
Abstract
Background and objective:
The gene encoding angiotensin-converting enzyme (ACE) has been implicated in the development of several malignancies. We aimed to meta-analyze the association of ACE gene insertion/deletion (I/D) polymorphism with digestive cancer risk and seek possible sources of between-study heterogeneity.
Methods:
Two authors independently assessed eligibility of each retrieved publication and gathered relevant data. Risk estimates were expressed as odds ratio (OR) and 95% confidence interval (CI).
Results:
Sixteen publications were qualified for analysis, involving 2903 digestive cancer cases and 10,833 controls. Overall analyses failed to show any significance for digestive cancer risk. There was moderate heterogeneity and lower publication bias for overall comparisons. In subgroup analyses, ACE gene II genotype was associated with a 15% reduced risk (OR=0.85, 95% CI: 0.57–1.27, p=0.434) for gastric cancer, but a 16% increased risk (OR=1.16, 95% CI: 0.89–1.52, p=0.273) for colorectal cancer. By source of controls, the I allele appeared to be a protective factor against digestive cancer in population-based studies (OR=0.87, 95% CI: 0.75–1.00, p=0.055) but a risk-conferring factor in hospital-based studies (OR=1.17, 95% CI: 1.01–1.35, p=0.033).
Conclusion:
Our findings suggested that ACE gene I allele might be a protective factor against gastric cancer, necessitating further confirmation in large, population-based studies.
Introduction
Angiotensin-converting enzyme (ACE, gene ID: 1636) is a zinc-dependent carboxypeptidase, and its expression is observed in several malignancies. 1 Accumulating data support that ACE inhibitors can suppress angiogenesis and tumor growth, especially for tumors originating from digestive organs.2-4 In humans, circulating ACE concentration is well known to have a substantial heritable component, with epidemiological investigations estimating that about half of the explained variation could be attributable to a single Alu element insertion/deletion (I/D) polymorphism within 16th intron of the ACE gene.5,6 The association of ACE gene I/D polymorphism with cancer susceptibility has been widely evaluated; however the results are not often reproducible.7,8 For instance, a previous study in a European population documented that ACE gene II genotype was significantly associated with a reduced risk of having gastric cancer relative to the DD genotype homozygotes, 9 and contrastingly carriers of II genotype were at an increased risk for gastric cancer in a Japanese population. 10 However, other studies have identified a nearly neutral contribution of ACE gene I/D polymorphism to gastric cancer risk.11,12 The most likely interpretation for such divergences is genetic heterogeneity between different populations, a possible confounding factor in any attempt to map loci for cancer. Another possible interpretation is that some individual studies are often underpowered to detect a true effect estimate. These two aspects justify the necessity of carrying out a meta-analysis. It was therefore our objective to gather available publications to systematically meta-analyze the association of ACE gene I/D polymorphism with digestive cancer risk from the current literature, and meanwhile seek possible reasons to explain between-study heterogeneity.
Methods
Searching publications
To ensure a comprehensive identification of all relevant publications, we accessed two electronic databases, MEDLINE and EMBASE, on 23 January 2015 using the following key words: ‘angiotensin converting enzyme’ or ‘angiotensin-converting enzyme’ or ‘angiotensin I converting enzyme’ or ‘ACE’ or ‘ACE1’ in the ‘Abstract’, in combination with ‘gastric’ or ‘stomach’ or ‘colorectal’ or ‘colon’ or ‘rectal’ or ‘esophageal’ or ‘liver’ or ‘hepatic’ or ‘hepatocellular’ or ‘pancreatic’ or ‘gallbladder’ or ‘biliary’ or ‘gall bladder’ or ‘gallbladder’ in the ‘Title’. The language of publications was restricted to English and the study subjects must be human beings. To identify additional publications of interest, we conducted a manual scanning on the reference lists of potential reviews and major original articles. According to the guidelines in the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement, 13 we formulated the protocols and standards of the current meta-analysis (see supporting materials: The PRISMA Checklist).
Assessing eligibility
Two of our authors (HY and CC) independently assessed the eligibility of each retrieved publication using pre-defined criteria as addressed below. A preliminary screening was targeted on the title and/or abstract of each publication to assess whether a genetic association was addressed between ACE genetic polymorphisms and any type of digestive cancer, and if it was not sure, the full text was checked further. Any uncertainty was adjudicated by a discussion and we reached a 100% agreement over eligibility. In addition, we checked whether the same study group was involved in more than one publication, and if so the largest study in sample size was reserved.
Criteria
Both inclusion and exclusion criteria were adopted to determine final qualified publications. All inclusion criteria should be satisfied, that is, (a) clinical endpoints should be any type of digestive cancer; (b) enrollment of study subjects should be described clearly; (c) both digestive cancer cases and cancer-free controls should be involved; (d) ACE gene I/D polymorphism should be genotyped and its genotype or allele distributions should be provided between cases and controls.
Any one of the following criteria was sufficient for exclusion: (a) conference abstracts or proceedings; (b) case reports or series; (c) lack of control group; (d) investigations on cancer severity, progression or survival; (e) the non-English publications.
Gathering data
Two authors (HY and CC) independently gathered relevant demographic and genetic data from all qualified publications and typed them into a predetermined data collection file designed by all contributing authors, followed by careful comparisons. The gathered data included: the first author’s name, publication year, ethnicity of study subjects, type of digestive cancer, study design, source of control group, matched status, valid sample size of cases and controls, genotype or allele distributions of ACE gene I/D polymorphism between the two groups, mean age and male percentage within each study group. In this meta-analysis, cases and controls were defined to be matched if there were relevant descriptions at the enrollment of study subjects or there was no statistically significant difference in age and/or gender between cases and controls (p<0.05) in case of no relevant descriptions.
Data analyses
Data analyses were completed with STATA software version 12.0 under Windows (StataCorp, College Station, Texas).
We quantified magnitude of the association between ACE gene I/D polymorphism and digestive cancer risk under assumption of allelic, homozygous genotypic and dominant models as odds ratio (OR) and its 95% confidence interval (95% CI) in a random-effects model using the DerSimonian and Laird method. 14 Hardy–Weinberg equilibrium was examined by Chi-squared test in the controls at a significance level of 1%.
To assess the degree of heterogeneity between studies, we employed the index I2 in percentage to define the percentage of the observed between-study variability that is due to heterogeneity rather than chance. Based on previous experience, we selected the cutoff value of 50% as a significance threshold with higher values paralleling stronger evidence of heterogeneity.
We stratified all qualified studies according to ethnicity, cancer type, study design, source of controls and matched status to assess whether risk estimates were homogeneous between subgroups. In addition, for the other continuous variables such as age and male, we modeled them in a meta-regress analysis to examine whether they can affect the ACE-cancer association based on regression coefficients and p-values.
We further used the Begg’s funnel plot and the Egger’s test at a significance level of 10% to assess publication bias. 15 In addition, we used the trim and fill method to estimate the number of potentially missing studies that was required to make the filled funnel plot symmetrical.
Results
Study descriptions
An initial search retrieved 231 potentially relevant publications, and after assessing eligibility and applying inclusion/exclusion criteria, a total of 16 qualified publications were left for the final analysis.9-12,16-27 The publication year was from 2001 16 to 2014. 27
Study characteristics
Out of 16 qualified publications, there were 16 available study groups with 2903 digestive cancer cases and 10,833 controls. The baseline characteristics of all study groups are shown in Table 1. By ethnicity, nine groups involved populations of White background and seven groups of Asian background. By cancer type, six study groups examined gastric cancer, five study groups examined colorectal cancer, two study groups examined hepatocellular carcinoma and one study group examined cancer of esophageal, gall bladder and pancreatic, respectively. By study design, 14 study groups were conducted in a retrospective design and two study groups in a prospective design. By source of the controls, there were seven and nine study groups with population-based and hospital-based controls, respectively. By matched status, eight study groups had cases and controls matched on age and/or gender. The genotype distributions of ACE gene I/D polymorphism satisfied Hardy–Weinberg equilibrium at a significance level of 1% for all study groups. The frequency of ACE gene I allele ranged from 30.98% to 72.22% in digestive cancer cases and from 27.45% to 66.85% in controls.
The baseline characteristics of study groups qualified in this meta-analysis.

NA: not available.
Overall association
When all study groups were analyzed together, no significance was observed for overall digestive cancer risk under allelic, homozygous genotypic and dominant models, with the I allele (vs. D allele) (Figure 1), II genotype (vs. DD genotype) and II plus ID genotypes (vs. DD genotype) of being 1.02-fold (95% CI: 0.91–1.15), 1.10-fold (95% CI: 0.83–1.46) and 1.10-fold (95% CI: 0.86–1.39) more likely to be digestive cancer, respectively. There was moderate evidence of heterogeneity (I2=64.4%, 70.6% and 72.1%).

Forest plot of ACE gene I allele vs. D allele in association with overall digestive cancer risk.
Subgroup analyses
Table 2 summarizes the results of subgroup analyses according to cancer type, ethnicity, study design, source of the controls, matched status and sample size, respectively. Stratifying study groups by cancer type indicated potential existence of tumor heterogeneity, as the II genotype (vs. DD genotype) associating with a 15% reduced risk (OR=0.85, 95% CI: 0.57–1.27, p=0.434) for gastric cancer, but a 16% increased risk (OR=1.16, 95% CI: 0.89–1.52, p=0.273) for colorectal cancer, albeit no observable significance, with improved heterogeneity. There were no material changes in risk estimates between populations of Asian and White backgrounds, between large (total sample size ⩾300) and small (total sample size <300) studies, between retrospective and prospective studies. Here, the cutoff of 300 for sample size is mainly based on the number of eligible studies in each side.
Subgroup analyses of ACE gene I/D polymorphism with digestive cancer risk.
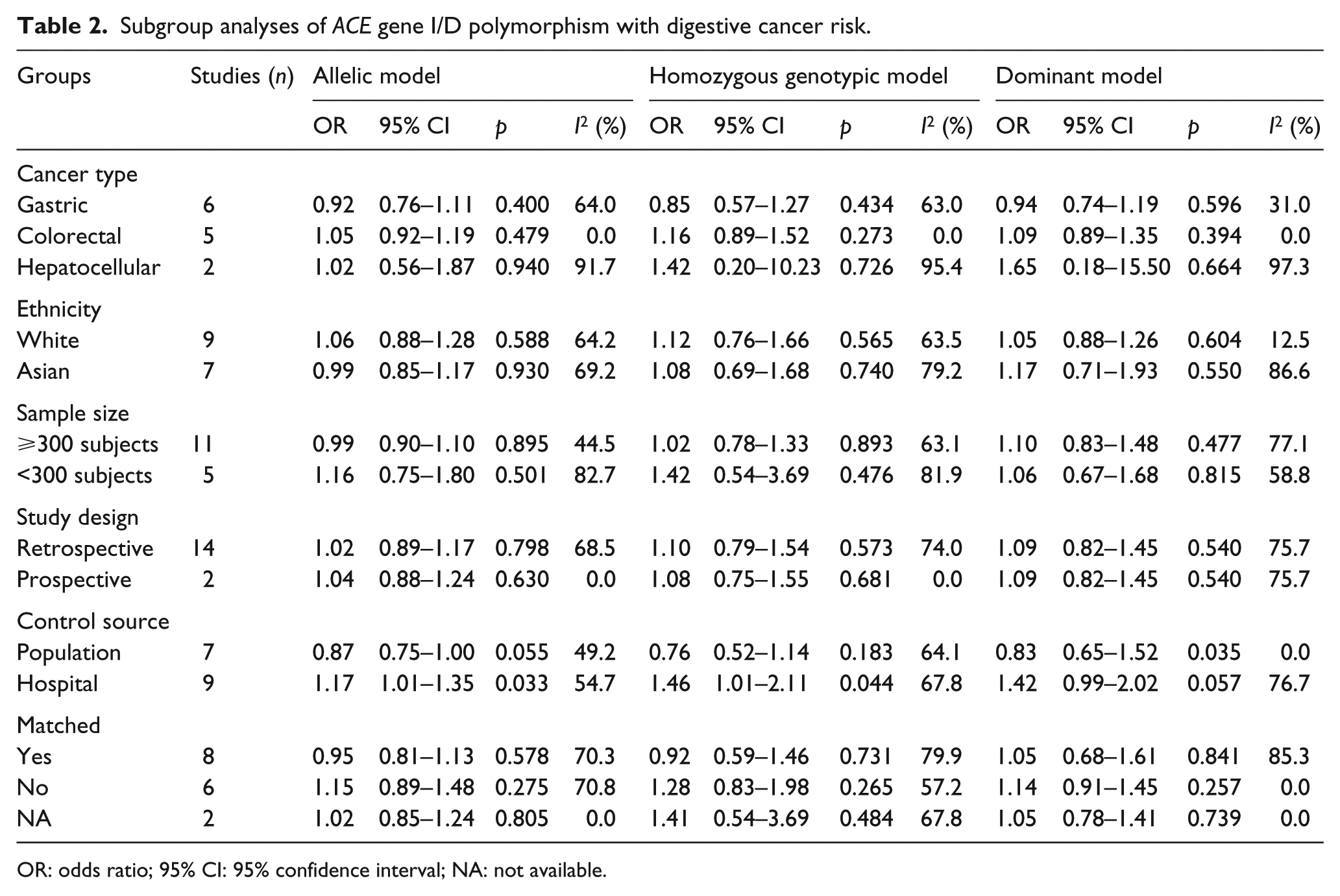
OR: odds ratio; 95% CI: 95% confidence interval; NA: not available.
Of note, difference in source of the controls was a confounding risk factor for the association of ACE gene I/D polymorphism and digestive cancer risk. For instance, the I allele appeared to be a protective factor against digestive cancer in population-based studies (OR=0.87, 95% CI: 0.75–1.00, p=0.055) but a risk-conferring factor in hospital-based studies (OR=1.17, 95% CI: 1.01–1.35, p=0.033) relative to the D allele.
Meta-regression analyses
To examine the confounding impact of age and gender, we modeled them in a meta-regression analysis respectively under three genetic models, and unfortunately no statistical significance was reached for both variables (p>0.10).
Publication bias
For allelic, homozygous genotypic and dominant models, there was a low probability of publication bias, as reflected by the Begg’s funnel plots and Egger’s tests (p=0.513, 0.307 and 0.413, respectively) (Figure 2). In addition, the trim and fill method indicated that three missing studies were required to make the filled funnel plots symmetrical under allelic and homozygous genotypic models, respectively (Figure 2).

The Begg’s funnel plots (the left) and the filled funnel plots (the right) for the association between ACE gene I/D polymorphism and overall digestive cancer risk.
Discussion
In this meta-analysis, we aimed to examine the association of ACE gene I/D polymorphism with digestive cancer risk by means of a comprehensive meta-analysis. On the basis of 16 qualified publications and a total of 13,736 study subjects, our findings were indicative of potential existence of tumor heterogeneity between gastric cancer and colorectal cancer. Moreover, the source of the controls was identified as a potential contributor to explain evident heterogeneity.
Tumor heterogeneity is not an uncommon phenomenon for many tumors, as tumor cells of different regions can exhibit distinct morphological and phenotypic profiles. 28 This phenomenon occurs both between tumors and within tumors. Digestive cancer is a group of heterogeneous tumors with different pathogeneses. 1 As exemplified in the current meta-analysis, we observed a completely opposite association of ACE gene I/D polymorphism with gastric cancer and colorectal cancer, irrespective of the genetic modes of inheritance, although no statistical significance was attained due to the limited number of individually underpowered studies involved. Previous investigations supported the functional relevance of ACE gene I/D polymorphism and its expression, with the II, ID and DD genotypes corresponding to the lowest, intermediate and highest ACE concentrations, respectively.29,30 It is a reasonable expectation that if involved, the ACE gene II genotype might be a protective factor for the development of cancer. Unexpectedly, we found that carriers with the II genotype were at an increased risk for colorectal cancer compared with those homozygous for the DD genotype, and this effect was unlikely explained by heterogeneity, possibly due to a compensatory mechanism to antagonize the lower synthesis of ACE, which is beyond the capability of this meta-analysis. Considering the multifactorial and heterogeneous nature of cancer, there is a necessity to establish a catalogue of driver genes or loci for each tumor type.
As an extension of a recent meta-analysis by Liu et al., 31 we identified the source of the controls as a potential contributor to account for strong evidence of heterogeneity in this meta-analysis. Ruano-Ravina and colleagues have done a methodological comparison between population-based and hospital-based controls on lung cancer risk, and highlighted obvious differences between the two sources of controls in risk estimates. 32 Generally, case-control comparisons are likely biased when controls are selected from an ill-defined study background and consequently do not represent the exposure experience of the true source population. Hospital-based studies differ from population-based studies because the study background is defined secondarily to the identification of cases. 33 By contrast, a population-based case-control study is based on a well-defined source population and the controls consist of random subjects without the disease of interest from the source population, which per se can reduce selection bias. 34 As expected in subgroup analysis of this meta-analysis, we observed a reduced risk of digestive cancer for the II genotype carriers in population-based case-control studies, in agreement with the biological implication of ACE gene I/D polymorphism in its expression profile. As only seven of 16 qualified studies enrolled controls from a population-based source, future large, prospective studies are warranted to confirm the contribution of this polymorphism to digestive carcinogenesis and other solid tumors.
There were several limitations to the present meta-analysis. First, only published articles written in English language were retrieved for analysis, which might introduce a potential selection bias. Second, this meta-analysis was not based on individual participant data of each qualified study, limiting further gene-to-environment interaction analysis. Third, only one polymorphism I/D in ACE gene was analyzed and other functional polymorphisms such as A-240T in the promoter region were not covered due to the insufficient available data. In addition, the I/D polymorphism exhibited wide divergences in allele frequency across studies, indicating the presence of allele heterogeneity. Fourth, circulating ACE concentration was not provided by all qualified studies, which precluded genotype–phenotype correlation analysis and further Mendelian randomization analysis. Fifth, the power of some subgroup analyses may be lower due to the limited studies of small sample sizes involved.
To sum up, through a meta-analysis of 16 qualified publications and a total of 13,736 study subjects we suggested that the ACE gene I allele might be a protective factor against gastric cancer, necessitating further confirmation in future large, population-based studies. If successfully confirmed, ACE gene I/D polymorphism might be a logical targeted biomarker for cancer therapeutic intervention.
Footnotes
Conflicts of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.