
Abstract
Aims:
The renin-angiotensin-aldosterone system is important to the development of atrial fibrillation (AF). A lot of research has focused on the relationship between angiotensin-converting enzyme (ACE) insertion (I) /deletion (D) gene polymorphisms and AF, with inconsistent results. A meta-analysis was carried out to find the correlation between ACE I/D gene polymorphisms and AF.
Methods:
Data were extracted from articles published before September 2013 on ACE I/D polymorphisms and AF in Embase, PubMed, WanFangData, and China National Knowledge Infrastructure.
Results:
The recessive model found that ACE I/D gene polymorphisms were related to AF (odds ratio (OR) = 1.61, 95% confidence interval (CI) = 1.16–1.72). Subgroup analysis showed a significant association in the recessive model for Asian (OR = 1.40, 95% CI = 1.19–1.80) and Caucasian (OR = 1.42, 95% CI = 1.01–1.99) populations.
Conclusions:
ACE I/D gene polymorphisms and AF are significantly related to ethnicity. Individuals with the ACE D/D genotype appear to be at higher risk of AF.
Introduction
Atrial fibrillation (AF) is one of the most common arrhythmias seen in clinical practice. AF can cause heart failure and thromboembolism, and increase the risk of cerebral embolism. In patients aged >75 years, AF has been identified as the one of the most dangerous features of ischemic stroke. 1 The mortality of AF patients is 1.5–1.9 times higher than that of non-AF patients. 2
Recent research has shown that the renin-angiotensin-aldosterone system (RAAS) is important to the development and perpetuation of AF. Angiotensin-converting enzyme (ACE) expression is important in several pathophysiological effects of the RAAS. Li et al. 3 have reported increased ACE expression in myocardial tissue of AF patients. ACE can stimulate the expression of angiotensin II, which promotes cardiac fibroblast proliferation by enhancing atrial fibrosis.4–6 The ACE gene is located on chromosome 17q23.3, and insertion (I) /deletion (D) polymorphisms result in homozygous D/D and I/I and heterozygous I/D genotypes. 7 Higher plasma levels of ACE are associated with the D/D genotype, lower levels with the I/I genotype, and intermediate levels with the I/D genotype. 8
In recent years, the relationship between ACE I/D gene polymorphisms and incidence of AF has been a major research focus, but inconsistent results have been obtained. 9 A meta-analysis of 18 case-control studies published before 2009 with 7577 patients was performed in 2011 that showed no significant correlation between ACE I/D polymorphism and AF. 10
Further research on the association between ACE I/D polymorphisms and AF was conducted from 2010 to 2013.11–15 Therefore, we conducted a meta-analysis of all 23 studies from 1990 to 2013. We estimated the correlation of ACE I/D gene polymorphisms and AF in populations in different areas and further assessed the incidence of AF, using the recessive model of D/D vs. I/D+I/I and the dominant model of D/D+I/D vs. I/I.
Methods
Inclusion criteria
Studies were selected based on the following criteria: (1) case-control or cohort studies; (2) studies examining the relationship between ACE I/D gene polymorphisms and risk of AF; (3) patients diagnosed with AF based on history and electrocardiography (ECG); (4) diagnosis points of ECG and/or 24-hour Holter monitoring as follows: absolutely irregular ventricular rate, P wave disappearance and replacement by fluctuation with irregular size and shape (f wave), general atrial frequency >350 times/minute; and (5) both cases and controls reporting genotype or allele frequencies. The exclusion criteria were as follows: (1) studies that did not fit within the selected conditions; (2) studies with repetitive data; and (3) studies with familial AF patients.
Search strategies
Embase, PubMed, WanFangData, and China National Knowledge Infrastructure were searched for studies between 1990 and 2013, using the keywords: “angiotensin-converting enzyme,” “I/D,” “gene polymorphisms” and “atrial fibrillation.”
Data extraction
Data were extracted by scanning the title and abstract, and cross-checked by two independent investigators. Variations were resolved by a third reviewer. Data extracted included: (1) surname of first author; (2) year of publication; (3) characteristics of study population, including country, ethnicity, age and sample size; (4) ACE genotypes; and (5) genotype distribution and allele frequency for the ACE I/D polymorphisms. Research quality was assessed according to the established methods of the Cochrane Collaboration (Table 1).
Characteristics of studies included in the meta-analysis.

D: deletion; I: insertion; H-W: Hardy-Weinberg equilibrium.
Statistical analysis
In the meta-analysis, allelic (distribution of the D allelic frequency of ACE I/D gene polymorphisms), recessive (D/D vs. (I/D+I/I)), and dominant ((D/D +I/D) vs. I/I) genetic models were performed. Statistical analyses were performed with Stata 12.0 software. The observed frequencies of genotypes in the control group were tested for conformation to the Hardy-Weinberg equilibrium. 16 The relationship between ACE I/D gene polymorphisms and AF was assessed taking odds ratios (ORs) and 95% confidence intervals (CIs). If the χ2 test for heterogeneity was significant, we used a random-effects model to calculate the pooled effect, which was used to calculate within-study and between-study variance. Alternatively, a fixed-effects model would be used to calculate the pooled effect. The funnel plot and Egger’s test checked for publication bias, while the influence analyses examined whether the results were important to the meta-analysis.
Results
Eligible studies
Seventy-nine studies were selected from the databases, and 43 were excluded based on the titles and abstracts. Thirteen of the remaining 36 studies were excluded. Five of them were excluded because they were duplicate publications and three because they were meta-analyses of the relationship between the ACE I/D gene polymorphisms and AF. We excluded three articles because of missing data for the genotyping frequency and two others that had no control group. Meta-analysis of the correlation between the ACE I/D gene polymorphism and risk of AF was conducted on the remaining 23 studies, which were based on research from Japan, China, Italy, Netherlands, USA, Romania, Greece, Brazil and Turkey (Figure 1).

Flow diagram of the trial selection process.
Meta-analysis
In the 23 studies, all the genotypes in the control group fit the Hardy-Weinberg equilibrium. ACE I/D gene polymorphisms and AF had no significant correlation with allelic D frequency of ACE I/D, using the random-effects model (OR = 1.18, 95% CI = 0.99–1.40; Figure 1) and the dominant model (OR = 1.12, 95% CI = 0.98–1.52). In contrast, there was a significant association in the recessive genotype (OR = 1.61, 95% CI = 1.16–1.72; Figure 2).

Forest plots of OR with 95% CI for association between ACE I/D gene polymorphisms and AF risk (additive genetic model: D vs. I). OR: odds ratio; CI: confidence interval; ACE: angiotensin-converting enzyme; I: insertion; D: deletion; AF: atrial fibrillation.
Bias diagnostics
The publication bias of the 23 remaining studies was estimated by funnel plot and Egger’s test. In the funnel plot, there was no obvious publication bias (T = 1.71, p = 0.087). Egger’s test revealed no marked differences (p = 0.137; Figure 3), indicating that the 23 studies had no obvious publication bias.
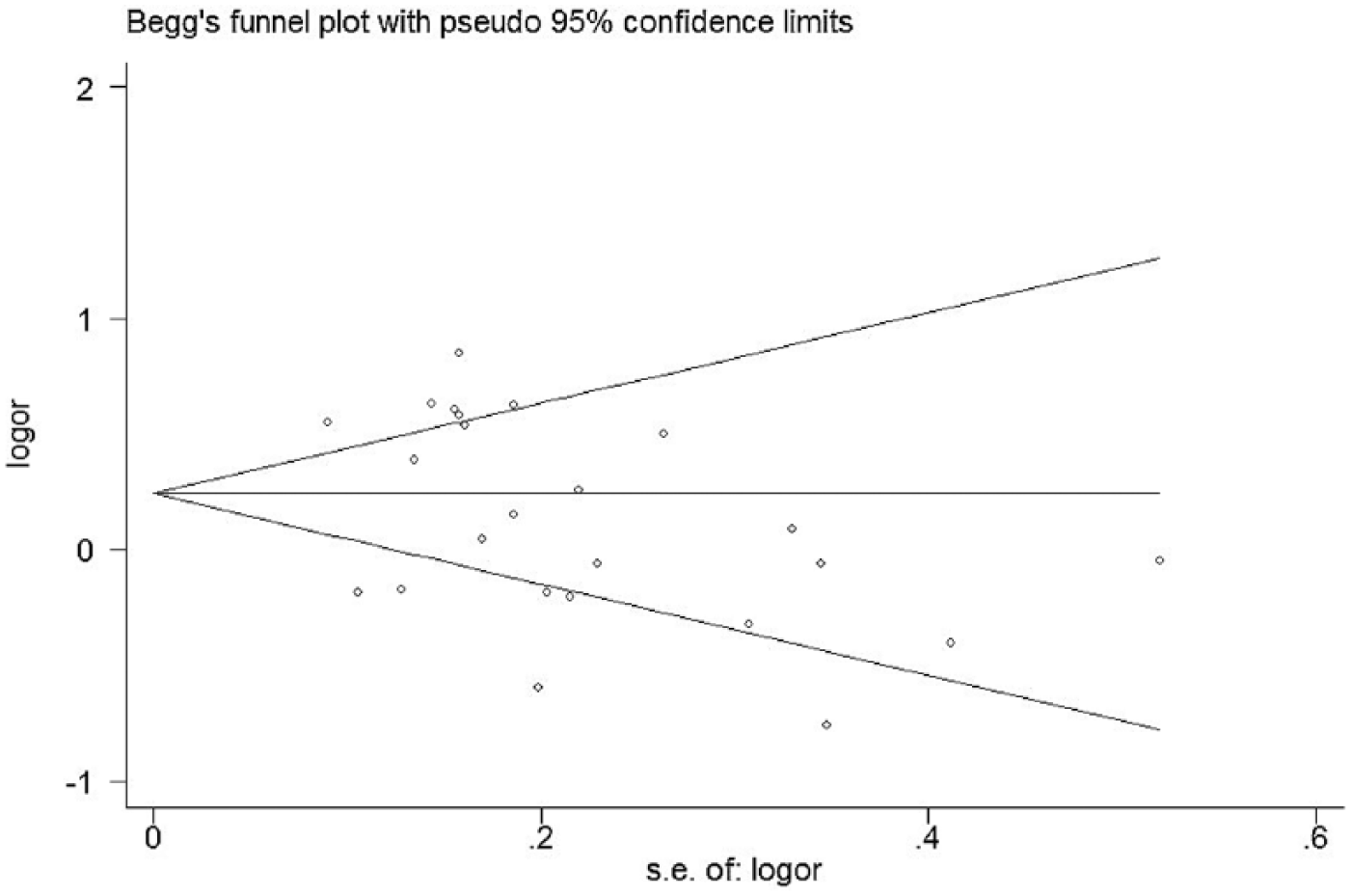
Funnel plot of data from studies on the association of AF with ACE I/D gene polymorphisms. AF: atrial fibrillation; ACE: angiotensin-converting enzyme; I: insertion; D: deletion.
Sensitivity analysis
A sensitivity analysis was conducted to establish whether the individual studies influenced the pooled ORs. We omitted one study at a time and calculated pooled ORs for the remaining studies. None of the individual studies affected pooled ORs, ranging from 0.99 (95% CI = 0.96–1.03) to 1.40 (95% CI = 1.35–1.44), for the association between ACE I/D polymorphisms and AF (Figure 4), signifying that the results of the meta-analysis were reliable and stable.

Sensitivity analysis for studies on the association of AF with ACE I/D gene polymorphisms.
Subgroup analyses
We subsequently performed subgroup analyses stratified by population ethnicity. No correlation between ACE I/D polymorphisms and AF was observed under allelic D with the random-effects model (OR = 1.16, 95% CI = 0.94–1.43), with dominance (OR = 1.19, 95% CI = 0.90–1.57), in contrast to the significant association demonstrated with the recessive model (OR = 1.40, 95% CI = 1.19–1.80) in the Asian population (Figure 5). Similarly, we found that ACE I/D gene polymorphisms were not related to AF under allelic D using the random-effects model (OR = 1.20, 95% CI = 0.88–1.63), with dominance (OR = 1.24, 95% CI = 0.82–1.88), while the recessive genotype (OR = 1.42, 95% CI = 1.01–1.99) showed significance in the Caucasian population (Figure 6).
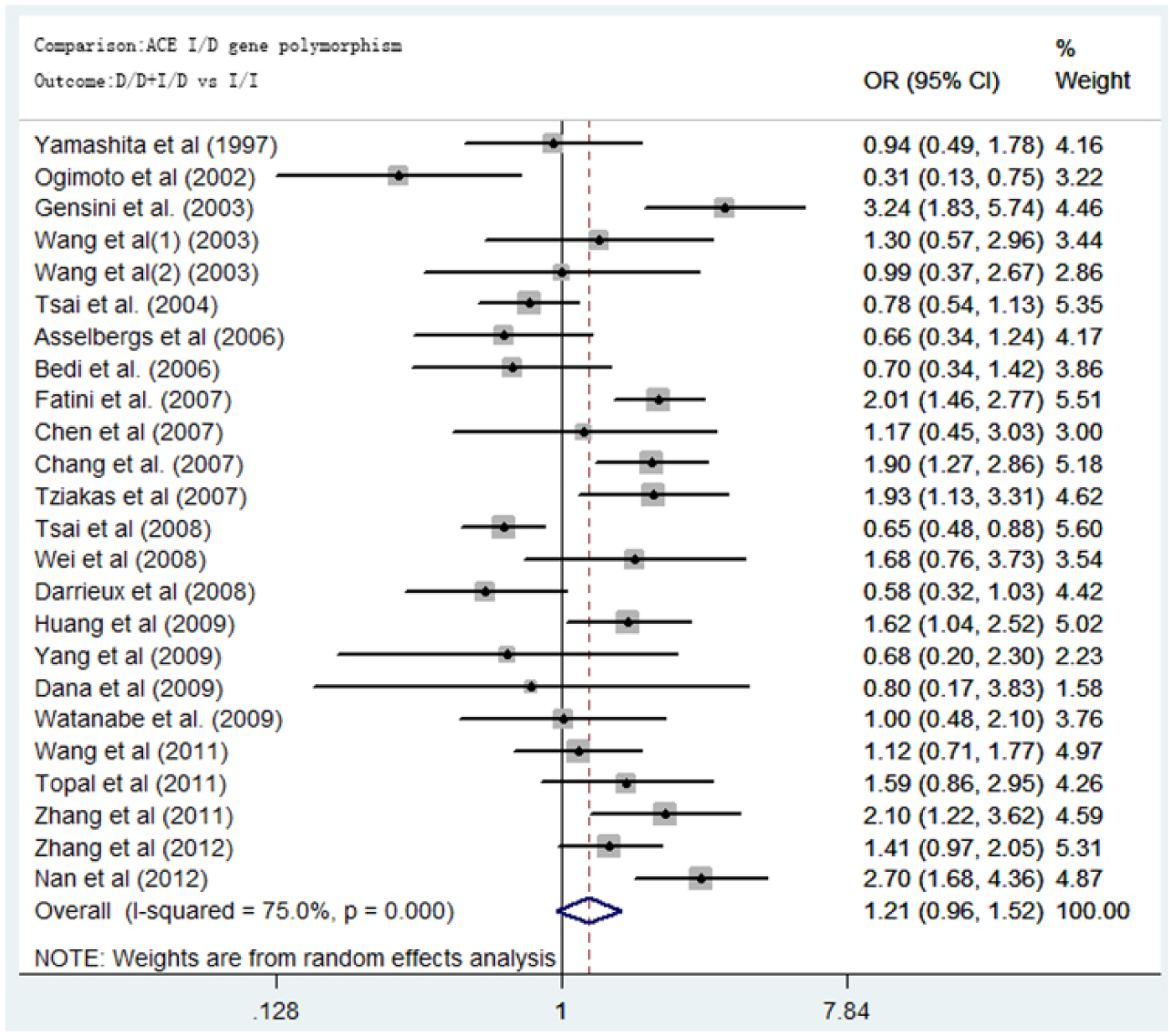
Forest plots of OR with 95% CI for the association between ACE I/D gene polymorphisms and AF risk (dominant genetic model: (D/D+I/D) vs. I/I). OR: odds ratio; CI: confidence interval; ACE: angiotensin-converting enzyme; I: insertion; D: deletion; AF: atrial fibrillation.

Forest plots of OR with 95% CI for the association between ACE I/D gene polymorphisms and AF risk (recessive genetic model: D/D vs. (I/D+I/I)). OR: odds ratio; CI: confidence interval; ACE: angiotensin-converting enzyme; I: insertion; D: deletion; AF: atrial fibrillation.
Ultimately, the subgroup analysis separated by population ethnicity showed that the relationship between the ACE I/D polymorphisms and AF had an obvious correlation only under the recessive model. The ACE I/D gene polymorphisms were associated with AF using the recessive model in the subgroup analysis.
Discussion
Our meta-analysis helped to ascertain whether ACE I/D gene polymorphisms had an apparent correlation with AF. Our results provide sufficient evidence of a relationship between the D/D genetic variant and AF. A similar association was observed in subgroup analyses stratified by ethnicity.
Our study strongly suggested that ACE D/D is a risk factor for AF. However, a meta-analysis in 2011 showed that there was no significant evidence to show that ACE I/D polymorphism was related to AF. 10 There were 7577 patients in the 2011 analysis of 18 case-control studies, and the additive genetic model used D/D vs. I/I. However, our analysis included 23 case-control studies with 9262 patients, and the additive genetic model was D vs. I. By analyzing more cases and using a different method, our results show that the ACE I/D gene polymorphism is related to AF.
Recent research has shown that activation of RAAS is important for AF.33–35 RAAS is the key mechanism of atrial remodeling, which is believed to be the main cause of AF. The ACE I/D gene polymorphisms are related to the activity of angiotensin, which is the main effective component of the RAAS. ACE converts angiotensin I to angiotensin II, which may promote cardiomyocyte hypertrophy, 36 apoptosis 37 and fibrosis,38,39 and lead to simulated AF. A previous study has linked the ACE D/D genotype with higher plasma levels and increased ACE activity. 8 Recent clinical evidence shows that RAAS inhibition with ACE inhibitors and/or angiotensin receptor blockers suppresses left ventricular dysfunction and hypertrophy in AF patients. 40
Theoretically, the ACE D/D genotype may promote angiotensin II production and atrial fibrosis through increasing ACE activity, leading to atrial structural remodeling and promotion of AF. Consistent with this assumption, our results showed that the ACE D/D genotype is significantly related to AF. However, it is not the only reason for development of AF. There are many genes in the RAAS, and some studies have shown that other gene polymorphisms in the RAAS are related to AF.9,25,26 Future research can investigate the association between the RAAS and AF.
Subsequent sensitivity analysis showed that, even after excluding one study at a time and calculating pooled ORs for the remaining studies, the results of the main meta-analysis were reliable and stable. The funnel plot and Egger’s test indicated no significant publication bias. Subgroup analysis by ethnicity was performed to investigate the different causes of AF among distinct populations.
It should be noted that our study had several limitations. First, we did not consider other influences on AF, such as age, smoking, hypertension, and other cardiovascular diseases, that could have led to potential bias. Second, ACE I/D gene polymorphism is not the only cause of AF, and gene-gene and gene-environment interactions also play an important role in the development and perpetuation of AF. Owing to the lack of related data, these interactions were not included in our study. Finally, meta-analysis is a retrospective research technique, and it has methodological defects, therefore, our data should be interpreted with caution.
Conclusions
Our results provide sufficient evidence to show that ACE I/D gene polymorphisms are related to AF. Subgroup analysis revealed a significant correlation in different ethnic populations in the recessive model. Comprehensive meta-analysis further demonstrated that the D/D genetic variant is highly associated with AF. However, ACE I/D gene polymorphisms are not the only cause of AF, and further studies are essential to elucidate the potential relationship between the RAAS and AF.
Footnotes
Conflict of interest
None declared.
Funding
This work was supported by grants from the Association Foundation Program of Yunnan Provincial Science and Technology Department and Kunming Medical University (no. 2012FB077).