
Abstract
Background:
Previous studies investigating the association between the angiotensin-converting enzyme I/D polymorphism and sepsis have provided inconsistent results. Thus, a meta-analysis was performed to clarify the effect of the angiotensin-converting enzyme I/D polymorphism on sepsis risk and sepsis-related mortality.
Methods:
A comprehensive literature search was performed. Six case–control studies and two cohort studies were included in this meta-analysis. Odds ratios and corresponding 95% confidence intervals were estimated using random-effects models.
Results:
Pooled analysis of six case–control studies showed that there was a significant association between the angiotensin-converting enzyme I/D polymorphism and sepsis risk in a recessive genetic model (odds ratio = 0.75, 95% confidence interval 0.62–0.91, p = 0.004). However, no significant association between the angiotensin-converting enzyme I/D polymorphism and mortality was observed (odds ratio = 0.84, 95% confidence interval 0.57–1.24, p = 0.38).
Conclusions:
Our meta-analysis confirmed that the angiotensin-converting enzyme I/D polymorphism was associated with sepsis risk. However, the angiotensin-converting enzyme I/D polymorphism was not associated with sepsis mortality.
Introduction
Sepsis is relevant due to its high morbidity and mortality. 1 Despite modern resuscitating strategies and new anti-infective options, sepsis remains the leading cause of death in critically ill patients. 2 Therefore, predictive markers to identify high-risk populations are urgently needed for early detection and preventive care. The host genetics may play a role in the susceptibility to and outcomes from sepsis were supported by a previous study. 3 Up to now, many researchers have begun the search for genetic risk factors influencing clinical outcomes in sepsis 4 and the angiotensin-converting enzyme (ACE) gene has been studied extensively. 5
ACE is a key enzyme in the renin−angiotensin system (RAS), can convert angiotensin (Ang) I to Ang II, which is the main effector peptide of the system. The ACE gene spans 21 kb and is located on the 17th chromosome. There were more than 160 ACE polymorphisms in this gene, most of which are single nucleotide polymorphisms. 6 A lot of studies focused on one polymorphism: ACE I/D polymorphism. This polymorphism is characterized by a single guanosine nucleotide insertion/deletion variation at 287 bp in intron 16 of ACE. This polymorphism has a role in the regulation of serum ACE concentration. 7 Mean ACE activity levels in DD carriers were approximately twice those found in II genotype individuals. Subjects with the ID genotype had intermediate levels. 8 The location of this polymorphism is in a non-coding region of the gene, however, this makes it unlikely to be a functional variant. It is more likely a marker in linkage disequilibrium with functional genetic variation.9,10 Therefore, it is important to perform transfection experiments to really know the effect of this polymorphism.
To date, several studies have investigated the association of ACE I/D polymorphism with sepsis.11–18 However, the results of these studies were inconsistent, possibly due to the insufficient sample size. Meta-analysis is a statistical procedure for combining results from published studies, in order to acquire a precise estimation of the major effect. One of the major advantages of meta-analysis is to increase the sample size, which may reduce the probability of false-positive or false-negative associations. 19 Thus, we carried out a meta-analysis on the association of the ACE gene I/D polymorphism with sepsis risk. We also assessed the association between this polymorphism and sepsis-related mortality.
Methods
Publication search
We searched PubMed, Embase and CBM database using the following search terms: (sepsis or septic) and (angiotensin-converting enzyme or ACE) and (polymorphism or mutation or variant). The last search was updated on 11 September 2012. We also carefully reviewed all reference lists of the relevant articles for additional relevant papers. No language limitation was imposed.
Study selection
Studies were included if all of the following conditions were met: (1) evaluation of the ACE I/D polymorphism and risk of sepsis or sepsis mortality; (2) case–control study or cohort study; (3) reported ACE genotype as II vs. ID vs. DD. Studies were excluded if one of the following existed: (1) not relevant to ACE I/D polymorphism, sepsis or mortality; (2) non-clinical studies; (3) reviews or comments.
Data extraction
The following data were abstracted from each article: first author’s surname; publication year; ethnicity; study design; age; numbers of cases and controls; outcomes; genotype numbers in cases and controls. The data were extracted and independently entered into two databases by two of the authors (Hou and Zhang), who were blind to journal names, institutions and funding grants.
Statistical analysis
Where the data from at least three similar studies were available, the meta-analysis was performed. The strength of the associations between the ACE I/D polymorphism and risk of sepsis and death were measured by odds ratio (ORs) with 95% confidence intervals (CIs). Because there is often no clear evidence of the genetic mode of inheritance in complex disease genes, we used a pooling method that did not a priori assume a genetic model and avoided the problem of multiple comparisons. 20 OR1, OR2 and OR3 were assessed for genotypes DD versus II, ID versus II, and DD versus ID, respectively. These pairwise differences were used to indicate the most appropriate genetic model as follows: if OR1 = OR3 ≠ 1 and OR2 = 1, then a recessive model was suggested; if OR1 = OR2 ≠ 1 and OR3 = 1, then a dominant model was suggested; if OR2 = 1/OR3 ≠ 1 and OR1 = 1, then a complete over-dominant model was suggested; if OR1 > OR2 > 1 and OR1 > OR3 > 1 (or OR1 < OR2 < 1 and OR1 < OR3 < 1), then a co-dominant model was suggested.20–25 Once the best genetic model was identified, this model was used to collapse the three genotypes into two groups (except in the case of a co-dominant model) and to pool the results again.
Heterogeneity among studies was examined with I2 statistic interpreted as the proportion of total variation contributed by between-study variation. A random-effects model was used to calculate the pooled ORs. The significance of the pooled OR was determined by the Z-test and two-tailed p < 0.05 was considered to be statistically significant. Departure from Hardy–Weinberg equilibrium (HWE) in controls was tested by the χ2 test. Subgroup analyses were carried out by age. To validate the credibility of outcomes in this meta-analysis, sensitivity analysis was performed by sequential omission of individual studies. Evidence of publication bias was determined by visual inspection of the funnel plot and the degree of asymmetry was tested using Egger’s test. 26 All statistical tests were performed using Revman 5.1 software (Nordic Cochrane Center, Copenhagen, Denmark) and STATA 11.0 software (Stata Corporation, College Station, TX, USA).
Results
Eligible studies
Figure 1 shows the study selection process. The literature search yielded 42 references. After discarding overlapping references and those that clearly did not meet the criteria, a total of six case–control studies and two cohort studies were included in this meta-analysis.11–18 All studies were performed in a Caucasian population. There were five studies of a pediatric population11–13,15,17 and three studies of an adult population.14,16,18 Five case–control studies indicated that the distribution of genotypes in the controls was consistent with HWE. However, one study conducted by Celik et al. 15 was not consistent with HWE. The characteristics of the selected studies are presented in Table 1. Genotype numbers and HWE examination results are shown in Table 2.

Flow of study identification, inclusion and exclusion.
Characteristics of the studies included in meta-analysis.

NA: not available.
Distribution of ACE I/D polymorphism genotype among patients with sepsis and controls.

NA: not available.
Meta-analysis
Six studies determined the association between ACE I/D polymorphism and sepsis risk.12–17 Total sample sizes for sepsis and control were 735 and 1902, respectively. The estimated OR1, OR2 and OR3 were 0.76, 1.06, and 0.74, respectively (Table 3). These estimates suggested a recessive genetic model; therefore, ID and II were combined and compared with DD. The pooled OR was 0.75 (95% CI 0.62–0.91, p = 0.004) (Figure 2). In the subgroup analysis by age, a significant association was found among the pediatric population (OR = 0.72, 95% CI 0.54–0.96, p = 0.03). As shown in Figure 3, the most influencing single study on the overall pooled estimates seemed to be the study conducted by Cogulu et al. 13 The OR was 0.80 (95% CI 0.65–0.99, p = 0.04) after the removal of that study. These data suggested high stability of the results.
Determination of the genetic effect of ACE I/D polymorphism on sepsis and subgroup analyses.

R: random-effects model.

Meta-analysis for the association between sepsis risk and the ACE I/D polymorphism.
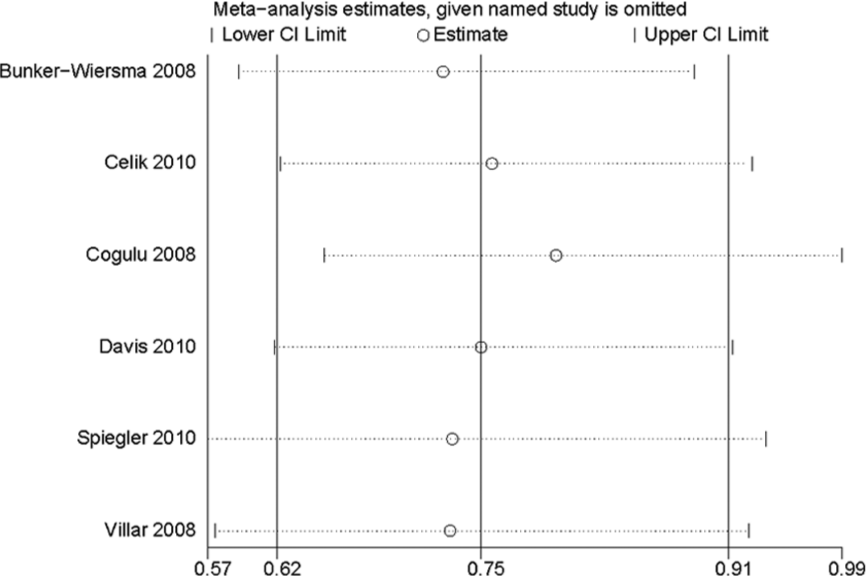
Influence analysis of the summary odds ratio coefficients on the association for the ACE I/D polymorphism with sepsis risk.
Five studies identified an association between the ACE I/D polymorphism and sepsis-related mortality risk.11,13–15,18 Figure 4 shows that there was no significant association between ACE I/D polymorphism and sepsis-related mortality with an OR of 0.84 (95% CI 0.57–1.24, p = 0.38). In the subgroup analysis by age, the results were similar in showing no genetic effect (OR = 0.65, 95% CI 0.26–1.60, p = 0.35). Figure 5 shows that the study performed by Tsantes et al. 18 had the most influence on the overall pooled estimates. However, the sensitivity analysis showed that the OR was 0.73 (95% CI 0.44–1.22, p = 0.23) after the removal of that study respectively, indicating high stability of the results. Summary results of comparisons are listed in Table 3.

Meta-analysis for the association between mortality risk and the ACE I/D polymorphism.

Influence analysis of the summary odds ratio coefficients on the association for the ACE I/D polymorphism with mortality risk.
Publication bias
Publication bias was examined by funnel plots qualitatively and estimated by Egger’s tests quantitatively. Funnel plots suggested no publication bias was observed (Figures 6 and 7). Furthermore, Egger’s tests did not show evidence of publication bias (p = 0.823 and p = 0.546, respectively).

Begg’s funnel plot for sepsis risk and ACE I/D polymorphism.

Begg’s funnel plot for mortality risk and ACE I/D polymorphism.
Discussion
Sepsis disrupts cardiovascular homeostasis by multiple mechanisms, including dehydration, mechanical contraction of the heart, variable effect on energy metabolism and altered vasoregulation and distribution of blood flow. 27 The accumulative effect of these mechanisms leads to hypotension. This meta-analysis of eight studies systematically evaluated the association between the ACE I/D polymorphism and sepsis risk and mortality risk. We found that the DD genotype was a protective factor for developing sepsis in the overall study population. The result showed that carriers of the DD genotype had 25% decreased sepsis risk compared to those individuals with the ID or II carriers. In the subgroup analysis, we found that individuals carrying the DD genotype had a decreased sepsis risk in a pediatric population. There were only two case–control studies performed using adult populations. Thus, subgroup analysis was not performed in this population. However, the statistically significant association between ACE I/D and sepsis risk in adults could not be ruled out because of the limited sample size. More studies with adult population are needed to evaluate the effect of the ACE I/D polymorphism on sepsis risk. In addition, our meta-analysis demonstrated that there was no significant association between the ACE I/D polymorphism and sepsis-related mortality. Moreover, there was also no significant association between the ACE I/D polymorphism and mortality in a pediatric population. There are two potential explanations for the negative result. First, only five studies including 889 patients evaluated the association between the ACE I/D polymorphism and mortality risk. Therefore, the positive association between this polymorphism and sepsis-related mortality should not be excluded, because studies with small sample sizes may have insufficient statistical power to detect a slight effect. Second, in addition to genetic predisposition, other factors, such as severity of sepsis, complications and medical treatment, are also thought to play a crucial role in the prognosis of sepsis. These data should be considered in further studies.
The RAS is important for regulating systemic blood pressure and volume. ACE transforms Ang I into Ang II, an octapeptide hormone that has potent hemodynamic effects. During hypotensive states, Ang II is primarily produced to increase vascular tone and systemic arterial blood pressure. A previous study reported that decreased serum ACE activity was found in patients with sepsis. 28 A recent study found that non-sustained hypotension in the emergency department conferred a significantly increased risk of death during hospitalization in patients admitted with sepsis. 29 Thus, high ACE activity may be beneficial for septic patients, especially patients with hypotension. The ACE I/D polymorphism could regulate the concentration of serum ACE. 8 Therefore, it is biologically plausible that the ACE I/D polymorphism could influence the risk of sepsis.
Recently, Cardinal-Fernandez and colleagues showed that the presence of the allele D of the ACE gene is associated with acute respiratory distress syndrome (ARDS) in patients with severe sepsis. 30 Thus, it was proposed that ACE inhibition therapies might be useful to reduce ARDS risk in severe sepsis. However, we found that DD genotype carriers had a decreased sepsis risk compared to ID or II carriers, suggesting that ACE inhibitors may be harmful for septic patients. The goal of providing personalized care to each patient with sepsis is difficult to achieve. Randomized controlled trials are needed to examine whether the use of this medication in patients hospitalized with sepsis may be beneficial.
Heterogeneity is a potential problem when interpreting the results of all meta-analyses. In this present meta-analysis, we did not find obvious heterogeneity (I2 = 0% and I2 = 11%). Additionally, funnel plots and Egger’s tests suggested no publication bias. Thus, it seemed that heterogeneity and publication bias did not influence the results. Furthermore, sensitivity analyses were carried out. Excluding each study did not alter the conclusions of sepsis risk and mortality risk, suggesting high reliability of our results.
Several limitations need to be addressed. First, only eight published studies fulfilled our selection criteria. The sample size was still relatively small and thus may not be sufficient enough to detect a possible minor effect of ACE I/D polymorphism on mortality risk. Second, all of the studies were performed in a Caucasian population. Thus, our results may be applicable only to Caucasians. Third, our results were based on unadjusted estimates. A lack of the original data of eligible studies limited the evaluation of the effects of the gene–gene interactions in sepsis. Finally, the controls for one study included in this meta-analysis were not in HWE. 15 However, the result was not changed after omitting this study.
Conclusion
In summary, this meta-analysis suggested that the ACE I/D polymorphism may be associated with the risk of sepsis. However, this polymorphism was not associated with sepsis mortality. Well-designed studies with larger sample sizes and more ethnic groups should be considered to further clarify these associations.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.