
Abstract
There is preliminary evidence that the local renin-angiotensin system (RAS) could affect neoplastic hematopoiesis. The aim of this study is to search messenger RNA (mRNA) expressions of the essential RAS elements in myeloid and lymphoid hematological neoplastic disorders. Forty-six patients with newly diagnosed myeloid (AML, biphenotypic leukemia, CML) or lymphoid (CLL, NHL, B-ALL, T-ALL) hematological disorders were included in the study. In the lymphoid group, the median expression values of RENIN, ACE1, ACE2 and ANGIOTENSINOGEN (ANGTS) mRNAs were 1.96%, 0.42%, 0.00% and 0.00%, respectively; in the myeloid group, 0.73%, 1.55%, 0.04% and 0.006%, respectively. In the lymphoid group, RENIN levels were significantly higher (p = 0.001), whereas ACE1 and ACE2 levels were significantly higher in the myeloid group (p values were 0.013 and 0.010, respectively). ANGTS levels were similar in both groups. In patients with non-ALL lymphoid malignancies, RENIN expressions were significantly higher when compared to ALL patients (p = 0.004). All patients with active disease had significantly higher RENIN mRNA expression levels than patients without active disease (2.03% vs 0.30%) (p = 0.034). The result of our present study indicates that the activities of local RAS may differ in distinct disease states such as leukemia and lymphomas.
Introduction
The concept of a local hematopoietic renin-angiotensin system (RAS) in bone marrow (BM) was first suggested in 1996.1,2 Locally active BM RAS affects critical steps of physiological and pathological blood cell production in autocrine, paracrine and intracrine ways.3,4 The stimulation of the angiotensin type 1 and 2 receptors (AT1/AT2) by angiotensin II (Ang II), the principal effector molecule of the RAS, exerts an stimulatory/inhibitory action on the janus-kinase-signal transducer and activator of transcription (JAK-STAT) pathway, which is directly linked to activities of the erythropoietin, thrombopoietin and other hematopoietic cytokines during normal hematopoiesis and in myeloproliferative neoplasms.3,5,6 Local RAS is effective even at the stage of primitive embryonic hematopoiesis.7,8
There is preliminary evidence that local BM RAS could affect neoplastic hematopoiesis.9–16 Over-expression of the angiotensin-converting enzyme (ACE) (CD 143) surface antigen in leukemic myeloid blast cells have been detected by flow cytometric analyses. Moreover, a positive correlation has been found between the ACE and BM blast count. 11 ACE and p53 expressions were detected in the CD34+cells of patients with acute leukemia during and after induction chemotherapy. 17 ACE-expressing macrophages in lymph nodes of Hodgkin’s disease have been detected. 15 The renin system is present in the K562 leukemic cell line in vitro model. Multipotential, hematopoietic malignant K562 leukemic blast cells also exhibited significant expressions of RENIN, ANGIOTENSINOGEN (ANGTS) and ACE. 14
The purpose of this study is to research mRNA expressions of the essential RAS elements (RENIN, ANGTS, ACE1 and ACE2) in myeloid and lymphoid hematological neoplastic disorders. Elucidation of the presence of local RAS in the neoplastic myeloid and lymphoid pathological hematopoiesis is important because targeting the actions of local RAS may represent a valuable therapeutic option for the management of cancer.18–20
Materials and methods
Study population
The study group comprised 46 newly diagnosed myeloid (acute myeloid leukemia (AML), biphenotypic leukemia, chronic myeloid leukemia (CML)) or lymphoid (chronic lymphocytic leukemia (CLL), non-Hodgkin’s lymphoma (NHL), B cell acute lymphoblastic leukemia (B-ALL), T cell acute lymphoblastic leukemia (T-ALL)) hematological disorders. The diagnoses of hematological neoplasms were reached based on the criteria of the World Health Organization (WHO).21,22 Samples from BM were collected prior to the chemotherapy administered to each patient. The BM aspiration procedure from the iliac crest was performed only at the clinically indicated situation. At the time of the sample collection, all of the patients were in good health and well hydrated. Pediatric and adult patients receiving chemotherapy were excluded from this study. Written informed consent was obtained from all participants and the study protocol was approved by the local ethics committee of Hacettepe University with project number LUT 10/45.
Isolation of RNA and synthesis of cDNA
BM samples were collected in 2-ml ethylenediaminetetraacetic acid (EDTA) tubes. Total RNA was isolated according to the manufacturer’s instructions (Qiagen, Germany). RNA quality was measured by spectrophotometer (ND-1000, Nanodrop Technologies, Inc., USA), and one microgram of total RNA was used. Random primers (20 µM, Roche Diagnostics, Germany), dNTP set 10 mM, Fermentas UAB, Lithuania), RiboLock Rnase Inhibitor (20 U/µl, Fermentas) and Moloney murine leukemia virus (MMLV) reverse transcriptase (200 U/µl, Fermentas) were used for cDNA synthesis. cDNA samples were stored at −20°C.
Quantitative real-time polymerase chain reaction (PCR) analysis (qRT-PCR)
We searched for the gene expression of the major RAS components (ACE1, ACE2, RENIN and ANGTS) in myeloblasts and lymphoid hematopoietic cells by qRT-PCR. The probes used in this study were designed by Universal Probe Library (UPL, http://www.roche-applied-science.com/sis/rtpcr/upl/index.jsp). The primer forward and reverse sequences used in this study are shown in Table 1. mRNA expression levels were normalized to three reference genes (CYPA, B-ACT and ABL).
The primer sequences-probe sets.

UPL: Universal Probe Library, ACE: angiotensin-converting enzyme; ANGTS: angiotensinogen.
qRT-PCR analyses for ACE, RENIN and ANGTS gene expressions were performed using a LightCycler 480 instrument (Roche Diagnostics). Real-time amplification was performed with a final reaction mixture of 20 µl containing 5 µM of each primer, 0.5 µM of each probe, LightCycler 480 Probe Master Mix and 100 ng/µl of cDNA. Each sample was studied in duplicate and all runs were repeated twice. The PCR protocol was as follows: initial denaturation at 95°C for 7 min, amplification segment at 5 sec at 95°C, 10 sec at 60°C, and 10 sec at 72°C for 45 cycles.
The 2–ΔΔCt method was used to calculate relative expression levels determined from the RT-PCR experiments. 23
Statistical analyses
Statistical Packages for the Social Sciences v13.0 (SPSS Inc., Chicago, IL, USA) software was used for all statistical analyses. The results were given as the mean ± standard error for the data with normal distribution, and as median (min-max) for the data without a normal distribution and ratio for the nominal data. Data distribution was tested with Kolmogorow-Smirnow’s test. Homogeneities of variances were evaluated with Levene’s test. Nonparametric tests were used since the sample sizes of the groups were small. Differences between two groups were assessed by the Mann-Whitney U test. A p value of ≤ 0.05 was considered as statistically significant.
Results
BM samples were obtained from 46 patients, with lymphoid (n = 30) or myeloid (n = 16) hematological neoplasms (Table 2). The comparison of the two groups on the basis of biochemical parameters yielded significantly higher concentrations of hemoglobin, platelet, creatinine and calcium levels in the lymphoid group; while lactate dehydrogenase levels were significantly higher in the myeloid group.
The hematological diagnoses of patients with lymphoid and myeloid neoplasms.

CLL: chronic lymphoid leukemia; NHL: Non-Hodgkin’s lymphoma; ALL: acute lymphoblastic leukemia: AML: acute myeloid leukemia; APL: acute promyelocytic leukemia; CML: chronic myeloid leukemia.
RENIN, ACE1, ACE2 and ANGTS mRNA expressions
Specific mRNA expressions for the components of the RAS were detected in the BM samples by qRT-PCR analysis. RENIN mRNA expression levels were found to be significantly higher in the samples of the lymphoid group compared to the samples of the myeloid group. Seven of the nine AML patients, and all ALL (B- and T-) patients expressed RENIN. Only two AML patients with minimal differentiation/without maturation did not express RENIN. On the other hand, ACE1 and ACE2 mRNA expressions were found to be significantly higher in myeloid group patients when compared to the lymphoid group (Tables 3 and 4).
RENIN, ACE1, ACE2 and ANGIOTENSINOGEN mRNA expression levels of lymphoid and myeloid group patients.

RNA: ribonucleic acid; ACE: angiotensin-converting enzyme; ANGTS: angiotensinogen.
RENIN, ACE1, ACE2 and ANGIOTENSINOGEN mRNA expression levels of non-ALL patients and myeloid group patients.

ALL: acute lymphoblastic leukemia; RNA: ribonucleic acid; ACE: angiotensin-converting enzyme; ANGTS: angiotensinogen.
We also analyzed separately ALL and non-ALL patients versus those in the myeloid group. RENIN expressions were significantly higher in non-ALL patients, similar to all lymphoid patients, and ACE expressions were significantly lower than the myeloid group expressions. However, in ALL patients vs those in the myeloid group, there was borderline significance with respect to ACE2 mRNA expression levels in favor of the myeloid group (Table 5). There was no difference between ALL patients and non-ALL patients in terms of ACE1, ACE2 and ANGTS gene expression levels (p = 0.082, p = 0.803, p=0.977, respectively). On the other hand, RENIN expressions of non-ALL patients were significantly higher when compared to ALL patients (p = 0.004).
RENIN, ACE1, ACE2 and ANGIOTENSINOGEN mRNA expression levels of ALL patients and myeloid group patients.
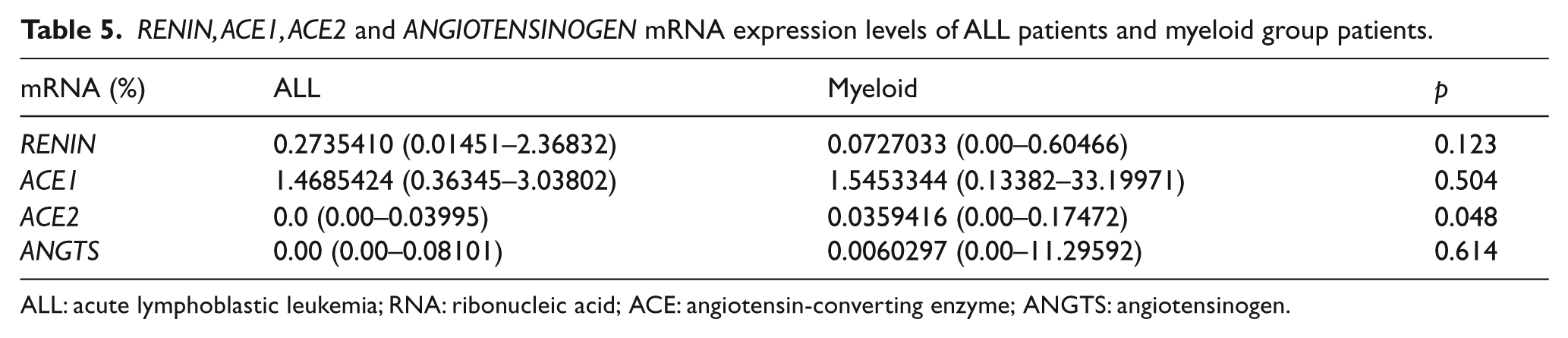
ALL: acute lymphoblastic leukemia; RNA: ribonucleic acid; ACE: angiotensin-converting enzyme; ANGTS: angiotensinogen.
Active disease status in all patients
RENIN mRNA expression levels of patients with active disease were significantly higher than those from patients without active disease (p = 0.034). No significant statistical difference existed between the patients with or without active disease with respect to the ACE1, ACE2 and ANGTS (Table 6) mRNA expression levels.
RENIN, ACE1, ACE2 and ANGIOTENSINOGEN mRNA expression levels of all patients with or without active disease.

RNA: ribonucleic acid; ACE: angiotensin converting enzyme; ANGTS: angiotensinogen
Active disease status in lymphoid group
RENIN, ACE1, ACE2 and ANGTS mRNA expression levels were similar in patients with and without active disease (Table 7). All patients with ALL had active disease at the time of diagnosis. However, the rest of the lymphoid group (CLL, NHL) included patients with or without active disease. We re-analyzed the data by separating the ALL patients from the rest of the lymphoid group; the RENIN, ACE1, ACE2 and ANGTS mRNA expressions of the patients with or without active disease were similar.
RENIN, ACE1, ACE2 and ANGIOTENSINOGEN mRNA expression levels of lymphoid group patients with or without active disease.
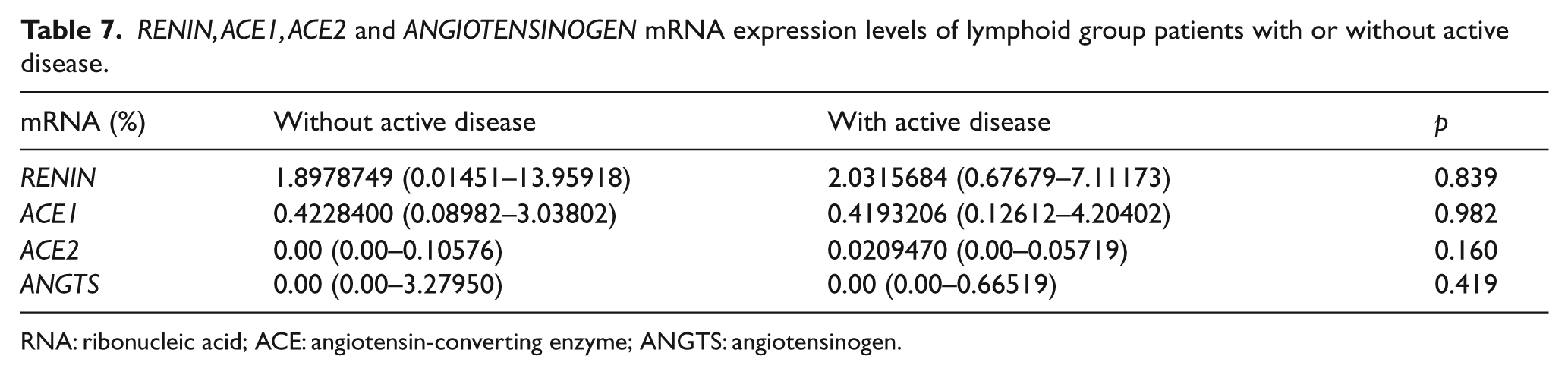
RNA: ribonucleic acid; ACE: angiotensin-converting enzyme; ANGTS: angiotensinogen.
Discussion
In this study, specific mRNA expressions of the components of the RAS (RENIN, ANGTS, ACE1 and ACE2) were detected in the BM of patients with myeloid and lymphoid hematological neoplastic disorders. RENIN expression levels were significantly higher in the lymphoid group, whereas ACE1 and ACE2 expression levels were significantly higher in the myeloid group. Moreover, RENIN expression levels in all patients with active disease were significantly higher than in those without active disease. These data further support the original hypothesis that there is a local RAS in the BM affecting physiological and pathological hematopoiesis.1,2 The main RAS molecules, including renin, angiotensinogen, angiotensin receptors and ACE had been previously detected in the rat BM microenvironment. 24 We have found the same RAS molecules in human samples, indicating that local hematopoietic RAS is a universal autocrine-paracrine system. The results of our present study also indicate that the activities of local RAS may differ in distinct disease states such as leukemia and lymphomas.
Renin, as an aberrant leukemic marker of acute leukemia, was expressed in leukemia cell lines such as K562, KU812 and MEG-01.14,25,26 Renin-like enzyme activity due to specific immunoreactive renin-like peptide of 47 kDa converting angiotensinogen to Ang-I had been detected in leukemic myeloid blast cells.27,28 Increased activity of the renin gene was detected during the NUP98-HOXA9 enhanced blast formation.29,30 Gómez-Casares et al. previously disclosed renin expressions in cells from AML, CML and ALL. The highest frequency was observed in AML patients (47.2% of the cases). 25 Renin expression disappeared during the complete remission of AML.25,26 The same investigation team has analyzed 76 samples taken from patients with AML with follow-up of the positive patients. Thirty-one patients (41%) were positive for renin gene expression at diagnosis in their study. All of the renin-positive patients at diagnosis showed no expression during complete remission (CR), but expression recurred in those experiencing relapse and persisted when the disease was refractory to treatment. 26 In our study, RENIN expressions were found to be significantly higher in the lymphoid group in comparison to the myeloid group. After dividing the lymphoid group into two groups including ALL patients and non-ALL patients, we noticed that RENIN expressions were significantly higher in the non-ALL patient group when compared to RENIN expression levels of the ALL patient group. Thus, the difference of the RENIN expression levels between lymphoid and myeloid groups was likely to be due to the non-ALL patient group. Furthermore, RENIN gene expression levels of the patients with active disease were significantly higher than the expression levels of the patients without active disease (p = 0.034). These findings indicate that RENIN is an active molecule for both myeloid and lymphoid neoplastic disorders.
ACE existence throughout hematopoietic ontogeny7,8 indicates primitive hematopoiesis casts attention on the effects of RAS on neoplastic tissues. Immunohistochemical studies have shown the possible role of ACE/RAS in BM by evaluating ACE expression in normal BM, several myeloproliferative disorders and myelodysplasia. 31 ACE and p53 expressions were detected in the CD34+ cells of patients with acute leukemia during and after induction chemotherapy. 17 ACE-expressing macrophages in lymph nodes of patients with Hodgkin’s disease have been detected. 15 Enhanced ACE activity was also linked to multiple myeloma.32,33 ACE hyperfunction results in faster hydrolysis of the AcSDKP peptide, which in turn decreased in BM tissues, allowing hematopoietic stem cells (HSCs) to enter the S stage of the cell cycle.9,34 Ang 1-7 can be formed directly from the major RAS peptide Ang-II by the actions of the enzyme ACE2 and also from the Ang-I peptide. Mas receptors present in the BM microenvironment mediate the proliferative effect of Ang 1-7 on HSCs. 35
Deficiency of ACE2 in BM-derived cells increased mRNA abundance of a macrophage marker (F4/80) and tumor necrosis factor-alpha (TNF-α) in the stromal vascular fraction of retroperitoneal adipose tissue, suggesting increased infiltration of macrophages into adipose tissue of chimeric mice lacking ACE2 in leukocytes. 36 In our study, ACE1 and ACE2 expressions were found to be significantly higher in the myeloid neoplastic disorders when compared to the lymphoid cancers. Our results confirm previous observations that ACE is an important molecule in the pathobiology of leukemias.3,4 ACE inhibitors have inhibitory actions against leukemic cells via induction of apoptosis in vitro. A Spanish group 37 investigated the effect of captopril, trandolapril and losartan on the K562 leukemic cell line and K562 transfected with c-myc, bcl-x and bcl-2 (KmycB, Kbclx and Kbcl2, respectively). ACE1 and losartan inhibited cell growth, decreased c-myc expression and increased apoptosis in leukemic cells. The pro-apoptotic effects of the RAS blockers were associated with the Ang-II induced Smad activation. 37 Therefore, the place and function of ACE in hematological neoplasia are not just an academic issue but deserve to be investigated for the management of tumors in future trials.
Human umbilical cord blood cells express RENIN, ANGTS and ACE mRNAs. 38 Savary and colleagues detected the expression of ACE, RENIN, ANGTS and the chicken Ang-II receptor at a stage when blood circulation is not yet established and systemic regulation of blood pressure by the RAS is therefore not yet required. It therefore seems likely that the RAS is locally functional. The location of ACE in the extraembryonic endoderm, in contact with the first blood islands differentiating in the posterior extraembryonic mesoderm, puts ACE in a strategic position for primitive erythropoiesis. In vivo inhibition of the enzyme by a specific ACE inhibitor or application of a specific antagonist of the chicken Ang-II receptor resulted in a significant decrease in both the hematocrit and the mitotic index of erythroid cells. 39
ANGTS, ACE and RENIN mRNA expressions are increased in polycythemia rubra vera. 40 Leukocytes also expressed the ANGTS gene, synthesizing and releasing angiotensinogen with the capability to generate angiotensin. 41 CML patients had increased ACE, ANGTS and RENIN mRNA levels, and these expression levels decreased following administration of imatinib. Expressions of RAS components were studied in patients with CML at the time of diagnosis and at three, six and 12 months after diagnosis by qRT-PCR. De novo CML patients had increased ACE, ANGTS and RENIN mRNA expression levels, and these levels decreased following administration of imatinib. The RAS activities were significantly different among Sokal risk groups of CML, highlighting the altered biological activity of RAS in neoplastic disorders. Therefore the hematopoietic RAS affects neoplastic cell production, which may be altered via administration of tyrosine kinase inhibitors such as imatinib mesylate. 16 In our study, ANGTS gene expression levels were similar in myeloid as well as lymphoid patients with or without active disease. Paracrine and autocrine activities of the renin and ACE seem to be superior to angiotensinogen in the pathobiology of hematological neoplastic disorders.
The contributions of the RAS components to primitive and neoplastic hematopoiesis are evident.3,4 AT type 1a (AT1a) receptors are present on human CD34+CD38– cells, CD34+CD38+ cells, lymphocytes and stromal cells. Ang-II, the main effector peptide of RAS, increased hematopoietic progenitor cell proliferation by acting on AT1a receptors present on the CD34+ HSCs. 42 Ang-II was found to be acting as an autocrine growth factor for AML. 43 BM AT1 expression levels of the myeloma patients disclosed positive correlation with their BM infiltration pattern and tumor load indicated by serum beta 2 microglobulin levels. 33 The pharmacologically developed drug Ang-1-7 is already in phase I/II clinical trials for the modulation of BM RAS in distinct disease states.44,45 However, since most of the cellular effects of the local RAS are in an autocrine, paracrine and intracrine fashion, future drugs intended to modulate local RAS functions shall be prepared to have local targeted actions in the tissue microenvironment, such as inside BM.
Conclusions
The results of our present study indicate that the activities of local RAS may differ in distinct disease states such as leukemia and lymphomas. These data further support the original hypothesis that there is a local RAS in the BM affecting physiological and pathological hematopoiesis.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.