
Abstract
Introduction:
The purpose of this study is to examine whether the insertion (I) and deletion (D) polymorphism of the angiotensin-converting enzyme (ACE) confers susceptibility to aortic aneurysms (AAs).
Materials and methods:
A meta-analysis was conducted on the associations between the ACE I/D polymorphism and all AAs and abdominal aortic aneurysms (AAAs).
Results:
Ten studies consisting of 2784 cases and 2682 controls were available for the meta-analysis. Meta-analysis showed a significant association between the D allele and all types of AA (OR 1.378, 95% CI 1.103–1.723, p = 0.005) and AAA (OR 1.274, 95% CI 1.004–1.617, p = 0.046). Meta-analysis of both the DD genotype and the DD vs. II genotype showed an association with AAAs. Stratification by ethnicity indicated an association between the D allele of the ACE I/D polymorphism and AAAs in Europeans (OR = 1.338, 95% CI = 1.026–1.745, p = 0.031), but not in Asians (OR = 0.927, 95% CI = 0.660–1.303, p = 0.663). Furthermore, analysis using the recessive model, dominant model, and homozygote contrast all showed the same pattern for the D allele.
Conclusions:
Our meta-analysis demonstrates that the ACE I/D polymorphism is associated with susceptibility to AAAs in European populations.
Introduction
Aortic aneurysms (AAs) are characterized by the degradation of structural proteins, including both collagen and elastin. Abdominal aortic aneurysm (AAA) is a chronic degenerative condition characterized by the segmental weakening and dilatation of the aortic wall and is the most common type of AA. 1 Although the etiology of AAs is not fully understood, having a susceptible genetic background to certain environmental factors as well as inflammatory processes and proteases like metalloproteinase have been reported as causes of AAs.1,2
Angiotensin-converting enzyme (ACE) converts angiotensin I into angiotensin II and inactivates bradykinin via the kallikrein-kininogen system. 3 Angiotensin II is the main effector molecule of the renin-angiotensin system (RAS), is pleiotropic, and is a mediator of the development and progression of diseases. 4 Furthermore, angiotensin II is a potent pro-inflammatory modulator that augments and perpetuates the immune response. 4 Angiotensin II infusion produces large AAAs in animals and ACE is highly expressed in the tissues of the human aneurysmal aorta. Thus, increased local angiotensin II formation may play a key role in the development of AAs. The ACE gene, which is located on chromosome 17q23, contains an insertion/deletion (I)/(D) polymorphism within intron 16 that may contain or lack a 287 basepair repeat sequence. 5 The DD genotype is associated with approximately a two-fold increase in both tissue and plasma concentrations of ACE over the II genotype. 5 Thus, it seems possible that the D allele could play a role in the pathogenesis of AAs.
The ACE I/D polymorphism has been studied in the context of AAs. However, the published results on the genetic association of the ACE I/D polymorphism with AAs are controversial and inconclusive.6–15 This may be because of small sample sizes, low statistical power, and/or clinical heterogeneity. In order to overcome the limitations of individual studies, resolve inconsistencies, and reduce the likelihood that random errors were responsible for false-positive or false-negative associations, we employed a meta-analysis to further characterize the association.16–18 In the present study, we used a meta-analysis to investigate whether the ACE I/D polymorphism contributes to the susceptibility of AAs.
Materials and methods
Identification of eligible studies and data extraction
A literature search was conducted for studies that examined the association between the ACE I/D polymorphism and AAs. We utilized the MEDLINE and EMBASE citation indices to identify articles in which the ACE I/D polymorphism was determined in patients with AAs and controls (through November 2012). In addition, all of the references that were cited in the identified articles were reviewed in order to identify studies that were not indexed by either MEDLINE or EMBASE. The following keywords and subject terms were used in our search: angiotensin-converting enzyme, ACE, and aortic aneurysm. Studies were included in the analysis if: (1) they were case-control studies; (2) contained original data; and (3) contained sufficient data to calculate odds ratios (ORs). No language restrictions were applied. We excluded the following: (1) studies containing overlapping data; (2) studies in which the number of null and wild genotypes or alleles could not be ascertained; (3) studies in which family members had been studied because their analysis was based on linkage considerations; and (4) studies in which the genotype distribution of controls were not in Hardy-Weinberg Equilibrium (HWE), because deviation from HWE among controls suggests the possibility of bias during control selection or genotyping errors. The following information was extracted from each identified study: author, year of publication, ethnicity of the study population, demographics, number of cases and controls, the frequencies of the genotypes and alleles of the ACE I/D polymorphism, and the type of AA.
Evaluation of publication bias and study quality
The chi square test was used to determine if the observed genotype frequencies among the controls conformed to Hardy-Weinberg (H-W) expectations. Funnel plots are generally used to detect publication bias, but these plots require a number of studies that vary in size and subjective judgments, and thus, we evaluated the publication bias using the Egger’s linear regression test. 19 Egger’s linear regression measures funnel plot asymmetry on a natural logarithmic scale of ORs. When asymmetry was indicated, we used the “trim and fill” method to adjust the summary estimate for the observed bias. 20
Evaluation of statistical associations
We performed meta-analyses using (1) the allelic contrast (D vs. I); (2) the recessive (DD vs. ID + II); (3) the dominant (DD + ID vs. II); and (4) the homozygote contrast (DD vs. II) models. Point estimates of risks, ORs, and 95% confidence intervals (CIs) were estimated for each study. In addition, within- and between-study variations and heterogeneities were assessed using Cochran’s Q-statistic. Cochran’s Q-statistic assesses the null hypothesis that all studies evaluated the same effect. The effect of heterogeneity was quantified using I2, with a range between 0% and 100%, which represents the proportion of between-study variability that is attributable to heterogeneity rather than chance. 21 I2 values of 25%, 50%, and 75% were nominally assigned as low, moderate, and high estimates, respectively. The fixed-effects model assumes that a genetic factor has a similar effect on disease susceptibility across all studies investigated and that observed variations among studies are caused by chance alone. 22 The random-effects model assumes that different studies show substantial diversity and assesses both within-study sampling error and between-study variance. 23 When study groups are homogeneous, the two models are similar to one another. If the study groups lack homogeneity, then the random-effects model usually provides wider CIs than the fixed-effects model. The random-effects model is most appropriate in the presence of significant between-study heterogeneity. 23 Statistical manipulations were performed using the Comprehensive Meta-Analysis computer program (Biosta, Englewood, NJ, USA). The power of each study was computed as the probability of detecting an association between the ACE polymorphism and AAs using a significance level of 0.05 and assuming an OR of 1.5 (small-effect size). Power analysis was performed using the statistical program G*Power (http://www.psycho.uni-duesseldorf.de/aap/projects/gpower).
Results
Studies included in the meta-analysis
Eighteen studies were identified by an electronic and manual search and 15 were selected for a full-text review based on the title and abstract details (Figure 1).6–15,24–28 Five studies were excluded from our analysis because three contained no data,26–28 one had a genotype distribution in the control group that was not in HWE, and another was not a case-control study.24,25 Thus, a total of 10 studies met our inclusion criteria.6–15 These studies comprised seven AAAs, and one each of thoracic aortic dissection (TAD), aortic dissection (AD), and type I AD. They consisted of six European, two Asian, and two Turkish studies, and in total, they included 2784 cases and 2682 controls. Selected details of the individual studies are summarized in Table 1. The statistical powers of these 10 studies ranged from 9.5% to 91.6%. Two of the studies had a statistical power that exceeded 80%.

Study flowchart.
Details of the individual studies included in the meta-analysis.

Ref: citation reference; TAD: thoracic aortic dissection; AAA: abdominal aortic aneurysm; AD: aortic dissection; OR: odds ratio; CI: confidence interval; HWE: Hardy-Weinberg equilibrium; a: Power calculations assume α = 0.05, OR = 1.5.
Frequencies of the D allele of the ACE I/D polymorphism in different ethnic groups
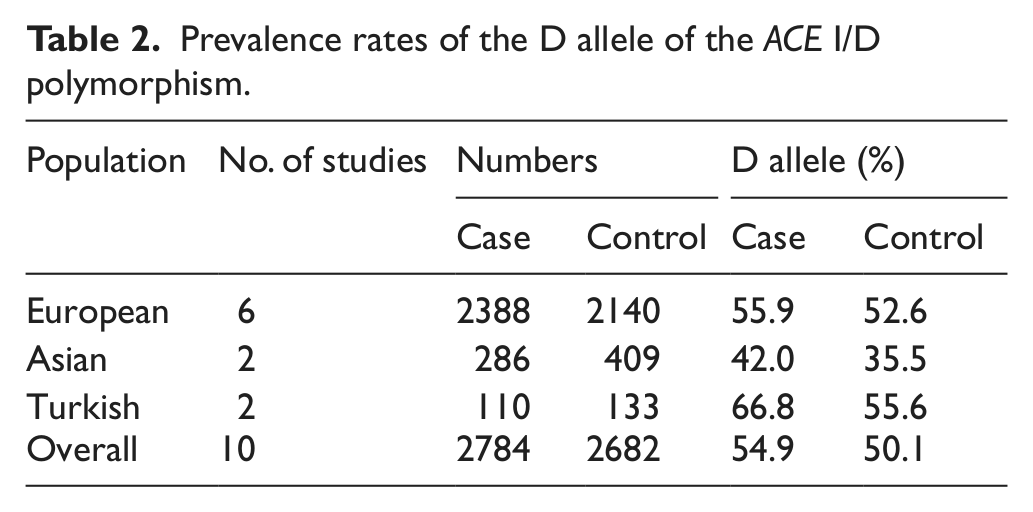
The mean frequency of the D allele of the ACE I/D polymorphism was 50.1% among all normal controls, and Asians had the lowest D allele prevalence of the other ethnic groups tested in this study (35.5%). Among the normal controls, the frequencies of the D allele in the Asian, European, and Turkish populations were 35.5%, 52.6%, and 55.6%, respectively (Table 2).
Prevalence rates of the D allele of the ACE I/D polymorphism.
Meta-analysis of the association between the ACE I/D polymorphism and AAs
Meta-analysis was performed on all AA cases and on patients with AAAs. A summary of the meta-analysis findings of the relationship between the ACE I/D polymorphism and AAs is provided in Table 3. Meta-analysis revealed a significant association between the D allele and AAs (OR 1.378, 95% CI 1.103–1.723, p = 0.005) (Table 3, Figure 2). Furthermore, analysis using both the recessive and dominant models, and the homozygote contrast, showed the same pattern for the D allele of the ACE I/D polymorphism, showing an association between the D allele and all types of AAs (Table 3). Stratification by ethnicity indicated an association between the D allele of the ACE I/D polymorphism and AAs in Europeans (OR = 1.338, 95% CI = 1.026–1.745, p = 0.031), but not in Asians (OR = 1.250, 95% CI = 0.706–2.215, p = 0.444).
Meta-analysis of the association between the ACE I/D polymorphism and aortic aneurysms and abdominal aortic aneurysms in the overall group.

ACE I/D: angiotensin-converting enzyme insertion and deletion polymorphism; AA: aortic aneurysm; AAA: abdominal aortic aneurysm; OR: odds ratio; CI: confidence interval; F: fixed-effects model; R: random-effects model.
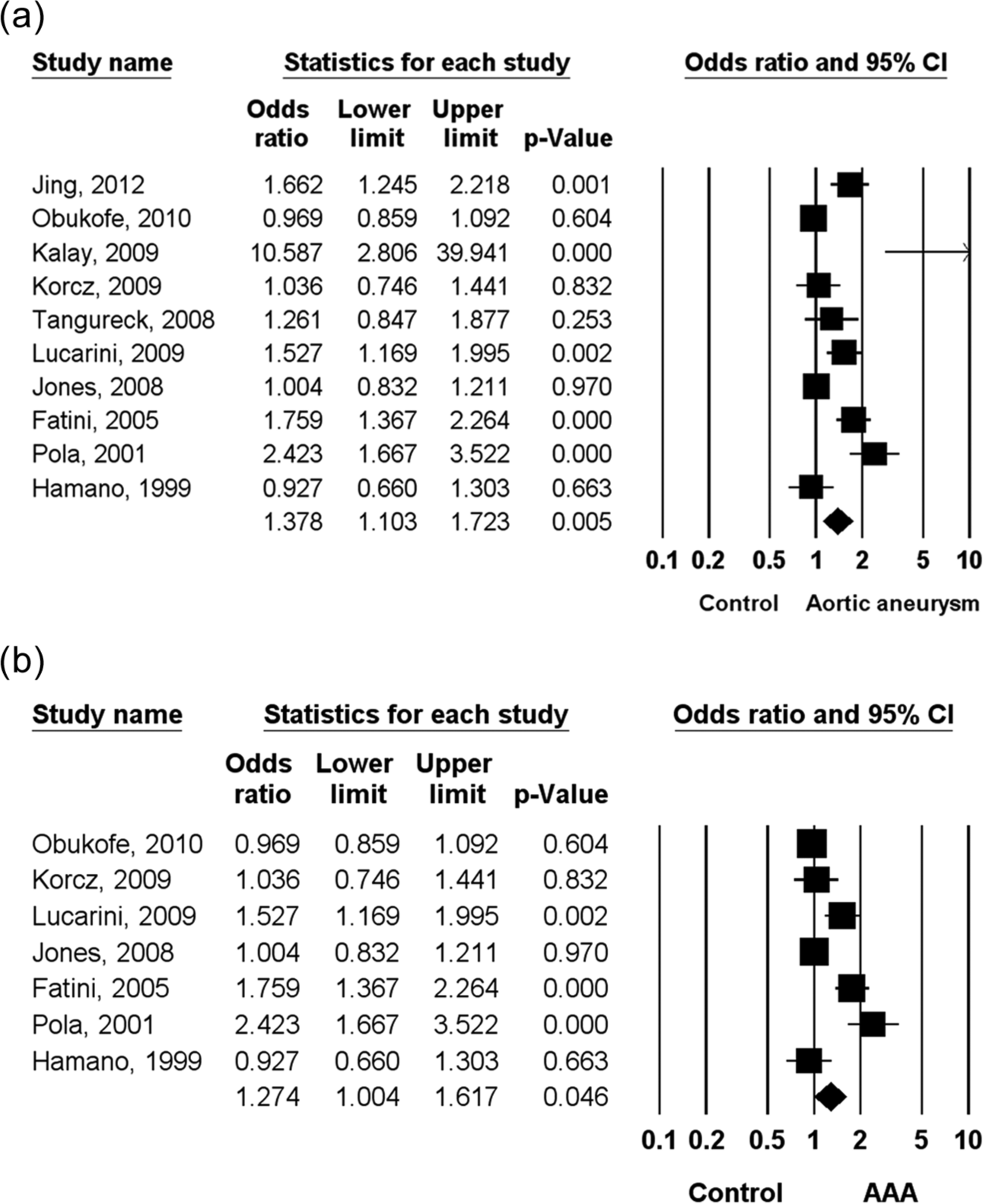
ORs and 95% CIs of individual studies and pooled data for the association between the D allele of the ACE I/D polymorphism and aortic aneurysms (a) and abdominal aortic aneurysms (b) in the overall group. ORs: odds ratios; CIs: confidence intervals; ACE I/D: angiotensin-converting enzyme insertion and deletion polymorphism.
Meta-analysis of the association between the ACE I/D polymorphism and AAAs
A summary of the meta-analysis findings concerning the associations between the ACE I/D polymorphism and AAAs is shown in Tables 3 and 4. The overall OR for the D allele was significantly higher in AAAs (OR 1.274, 95% CI 1.004–1.617, p = 0.046) (Table 3, Figure 2). Meta-analysis of the DD genotype and the DD vs. II genotype showed an association with AAA (OR 1.397, 95% CI 1.024–1.906, p = 0.035; OR 1.551, 95% CI 1.032–2.378, p = 0.044, respectively), whereas no such relation was found for the DD + ID genotype (Table 3). Stratification by ethnicity indicated an association between the D allele of the ACE I/D polymorphism and AAAs in Europeans (OR = 1.338, 95% CI = 1.026–1.745, p = 0.031), but not in Asians (OR = 0.927, 95% CI = 0.660–1.303, p = 0.663) (Figure 3, Table 4). Furthermore, analysis using the recessive model, dominant model, and homozygote contrast all showed the same pattern for the D allele in European and Asian populations, which showed an association between the ACE I/D polymorphism and AAAs in Europeans (Table 4).

ORs and 95% CIs of individual studies and pooled data for the association between the D allele of the ACE I/D polymorphism and abdominal aortic aneurysms in each ethnic group studied. ORs: odds ratios; CIs: confidence intervals; ACE I/D: angiotensin-converting enzyme insertion and deletion polymorphism.
Meta-analysis of the association between the ACE I/D polymorphism and abdominal aortic aneurysms in the European and Asian populations.

ACE I/D: angiotensin-converting enzyme insertion and deletion polymorphism; OR: odds ratio; CI: confidence interval; F: fixed-effects model; R: random-effects model; NA: not available.
Heterogeneity and publication bias
Between-study heterogeneity was found during the meta-analyses of all types of AAs and AAAs. Thus, the meta-analysis was performed using a random-effects model whenever heterogeneity was present in a population (Tables 3 and 4). Publication bias causes a disproportionate number of positive studies, and this poses a problem for meta-analyses. Evidence of publication bias was found for the meta-analyses of the D allele of the ACE I/D polymorphism in all types of AAs (Egger’s regression test p values = 0.023). However, the adjusted OR that was calculated using the trim and fill technique remained significant (OR 1.378, 95% CI 1.103–1.723, p = 0.005).
Discussion
ACE is expressed in a number of tissues including the kidneys, heart, lungs, vascular endothelium, skin, joints, and testes. ACE plays an important role in RAS and angiotensin II conversion, it directly increases vascular smooth muscle cell contraction, and it also affects smooth muscle proliferation, monocyte adhesion, platelet adhesion, and aggregation. Angiotensin II also acts as a potent pro-inflammatory modulator.4,29 The ACE I/D polymorphism is located within an intron of the ACE gene, and is in strong linkage disequilibrium with genetic factors that influence serum ACE levels. 5 In fact, the ACE I/D polymorphism accounts for approximately half of the variance in ACE plasma levels in humans. ACE activity is higher in patients with the D allele, which results in an increase of angiotensin II. 5 Furthermore, this polymorphism has been studied in several diseases, including Alzheimer’s disease, myocardial infarction, cerebral infarction, hypertension, and diabetic nephropathy. These studies also reported associations between the susceptibilities to these diseases and the DD genotype and the D allele of the ACE I/D polymorphism.30–43 In animal models, angiotensin II infusion induces AAA formation and the inhibition of RAS reduces aortic elastic degradation. 44 ACE inhibitors showed a decreased risk of aneurysm rupture. 45
In this meta-analysis, we combined the evidence of the associations between the ACE I/D polymorphism and the susceptibility to AAAs. Meta-analysis revealed that the overall OR for the D allele was significantly higher in AAAs (OR 1.274, 95% CI 1.004–1.617, p = 0.046). Stratification by ethnicity indicated an association between the ACE I/D polymorphism and AAAs in Europeans (OR for the D allele = 1.338, 95% CI = 1.026–1.745, p = 0.031). Our findings support the notion that the ACE I/D polymorphism has a role in the pathogenesis of AAAs in Europeans.
ACE is highly expressed in an aneurysmal aorta. 46 Higher ACE activity in cardiac tissue results in higher angiotensin II levels. Increased angiotensin II levels may lead to the remodeling of vascular tissue through the activation of growth factors and inflammation. 46 Experimental data show a relationship between angiotensin II and AA formation. 44 Angiotensin II promotes hypertension and alters shear stress. RAS plays an important role in the modulation of vascular tone, and ACE plays a key role in regulating RAS activity. 4 Moreover, because the ACE I/D polymorphism accounts for approximately half of the variance in ACE plasma levels, 5 it is likely that the ACE I/D polymorphism plays a role in the susceptibility of AAAs.
The ACE I/D polymorphism may influence the antihypertensive response of ACE inhibitors (ACEI). The ACEI has been known to be associated with better response for hypertension in the DD genotype compared with the II genotype. 47 Our meta-analysis confirmed the association between the ACE I/D polymorphism and AAAs. Thus there is a possibility that the ACEI use is associated with better clinical improvement of AAAs in patients carrying the DD genotype in comparison with the II genotype. Further evaluation is needed to clarify the relation between the ACE I/D polymorphism and response to ACEI therapy in patients with AAAs.
The present study has some limitations that should be considered. First, heterogeneity and confounding factors may have distorted the analysis. Publication bias may also have affected the analysis, since studies that produced negative results may not have been published or may have been missed. Second, another polymorphism located in the ACE gene that may have been capable of affecting ACE activity could also have been associated with AAs. However, the limited amount of data available prevented further meta-analysis. Third, there are varying levels of severity of AAs and the severity of these AA cases was unclear. Further research is required in order to examine whether an association exists between the ACE I/D polymorphism and the severity and clinical features of AAs. Fourth, we included data from European, Asian, and Turkish patients in our meta-analysis, but our ethnicity-associated results are applicable to only the European ethnic groups.
In conclusion, this meta-analysis of the ACE I/D polymorphism demonstrates that the ACE I/D polymorphism is associated with susceptibility to AAAs in Europeans. Accordingly, our findings support the notion that the ACE I/D polymorphism has a role in the pathogenesis of AAAs in Europeans. Larger-scale studies in populations with different ethnicities are required to further explore the relationships between the polymorphisms of the ACE gene and the pathogenesis of AAAs.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.