
Abstract
Background:
Some studies have evaluated the associations between the angiotensin-converting enzyme 2 (ACE2) gene polymorphisms and essential hypertension (EH) risk. However, the results remain uncertain. We carried out a meta-analysis to derive a more comprehensive estimation of these associations.
Methods:
Case-control studies were identified by searching PubMed, EMBASE, Chinese National Knowledge Infrastructure (CNKI) and Wangfang databases. Odds ratios (ORs) with 95% confidence intervals (CIs) were used to assess the strength of the associations.
Results:
Significant associations were found between the ACE2 G8790A polymorphism and EH risk in males (OR = 1.27; 95% CI, 1.11–1.44; p = 0.0004; I2 = 34%) and females (OR = 1.21; 95% CI, 1.09–1.34; p = 0.0003; I2 = 31%), respectively. Significant associations were also observed between the ACE2 rs2106809 polymorphism and EH risk in males (OR = 1.24; 95% CI, 1.10–1.39; p = 0.0004; I2 = 18%) and females (OR = 1.39; 95% CI, 1.27–1.51; p < 0.00001; I2 = 0%), respectively. However, there was no significant association between the ACE2 A1075G polymorphism and EH risk in males (OR = 1.27; 95% CI, 0.77–2.10; p = 0.35; I2 = 69%) and females (OR = 1.02; 95% CI, 0.83–1.26; p = 0.84; I2 = 33%), respectively.
Conclusions:
These results suggest that the ACE2 G8790A and rs2106809 polymorphisms may be associated with EH risk.
Introduction
Essential hypertension (EH) is the most common cardiovascular disease, affecting about one billion individuals worldwide. It is evident that EH is a very important public health challenge because its complications, including cardiovascular, cerebrovascular, and renal diseases, are major causes of morbidity and mortality.
Angiotensin-converting enzyme 2 (ACE2), a recently described renin-angiotensin-aldosterone system (RAAS) component that shares 42% identity with the catalytic domain of somatic ACE, has been found to play a protective role in regulation of blood pressure homeostasis and cardiac function. 1 ACE2 has one active enzymatic site and is responsible for degrading Ang II to the vasodilator Ang 1–7. 2 ACE2 is a type 1 integral membrane glycoprotein that is found in most tissues, with its highest expression observed in the endothelium and heart. 3 Yagil and Yagil showed that ACE2-knockout mice had 10 mmHg higher blood pressure and an enhanced response to angiotensin-II infusion compared with normal mice. 4 Thus, it was reasonable to hypothesize that ACE2 might potentially be a candidate gene of EH.
So far, a lot of studies have investigated the association between ACE2 polymorphisms and susceptibility of EH.5–19 However, the results from these studies were inconsistent. Although three meta-analyses on this topic have be published, some inconsistent results still exist.20–22 For example, Lu et al. reported that the ACE2 gene polymorphism G8790A was probably a genetic risk factor for essential hypertension. 20 However, Zhou et al. and Li found that the ACE2 G8790A polymorphism might not be related to increased EH risk.21,22 In addition, all these meta-analyses focused on one polymorphism: G8790A polymorphism. They did not evaluate the associations between other polymorphisms and EH risk. Hence, we performed a meta-analysis of all eligible studies to derive a more precise estimation of the associations of ACE2 polymorphisms with EH risks. This is, to our knowledge, the most comprehensive meta-analysis of the association between ACE2 polymorphisms and EH susceptibility.
Methods
Publication search
Published studies were identified through a computerized search of PubMed, EMBASE, Chinese National Knowledge Infrastructure (CNKI) and Wangfang databases (last search was updated on May, 2014). The search terms were used as follows: (essential hypertension or hypertension) and (angiotensin-converting enzyme 2 or ACE2) and (polymorphism or mutation or variant). We also perused the reference lists of all retrieved articles and relevant reviews. There was no language restriction.
Inclusion and exclusion criteria
Eligible studies had to meet the following criteria: (a) only case-control studies were considered, (b) the study explored the correlation between ACE2 polymorphisms with EH risk. Major exclusion criteria were: (a) no control population, (b) no available genotype frequency, (c) when duplication of the previous publications existed, the largest or most recent publication was selected.
Data extraction
Information was extracted from all eligible publications independently by two authors according to the inclusion criteria listed above. The following information was extracted from each study: first author, publication year, racial background, age of patients, gender, number of cases and controls, polymorphisms, and odds ratios (ORs) and the corresponding 95% confidence intervals (CIs) of EH risk.
Statistical analysis
OR and 95% CI were applied to assess the strength of the association of ACE2 polymorphisms and EH risk. An allele model was used in this meta-analysis, because most of the studies reported the results in this model. Because the ACE2 gene is located on the X chromosome, all of the data for each sex were analyzed separately. Heterogeneity among studies was calculated using the χ2-based Cochran’s Q-statistic test (p < 0.10 was considered statistically significant heterogeneity); the inconsistency index I2 statistic was also calculated to observe between-study variability that was due to heterogeneity rather than chance. This statistic, which was documented by percentage, yields result ranging from 0 to 100% (I2 = 0–25%, no heterogeneity; I2 = 25–50%, moderate heterogeneity; I2 = 50–75%, large heterogeneity; I2 = 75–100%, extreme heterogeneity). A random effects model using the method of DerSimonian and Laird was used in this meta-analysis. Sensitivity analyses were conducted by deleting a single study each time involved in the meta-analysis to identify the potential influence of the individual data set on the pooled ORs. Potential publication bias was assessed by Egger’s weighted regression method. 23 All statistical analyses were conducted using Stata software version 11.0. All p values were two sided.
Results
Study characteristics
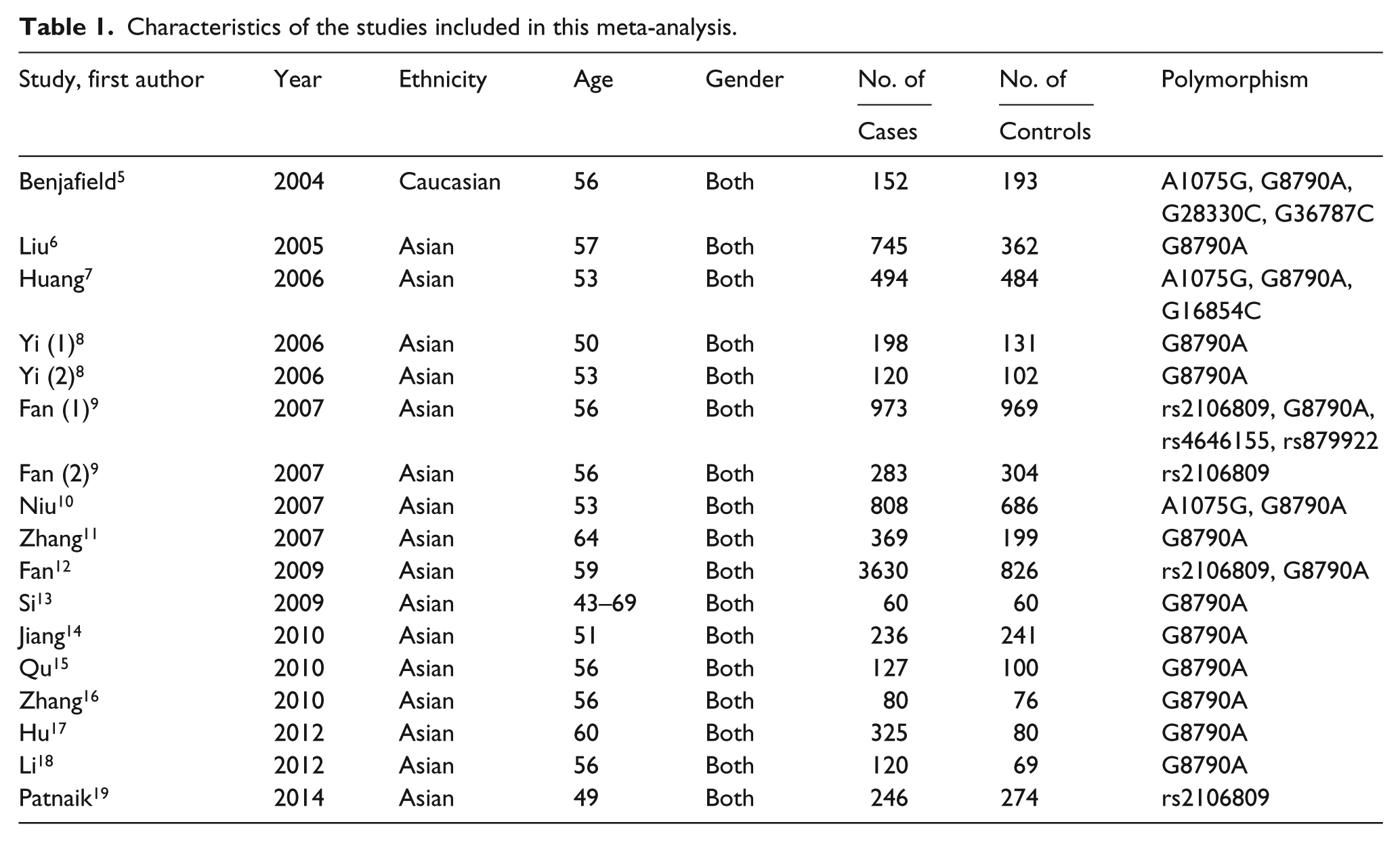
After a comprehensive literature search applying our inclusion criteria, 15 relevant studies comprising 8966 patients and 5156 controls were identified in the final analysis. Two studies reported two case-control studies. Therefore, a total of 17 studies were included in this meta-analysis. There was only one study with Caucasians, while the rest of the studies used Asians. There were three studies on A1075G polymorphism, 15 studies on G8790A polymorphism, and four studies on rs2106809 polymorphism. The main study characteristics are summarized in Table 1.
Characteristics of the studies included in this meta-analysis.
Quantitative data synthesis
The ACE2 A1075G polymorphism
Three studies determined the association between A1075G polymorphism and EH risk. The sample sizes for case and control groups were 1454 and 1363, respectively. There was no significant association between ACE2 A1075G polymorphism and EH risk in males (OR = 1.27; 95% CI, 0.77–2.10; p = 0.35; I2 = 69%) and females (OR = 1.02; 95% CI, 0.83–1.26; p = 0.84; I2 = 33%), respectively. Results of this meta-analysis are shown in Table 2. We conducted one-way sensitivity analysis to evaluate the stability of the meta-analysis. The statistical significance of the results was not altered when any single study was omitted (data not shown). Egger’s test did not indicate significant publication bias (p = 0.13 and 0.64, respectively).
Results of the meta-analysis.

R: random-effects model; OR: odds ratio; CI: confidence interval.
The ACE2 G8790A polymorphism
Fifteen studies determined the association between G8790A polymorphism and EH risk. The sample sizes for case and control groups were 8437 and 4578, respectively. Significant associations were found between ACE2 G8790A polymorphism and EH risk in males (OR = 1.27; 95% CI, 1.11–1.44; p = 0.0004; I2 = 34%) and females (OR = 1.21; 95% CI, 1.09–1.34; p = 0.0003; I2 = 31%), respectively. Results of this meta-analysis are shown in Table 2. We conducted one-way sensitivity analysis to evaluate the stability of the meta-analysis. The statistical significance of the results was not altered when any single study was omitted (data not shown). Egger’s test did not indicate significant publication bias (p = 0.47 and 0.21, respectively).
The ACE2 rs2106809 polymorphism
Four studies determined the association between rs2106809 polymorphism and EH risk. The sample sizes for case and control groups were 5132 and 2373, respectively. Significant associations were observed between ACE2 rs2106809 polymorphism and EH risk in males (OR = 1.24; 95% CI, 1.10–1.39; p = 0.0004; I2 = 18%) and females (OR = 1.39; 95% CI, 1.27–1.51; p < 0.00001; I2 = 0%), respectively. Results of this meta-analysis are shown in Table 2. We conducted one-way sensitivity analysis to evaluate the stability of the meta-analysis. The statistical significance of the results was not altered when any single study was omitted (data not shown). Egger’s test did not indicate significant publication bias (p = 0.89 and 0.29, respectively).
Discussion
To evaluate the role of ACE2 in hypertension, various genetically manipulated animal models were developed for ACE2 deletion or overexpression. In the C57BL/6 mouse, ACE2 deficiency was associated with a modest increase in blood pressure. 24 ACE2 knockout mice have highlighted hypertensive responses to Ang II infusion associated with exaggerated accumulation of Ang II in the kidney. The transgenic ACE2 overexpression in spontaneous hypertensive rat (SHR) showed a reduction of mean arterial pressure irrespective of heart rate. This ACE2 overexpression model showed an increase of Ang-(1–7) in plasma and kidney, and attenuated blood pressure elevation response to Ang II infusion. 25 Taken together, these results suggested that ACE2 was critical in the development of EH. ACE2 was one of the most studied of the candidate genes for EH. The G8790A polymorphism was situated in the intron adjoined to the extron, suggesting that this locus could alter messenger RNA (mRNA) alternate splicing and affect ACE2 gene expression. The latter led to changes in the serum content of Ang1–7 that inhibited vasoconstriction and cell proliferation. 25 The functional impact of rs2106809 remained unclear, but it has been reported that some regulatory elements within intronic sequences or residing up to 85 kb upstream of the gene’s promoter were still able to communicate with the promoter and regulate gene expression. 26 Thus, one can reasonably speculate that the ACE2 rs2106809 T allele may be functional and could downregulate the expression of ACE2 and contribute to the increase in the susceptibility to hypertension. Thus, it was plausible that these two polymorphisms could influence the susceptibility to EH.
In the present meta-analysis, we explored the associations between the ACE2 A1075G, G8790A and rs2106809 polymorphisms and EH risk, including 17 eligible case-control studies. For the ACE2 A1075G polymorphism, no significant result was detected. However, only three studies were included. Thus, the positive association between ACE2 A1075G polymorphism and EH could not be ruled out because studies with small sample size may have insufficient statistical power to detect a slight effect. For the ACE2 G8790A polymorphism, 8437 cases and 4578 controls were included. We found that individuals with the 8790A allele showed an increased risk of EH in males and females, respectively. Actually, there was only one study with Caucasians. Thus, we can conclude only that Asians with ACE2 A1075G polymorphism might have increased EH risk. This result was consistent with the previous meta-analysis. 20 For the ACE2 rs2106809 polymorphism, 5132 cases and 2373 controls were included. There was a significant association between this polymorphism and EH risk. Taken together, these results suggested that ACE2 G8790A and rs2106809 polymorphisms may play important roles in the etiology of EH.
The present meta-analysis should be interpreted with caution; several limitations merit consideration. First, because of a lack of original data from the eligible studies, we could not perform other subgroup analyses based on age, smoking, and so on. Second, the numbers of published studies were not sufficient for a comprehensive analysis, particularly for Caucasians and Africans. However, our meta-analysis also had some merits. First, we investigated the association between three polymorphisms and EH risk. Second, there was low heterogeneity in this meta-analysis.
This meta-analysis suggested that the ACE2 G8790A and rs2106809 polymorphisms may be associated with EH development. Further studies with a larger sample size are needed to further assess the presence of an association.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.