
Abstract
Background:
Previous studies examined the association between angiotensin-converting enzyme (ACE) I/D polymorphism and pneumonia, but their results were inconsistent. Thus, a meta-analysis was performed to clarify the effect of ACE I/D polymorphism on pneumonia risk and pneumonia-related mortality.
Methods:
The PubMed, Embase, and Chinese National Knowledge Infrastructure (CNKI) databases were searched for relevant studies published up to 27 April 2013. Data were extracted and pooled odds ratios (ORs) with 95% confidence intervals (CIs) were calculated.
Results:
Pooled analysis of 12 case-control studies (1431 cases and 3600 controls) showed that there was a significant association between ACE I/D polymorphism and pneumonia risk in a recessive genetic model (OR = 1.53, 95% CI 1.30–1.80, p < 0.00001). No significant association between ACE I/D polymorphism and mortality was observed (OR = 2.68, 95% CI 0.80–8.90, p = 0.11).
Conclusions:
Our meta-analysis confirmed that ACE I/D polymorphism was associated with pneumonia risk. However, ACE I/D polymorphism was not associated with pneumonia mortality.
Introduction
Despite modern resuscitating strategies and new anti-infective options, pneumonia remains the leading cause of death.1,2 For example, community-acquired pneumonia (CAP) affects more than 5 million adults, and causes 1.1 million hospital admissions and more than 60,000 deaths every year in the USA.1,2 Therefore, predictive markers to identify high-risk population are urgently needed for early detection and preventive care. Previous studies suggested that host genetic susceptibility may play a key role in the pathogenesis of pneumonia. 3 Recently, many investigators have begun the search for genetic risk factors influencing clinical outcomes in pneumonia, and angiotensin-converting enzyme (ACE) gene has been studied extensively.
ACE, a key enzyme in the renin–angiotensin system (RAS), is a zinc metallopeptidase whose main function is to maintain blood pressure and electrolyte homeostasis. ACE cleaves angiotensin I to generate angiotensin II, a powerful vasoconstrictor and stimulator of aldosterone secretion. 4 An insertion/deletion (I/D) polymorphism of the human ACE gene on chromosome 17q23 comprising the presence or absence of a 287 base pair (bp) insert in intron 16 was described by Rigat et al. in 1990. 5 This polymorphism has a role in the regulation of serum ACE concentration. 6 Mean ACE activity levels in DD carriers were approximately twice that found in II genotype individuals. Subjects with the ID genotype had intermediate levels. 5
So far, a number of studies have investigated the association of ACE I/D polymorphism with pneumonia.7–18 Unfortunately, these epidemiological studies, performed in different countries, have yielded conflicting results, from strong links to no association. For instance, Morimoto et al. indicated that the ACE DD genotype was associated with an increased risk of pneumonia and fatal pneumonia. 8 However, van de Garde and coworkers found that the ACE I/D polymorphism was not associated with risk and outcome of CAP. 13 The inconsistency in the results from these studies may be explained by the relatively small sample size and differences in population background. Therefore, we carried out a quantitative meta-analysis that increased statistical power to derive a more precise estimation of the association between ACE I/D polymorphism and pneumonia risk. In addition, we investigated the association between this polymorphism and pneumonia mortality risk.
Materials and methods
Publication search
We searched PubMed, Embase and Chinese National Knowledge Infrastructure (CNKI) databases using the following search terms: (pneumonia or community-acquired pneumonia or hospital-acquired pneumonia or ventilator-associated pneumonia) and (angiotensin-converting enzyme or ACE) and (polymorphism or mutation or variant). The last search was updated on 27 April 2013. The following MeSH terms were used in PubMed: “pneumonia” and “polymorphism, genetic” and “peptidyl-dipeptidase a”. The reference lists of review articles and the references cited in the retrieved studies were hand-searched for the collection of omitted relevant studies. No language limitation was imposed.
Study selection
Studies were included if all of the following conditions were met: (1) evaluation of the ACE I/D polymorphism and risk of pneumonia or pneumonia mortality; (2) case-control study; (3) studies should provide the sample size, odds ratios (ORs) and 95% confidence intervals (CIs), the genetic distribution or the information to infer the results.
Studies were excluded if one of the following existed: (1) not relevant to ACE I/D polymorphism, pneumonia, or mortality; (2) non-clinical studies; (3) reviews or comments.
Data extraction
Data were carefully extracted from all eligible publications independently by two of the authors. The following data were abstracted from each article: first author’s surname, publication year, ethnicity, study design, age group, type of pneumonia, sample size, and genotype numbers in cases and controls. Correspondence authors of the studies were contacted via email when more data were needed.
Statistical analysis
Where the data from at least three similar studies were available, the meta-analysis was performed. The strength of the associations between the ACE I/D polymorphism and risk of pneumonia and mortality were measured by ORs with 95% CIs. OR1, OR2, and OR3 were assessed for genotypes DD versus II, ID versus II, and DD versus ID, respectively. These pairwise differences were used to indicate the most appropriate genetic model as following: if OR1 = OR3 ≠ 1 and OR2 = 1, then a recessive model was suggested; if OR1 = OR2 ≠ 1 and OR3 = 1, then a dominant model was suggested; if OR2 = 1/OR3 ≠ 1 and OR1 = 1, then a complete overdominant model was suggested; if OR1 > OR2 > 1 and OR1 > OR3 > 1 (or OR1 < OR2 < 1 and OR1 < OR3 < 1), then a codominant model was suggested.19–23 Once the best genetic model was identified, this model was used to collapse the three genotypes into two groups (except in the case of a codominant model) and to pool the results again. The significance of the pooled OR was determined by the z-test, and two-tailed p < 0.05 was considered as statistically significant.
We calculated the Hardy–Weinberg equilibrium (HWE) with the Chi-square goodness-of-fit test only in the control group (p < 0.05 was considered significant). In consideration of the possibility of heterogeneity across the studies, a statistical test for heterogeneity was performed based on the Q-statistic. If p > 0.1 of the Q-test, which indicated a lack of heterogeneity among studies, the summary OR estimate of each study was calculated by the fixed-effects model (the Mantel–Haenszel method). Otherwise, the random-effects model (the DerSimonian and Laird method) was used. Subgroup analyses were stratified by ethnicity, age group, and type of pneumonia. To validate the credibility of outcomes in this meta-analysis, sensitivity analysis was performed by sequential omission of individual studies and the studies’ departure from HWE. We did cumulative meta-analysis by undertaking sequential fixed-effects pooling, starting with the earliest studies. 7 Results were presented as a series of mini meta-analyses, which were ordered chronologically in a forest plot to show the consequence of adding studies on the effect size. Publication bias was assessed by visual inspection of funnel plots, in which the standard error of log (OR) of each study was plotted against its log (OR). The symmetry of the funnel plot was further evaluated by Egger’s linear regression test. 24 Statistical analysis was undertaken using the program STATA 11.0 software (Stata Corporation, College Station, TX, USA). The Bonferroni correction of critical p values was applied when performing a high number of comparisons.
Results
Eligible studies
Figure 1 shows our study selection process. A total of 12 eligible studies involving 5031 subjects were included in the meta-analysis.7–18 The characteristics of selected studies are summarized in Table 1. There were four studies of Caucasians and seven studies of Asians. There were three studies of pediatric populations and nine studies of adult populations. Eight studies used patients with CAP, while three studies used patients with hospital-acquired pneumonia (HAP). Genotype numbers and HWE examination results are shown in Table 2. Ten case-control studies indicated that the distribution of genotypes in the controls was consistent with HWE. However, two studies were not in HWE.

Flow of study identification, inclusion, and exclusion.
Characteristics of the studies included in meta-analysis.
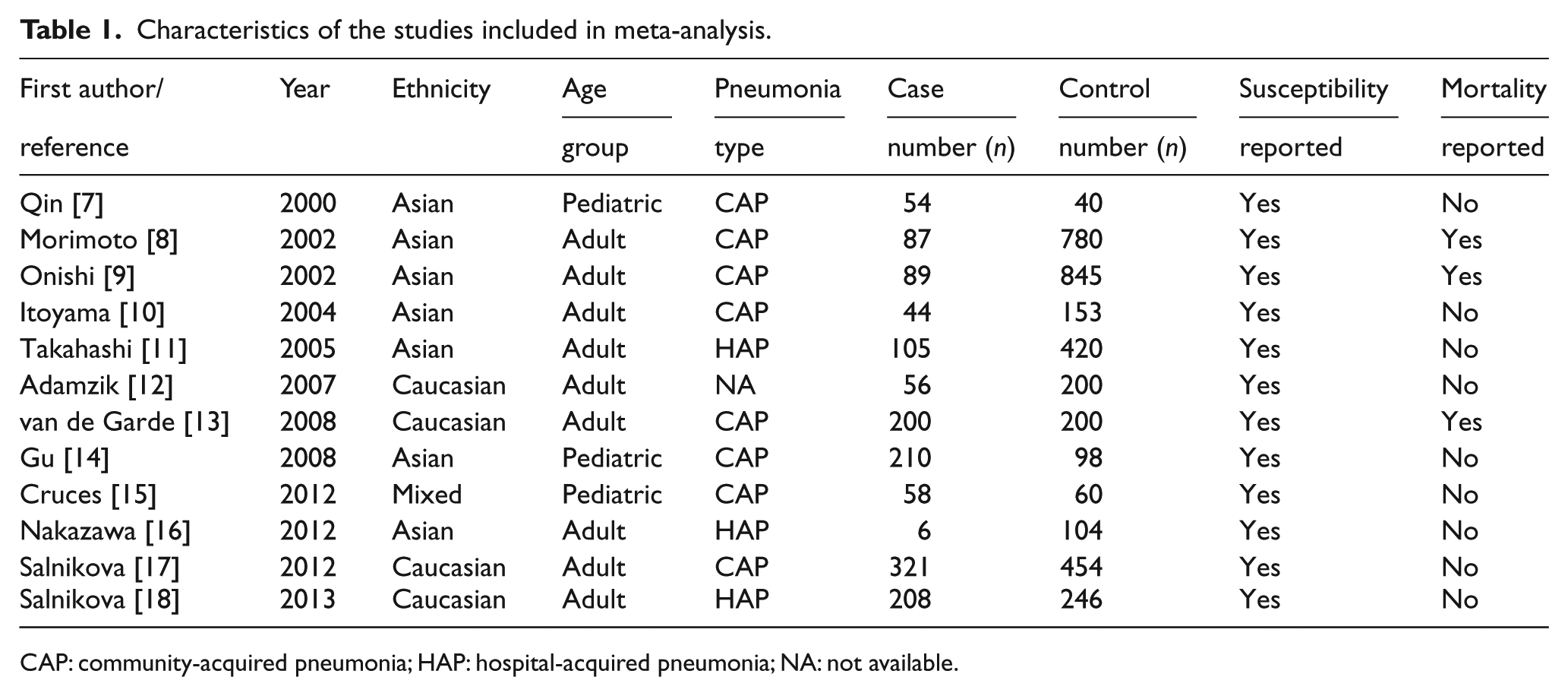
CAP: community-acquired pneumonia; HAP: hospital-acquired pneumonia; NA: not available.
Distribution of ACE I/D genotype among patients with pneumonia and controls.
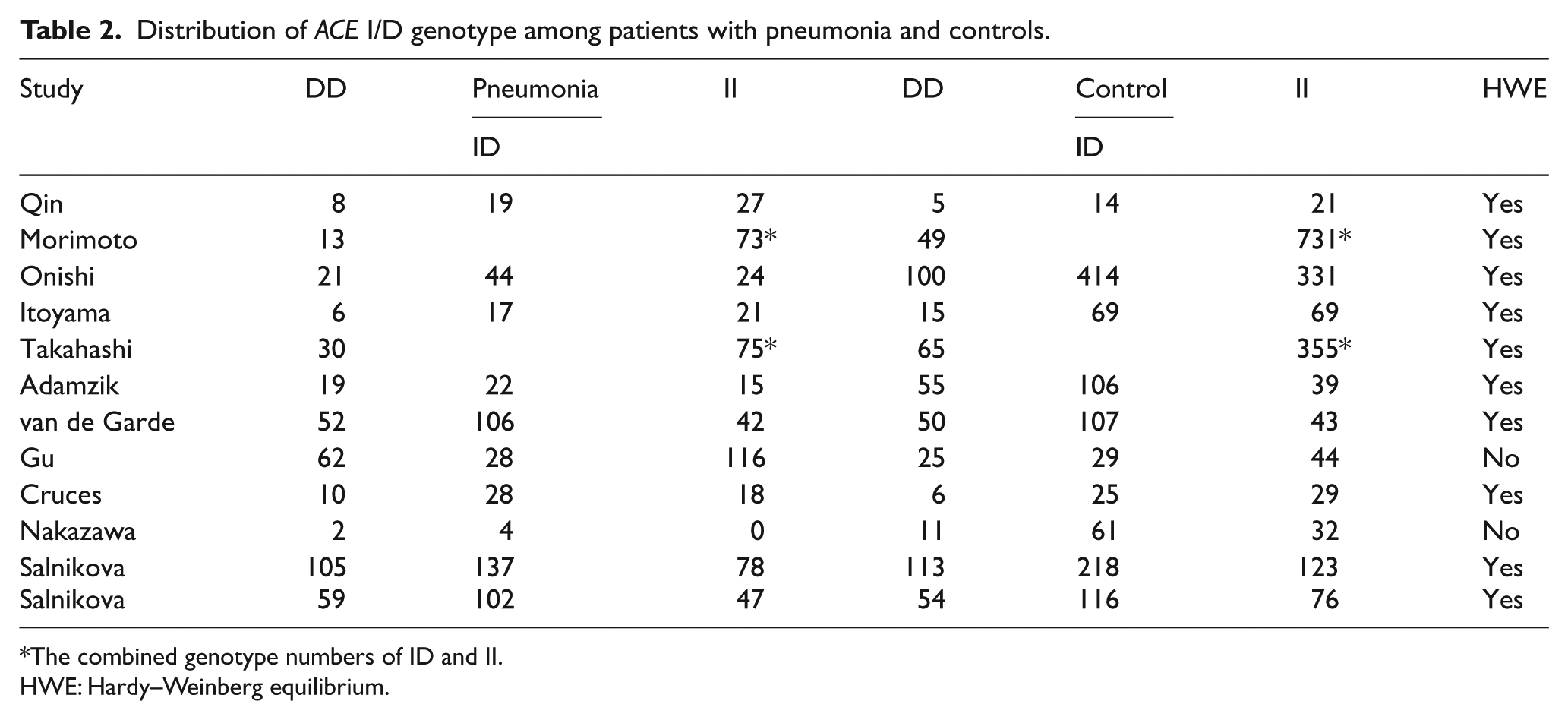
The combined genotype numbers of ID and II.
HWE: Hardy–Weinberg equilibrium.
Meta-analysis
Twelve studies determined the association between ACE I/D polymorphism and pneumonia risk. Total sample sizes for pneumonia case and control were 1431 and 3600, respectively. The estimated OR1, OR2 and OR3 were 1.45, 0.98, and 1.47, respectively (Table 3). These estimates suggested a recessive genetic model; therefore ID and II were combined and compared with DD. The pooled OR was 1.53 (95% CI 1.30–1.80, p < 0.00001) (Figure 1). In the subgroup analysis by ethnicity, significant associations were found among Asians (OR = 1.87, 95% CI 1.44–2.43, p < 0.00001) and Caucasians (OR = 1.34, 95% CI 1.09–1.65, p = 0.006). In the subgroup analysis by age group, a significantly increased risk of pneumonia was found among adults (OR = 1.56, 95% CI 1.31–1.85, p < 0.00001) but not among children (OR = 1.35, 95% CI 0.86–2.12, P = 0.19). The subgroup analysis stratified by type of pneumonia showed that significant associations existed in CAP (OR = 1.49, 95% CI 1.22–1.81, p < 0.0001) and HAP (OR = 1.71, 95% CI 1.24–2.36, p = 0.001).
Determination of the genetic effect of ACE I/D polymorphism on pneumonia and subgroup analyses.

Bonferroni correction was applied (p < 0.00625).
CAP: community-acquired pneumonia; HAP: hospital-acquired pneumonia; R: random-effects model; F: fixed-effects model.
As shown in Figure 2, the most influencing single study on the overall pooled estimates seemed to be the study conducted by van de Garde et al. 13 The OR was 1.62 (95% CI 1.36–1.93, p < 0.00001) after the removal of that study. In addition, there was still a significant result even omitting two studies not in HWE (OR = 1.55, 95% CI 1.31–1.84, p < 0.00001). These data suggested high stability of the result. Cumulative meta-analyses of ACE I/D polymorphism and pneumonia were conducted. An inclination toward significant association with pneumonia risk was found (Figure 3).
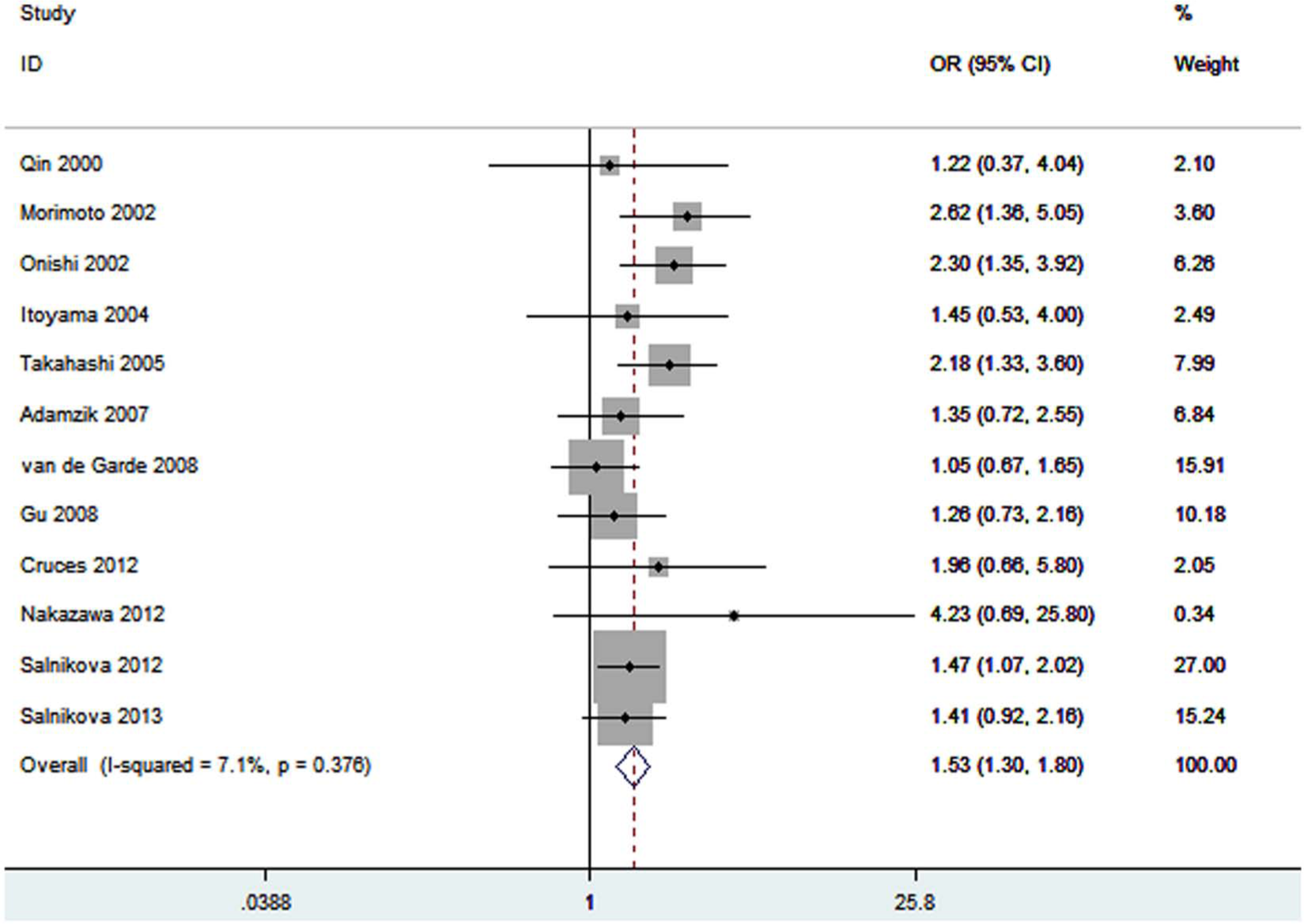
Meta-analysis for the association between pneumonia risk and the ACE I/D polymorphism.

Sensitivity analysis of the summary odds ratio coefficients on the association for the ACE I/D polymorphism with pneumonia risk.
Three studies identified the association between ACE I/D polymorphism and pneumonia-related mortality risk. Total sample size of patients was 376. No significant association between ACE I/D polymorphism and pneumonia-related mortality was found (OR = 2.68, 95% CI 0.80–8.90, p = 0.11). Summary results of comparisons are listed in Table 3.
Publication bias
Publication bias was examined by funnel plots qualitatively and estimated by Egger’s tests quantitatively. Funnel plots suggested no publication bias was observed (Figure 4). Furthermore, Egger’s test did not show evidence of publication bias (p = 0.325) (Figure 5).

Cumulative meta-analysis for the association between pneumonia risk and the ACE I/D polymorphism.

Begg’s funnel plot for pneumonia risk and ACE I/D polymorphism.
Discussion
ACE has a wide tissue and cellular distribution, and is mostly expressed on the luminal membrane of vascular endothelial cells, in particular of the pulmonary endothelium. ACE catalyzes the generation of angiotensin II from angiotensin I as well as the cleavage of bradykinin. 25 Basic investigation has shown that bradykinin and substance P sensitize the sensory nerves of the airways and enhance the cough reflex, which may have a protective role on the tracheobronchial tree.26–28 Therefore, increased ACE levels may be associated with increased pneumonia risk, and the use of ACE inhibitors may decrease the risk of pneumonia. Recently, Caldeira et al. showed a protective role of ACE inhibitors in the risk of pneumonia. 29 However, whether different levels of ACE could influence the risk of pneumonia was still unknown. Rigat and colleagues suggested that high plasma ACE levels have been shown to be associated with the ACE DD genotype. 5 In addition, Li et al. pointed out that the ACE D allele was associated with decreased ACE inhibitor-related cough. 30 Thus, it is biologically plausible that ACE DD genotype might increase pneumonia risk.
This meta-analysis of 12 studies systematically evaluated the associations between ACE I/D polymorphism and pneumonia risk. We found that DD genotype was a risk factor for developing pneumonia in the overall study population. The result showed that carriers of the DD genotype had 53% increased pneumonia risk compared with those individuals with the ID or II carriers. In the subgroup analysis by ethnicity, we found that the association between ACE I/D polymorphism and pneumonia risk remained significant in Asians and Caucasians. In the subgroup analysis based on age, a significant association was observed in the adult population but not in the pediatric population. There were only three case-control studies (n = 514) performed using pediatric populations. Therefore, the positive association between this polymorphism and pneumonia risk should not be excluded, because studies with small sample size may have insufficient statistical power to detect a slight effect. When the data were stratified based on the type of pneumonia, the ACE DD genotype showed increased CAP risk and HAP risk. This result suggested that ACE I/D polymorphism may play similar roles in the pathogenesis of CAP and HAP.
We also tried to address the relationship between ACE I/D polymorphism and pneumonia mortality risk. No statistically significant association was detected. There were at least three potential explanations for this negative result. First, only three studies including 376 patients evaluated the association between ACE I/D polymorphism and pneumonia mortality risk. Our result lacked sufficient reliability to confirm or refute an association in a definitive manner. Therefore, we cannot exclude the positive result. More studies are needed to further investigate the effect of this polymorphism on pneumonia mortality. Second, in addition to genetic predisposition, other factors, such as body mass index, complications, and medical treatment, are also thought to play crucial roles in the prognosis of pneumonia. These data should be considered in further studies. Third, the significant heterogeneity (I2 = 68% and p = 0.05) can distort the result.
The location of ACE I/D polymorphism in a noncoding region of the gene makes it unlikely to be a functional variant. Many assays demonstrated that this polymorphism was in close linkage disequilibrium to at least one, and perhaps more functional polymorphisms determining the phenotypic variations of enzyme levels. 31 Sayed-Tabatabaei and colleagues suggested that a functional polymorphism was most likely located between intron 18 and the 3’ UTR. 32 The potential existence of another functional polymorphism in the 5’ UTR, however, cannot be excluded. 32 Thus, more functional experiments are needed to explore the effect of this polymorphism.
We should acknowledge the importance of heterogeneity and publication bias, which could influence the results of meta-analysis. In our meta-analysis, there was no significant heterogeneity in most of the comparisons. In addition, funnel plots and Egger’s tests were performed to find potential publication bias. No significant publication bias was detected. Thus, it seemed that heterogeneity and publication bias did not influence the results. Furthermore, sensitivity analyses were carried out. Excluding each study and the studies not in HWE did not change the conclusion of pneumonia risk. Cumulative meta-analysis was also conducted. This analysis showed that the evidence was consistent over time. Taken together, these data suggested that our results were robust and stable.
Our study had some limitations. First, only 12 studies were included in this meta-analysis and our results were based on unadjusted estimates. Thus the effect estimates were relatively imprecise. A more precise evaluation should be adjusted by other potentially suspected factors, such as age and sex. Second, in this meta-analysis, the primary articles only provided data regarding Caucasians and Asians. Other ethnicities such as African should be investigated in future studies. Third, the lack of original data in the eligible studies limited the evaluation of the effects of gene–gene interactions in pneumonia. Fourth, because of the complex nature of pneumonia, it is unlikely that a single nucleotide polymorphism (SNP) in one single gene would be obviously associated with an increased pneumonia risk. However, insufficient data could be extracted from primary studies. Therefore, we did not perform the analysis of other SNPs in ACE and a haplotype analysis. Finally, the controls for two studies were not in HWE. However, the result was not altered after omitting these studies.
Conclusion
In summary, this meta-analysis suggested that ACE I/D polymorphism may be associated with the risk of pneumonia. However, this polymorphism was not associated with pneumonia mortality. Large case-control studies with more ethnic groups should be performed to verify the conclusions of our meta-analysis.
Footnotes
Acknowledgements
We thank Keisuke Nakazawa MD (Department of Anesthesiology, Tokyo Women’s Medical University, Tokyo Women’s Medical University. 8-1 Kawada-cho, Shinjuku, Tokyo 162-8666, Japan) for providing relevant information.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.