
Abstract
This article explores the similarities and differences between oral history and participatory action research (PAR) as two qualitative research methods that both accord with an interpretivist paradigm. It examines how combining these two methodologies can benefit mental health research, offering opportunities for reflection and reciprocity. Drawing from the authors’ respective knowledge and experience of using oral history and PAR methods within social care and mental health settings in the UK, the article considers these opportunities in relation to key concepts, namely, the sharing of power, reciprocity and positionality that are inherent in both methodological approaches. The article concludes that PAR-led oral history offers a trans-disciplinary methodology that can offer fresh insights for improving practices and social outcomes and for reducing inequalities.
Keywords
Introduction
This article discusses combining oral history and participatory action research (PAR) as interpretivist research methods with the intention of making visible the experiences of those who received and delivered care in the now-closed psychiatric asylums in one district of England. 1 We advocate that combining the two methods allowed for the production of alternative knowledge that challenged the hitherto dominant narrative of psychiatric care in the asylums in the latter part of the 20th century as total institutions (Goffman, 1961), predominantly perceived to be based on discipline and punishment (Foucault, 1975).
The project began in 2015 as doctoral research that combined the two methodologies from the outset (Calabria, 2020). Calabria, who conducted the research, is an experienced oral historian; 2 while Bailey as the supervisor and initial proponent of the project had a long-standing track record of conducting PAR in mental health settings (Bailey and Kerlin, 2015; Ward et al., 2012).
Oral history was identified as an essential method of data collection as the interview process practiced by oral historians affords participants an opportunity to address the historical record (Thompson, 2017). The purpose of the research was to capture and preserve for posterity the historical, lived experiences of ex-patients and staff in the asylums in the latter part of the 20th century, understood through the value of relationships and the influence of place in the form of the institutional environment. Patient and staff perspectives on institutional care practices remain marginalised in the history of psychiatry (Porter, 1985). The central motif in published stories about institutional life foregrounds punishment and resistance (Rolph and Walmsley, 2006). A review of the sparse published and unpublished oral histories of asylum life in the UK in the second half of the 20th century revealed often contradictory meanings of care provided therein; asylums could operate as total institutions as well as permeable environments (Calabria, 2016).
Oral histories were intended to capture the mutual relationships between patients and the relationships between patients and staff which were of interest to Bailey. Calabria has had a long-standing commitment to social justice helping to amplify seldom-heard voices and has fostered memory work in communities whose stories have not yet become part of the mainstream historical record. Drawing on this experience, she intended that the oral histories would capture participants’ lived experiences of the spatial aspects of asylum life and its surroundings as contributing to the relationships that developed therein (Calabria, 2020; Calabria et al., 2021).
The decision to combine oral history and PAR from the outset contrasts with previous research, where the approach of bringing the two methods together has evolved during the course of the study (Kong, 2017). This research highlighted the relatively different positions of power and influence commonly encountered by the participant population and the potential for marginalisation and ‘othering’ in the collection of oral histories of groups that remain hidden in the public discourse. The aim of this article is to explore in detail the methodological considerations of the research in relation to three key themes: (1) power and shared authority, (2) reciprocity in research relationships and (3) the positionality of the researcher and the researched. These themes are considered in terms of the relative merits of combining oral history and PAR as natural allies in highlighting the contested narratives relating to care in the now-closed psychiatric asylums.
Participatory action research with oral history
PAR was used as the overarching research design so that the different positions of the respective knowledge holders in the study could be reflected upon, as advocated by (Kemp et al., (2019). The term ‘patients’ has been used throughout this article in order to take into account the dominance of the medical model in mental health care (Ramon, 2018) at the time when participants were receiving care in the psychiatric asylums. The recovery movement in the UK refers to care delivered in these hospitals as a ‘doing to’ rather than ‘working with’ approach (Slade et al., 2017: 29). 3
Combining oral history with PAR influenced how the oral histories were solicited, collected and analysed. The research put on record the lived experiences of care practices, through the relationships and the meanings attached to the experiences of internal and external asylum spaces. The research called for guarding against replicating the power relationships between the researcher as a privileged knowledge holder and the researched as a relatively disempowered group in this regard. The unequal power relationships in research carried out with vulnerable groups mirrors previous research on what typified the relationships between clinicians and patients in the old asylums (Chow and Priebe, 2013; Quirk et al., 2006).
Authors were cognisant of Evans and Kotchetkova’s (2009) critique of PAR’s limited contribution to scientific knowledge on account of researchers being overly preoccupied with the practical tasks associated with empowerment and change. The inclusion of oral history as a recognised method of qualitative data collection in the humanities and history in particular, allowed for a better balance to be struck between the practical and the theoretical. The importance of this balancing act is underlined by Åkerström and Brunnberg (2013) and Svensson et al. (2007). Including oral history allowed Calabria to balance the involvement of the knowledge holders and theorise about how aspects of meaningful care practices in the old asylums could be understood in the context of conflicting narratives. Importantly, it enabled consideration for how a more nuanced discourse about the positives of these historical care practices could be applied to influence contemporary care models that are a current focus for legislative change in England and Wales, UK (Wesley, 2018).
The combined use of PAR with qualitative methods such as narrative inquiry is well-established as both methods share epistemological and ontological commitments towards social change (Kurtz, 2014; Pushor and Clandinin, 2009). Examples in the context of UK mental health research include Hutchinson and Lovell (2013) and Torrissen and Stickley (2018).
However, literature that deals with the overlap between PAR and oral history remains scarce (Starecheski and Freund, 2013). PAR and oral history both hail from the interpretivist research paradigm. These methodologies are concerned with the social construction of knowledge and are grounded in the lived experiences of individuals (Denzin and Lincoln, 2011). Both methods rely on research participants giving consent for their participation and sharing their lived experiences. Both methods put emphasis on the researcher developing trusting relationships with stakeholders (Hesse-Biber and Leavy, 2010). These were important considerations to heed, given the vulnerabilities of the chosen population for this study, which included people who had experienced the psychiatric system.
A key difference between the two methods rests on how participation is conceptualised. Oral history is particularly suited to studying the experiences of marginalised groups and to put on record how given populations experience historical events through the process of the oral history interview (Thompson, 2017) – an example of what Schön would deem ‘reflection on action’ (1991: 50). PAR includes action as one of the stages in a cyclical process with planning and critical reflection (Kemmis, 2001). As a methodological process, PAR seeks to foster social justice through the ways in which the researcher engages with those who hold a stake in the research area in question. PAR therefore provides the opportunity to go beyond the past to include Schön’s ‘reflection in’, ‘reflection on’ and ‘reflection for action’ (1991: 50–51). Because the intention was to involve participants in the research process, (reflecting in action), record their lived experiences (reflecting on care practices through time) and re-evaluate these experiences in the psychiatric asylums in the context of modern day mental health services (reflecting for action), combining PAR and oral history offered a new opportunity for deeper reflective insights.
Both methods adhere to standard ethical codes of research involving people by ensuring confidentiality and anonymity to participants. However, what characterises oral history is the duty of confidentiality until interviewees have given permission for the use of the interview recording (Yow, 2014). Oral history entails the recording of people’s memories; in the UK interviewees own the copyright to their own spoken words, which cannot be used by third parties without their express permission. 4 Copyright release must be obtained for researchers to gain the right to access and use. Moreover, oral historians make a concerted effort to reveal the identity of their interviewees in publication and public display when the interviewees expressly ask to be identified (Thompson, 2017). Identifying individuals is often central to the project of oral history research, which seeks to contribute to historical understanding and validate respondents’ lives (Le Roux, 2015).
The validity of the knowledge produced in PAR mainly rests on the level of authenticity achieved in research relationships (Lincoln, 2001), whereas oral history demands a critical engagement with the nature of storytelling, which is viewed as rhetorical constructs rather than transparent windows onto past worlds. Since the cultural turn, oral historians have been acutely aware of the peculiarities of oral history, bound up with the nature of memory (Portelli, 2015). For instance, omissions and conflations can reveal not only the effects of oppression and control but can also be expressions of agency that can transpire through the multiple negotiations between the narrator and the researcher, before, during and after the interview (Freund, 2013). Whereas PAR, through the process of action and critical reflection, seeks to engage in sense making with the participants as an iterative process, the academic authority of oral historians becomes pivotal in making sense of the things that are occluded in the storytelling process (Abrams, 2016).
By bringing both methods together, the study was able to foster participation as a form of empowerment for ex-patients and staff through the process of remembering and reinterpreting the past (Thompson, 2017). Involving former patients and staff from the closed psychiatric asylums in the study also mirrored the emphasis on public and patient involvement in the UK’s National Health Service policy and planning agenda. This policy states that those who use services should be able to voice their experiences of receiving care and should be able to actively influence them for the better (Barham, 2011). One of the key priorities in the UK’s National Health Service Plan (Alderwick and Dixon, 2019) is the need to create genuine partnerships between professionals and patients, and their significant others. Understanding the legacy of how care practices have shifted through time in the context of mental health provision was considered central to this policy change agenda.
Shared power and shared authority
What defines oral history is the intrinsic process of collaborative dialogue between the interviewer and the narrator in which authority is shared through the dynamic, evolving exchange of questions and responses in the development of the oral history interview (Frisch, 1990). Frisch urged historians to share authority with their informants beyond the interview encounter by embracing collaboration in the interpretation and presentation as a means of democratising historical research (Thomson, 2003: 23). Moving from shared to sharing authority has been largely understood as a vehicle for combining research with advocacy by going beyond the interview encounter as a platform for movement building through divulging skills and knowledge to the disenfranchised in order to create more representative histories, from below (High, 2009; Shopes, 2003).
While PAR does not use the term sharing authority per se, PAR recognises that individuals, groups and stakeholders as communities hold distinctive knowledge and/or experience about the research issue in question (Kemp et al., 2019). PAR is conducted iteratively through cycles of planning, action and reflection to ensure that activism is balanced with shared thinking about issues and implications (Koch and Kralik, 2006). It allows for the involvement of participants, ideally in every stage of the research cycle (Kemmis et al., 2014: 1–31). This intended inclusivity therefore distinguishes it from other epistemological approaches ‘that seek to either generate knowledge or effect causal change through experimental means’ (Ward et al., 2012: 151).
Through participation, action and critical reflection, human agency is recovered to promote an action-oriented understanding of key issues that need to be addressed. Combining PAR and oral history reinforces the sharing of power and authority throughout the research process in the way that data is collected and analysed, informed by a process of knowledge co-construction (Figure 1). The Action research cycle (Kemmis and McTaggart, 1982).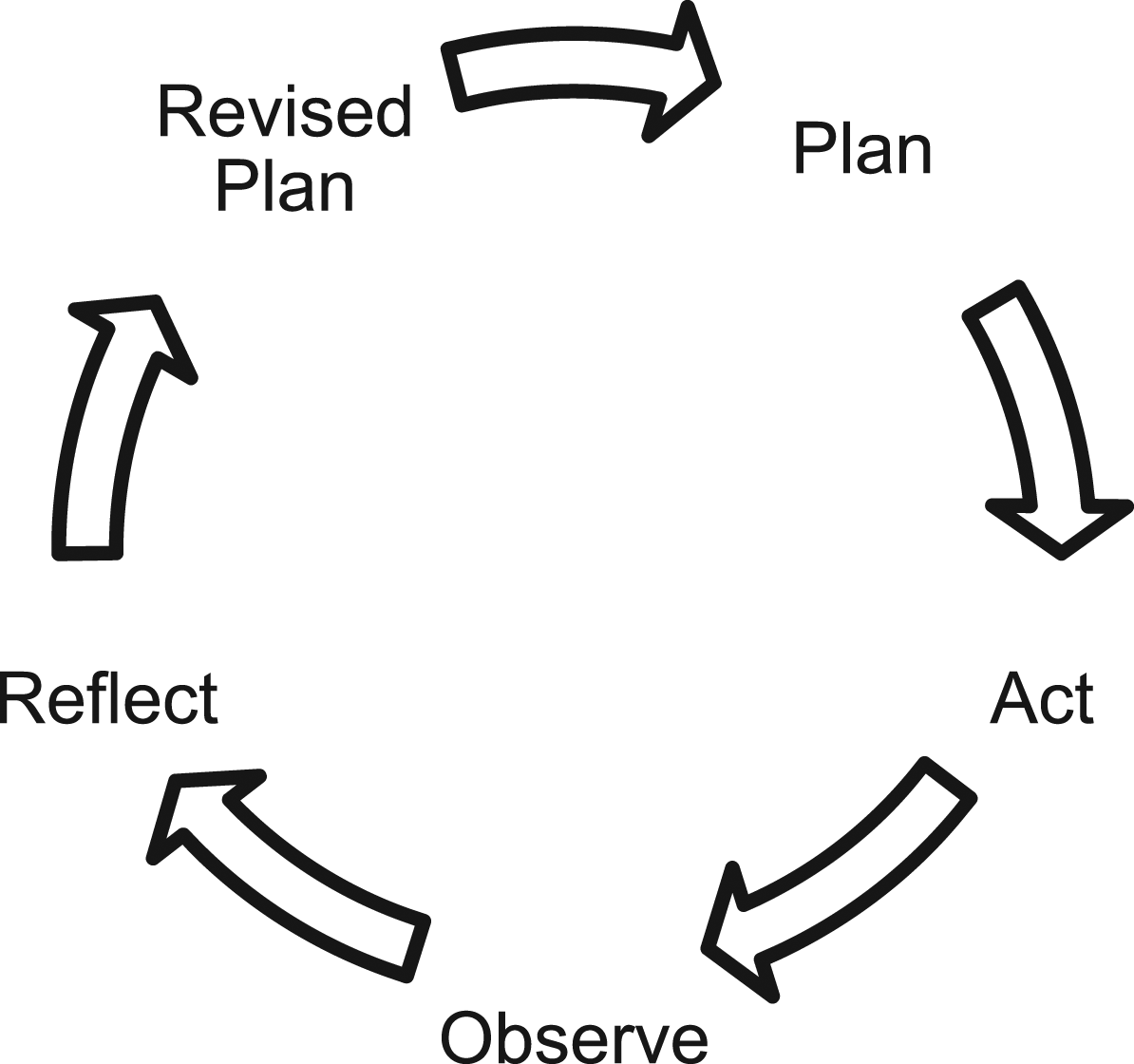
Twenty people with first-hand experience of the asylums were interviewed multiple times. These included six former patients and 14 retired medical and non-medical staff who gave and received care at the Nottingham asylums between 1948 and 1994. 5 Some of the ex-patients’ family members and carers took part in group discussions to aid planning of the project and reflection on findings as they emerged. Participants were recruited through promotional activities in print and online, and via community talks aimed at service user-led groups, adopting a snowballing approach. A partnership was set up with a local day centre, 6 which was pivotal in gaining access to ex-patients.
Phases of participation combining PAR and oral history.
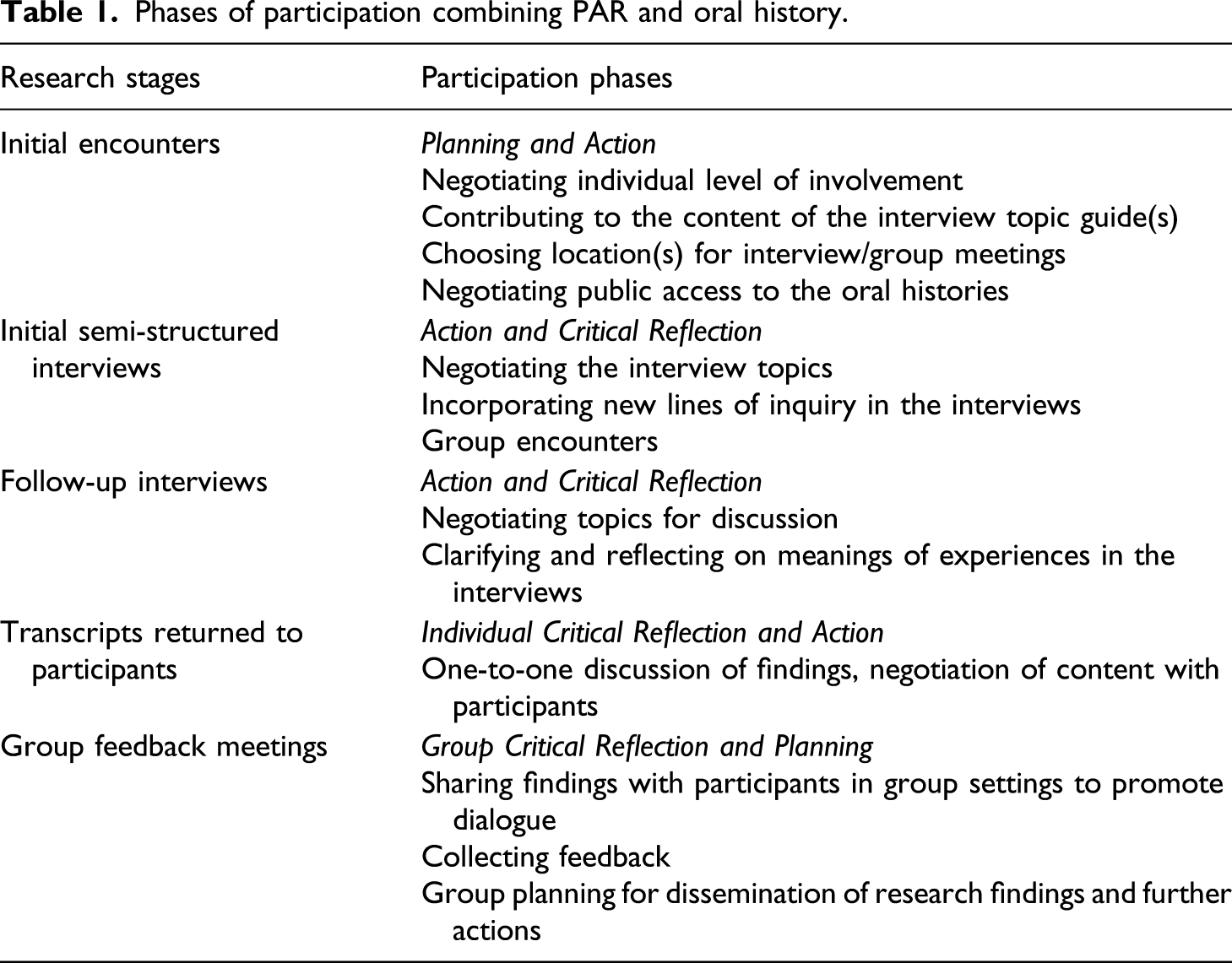
The initial encounters with participants took place over a 6-month period to gauge potential interest in the study. Participants had opportunities to ask questions about the research and about the researcher and to raise any concerns. These ‘off-tape’ encounters were crucial for encouraging participants to shape the content and rhythm of the interviews. Calabria was able to negotiate with individuals wanted to talk about and explore their motivations for taking part. Individuals’ perspectives were gathered on key themes and topics that formed their experiences in the hospital. For instance, some ex-patients wanted to include their experiences of interacting with the local community adjacent to the hospital during their hospitalisation.
Once the planning of the study had taken place, power sharing continued to be promoted. Participants were encouraged to offer new lines of inquiry during the oral history interviews; this shaped the topic guide in an iterative way. The shared endeavour produced rich and reflective interviews that reveal the multiplicity of individual and collective meanings attached to care practices in the hospital, and the ramifications of these experiences for modern day mental health care provision. The in-depth interviews encouraged the participants to speak in terms that were relevant to them, thus providing a way of balancing the researcher’s power in relation to how the interview agenda was set. This was achieved by asking open-ended and reflective questions, while probing on the main themes of the research. Participants were encouraged to continuously reflect on the meanings of their experiences, a key technique in oral history interviewing (Yow, 2014). Sharing authority in this way encourages research participants to articulate their perspectives and to collaboratively generate knowledge between the researcher and the research participants (Thomson, 2003: 49–70; Hesse-Biber and Leavy, 2010: 163–192).
As part of the PAR cycle of action and reflection, transcripts were shared with the participants from the outset, a common process to encourage collaboration in the interpretation of oral histories (Rickard, 2003). The process enabled both Calabria and the participants to ask questions and seek clarification, to sound out her initial interpretations and establish the need for further interviews. At this stage of the research, Calabria gathered stakeholders’ opinions and concerns and any omissions/additions to the transcript. Although all agreed to take part in group discussions, one of the main obstacles to active collaboration rested on participants wanting to work individually with Calabria. This required numerous encounters with them beyond what had been originally anticipated.
Participants were offered the option to remain anonymous in the transcript and in the publication of any information relating to their testimonies unless they specifically agreed to share their personal details. Only two out of the 20 people requested anonymity; all agreed to have their oral history transcripts deposited in a local public archive. However, efforts to share authority posed risks for Calabria and the participants when making shared decisions about whether the interviews should be open or closed. Two participants, who opted not to remain anonymous, openly shared the mental health diagnosis of their children throughout their interviews. Oral history interviews that contain health related data about a third party without their consent are in breach of new data protection regulations. 7 To this end, the interviews were embargoed.
During the research project, examples of power/authority sharing included ex-patients suggesting actions to bring about practical change. These included the production of an exhibition to showcase the intangible heritage of the local psychiatric asylums. Although Calabria’s drive to create a public archive of the legacy of the asylums matched that of the participants, her priority as a PhD student wanting to publish the findings for policy impact were not necessarily shared by participants who saw practical change happening through public engagement. However, after the research was concluded, Calabria secured funding for the co-production of an exhibition, thus developing socially engaged outputs that are relevant and meaningful to the communities under research. 8 Projects that combine oral history work with participatory methodologies should take into account the need for multiple outputs to suit all stakeholders (Sheftel and Zembrzycki, 2013). Importantly, PAR-driven qualitative projects tend to have no end date; in this respect, researchers have a moral imperative to be involved in the longer term to help develop community-driven outputs (Lemley, 2017). This awareness makes it necessary to manage participants’ expectations in the context of what can be achieved within projects that lack adequate resources and involve people who rely on social care and health services and often experience user-involvement as tokenistic (Pollard and Evans, 2013; Ward et al., 2009).
Oral historians have warned against uncritically embracing forms of storytelling (Freund, 2019). The specificity of oral history demanded a critical engagement with the nature of memory and subjectivity (Portelli, 2015). Calabria identified instances of silences and misremembering across the oral histories, including an overwhelming sense of nostalgia for the old asylums. As part of her commitment to scholarship, Calabria retained her scholarly authority by examining the reasons for portraying an overly optimistic view of the care provided in the old system in the context of the destruction of the asylums as sites of memory and the current fragmentation of mental health services. She concluded that nostalgia for the old system of care not only served to legitimise a particular version of the past largely denied to residents and staff alike; nostalgia was marshalled as an appeal for a better future (Calabria, n.d.).
Reciprocity in research relationships
Both PAR and oral history emphasise the importance of developing mutual and reciprocal relationships in an attempt to balance the unequal power inherent in research relationships and to enable democratic action and greater social equality (Hesse-Biber and Leavy 2010; Lemley, 2017; Starecheski and Freund 2013). This is achieved by building trust, a central aspect of both PAR and the oral history interview (Kemmis et al., 2014; Yow, 2014). Engendering power sharing and building trust was particularly important for this study because of the unequal power relationships that ex-patients would have encountered in the psychiatric asylums. The research was designed to redress these power imbalances and avoid replicating them in the way the research was conducted.
Calabria set out to build trust by attending social events at a local community centre, which most of the former patients relied on for their social contact and support. The structural inequalities commonly faced by ex-patients with mental health needs, such as poverty and isolation (Perkins and Slade, 2012), led her to offer practical support. For example, she offered lifts to and from meetings to participants who live in geographically isolated areas, bought food and drinks when meeting in public settings, and travelled to participants’ homes if they were reluctant to travel. Over time, these acts of reciprocity reportedly helped participants to feel they could speak frankly and openly about their experiences of receiving care. This kind of closeness and reciprocity in relationships with people who use mental health services is highlighted by Ramon and Williams as being qualitatively distinct in mental health and important for successful engagement (2005: 15).
Reciprocity in the research relationships was also fostered through the creation of ‘safe spaces’ where the research exchanges before, during and after the oral history interviews could take place to enable the building of rapport and common ground and allow for differences of opinions and conflicts to emerge (Bergold and Thomas, 2012). Creating safe spaces for different individuals who might have conflicting views with each other is especially important when engaging with persons with experience of the psychiatric system, whose narratives have traditionally been excluded in research about them (Cook, 2012) or presented as uncontested. During the interviews and off-tape encounters, Calabria facilitated the process of shared decision-making by subjugating her own agenda to active listening, a well-established technique in oral history methodology (Anderson and Jack, 1991). She was acutely aware that people with mental health problems are seldom listened to and that their stories tend to be disregarded as lacking coherence. This served to balance the inherent unequal power she held as researcher and allowed participants to steer the focus of the iterative phases of the research towards what mattered most to them and critically reflect upon the issues that they deemed important in their care. Follow-up interviews, requested by participants, became a means of engendering active involvement and genuine collaboration by sharing control over decision-making (Baum et al., 2006). As a consequence of the follow-up interviews, the planning was revised to take into account the needs of participants and those of the researcher (Kemmis et al., 2014). Conflicting narratives emerged frequently during the course of the research between participant groups, but also within participants’ individual accounts; for instance, most of the staff maintained that the administration of electro-convulsive therapy (ECT) as a form of treatment helped the patients’ recovery. However, patients’ views on receiving ECT were markedly different, fearing the treatment for its long-term adverse effects. In addition, some of the former patients recalled instances of psychological abuse, while also remembering positive relationships with staff, including helpful aspects of the care provided in the psychiatric asylums that aided their recovery.
Ex-patients requested separate group feedback events from those with retired staff, as they felt more comfortable speaking in the presence of other ex-patients. During these reflective meetings, however, the broad themes that emerged from the analysis of all participants’ interviews were shared. This promoted reflection on the ‘othering’ process as part of PAR from the relatively safe space of a group who shared experiences. Drawing on Habermas’ social theory of communicative action (Kemmis, 2001), these meetings served as key ‘communicative spaces’ that encouraged open sharing of testimonies with others, strong peer identification and a sense of solidarity among the relevant patient and staff groups that took part in this study. As a result, actions for change advocated by the respective groups were different and also similar, focusing on the importance of therapeutic relationships and access to internal and external therapeutic spaces for recovery. This evidenced the extent to which stakeholders were able to steer the research agenda to include topics that were relevant to them. However, there were limitations to the way in which power could be shared. Some participants resisted becoming involved in group data analysis and reflection sessions, instead viewing their individual testimonies as valid on their own terms and seeing no value in taking part in interpreting the overall findings. Their responses raise the question of whether it is always possible or even desirable to involve research participants in the collective interpretation process, as their vested interests in taking part may be at odds with the overall research agenda (Shopes, 2003: 109).
The data collected in the group events were qualitatively different from the one-to-one oral history interviews in that individual actors expressed their own opinion and hopes for dissemination in a much more assertive way. For instance, an ex-patient felt that ‘this is the start of some real change, we’ve been listened to, during closure only those who had the loudest voice were heard, those concerned were ignored’. Retired staff offered to share the findings with local commissioners of mental health services. Many stakeholders recognised each other from past grassroots campaigns to save services and shared their experiences of tokenism in previous consultations during the transition from asylum to community care. All wanted to know what happened to the funds raised from the real estate from the sale of the old Victorian hospital buildings, which were not ring-fenced.
Even though this was a collaborative research project initiated by an academic researcher and not by mental health activists/researchers, the group meetings still encouraged ownership and collective action for both ex-patients and staff, some of whom were carers. Within the group settings, participants formulated a collective plan for dissemination of the findings through talks aimed at key decision makers in the community and the public at large to make visible the legacy of care provided in the now-closed psychiatric asylums. Many felt a deep sense of loss caused by the removal of the signs of the asylums’ history by real estate developers and wanted to preserve and share the hospitals’ social history. In this respect, participants’ reciprocal relationships with each other demonstrated overtures of what Russo (2012: 4) refers to as survivor-controlled research, which by its very nature sets off a collective process that instigates ownership of the research. This embodies the purpose of PAR to balance knowledge-by-expertise with knowledge-by-experience – producing research outcomes that are relevant to the communities being researched (Baum et al., 2006). In this way, PAR afforded participants the opportunity to influence the research and ultimately to instigate practical change. These reciprocal relationships of influence reflect both a growing trend in health and social care in the UK and the importance of involving those who use mental health services by enabling them to bring their lived experiences to bear on the professional practice of people who deliver services (Ward et al., 2013).
Although Calabria controlled the project in the initial phase of the research, the research agenda shifted from an initial interest in relationships and the therapeutic environment towards what mattered most to participants as the iterative phases of PAR got under way. Participants brought a significant focus on their individual experiences of not only the old system of care in the psychiatric asylums but also their opinions on aspects of contemporary care, which they found wanting. Proponents of PAR consider it an approach that moves us away from research that is ‘done to’ to research that is ‘done with’ and on behalf of disempowered groups as a means to redress this power imbalance (Kemmis et al., 2014). It emerged from the research that participants were focused both on community care as delivered by contemporary mental health services and the need for this to change in order to redress the balance of therapeutic relationships; this focus is now being used in education. 9 By concentrating on the priorities of the participants rather than the agenda of the researcher, reciprocity fostered good working relationships in the research encounter.
Positionality – insider-outsider
Positionality was fundamental to how the research was conducted from the outset, as the participants, whether retired staff or ex-patients, had all experienced being insiders of the psychiatric asylums. Both authors were outsiders, not having experienced the mental health system first-hand; yet this was not as clear cut as first imagined. Bailey’s advocation of PAR as the overarching design for the study stemmed from her previous experience as a mental health social worker who had supported patients during their transition to community-based care in line with the asylum closure programme. her position as a practitioner-researcher influenced her attempts to focus the research on the relational aspects of asylum care and the way the study was conducted (Bailey, 1997; Smith and Bailey, 2010).
Calabria’s positionality shifted during the course of the study. Initially she considered herself an outsider with no personal experience of having used or worked in mental health services. However, as the opportunity for critical reflection arose through one-to-one debriefs with participants, she experienced a conceptual shift in her own positionality. Her position changed once she reflected on the experiences shared by mental health service users, punctuated by grief and loss, which brought back suppressed memories of her own first-hand experience of her mother’s mental illness. She no longer saw herself as an outsider by virtue of her knowledge by experience, thus reducing the distance between the participants and herself. Engaging with the notion of liminality in sensitive research (Janzen, 2016), Calabria came to realise that she occupied a third position in the research by having the privilege of entering and leaving her new-found position at her own choosing, a choice not afforded to the participants. The dialogue that developed between Calabria and the research participants through prolonged interactions was instrumental in fostering new understandings and readjusted her views on the care her mother received with respect to the value of the relationships her mother formed and fostered with staff in her own recovery (Calabria, 2019). Reflexivity on the part of researchers regarding their own positionality thus became integral to how this research was conducted, supporting reflection in, and for action (Schön, 1991). Reflexivity in research relationships is one of the fundamental components of PAR methodology (Kemmis and McTaggart, 2005). A key aspect of the practice of PAR-led research is an examination of the different ways researchers and participants interpret the findings (Baum et al., 2006). As members of the stakeholder community engaged in what became recognised as PAR-led oral history, Calabria prepared for changes to her own views and experiences of the research as a consequence of the participation and influence of those who had given and received care within the psychiatric asylums. The contested realities that emerged during the course of the study, which reflected the importance of relational care in mental health, elicited change in her own reflections about the value of the professional care her own mother received. Calabria started volunteering for a local carers group, recognising her need to better understand the challenges she faced as a carer and wanting to effect change among the local community of stakeholders. Such change is viewed as a necessary outcome of PAR on both personal and collective levels; the emphasis rests on mutual learning in what Ponzoni refers to as ‘windows of understanding’ (2016: 566). In this context, the boundaries dissolve between the ‘knowledge producing’ and the ‘knowledge consuming’ elites and the community under study. This outcome has the potential of producing practical change for all involved by encouraging capacity and knowledge development (Lincoln, 2001: 127).
The iterative process of storytelling, reviewing, interpreting and disseminating the knowledge produced generated new understandings for all. Ex-patients who still use the mental health system considered this project to be the start of some real change in terms of rediscovering aspects of care that had been meaningful to them in the old asylums. They reported increased self-confidence through the process of reflection during interviews, frequent interactions and discussions of the research findings. A service user felt that ‘I never knew I could speak so coherently about what it was like before [the hospitals closed], I feel much more confident to speak in public’. He used his interview transcript to give talks about his journey through the mental health system. A group led by ex-patients was set up to research the history of their local mental health day centre; the group delivered public talks based on their interviews to increase awareness of the importance of having access to a welcoming environment during crisis. An important outcome of this study has been the preservation of participants’ memories through the creation of a publicly accessible oral history collection. 10 Overall, participants were positively affected by participation, and the burgeoning activities in the community demonstrate how participants effected change at the local level by initiating communities of dialogue about meaningful care practices, little of which is known in the public discourse. The positive impact of participation reflects other research that actively involved stakeholders to reduce health inequalities, which reported a range of positive benefits, including improved social networks and wellbeing (Bailey and Kerlin, 2015; Ward et al., 2012).
Discussion and conclusion
This article has examined how combining oral history with PAR uncovered the multiple ways in which ex-patients and staff experienced the closure of the psychiatric asylums and the complex meanings of care practices therein. It has highlighted how reciprocity in the research relationships afforded an opportunity to re-examine theory and method. The iterative process of PAR allowed turn taking between the respective positions of conducting the research as well as reflecting on doing it. Through a PAR-led oral history approach, ex-patients and former staff challenged the dominant overall perception of the psychiatric asylums as undesirable and outmoded institutions. They provided alternative interpretations of aspects of care they found meaningful for their care and also criticised some aspects of care as unhelpful and depersonalising. In addition, reciprocity in PAR-led oral history entails being accountable to the community or groups who are the subjects of the research. This requires a shift in academic priorities to fit with community agendas, which must guide participation and frame the research. Essentially, PAR-led research calls for a re-positioning of the researcher and the subject of research by creating social spaces and dynamics of reciprocity that give participants the power to make meaningful contributions. The multiple encounters with participants throughout the study helped to actively share the decision-making process to forge meanings through critical discussion at every stage of the research. Participants actively shaped the research design process, determining areas of inquiry and expressing their views on future outcomes. Ultimately, the stakeholders in this project developed a sense of ownership of the research outputs by steering the development of the research into meaningful actions proposed by them.
On reflection, this research illustrates an example of PAR-led oral history with mental health service users, whose voices have traditionally been ignored in mental health policy, making valuable theoretical and practical contributions. Using oral history as a method of data collection helped to redress imbalances in the historiography of psychiatry, where certain narratives have been held up as legitimate and authoritative at the expense of others (Davies, 2001). PAR, through its cyclical process of action and reflection, allowed the ‘reflecting on’ participants' lived experience to shift to ‘reflecting for’ change in the future, both in respect of their individual experiences and their influence on type of community mental health services which many continued to access.
Such critical reflection was a constant feature of the dialogue between the authors during the research, with Calabria reflecting on her experience of becoming an independent researcher experienced in both research methods as the study concluded. To sum up, PAR can benefit from the focus oral historians put on the intersubjectivities at play, such as the interplay between the public and the private, and between the past and the present if new knowledge that informs change is to be truly co-constructed. Conversely, oral historians can benefit from taking a PAR-led, oral history approach in redressing collective issues experienced by disenfranchised groups and bringing about change that is meaningful for the communities with whom the research is conducted.
Based on the authors’ shared experiences, we conclude that oral history and PAR are natural allies and that researchers engaging in PAR-led oral history should do so by design and not by accident. Including the iterative PAR cycles of planning, observation and reflection in the way that oral histories are solicited, collected and analysed can significantly balance the differing power dynamics in the research encounter and afford practical outcomes for all. By analysing the positionalities of the researcher and the researched, this article has shown that PAR-led oral history offers genuine participation through mutual and multiple levels of reflexivity in the process of scrutinising the connections between the researcher and both the object of the research and the intersubjective dynamics at play.
As evidenced in this article, combining these methodologies captured rich data that reflected participants’ contested realities of care in the now-closed psychiatric institutions that hitherto have been missing from the record. This allowed for a process of reflection on, in and for action so that participants moved beyond a traditional approach to shared authority (Shopes, 2003), to collective insights that challenged dominant historical accounts of asylums as total institutions. The deliberate combination of methods makes a unique contribution to the methodological literature concerning PAR and oral history. These two distinct but complementary methodologies when combined are particularly suitable for engaging and giving a voice to marginalised communities and for producing knowledge-by-experience that can help reduce social inequalities. Combining PAR with oral history has the potential to increase democratic practices of research by keeping people and politics at the heart of the research cycle, while also requiring a balance between the researcher’s commitment to scholarly work and advocacy in order to promote change.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.