
Abstract
Background:
Reduction of blood pressure and proteinuria by blockade of the renin-angiotensin-aldosterone system (RAAS) has been the cornerstone of renoprotective intervention for patients with chronic kidney disease (CKD) for many years.
Aims:
The aims were to check the use of angiotensin converting enzyme inhibitors (ACEIs) and/or angiotensin II receptor blockers (ARBs) in CKD patients.
Methods:
This was a retrospective, cross-sectional study analysing data from medical records of patients who received specialist care in 1996, 2001, 2006, 2011 in the Outpatient Unit.
Results:
The numbers of CKD subjects included in the four independent surveys were as follows: 190, 490, 1799, 1696. The usage of RAAS blocking agents overall increased significantly in subsequent years as follows: 25, 49, 63, 74%. Patients with proteinuria and cardiovascular complications and/or diabetes were receiving RAAS blocking agents more commonly than others. The use of ACEI and/ or ARB in stage 4–5 CKD increased in subsequent years. In 2011 dual RAAS blockade was used in 10% CKD patients overall and 19% patients presented proteinuria.
Conclusion:
The use of RAAS blocking agents were increasing in CKD patients under specialist care between 1996–2011. The quality of the management was gradually improved.
Introduction
Reduction of blood pressure and proteinuria by blockade of the renin-angiotensin-aldosterone system (RAAS) has been the cornerstone of renoprotective intervention for patients with chronic kidney disease (CKD) for many years. 1 Angiotensin converting enzyme inhibitors (ACEIs) and angiotensin II receptor blockers (ARBs) have well documented effects in delaying the progression of both diabetic and non-diabetic CKD. 2 For this reason, national guidelines recommend that pharmacologic therapy for CKD patients with proteinuria and hypertension should include an ACEI or ARB. 3 Little is known about the adherence to these guidelines and methods of implementation of such therapy. The available studies showed that despite these known benefits, inadequate numbers of persons with clinical indications for RAAS blockade use an ACEI or ARB.4,5 To shed more light on this issue we performed four independent retrospective surveys to check the use of RAAS blocking agents in CKD patients under specialist care during the last 15 years and to find out how these treatments were managed.
Methods
The study was performed at the Outpatient Unit of the Department of Nephrology Transplantology and Internal Medicine, Medical University of Gdansk, Poland. It was a retrospective, cross-sectional study analysing data from medical records in four independent surveys. Data were collected from January 2012–April 2012. The authors analysed 1952 medical records of all non-dialysed and non-transplanted adults patients treated in the unit. Four independent cross-sectional analyses at four different time-points were performed. The first survey analysed data from 1996. The second, third and fourth surveys analysed data of patients who received outpatient care in 2001, 2006 and 2011 respectively. Data from the first visit in the year was gathered for the analysis. The authors analysed demographic status and clinical information including renal, cardiovascular and diabetic status as well as current antihypertensive treatment. Data concerning serum creatinine and potassium concentration referred to a single assessment, the first in the year. Serum potassium above 5.1 mmol/l was treated as hyperpotassaemia. In particular, the use of RAAS blocking agents was analysed. Subgroup analysis was performed to check the usage of ACEIs and ARBs in combination with the presence of proteinuria, cardiovascular complications and/or diabetes, CKD stage, sex and age. Dosing of ACEIs and ARBs was determined as the % of patients receiving drugs in the following ranges of their maximal doses: <25%; 25–50%; 51–75%; >75%. The implementation of a combination RAAS blockade including simultaneous usage of an ACEI and ARB was analysed. We checked also the use of diuretics in addition to RAAS blocking agents as well as the presence of hyperkalaemia in subjects treated with ACEI and/or ARB.
Study population
Non-dialysed, non-transplanted adults patients with CKD diagnosed according to the Kidney Disease Outcomes Quality Initiative (KDOQI) definition were included in the study. 6
Aims
The aims were to check the use of RAAS blocking agents i.e. ACEIs and/or ARBs in CKD patients. The secondary goal was to illustrate the management of RAAS blockade i.e. dosing, combination with other drugs, use of ACEI and ARB in different stages of CKD, presence of hyperkalaemia.
Definitions
CKD was diagnosed as a glomerular filtration of less than 60 ml/min per 1.73 m2 or the presence of kidney damage for more than three months, according to KDOQI guidelines. 6 The estimated glomerular filtration rate (eGFR) was calculated from serum creatinine using the Modification of Diet in Renal Disease Study Group (MDRD) formula 7 . Hypertension was defined as systolic blood pressure (BP)≥140 mm Hg and/ or diastolic BP≥90 mm Hg or undergoing current treatment with antihypertensive drugs.
Statistics
Categoric and continuous variables are expressed as frequencies (%) and mean±standard deviation (SD), respectively. A χ2 test was used for categorical variables, while analysis of variance (ANOVA) was used for continuous variables. In secondary analyses patients were stratified according to age, sex, CKD stage, diagnosis, cardiovascular complications and/or diabetes presence.
Results
Demographic and clinical characteristic
Overall 193, 500, 1952 and 1706 patients were screened using their medical records from 1996, 2001, 2006 and 2011, respectively. The number of CKD subjects included in the four independent surveys were as follows 190, 490, 1799 and 1696. The general characteristics of the participants are summarised in Table 1. An increasing number of patients were diagnosed as having hypertensive nephropathy (p<0.001) and diabetic nephropathy (p<0.001). The average eGFR decreased significantly in subsequent years and was as follows 67, 56, 54 and 51 ml/min (p<0.001). There was a remarkable change in the average age of CKD patients which was as follows: 43.8, 47.2, 54.9 and 62.7 (p<0.001). The number of patients who were more than 65 years of age increased significantly from 8.5% in 1996 (up to 52% in 2011 (p<0.001). The number of patients with cardiovascular disease increased significantly as well (p<0.001).
General characteristics of participants.

CKD: chronic kidney disease; eGFR: estimated glomerular filtration rate.
p<0.001.
Usage of RAAS blockade
The usage of RAAS blocking agents increased significantly in subsequent years (p<0.001) (Figure 1). ACEIs were used in 25.26%, 46.73%, 50.69% and 46.34% in 1996, 2001, 2006 and 2011, respectively. ARBs were not used in 1996 and significant increments in their usage were observed in subsequent years as follows: 1.02%, 4.28% and 17.92%. In the subgroup with proteinuria more patients received RAAS blocking agents (Figure 2). Overall 78.46% proteinuric subjects were treated with ACEIs and/or ARBs in 2011 as compared to 72.99% CKD patients without proteinuria (p<0.05) (Table 2). Similarly, men as well as patients with cardiovascular complications and/or diabetes were receiving RAAS blockade agents more commonly. There were no difference in the use of RAAS blocking agents according to age (Table 2).

The use of renin-angiotensin-aldosterone system (RAAS) blocking agents (%) in chronic kidney disease (CKD) patients. ACEI: angiotensin converting enzyme inhibitor; ARB: angiotensin II receptor blocker.

The use of renin-angiotensin-aldosterone system (RAAS) blocking agents (%) in chronic kidney disease (CKD) patients with proteinuria. ACEI: angiotensin converting enzyme inhibitor; ARB: angiotensin II receptor blocker.
The use of renin-angiotensin-aldosterone system (RAAS) blocking agents overall (%) according to age, gender, presence of cardiovascular disease and/or diabetes, presence of proteinuria.

Significant difference: women vs men (–): p<0.05.
Significant difference: women vs men: p<0.001.
Significant difference: CV/DM (+) vs CV/DM (–): p<0.01.
Significant difference: CV/DM (+) vs CV/DM (–): p<0.001.
Significant difference: proteinuria (+) vs proteinuria (–): p<0.001.
Significant difference: proteinuria (+) vs proteinuria (–): p<0.05.
CV: cardiovascular complications; DM: diabetes.
Usage of RAAS in different stages of CKD
Subgroup analysis revealed that usage of RAAS blocking agents overall increased in all CKD stages. In stages 4–5 of CKD the % of patients receiving an ACEI and/or ARB increased in subsequent years and was as follows: 16.7%, 36.8%, 64.9% and 66.9% (p<0.001) . Nevertheless, use of ACEIs and/or ARBs was lower among patients in stage 4–5 CKD compared with patients in stage 1–2 CKD and stage 3 CKD in 2001, 2006 and 2011 (Table 3).
The use of renin-angiotensin-aldosterone system (RAAS) blocking agents overall (%) according to chronic kidney disease (CKD) stages.
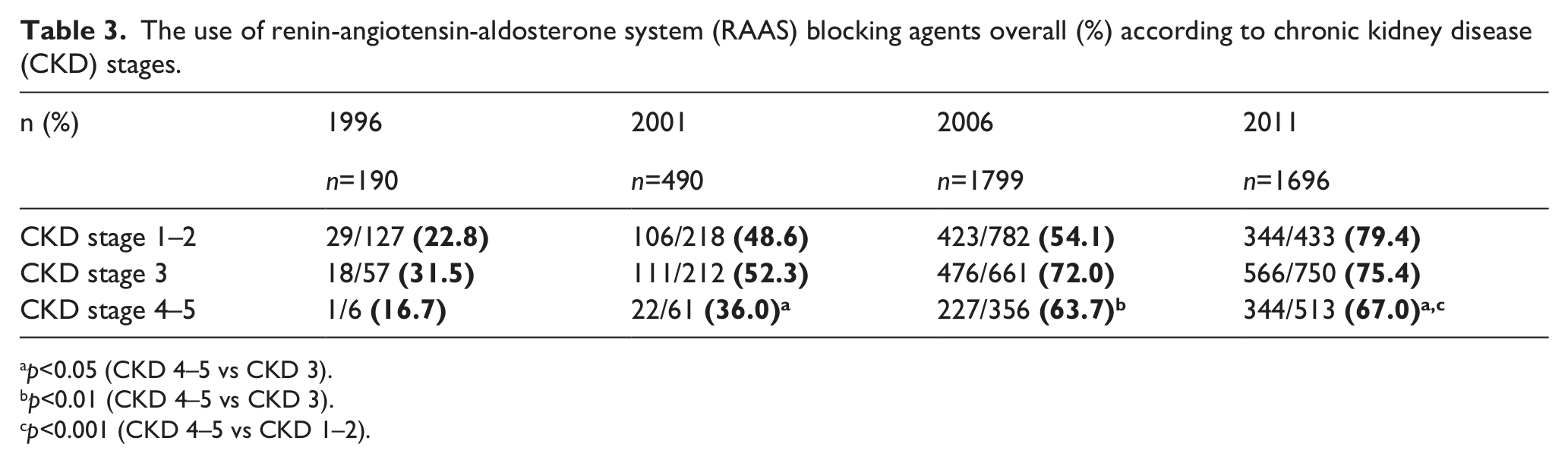
p<0.05 (CKD 4–5 vs CKD 3).
p<0.01 (CKD 4–5 vs CKD 3).
p<0.001 (CKD 4–5 vs CKD 1–2).
Dosing of RAAS blocking agents
The tendency to increase doses of ACEIs and ARBs used by CKD patients was observed in subsequent years. The percentage of patients receiving ACEIs in the range 76–100% of their maximal doses increased significantly (p<0.001) and was as follows: 4.2%, 7.4%, 14.7% and 48.2%. In 2011 most patients treated with ACEIs received these agents in the highest range of doses. Simultaneously, the % of patients receiving an ACEI below 25% of the maximal dose decreased in subsequent years (p<0.001) (Figure 3).

Dosing of angiotensin converting enzyme inhibitor (ACEI) as the % of patients receiving these drugs in different ranges of their maximal doses.
There was also a significant increment in dosing of ARBs. The percentage of patients receiving ARB in the range above 75% of their maximal doses increased significantly between 2006–2011 from 11.9% to 22.7% (p<0.001). Nevertheless, most patients treated with ARB were receiving these drugs in the range below 25% and 25–50% of their maximal doses in 2001 and 2006–2011 respectively (Figure 4).
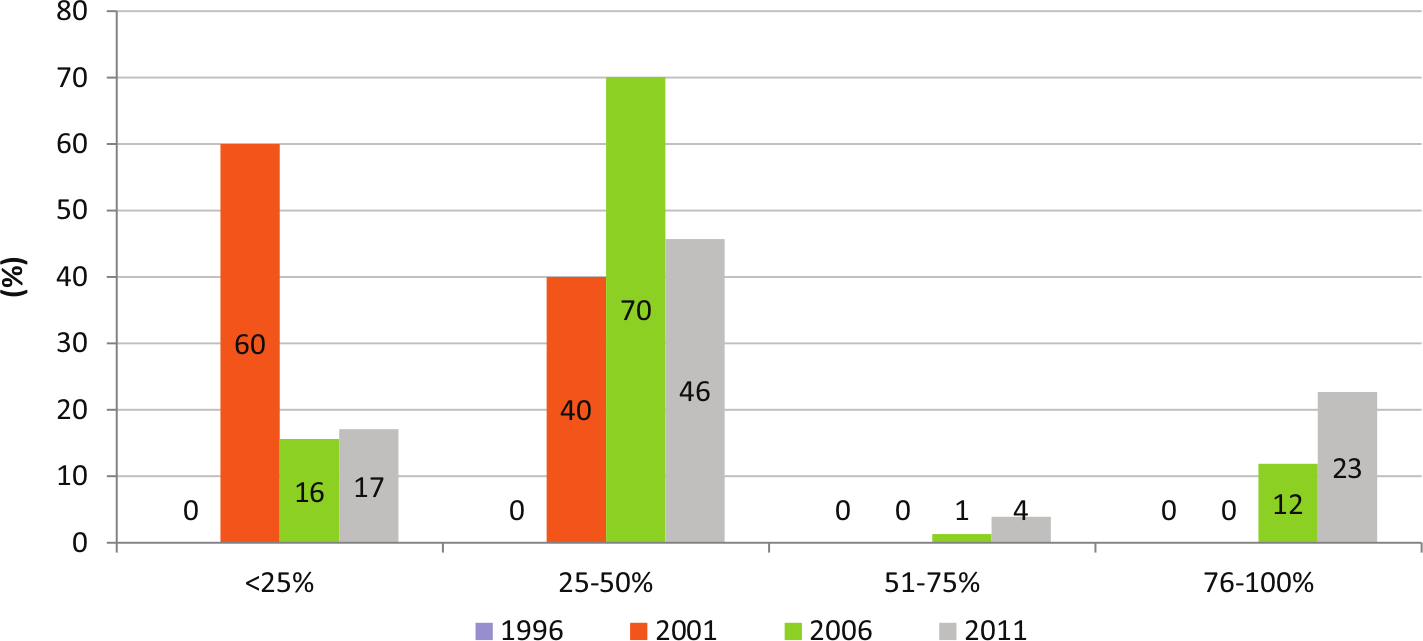
Dosing of angiotensin II receptor blocker (ARB) as the % of patients receiving these drugs in different ranges of their maximal doses.
Dual RAAS blockade
Dual RAAS blockade including ACEI+ARB was not prescribed in 1996. The usage of such a combination increased significantly in subsequent years and was as follows 0%, 1.02%, 7.73% and 10.02% (p<0.001). The similar increasing tendency was observed among subgroup CKD patients with proteinuria. In subsequent years 0%, 1.89%, 16.82% and 17.01% were treated with dual RAAS blockade among them (p<0.001) (Figures 1 and 2).
RAAS blockade accompanied by diuretics
The use of diuretics among patients receiving ACEIs and/or ARBs was as follows: 37.5%, 38.07%, 50.09% and 56.94% in 1996, 2001, 2006 and 2011 respectively (p<0.001).
RAAS blockade and serum potassium level
There were no significant differences in serum potassium concentration between patients treated with RAAS blockade as monotherapy, patients treated with dual RAAS blockade (ACEI plus ARB) and subjects who were not treated with RAAS blocking agents (Table 4). Although there were numerical differences in the frequencies of hyperpotassaemia between these subgroups (the highest during dual RAAS blockade) generally they did not reach statistical significance (Table 5).
Potassium serum concentration (mmol/l) in chronic kidney disease (CKD) patients (mean+/- SEM).

RAAS: renin-angiotensin-aldosterone system.
Frequency of hyperkalaemia defined as serum potassium concentration >5.1 mmol/l (n%) in chronic kidney disease (CKD) patients treated or not treated renin-angiotensin-aldosterone system (RAAS) blockade (angiotensin converting enzyme inhibitor (ACEI) or/and angiotensin II receptor blocker (ARB)).

p<0.01, no RAAS vs dual RAAS (2006).
Subgroup analysis of patients treated with ACEIs and/or ARBs revealed that the highest frequency of hyperkalaemia were observed in patients in CKD 4–5 stages as compared to CKD 1–2 and CKD 3 (2006 and 2011) (Figure 5).
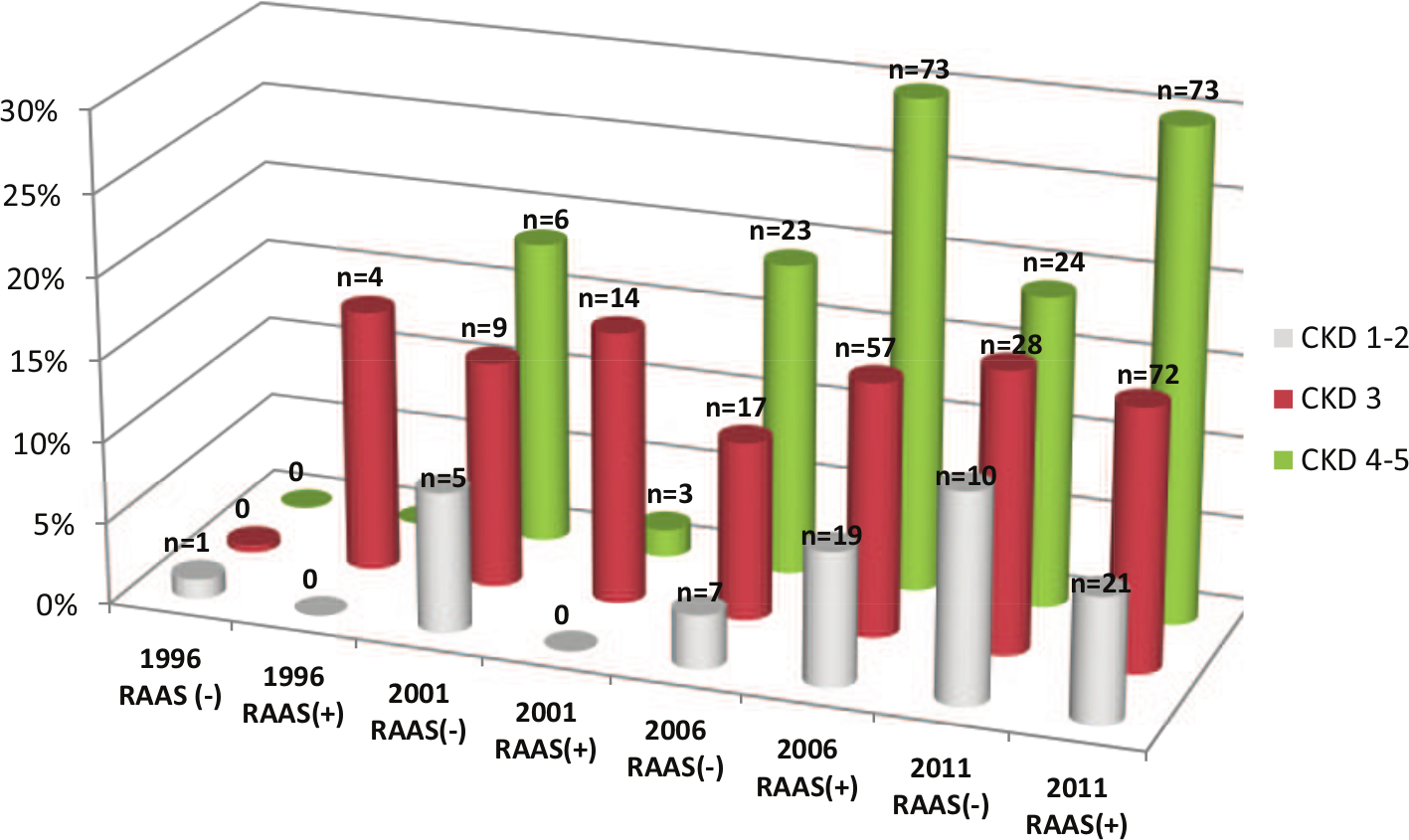
Frequency of hyperkalaemia defined as serum potassium concentration >5.1 mmol/l (n%) chronic kidney disease (CKD) patients treated or not treated renin-angiotensin-aldosterone system (RAAS) blockade (angiotensin converting enzyme inhibitor (ACEI) or/and angiotensin II receptor blocker (ARB)) related to CKD stages.
Discussion
The use of RAAS blocking agents increased in the studied populations in subsequent years. In 2011, 74% of patients received these drugs, with nearly 79% of patients with proteinuria. ACEI drugs are the most common ones, as approximately every other patient was treated with ACEI. In the Polish CKD population not managed by nephrologists (Epidemiology of Kidney Diseases in Poland - pilot study (PoINEF) analysis of 2007) approximately 61% of patients received ACEIs. 8 These indicators are high, taking into account the studies from other centres – for instance, National Health and Nutrition Examination Survey (NHANES) in 2006, which showed that in the American population of CKD patients who received antihypertensive treatment, only 37% of patients received an ACEI or ARB. 9 In the Mediterranean countries the proportion of patients treated with RAAS inhibitors is larger, with values reaching 39% (Spain, ACEI alone), 62% (France, ACEI or ARB, 2008) and 53–80% in Italy (2005).10–13 In our centre the % of patients receiving ACEI has been on a fairly unchanged level since 2001. This year, however, what we observed is an increasingly more frequent use of ARBs, a more recent group of RAAS inhibitors, which were introduced into Polish clinical practice in the late nineties. The stratified analysis of the use of RAAS blocking agents controlled by age did not reveal any differences. Patients with proteinuria, cardiovascular complications and/or diabetes and men, however, were more commonly treated with an ACEI and/or ARB as compared to others.
The matter of the ACEI and ARB administration in patients with impaired glomerular filtration has caused numerous controversies. 14 To this day, some clinicians reluctantly administer the RAAS inhibiting agents in patients with chronic renal failure due to a risk of sudden renal function deterioration or hyperkalaemia. The post-hoc, secondary analysis of the REIN trial shed new light on this intriguing issue. The study clearly established that the renoprotective effect of ACEI is independent of renal function and provided a strong background for the recommendation to administer the RAAS-inhibiting agents to all patients with proteinuric chronic nephropathies, regardless of renal function. 15 This seems to be reflected in the results of our study. The use of ACEIs and ARBs in the most advanced CKD stages increased in subsequent surveys.
Until now, the optimal nephroprotective dosing of ACEI and ARB has not been established and, therefore, the dosages used in the treatment of arterial hypertension are commonly administered. The results of our previous studies clearly showed that even very low ACEI or ARB doses, which have been found not to produce significant effect on arterial pressure, decrease proteinuria. 16 The evidence exists, however, that blockade of the RAAS is a closely dose-related phenomenon and the enhancement of the RAAS inhibition by increasing the dosage of ACEI or ARB allows for a greater decrement of proteinuria and attenuation of tubular injury. 17 Therefore, considering the prognostic impact of proteinuria reduction on renal outcome, it has been commonly recommended to uptitrate the ACEI or ARB for maximal antiproteinuric effect regardless of BP. The tendency to increase dosing of ACEIs was observed in subsequent years of our observation. In 2011 most patients received these agents in the highest range of their doses. ARBs were used most commonly in the range 25–50% of their maximal doses. The reason for limiting the dosing of ARBs in our population as compared to the dosing of ACEIs may derive from economic factors in Polish conditions in these years.
The combination therapy of ACEI and ARB has been studied extensively for some years with respect to renal protection. Several clinical studies have investigated dual RAAS blockade in nondiabetic, diabetic or mixed renal patients and documented a greater antiproteinuric effect of such a combination in comparison with monotherapy.9,18 Given these results, the dual RAAS blockade was considered for a time even as a gold standard of treatment for chronic proteinuric kidney disease. 19 In the world literature there is little data on the frequency of use of such a therapy. In Italy the use of dual RAAS blockade was in the range of 2–8% of the CKD population (2005).10,13,20 In 1996 there were no patients treated with ACEI plus ARB in our population whereas 1% and 8% of patients received such treatment in 2001 and 2006 respectively. Decrease of enthusiasm for the combination therapy and the inhibition of growth trend in use of it in 2011 was probably associated with the results of the ONTARGET study, which not only showed no long-term benefits resulting from such therapy, but drew attention to a number of its dangers including the risk of life-threatening hyperkalaemia and acute renal failure. 21 To shed some light on this issue we analysed potassium serum levels in patients treated with RAAS blocking agents as monotherapy, those who received dual RAAS blockade of an ACEI plus ARB and subjects without such treatment. Patients on the combination therapy ACEI plus ARB had a numerically higher concentration of serum potassium and the frequency of hyperkalaemia regarded as serum potassium level above 5.1 mmol/l, nevertheless, the differences did not reach significance level. The results may suggest that careful management of CKD patients treated with RAAS inhibitors, even with dual RAAS blockade, may prevent a dangerous rise of the potassium level. Subgroup analysis confirmed that special attention should be paid to patients with advanced CKD which are at highest risk of hyperkalaemia during such treatment. Of note, a potential limitation of this analysis is the fact that data concerning serum potassium concentration referred only to a single assessment.
The hypotensive and antiproteinuric effect of RAAS inhibitors is impaired with a high salt intake, thus, patients treated with an ACEI or ARB are commonly instructed to follow a low salt diet and their treatment should be accompanied by diuretics. 22 Awareness of this fact seems to increase slightly in nephrologists as the use of diuretics among patients receiving ACEI and/ or ARB was increasing in subsequent years of our observation. One should take into account the fact, however, that almost every other patients was unfortunately not treated with diuretics in 2011.
In summary the use of RAAS blocking agents was increasing in CKD patients under the care of nephrologists in Gdansk between 1996–2011. The quality of management was gradually improved.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.