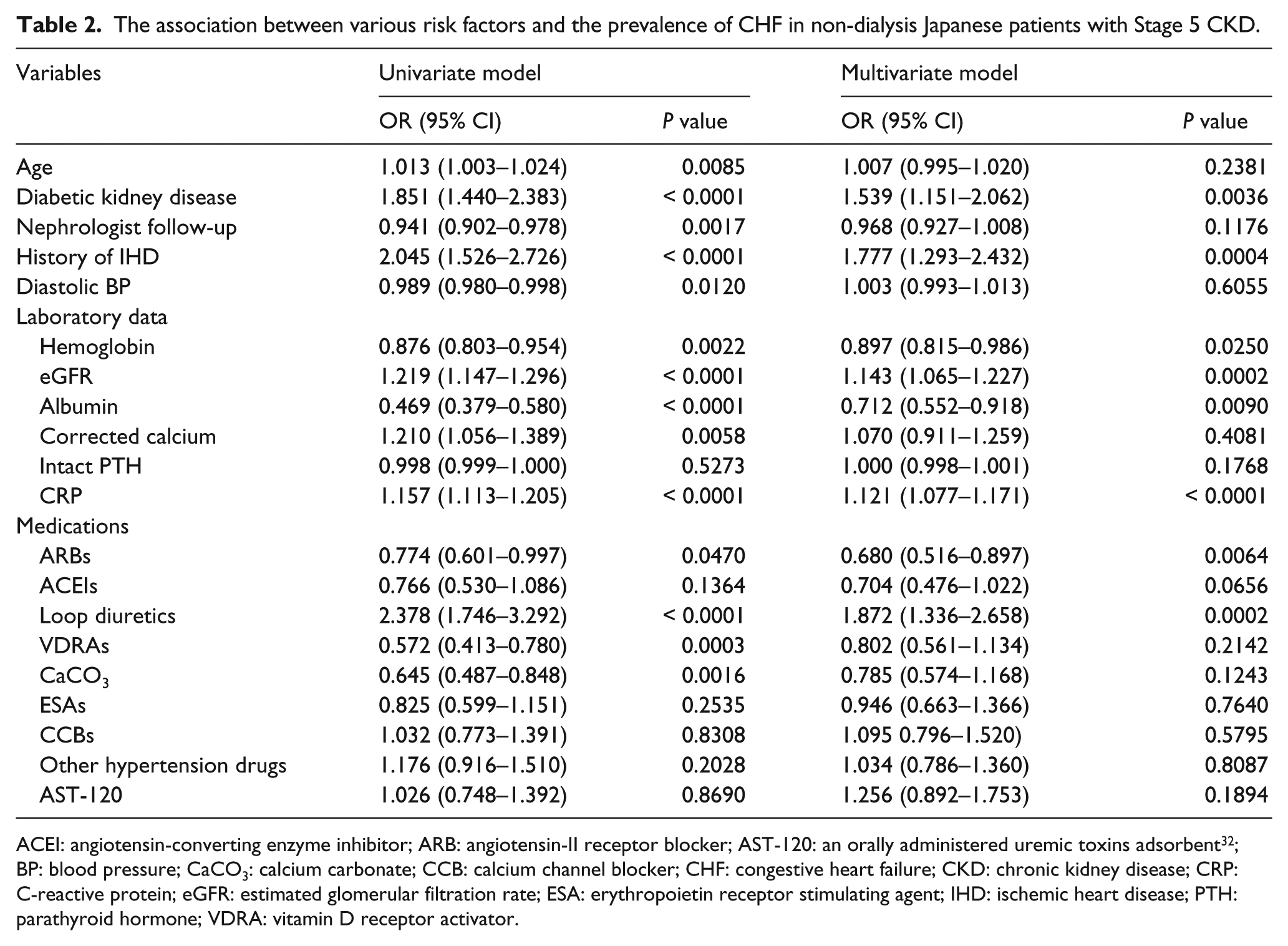
ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin-II receptor blocker; AST-120: an orally administered uremic toxins adsorbent32; BP: blood pressure; CaCO3: calcium carbonate; CCB: calcium channel blocker; CHF: congestive heart failure; CKD: chronic kidney disease; CRP: C-reactive protein; eGFR: estimated glomerular filtration rate; ESA: erythropoietin receptor stimulating agent; IHD: ischemic heart disease; PTH: parathyroid hormone; VDRA: vitamin D receptor activator.
The multivariate-adjusted logistic regression analysis revealed that, among all the medications that we examined, only ARB use was independently associated with a significantly reduced risk of dialysis-requiring CHF (OR: 0.680; 95% CI: 0.516–0.897; p = 0.0064). Though ACEI use was not independently associated with dialysis-requiring CHF (OR: 0.704; 95% CI: 0.476–1.022; p = 0.0656), a nonsignificant CHF-preventive tendency was observed. In contrast, no significant reduction in the risk of dialysis-requiring CHF was observed for the use of: VDRA, CaCO3, ESA, AST-120, CCB or the other hypertensive drugs. A significant positive correlation was also confirmed between CHF development and loop diuretic use (OR: 1.872; 95% CI: 1.336–2.658; p = 0.0002). Comorbid diabetic kidney disease (p = 0.0036), a history of IHD (p = 0.0004), high levels of serum CRP (p < 0.00001) and eGFR (p = 0.0002), low levels of serum albumin (p = 0.0090) and hemoglobin (p = 0.0250) were also independent risk factors for dialysis-requiring CHF.
Comparison of patients’ characteristics between ARB users and non-users
As only ARB was significantly associated with a decreased risk of dialysis-requiring CHF, we compared the characteristics of ARB users (940 patients (60.8%)) with ARB non-users (606 patients (39.2%)), to confirm whether any significant differences existed. As we show in Table 3, compared with non-users of ARB, the ARB users were significantly younger (66.5 ± 12.8 years versus 68.0 ± 12.4 years; p = 0.0243); had a higher frequency of diabetic kidney disease (47.1% versus 36.8%; p < 0.0001); had a shorter nephrologist follow-up period (3.48 ± 3.31 years, versus 4.03 ± 4.04 years; p = 0.0030); and had a higher frequency of CCB use (79.6% versus 70.1%; p < 0.0001), ACEI use (18.2% versus 13.2%; p < 0.0094) and other hypertensive drug use (48.3% versus 41.4%; p < 0.008).
Comparison of patients’ characteristics between ARB users and non-users. a

Data are expressed as number (%) of patients or mean ± SD.
ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin-II receptor blocker; BP: blood pressure; CaCO3: calcium carbonate; CCB: calcium channel blocker; CHF: congestive heart failure; CRP: C-reactive protein; CTR: cardiothoracic ratio; eGFR: estimated glomerular filtration rate; ESA: erythropoietin receptor stimulating agent; IHD: ischemic heart disease; PTH: parathyroid hormone; VDRA: vitamin D receptor activator.
ARB users had significantly higher levels of chloride (105.5 ± 5.8 mEq/L versus 104.1 ± 6.3 mEq/L; p < 0.0001), systolic blood pressure (153.6 ± 24.2 mmHg versus 149.5 ± 25.7 mmHg; p < 0.0016) and CTR (53.9 ± 6.5% versus 54.6 ± 6.5%; p = 0.0376). ARB users had a lower frequency of dialysis-requiring CHF, as compared to ARB non-users (18.5% versus 22.7%; p = 0.0460), despite their higher frequency of diabetic kidney disease, which was usually associated with a higher prevalence of CHF.10,11,13,15,16 Among the risk factors for CHF that were confirmed in our multivariate logistic analysis, no significant difference was seen in the frequency of IHD history and serum CRP concentration, between ARB-users and non-users.
Forrest plots of the factors associated with CHF
Figure 3 shows the log-scale Forrest plots for the significant explanatory variables in the multivariate-adjusted logistic regression analysis of risk factors for CHF. Among all CKD medications examined in this study, only ARB use was negatively and independently associated with dialysis-requiring CHF development in the Stage 5 CKD Japanese patients, although ACEI use was not significantly associated. Furthermore, the use of loop diuretics, diabetic kidney disease, a history of IHD, lower levels of serum albumin and hemoglobin, and higher levels of CRP and eGFR, were also independently associated with CHF development.
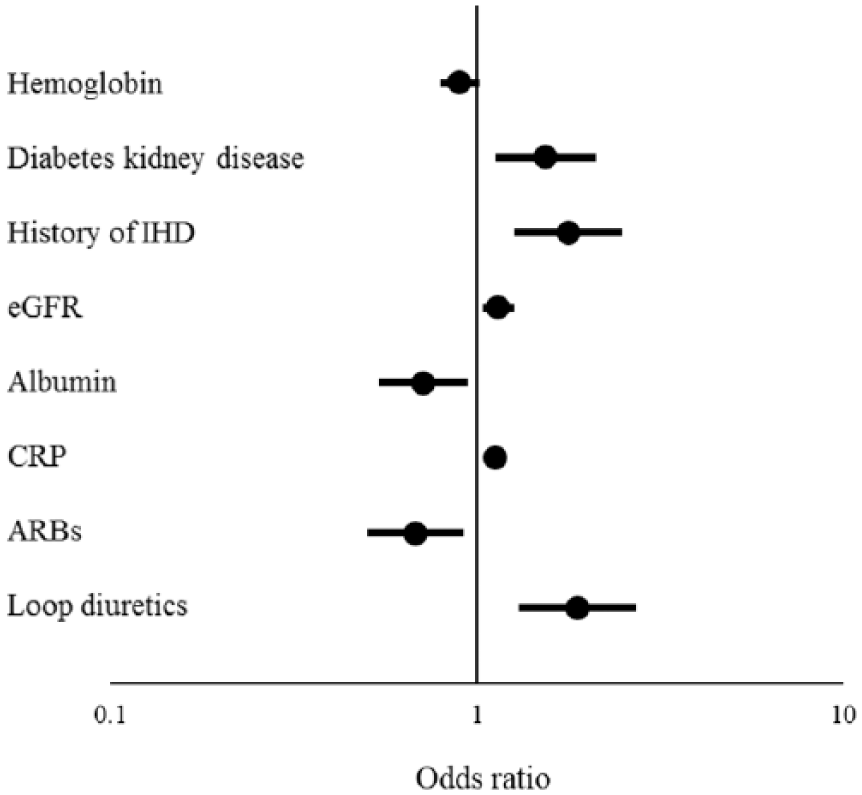
Log scale forest plots of the factors associated with CHF in non-dialysis Japanese patients with Stage 5 CKD. Factors significantly associated with CHF after adjusted multivariate analysis are shown.
Discussion
The present multicenter, retrospective, cross-sectional study showed only ARB use was significantly associated with the lower prevalence of dialysis-requiring CHF in non-dialysis Japanese patients with Stage 5 CKD among CKD medications examined in present study. The ARB users had a lower frequency of dialysis-requiring CHF, compared to ARB non-users, despite their higher frequency of diabetic kidney disease, which was usually associated with a higher prevalence of CHF.10,11,13,15,16,33 Logistic regression analysis revealed that diabetic kidney disease was also an independent risk factor for CHF, despite its higher comorbidity in the ARB user group. Therefore, we estimated that ARB use may prevent dialysis-requiring CHF in non-dialysis Japanese patients with Stage 5 CKD.
In the present study, ACEI use was not significantly associated with dialysis-requiring CHF. The maximum doses of ACEIs are permitted at a relatively lower range in Japan (enalapril, imidapril, lisinopril, trandolapril, cilazapril and captopril are used at one-quarter to one-half doses) than in Europe and USA, so ACEIs might not fully reduce CHF in Japan. For example, imidapril is used at lower doses, ranging from 2.5–10 mg in Japan, compared to relatively higher doses ranging from 5–20 mg in Europe; and ramipril, an effective ACEI for reduction of cardiovascular events, has not been used in Japan because of it giving persistent cough. Thus, different types and relatively lower doses of ACEIs used in Japan may affect the present consequence (no association between ACEI use and CHF development). Therefore, additional studies are needed to clarify the effect of these drugs on CHF development, in patients with Stage 5 CKD in Japan.
A recent meta-analysis revealed significant reduction of CHF by ACEIs in early-to-moderate CKD patients with diabetes mellitus, 12 but originally published articles34–41 included in this meta-analysis did not show a significant reduction by ACEIs, except for the HOPE study. 41 This HOPE study evaluated ramipril efficacy on CVD, but ramipril has not been approved in Japan. Thus, the results of the present study (ACEIs have non-significant reduction of CHF) are not inconsistent with previous studies. Though ARBs have been shown to have a significant reduction of CHF in early-to-moderate CKD patients with diabetes mellitus,42–44 the preventive effect of dialysis-requiring CHF in Stage 5 CKD patients by ARBs has not been reported to date. The present study revealed the possible prevention of dialysis-requiring CHF by ARBs, in CKD Stage 5 Japanese patients.
Unfortunately, the molecular mechanisms responsible for ARB-related prevention of CHF are poorly understood. In the context of tissue protection, blockade of the renin-angiotensin system using ACEIs or ARBs can prevent or reverse endothelial dysfunction and atherosclerosis, thereby reducing the risk of cardiovascular events. 45 One possible explanation is that angiotensin-II may increase the permeability of the lung vessels, 46 while another report suggests that angiotensin-II directly induces heart failure in a mouse model of heart failure. 47 Thus, it is possible that ARB use may reduce the risk of CHF via these mechanisms.
Recently, a large clinical trial involving 20,854 patients revealed the proportion of the patients with CHF at the initiation of dialysis was 19.8%, in Japan. 48 This prevalence rate was similar to our present data (20.1%); which is a relatively lower frequency, compared to both Canada (31%) 49 and USA (30.7% in the CKD without diabetes group and 52.3% in the CKD with diabetes group). 50
There was a significant trend for a stepwise increase in the prevalence of left ventricular ejection fraction (LVEF) to < 55%, corresponding to the advancement in the patients with diabetes kidney disease from CKD Stage 3 to Stage 5. 51 The percentage of LVEF in CKD patients is reported as 69.9 ± 10.4% in Stage 3; 68.2 ± 10.3% in Stage 4; and 67.1 ± 11.0% in Stage 5 pre-dialysis patients (P < 0.05, when compared with Stage 3), 52 suggesting a stepwise increase in the risk for CHF that corresponds to the stage of advancement of CKD.
Our present study also confirmed that loop diuretic users tended to start dialysis, due to CHF development. In addition, planned dialysis without obvious uremic symptoms was successfully performed more frequently in patients whom did not use loop diuretics (loop diuretics users: 42.39% versus non-users: 57.63%; p < 0.0001). Indeed, the patients with an edematous condition will frequently need loop diuretics to treat the edema and prevent CHF development. Furthermore, there was no significant difference in the use of loop diuretics between ARB users and non-users, suggesting that ARB non-users did not contain the patients with an edematous condition whom easily developed CHF.
In dialysis patients, CHF development is reported to be associated with diabetes mellitus, 33 a history of IHD, 49 anemia, 49 hypoalbuminemia, 49 and higher levels of eGFR53,54 and CRP.55–57 Our results also supported that these factors are associated with CHF development in non-dialysis Japanese patients with Stage 5 CKD; however, we did not observe any significant differences regarding the history of IHD, or hemoglobin, eGFR, albumin or CRP levels, when comparing the ARB user and non-user groups. This absence of significant differences supports the conclusion that these factors are independent risk factors for CHF development.
There are several limitations in this study:
The present study used a cross-sectional design, and we do not have any information regarding the types, dosage and duration of each medication;
We had no data from the echocardiography, such as left ventricular ejection fraction;
The low frequency of use for several medications (e.g. ACEI, VDRA, CaCO3 and AST-120) may have decreased the sensitivity of our statistical analysis; and
Finally, we did not analyze the patients’ lipid profiles or use of statins and other lipid-lowering drugs, as this information was not consistently available.
Conclusion
We found that ARB use during the pre-dialysis period is associated with a lower prevalence of CHF in non-dialysis Japanese patients with Stage 5 CKD, suggesting ARB may provide a possible prevention of dialysis-requiring CHF in non-dialysis Japanese patients with Stage 5 CKD; however, well-controlled prospective studies are needed to confirm our results, given the present study’s cross-sectional design.
Footnotes
Acknowledgements
The authors gratefully acknowledge Hiroyuki Sekihara, Moriaki Osaka, Takashi Watanabe, Hiromi Okamoto, Kazuhiko Kitano and Ryoji Kijima for data collection.
Conflict of interest
The authors declare that there are no conflicts of interest.
Funding statement
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.