
Abstract
Introduction:
Little is known about genetic predictors that modify the renoprotective effect of renin-angiotensin system (RAS) blockade in IgA nephropathy (IgAN).
Materials and methods:
The present multicenter retrospective observational study examined effect modification between RAS blockade and three RAS-related gene polymorphisms in 237 IgAN patients, including ACE I/D (rs1799752), AT1R A1166C (rs5186) and AGT T704C (rs699).
Results:
During 9.9 ± 4.2 years of observation, 63 patients progressed to a 50% increase in serum creatinine level. Only ACE I/D predicted the outcome (ACE DD vs ID/II, hazard ratio 1.86 (95% confidence interval 1.03, 3.33)) and modified the renoprotective effect of RAS blockade (p for interaction between ACE DD and RAS blockade = 0.087). RAS blockade suppressed progression in ACE DD patients but not in ID/II patients (ACE ID/II with RAS blockade as a reference; ID/II without RAS blockade 1.45 (0.72, 2.92); DD without RAS blockade 3.06 (1.39, 6.73); DD with RAS blockade 1.51 (0.54, 4.19)), which was ascertained in a model with the outcome of slope of estimated glomerular filtration rate (p = 0.045 for interaction).
Conclusion:
ACE I/D predicted the IgAN progression and the renoprotective effect of RAS blockade in IgAN patients whereas neither AT1R A1166C nor AGT T704C did.
Introduction
Immunoglobulin A (IgA) nephropathy (IgAN) is the most common glomerulonephritis worldwide,1–4 progressing to end-stage renal disease (ESRD) within 10 years of diagnosis in approximately 15%−25% patients. 5 A series of randomized controlled trials demonstrated that renin-angiotensin system (RAS) blockade using angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin-receptor blockers (ARBs) decreased urinary protein6–10 and suppressed progression of IgAN.6,7 RAS blockade is regarded as a major treatment strategy to prevent the progression of IgAN.11,12
Recent studies reported that intrarenal expression of angiotensinogen, a key regulator of RAS activity, is enhanced in IgAN patients13,14 and is correlated with urinary angiotensinogen level, a surrogate marker of intrarenal RAS activity. 14 Urinary angiotensinogen level predicts renal prognosis in patients with chronic kidney disease, 15 including IgAN. 16 RAS blockade is likely to suppress intrarenal RAS activity and therefore improve renal prognosis of IgAN patients. Accordingly, the patients with higher intrarenal RAS activity potentially reap the greater benefit of RAS blockade. Strong candidates affecting intrarenal RAS activity are RAS-related gene polymorphisms, including angiotensin-converting enzyme ACE insertion/deletion (I/D) polymorphism (rs1799752). Compared with ACE II/ID subjects, ACE DD subjects have higher circulating and tissue ACE level,17–19 suggesting that they may be amenable to treatment with RAS blockade.
The objective of the present multicenter retrospective observational study was to examine whether three major RAS-related gene polymorphisms modify the renoprotective effects of RAS blockade in IgAN patients. This study is one of the largest genetic studies of IgAN (n = 237) and involved the longest observational period (9.9 ± 4.2 years), thus providing pivotal information for establishing a therapeutic strategy of RAS blockade in IgAN patients.
Materials and methods
Participants
Genetic and clinical data of 237 IgAN patients included in the present study were derived from our previous study, Polymorphism REsearch to DIstinguish genetic factors Contributing To progression of IgA Nephropathy (PREDICT-IgAN).20–22 Briefly, between January 1990 and December 2005, 1132 patients aged ≥15 years were diagnosed with IgAN by kidney biopsy at the Osaka University Hospital, Osaka General Medical Center and Osaka Rosai Hospital in the Osaka prefecture, Japan. Among 482 patients who visited these hospitals between April 2006 and March 2008, 429 patients participated in PREDICT-IgAN. Of 281 patients aged ≥18 years with ≥0.3 g/day of urinary protein and ≥15 ml/min/1.73 m2 of estimated glomerular filtration rate (eGFR), 40 patients with RAS blockade (ACEIs (n = 31) and ARBs (n = 10)) at kidney biopsy were excluded, because RAS blockade at kidney biopsy might influence baseline prognostic confounders and potentially lead to the biased estimates of associations between RAS blockade and IgAN progression (prevalent user bias). 23 After excluding one patient with malignant hypertension at kidney biopsy and six patients with missing baseline data, a final 237 IgAN patients were enrolled in the present study. The study protocol was approved by the ethical committee of Osaka University, Osaka General Medical Center and Osaka Rosai Hospital.
Measurements
Based on previous genetic studies of RAS-related gene polymorphisms, we selected three major RAS-related gene polymorphisms as possible predictors of the renoprotective effect of RAS blockade: ACE I/D (rs1799752), 17 angiotensin II type 1 receptor AT1R A1166C (rs5186) 24 and angiotensinogen AGT T704C (rs699). 25 Clinical characteristics collected at kidney biopsy included age, gender, smoking status, mean arterial pressure (diastolic blood pressure + [systolic blood pressure – diastolic blood pressure]/3), hypertension (defined as systolic blood pressure ≥ 130 mmHg, diastolic blood pressure ≥ 80 mmHg or use of antihypertensive agents including calcium channel blockers, β-blockers, α-blockers and thiazides), serum creatinine level, eGFR based on the Japanese equation (eGFR (ml/min/1.73m2) = 194 × serum creatinine [mg/dl]–1.094 × age [year]–0.287 (× 0.739 if female)) 26 and urinary protein level and urinary occult blood. The values of eGFR and urinary protein were stratified into four categories (<45, 45–59, 60−89, and ≥90 ml/min/1.73 m2) and three categories (<0.50, 0.50−0.99 and ≥1.00 g/day), respectively. The values of urinary occult blood were measured using dipstick and were stratified into three categories (negative or trace, 1+ or 2+ and 3+ or more). Smoking status was based on a questionnaire completed at admission for kidney biopsy. 27 Nonsmokers and past smokers were combined into a single category (non- or past smokers) because the number of past smokers was very small (n = 7). Therapeutic interventions assessed were RAS blockade, including use of ACEIs and/or ARBs, and use of immunosuppressants, including corticosteroids and other immunosuppressive agents. As long-term survivors might have more opportunities to receive therapeutic interventions in an observational study, thus potentially biasing their effectiveness (survivor treatment selection bias),28,29 we confined the therapeutic interventions to those initiated within one year of kidney biopsy.
The observational period was defined as the time from kidney biopsy to incidence of ESRD or the last measurement of the serum creatinine level before September 2009, whichever came first. The study outcomes were an irreversible 50% increase in the serum creatinine level at kidney biopsy and the slope of eGFR (ml/min/1.73 m2 per year), which was calculated based on serum creatinine levels at kidney biopsy and the end of the observational period. To clarify the clinical course of blood pressure and urinary protein after initiating RAS blockade, we assessed blood pressure and dipstick urinary protein at one and two years after kidney biopsy. Measurements closest to year 1 and 2 within a caliper width of 60 days were collected.
Statistics
Clinical characteristics of patients with and without RAS blockade within one year of kidney biopsy and clinical courses of blood pressure and dipstick urinary protein within two years of kidney biopsy were compared using the Student’s t test, Wilcoxon’s rank sum test and χ2 test as appropriate. Genotype frequencies of three polymorphisms in the Hardy-Weinberg equilibrium were compared between the patients with and without RAS blockade, by using the χ2 test. Each gene polymorphism had three genotypes: major homozygote, heterozygote and minor homozygote. The associations between each polymorphism and the outcomes were examined using dominant models (homozygote of nonrisk allele vs heterozygote/homozygote of risk allele) and recessive models (homozygote of risk allele vs heterozygote/homozygote of nonrisk allele). Based on previous studies, we classified the following as risk alleles: ACE D allele of ACE I/D,30–32 C allele of AT1R A1166C 24 and C allele of AGT T704C. 25 We did not analyze dominant or recessive models with <10% frequencies of minor homozygotes because a small sample size would hinder any meaningful statistical analysis.
Genetic predictor of IgAN progression were identified using facility-adjusted Cox proportional-hazards (CPH) models and multivariate CPH models adjusting for facility and clinically relevant factors. To identify genetic predictors of the renoprotective effectiveness of RAS blockade, we examined the effect modification between each RAS-related gene polymorphism and RAS blockade in a multivariate CPH model. Because a test for interaction is generally conservative, p for interaction <0.1 was regarded as statistically significant. 33 To clarify the effect modification, patients were classified into four categories based on gene polymorphisms, and RAS blockade and their hazard ratios were calculated in multivariate CPH models. As a sensitivity analysis, the effect modifications of each gene polymorphism and RAS blockade were examined using multivariate linear regression model with the slope of eGFR as the outcome.
Normally distributed continuous variables were expressed as mean ± SD, and non-normally distributed continuous variables were expressed as median (interquartile range). Categorical variables were expressed as number (proportion). Statistical significance was defined as p < 0.05, if not specified. All statistical analyses were performed using STATA version 11 (STATA Corp., College Station, TX, USA).
Results
The baseline characteristics of 237 IgAN patients are presented in Table 1. Within one year of kidney biopsy, 124 patients (52.3%) received RAS blockade, including ACEIs (n = 95 (76.6%)) and/or ARBs (n = 43 (34.7%)). Compared to those without RAS blockade, patients with RAS blockade were significantly male predominant (57.3% vs 33.6%, p < 0.001), hypertensive (58.1% vs 45.1%, p = 0.047) and had a higher serum creatinine level (median 0.9 (interquartile range 0.7, 1.1) vs 0.8 (0.6, 1.0) mg/dl, p = 0.002). Genotype frequencies of the RAS-related polymorphisms were not significantly different between patients with and without RAS blockade. Because of the small sample size (<10%) of minor homozygotes, a recessive model of AT1R A1166C (CC; n = 1 (0.4%)) and a dominant model of AGT T704C (TT; n = 6 (2.5%)) were not assessed in subsequent analyses.
Clinical characteristics of 237 IgAN patients.

IgAN: IgA nephropathy; RAS: renin-angiotensin system; eGFR: estimated glomerular filtration rate; ACE: angiotensin-converting enzyme; I: insertion; D: deletion. Mean ± standard deviation (SD) or median (25%, 75%). aRAS blockade and use of immunosuppressants within one year of kidney biopsy. bDefined as systolic blood pressure ≥ 130 mmHg, diastolic blood pressure ≥ 80 mmHg or use of antihypertensive agents including calcium channel blockers, β-blockers, α-blockers and thiazides.
The predictors of a 50% increase in serum creatinine level were assessed using facility-adjusted and multivariate CPH models (Table 2). During 9.9 ± 4.2 years of the observational period, 31 (25.0%) patients with RAS blockade experienced a 50% increase in serum creatinine level and 12 (9.7%) progressed to ESRD. In comparison, 32 (28.3%) patients without RAS blockade experienced a 50% increase in serum creatinine level and 13 (11.5%) developed ESRD. In facility-adjusted CPH models, ACE DD was significantly associated with a 50% increase in serum creatinine level (vs ID/II, hazard ratio 1.97 (95% confidence interval 1.15, 3.40), p = 0.014), along with older age, male gender, current smokers, lower eGFR level and higher urinary protein level (Table 2). After adjusting for clinically relevant factors, ACE DD (vs ID/II; 1.86 (1.03, 3.33), p = 0.038), current smokers (vs non-/past smokers; 2.41 (1.38, 4.20), p = 0.002) and lower eGFR (vs eGFR ≥90 ml/min/1.73 m2; 60−89 ml/min/1.73 m2 1.02 (0.46, 2.23), p = 0.969; 45−59 ml/min/1.73 m2, 1.32 (0.51, 3.41), p = 0.562; <45 ml/min/1.73 m2, 5.02 (1.94, 12.9), p = 0.001) were identified as significant predictors of a 50% increase of serum creatinine level. No other genotype was associated with a 50% increase of serum creatinine level (Table 3).
Predictors of 50% increase in serum creatinine level.

eGFR: estimated glomerular filtration rate; 95% CI: 95% confidence interval; ACE: angiotensin-converting enzyme; I: insertion; D: deletion; RAS: renin-angiotensin system. aAdjusted for facility. bAdjusted for facility, clinical characteristics at kidney biopsy (age, gender, smoking status, hypertension, eGFR, urinary protein, and urinary occult blood); ACE I/D and therapeutic interventions within one year of kidney biopsy (RAS blockade and use of immunosuppressants). cRAS blockade and use of immunosuppressants within one year of kidney biopsy.
Effect modification between three gene polymorphisms and RAS blockade.

RAS: renin-angiotensin system; 95% CI, 95% confidence interval; ACE: angiotensin-converting enzyme; I: insertion; D: deletion. aAdjusted for facility. bAdjusted for facility, clinical characteristics at kidney biopsy (age, gender, smoking status, hypertension, eGFR, urinary protein, and urinary occult blood), ACE I/D and therapeutic interventions within one year of kidney biopsy (RAS blockade and use of immunosuppressants). cp for interaction between RAS-related gene polymorphisms and RAS blockade.
To identify genetic predictors that modify the renoprotective effectiveness of RAS blockade, effect modifications between each RAS-related gene polymorphism and RAS blockade were examined in multivariate CPH models. A significant interaction was observed in a recessive model of ACE I/D polymorphism (p for ACE DD * RAS blockade = 0.087) but not in other models (Table 3). To clarify the effect modification between ACE I/D and RAS blockade, patients were categorized into four groups based on ACE I/D and RAS blockade (Figure 1). The hazard ratio of ACE DD patients with RAS blockade was remarkably lower than that of ACE DD patients without RAS blockade; however, this trend was not observed in ACE ID/II patients (ACE ID/II without RAS blockade as a reference; ID/II patients with RAS blockade, 1.45 (0.72, 2.92), p = 0.292; DD patients without RAS blockade, 3.06 (1.39, 6.73), p = 0.006; DD patients with RAS blockade, 1.51 (0.54, 4.19), p = 0.432). RAS blockade approximately halved the risk of a 50% increase in serum creatinine level in ACE DD patients, whereas it did not in ACE ID/II patients.

Effect modification between ACE I/D (recessive model) and RAS blockade. Associations of ACE I/D and RAS blockade with 50% increase in serum creatinine level (a) and slope of eGFR (b) were assessed using Cox proportional-hazards model and linear regression models, respectively, after adjusting for facility, clinical characteristics at kidney biopsy (age, gender, smoking status, hypertension, eGFR, urinary protein and urinary occult blood) and use of immunosuppressants within one year of kidney biopsy.
A sensitivity analysis effect modification between ACE I/D and RAS blockade was also ascertained, with the slope of eGFR as the outcome. The slopes of eGFR of ACE ID/II patients without RAS blockade, ID/II patients with RAS blockade, DD patients without RAS blockade and DD patients with RAS blockade were −1.2 (interquartile range −2.6, –0.2), –1.4 (–2.9, 0.0), –2.3 (–4.8, –0.6), and −1.7 (–2.8, –0.2) ml/min/1.73 m2 per year, respectively. A multivariate linear regression model adjusting for the clinically relevant factors determined a significant effect modification between ACE I/D and RAS blockade (p for ACE DD * RAS blockade = 0.045). A similar effect modification was observed in the multivariate linear regression model (Figure 1(b)).
Similar effect modification between ACE I/D polymorphism and RAS blockade was observed in dipstick urinary protein within two years of kidney biopsy (Figure 2). At one year after kidney biopsy, the proportion of negative or trace urinary protein of ACE DD patients with RAS blockade was significantly higher than that of ACE DD patients without RAS blockade (56.2% vs 15.8%, p = 0.012). At two years after kidney biopsy, proportions of negative or trace urinary protein and also ≤1+ of urinary protein were significantly different between ACE DD patients with RAS blockade and those without RAS blockade (negative or trace urinary protein, 60.0% vs 22.8%, p = 0.027; ≤1+ of urinary protein 86.7% vs 50.0%, p = 0.026), even though six (33.3%) patients without RAS blockade within one year of kidney biopsy received RAS blockade two years after kidney biopsy. In contrast, proportions of dipstick urinary protein were not significantly different at one and two years after kidney biopsy between ACE II/ID patients with RAS blockade and those without RAS blockade, except a small difference in ≤1+ of urinary protein one year after kidney biopsy (76.0% vs 59.7%, p = 0.021). The findings described above were hardly ascribed to blood pressure control because mean arterial pressures at one and two years after kidney biopsy were comparable between the patients with RAS blockade and those without RAS blockade (Figure 3).

Urinary protein by dipstick test at kidney biopsy and one and two years after kidney biopsy. ACE DD patients with RAS blockade had higher proportions of negative or trace urinary protein at one year after kidney biopsy (p = 0.012) and negative or trace urinary protein and ≥1 of urinary protein at two years after kidney biopsy (p = 0.027 and 0.026, respectively), compared with those without RAS blockade. In contrast, no significant difference was observed at one and two years after kidney biopsy between ACE ID/II patients with RAS blockade and those without RAS blockade, except ≥2+ of urinary protein at one year after kidney biopsy (p = 0.021).
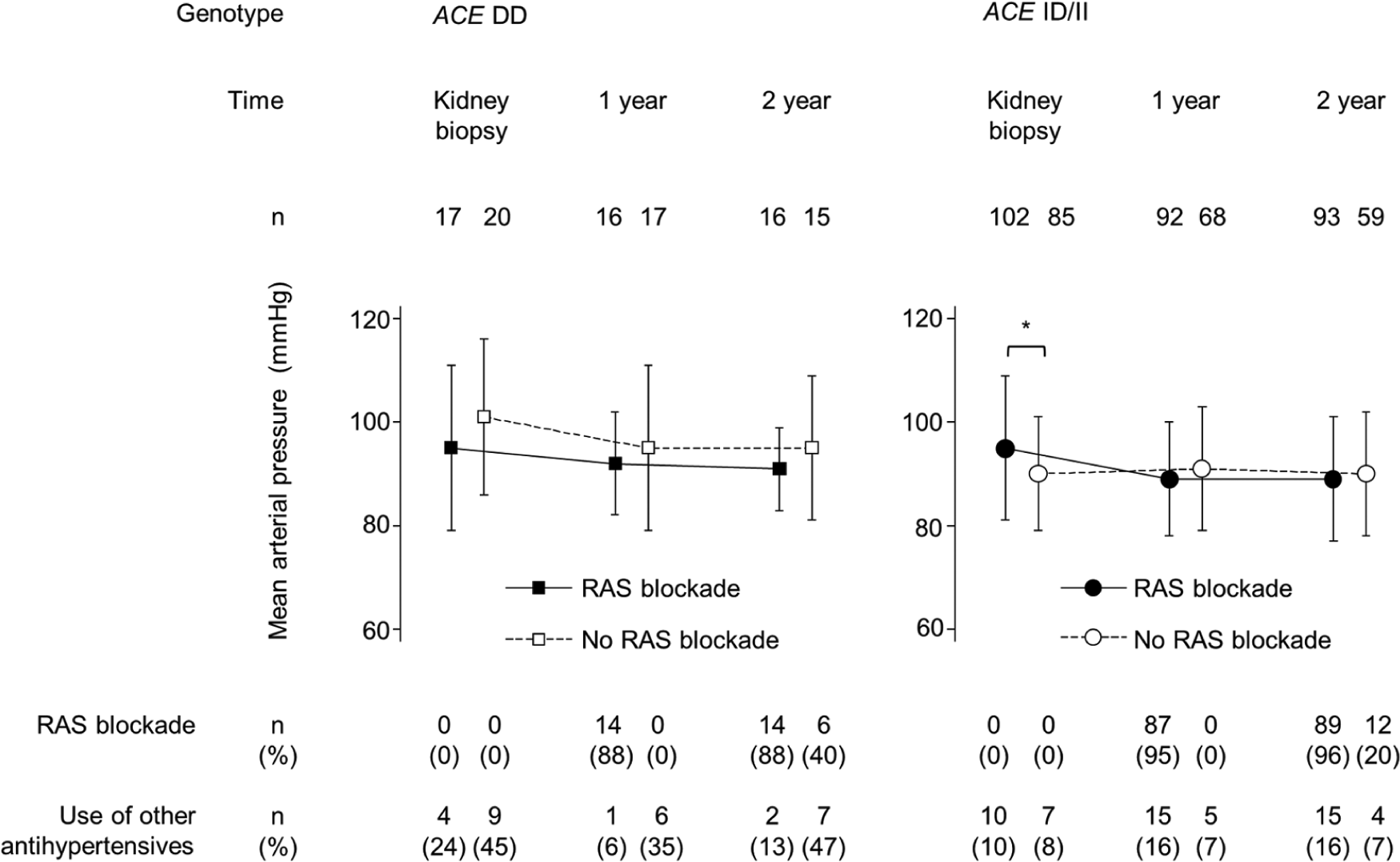
Mean arterial pressure at kidney biopsy and one and two years after kidney biopsy. No significant difference was observed between the patients with RAS blockade and those without RAS blockade at one and two years after kidney biopsy in ACE DD and II/ID patients, although ACE ID/II patients with RAS blockade had higher mean arterial pressure, compared with those without RAS blockade (95 ± 14 vs 90 ± 11 mmHg, p = 0.011).
Discussion
The present study showed that the ACE I/D predicted IgAN progression and the renoprotective effectiveness of RAS blockade in 237 IgAN patients. Compared with ACE II/ID patients, ACE DD patients were at higher risk of IgAN progression and RAS blockade halved their risk, mitigating their genetic disadvantage (Figure 1). These findings suggest that ACE I/D is a potentially useful marker to identify patients who will clinically benefit from RAS blockade. Compared with the previous studies assessing the associations between RAS-related gene polymorphisms and IgAN progression, this study is the third largest genetic study with 237 IgAN patients, following two larger studies (n = 527 34 and 267 35 ), and has the longest observational period (9.9 ± 4.2 years). Furthermore, we performed a comparative assessment of three major RAS-related gene polymorphisms and carefully controlled for several critical biases in observational studies, which no previous study took into consideration.
Although multiple studies have described the association between ACE I/D and IgAN progression, including several systematic reviews identifying ACE I/D as a predictor of IgAN progression,32,36,37 few studies assessed whether ACE I/D modified the renoprotective effect of RAS blockade. One exception was the largest genetic study by Suzuki and colleagues, which included 527 patients with IgAN. 34 Their study found that ACE I/D was not associated with the composite outcome of 100% increase in serum creatinine level or ESRD in all patients (n = 527) as well as in patients without RAS blockade during the entire observational period (n = 333), suggesting that ACE I/D did not modify the renoprotective effect of RAS blockade. In contrast, the present study revealed that RAS blockade remarkably improved renal prognosis in ACE DD patients, but not in ACE II/ID patients (Figure 1). These conflicting results may be owing to several biases such as the prevalent user bias 23 and survivor treatment bias,28,29 which were deliberately controlled in our study. Interestingly, a randomized controlled trial, the Ramipril Efficacy in Nephropathy (REIN) study, including mostly nondiabetic proteinuric patients, described an effect modification between ACE I/D and RAS blockade similar to the present study. 38 The incidence of ESRD was significantly suppressed by ramipril in ACE DD patients, but not in II/ID patients, which corroborates our study findings.
The present study clarified that RAS blockade exerted a renoprotective effect in ACE DD patients, but not in ID/II patients. ACE I/D affects the level of circulating and tissue ACE. 39 Serum ACE level was higher in ACE DD subjects compared with ID/II subjects.17,18 Furthermore, the local expression of ACE in T-lymphocytes 40 and cardiac tissue 19 were higher in ACE DD subjects compared with ID/II subjects. A Japanese study of 50 healthy kidney donors revealed that tubular and glomerular ACE messengerRNA (mRNA) signals measured using in situ hybridization were higher in ACE DD subjects than in ID/II subjects, 41 indicating that intrarenal RAS was more activated in DD patients compared to ID/II patients. Although its precise biological mechanism remains unknown, a recent study reported that ACE I/D regulated the transcriptional activity of ACE promoters, 42 providing new insight into the direct influence of ACE I/D on ACE activity. Therefore, ACE DD patients, who likely have higher activity of intrarenal RAS, might reap more renoprotective benefits from RAS blockade, compared to ID/II patients, as evidenced in the present study and REIN study.
The present study had several limitations. First, indication of RAS blockade was dependent on each physician and RAS blockade was not uniform in the present study because of its observational study design. Nevertheless, our results were compatible with the REIN study, 38 which is the largest randomized control trial assessing the efficacy of RAS blockade mainly in nondiabetic proteinuric patients. The similar findings support the validity of the present study. Second, minor genotype frequencies of AT1R A1166C and AGT T704C were too small to examine their clinical impact on effectiveness of RAS blockade. A larger cohort is essential for further investigation. Third, our study used the candidate gene approach and examined only one of a large number of gene polymorphisms in ACE. A previous study of 267 IgAN patients reported an effect modification between ACE A2350G and RAS blockade, though this was not ascertained in a multivariate model adjusting for clinically relevant factors. 35 A broader investigation of RAS-related gene polymorphisms is required to identify genetic predictors of the renoprotective effect of RAS blockade. Fourth, the present study assessed the associations between RAS blockade and RAS-related gene polymorphisms but did not measure systemic or intrarenal RAS activity. The precise biological mechanism of effect modification between the renoprotective effect of RAS blockade and ACE I/D-dependent RAS activity needs further clarification. Fifth, a lack of information on the histopathological lesion, one of the conventional prognostic factors, might affect the results of the present study. A slightly higher hazard ratio and lower β coefficient of ACE ID/II with RAS blockade compared with ID/II without RAS blockade might be due to the unmeasured histopathological lesion (confounding by indication).
Conclusions
The present study clarified that ACE I/D predicted renal outcomes and the renoprotective effectiveness of RAS blockade in IgAN patients. Recognition of ACE I/D potentially provides pivotal information for treatment optimization to prevent further progression of IgAN. Further studies are required to establish a therapeutic strategy based on both genetic and clinical evidence.
Footnotes
Acknowledgements
We are grateful for the time and efforts of the investigators who participated in the present study: Kenichiro Iio, Takahito Ito, Yoshiyuki Furumatsu, Takayuki Hamano, Noritaka Kawada, Isao Matsui, Yoshitsugu Obi, Maki Shinzawa, Yoshitsugu Takabatake (Department of Geriatric Medicine and Nephrology, Osaka University Graduate School of Medicine), Tomoko Namba, Atsushi Takahasi, Yoshito Yamaguchi, Masanori Takeji, Ken Takahara (Division of Nephrology, Department of Nephrology, Osaka Rosai Hospital), Kazunori Inoue, Tetsuya Kaneko, Akihiro Shimomura, Takuya Uehata (Osaka General Medical Center), and Masaru Horio (Department of Functional Diagnostic Science, Osaka University Graduate School of Medicine).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Ministry of Education, Culture, Sports, Science and Technology (MEXT) KAKENHI (18790563, 21790809, 22590891 and 23790940); the Osaka Kidney Foundation (OKF 09-0004 and 10-0003); and a travel grant from the 49th ERA-EDTA Congress in 2012.