
Abstract
This article tests the assumptions of the literature regarding the neoliberal agenda (‘Washington Consensus’) promoted by international organisations through knowledge transfer and about the power they supposedly have through loan conditionality to impose their will on countries in financial need. In addition, it examines ‘avant-garde measures’ of neoliberal reforms exceeding the requirements from international organisations. Looking at the social policy concepts and advice these organisations give countries in the former Soviet Union, it utilises the example of healthcare reform in Kazakhstan, Kyrgyzstan and Russia. The article examines the general advice these organisations gave between 1991 and 2018 for the reorganisation and management of the countries’ healthcare systems, especially concerning the introduction of a mandatory health insurance system.
Keywords
Introduction
The article analyses the policy-related knowledge transfer of international organisations (IOs), especially social policy concepts and advice these organisations give to countries in the former Soviet Union (FSU). The transfer of knowledge is based on the concept of ‘policy transfer’ which describes ‘the process by which knowledge about policies, administrative arrangements, institutions and ideas in one political system (past or present) is used in the development of policies, administrative arrangements, institutions and ideas in another political system’ (Dolowitz and Marsh, 2000: 5). Stone (2012) distinguishes between policy transfer and knowledge transfer, which necessitates the institutionalisation of the transferred ideas, their implementation:
The ‘soft’ transfer of ideas and information via networks whether they be personal, professional or electronic is rapid and frequent. It is rather more infrequent to see such ideas structure governance and become institutionalised. Knowledge transfer is more extensive than policy transfer. (p. 483)
Law-making can be considered a first step on the way to an institutionalisation making such a transfer of knowledge observable.
The transfer of knowledge needs ‘knowledge actors’ as carriers, exporters and inducers of new policy ideas (cf., for example, Jacoby, 2008; Stone, 2000, 2017) IOs, understood as international governmental organisations, such as the International Monetary Fund (IMF), the World Bank (WB), the World Health Organization (WHO) and the organisations of the United Nations, have been identified as major actors in transnational policy-related knowledge transfer.
Academic research on knowledge transfer in the area of social policy has strongly focused on the ‘Washington Consensus’, a set of neoliberal policy prescriptions promoted primarily by international financial organisations (cf., for example, Appel and Orenstein, 2018; Babb, 2013; Babb and Carruthers, 2008; Ban and Gallagher, 2015; Béland and Orenstein, 2013; Brooks, 2015; Broome, 2015; Farnsworth and Irving, 2018; Li et al., 2015; Orenstein, 2008b, 2011; Sabatovych, 2016; Schlaufer, 2019; Schmitt and Obinger, 2013; Vadlamannati, 2019). Conditional loan agreements of the WB and IMF for financially struggling countries were often accompanied by structural adjustment programmes (SAP), which ‘have long been criticised as a coercive form of economic reform measures’ (Stone, 2012: 491; on the effect of IMF conditionality, see Daoud et al., 2017; Forster et al., 2019; Kentikelenis et al., 2015, 2016; Lee and Woo, 2020; Nelson, 2017; Rickard and Caraway, 2019; Stubbs et al., 2017).
However, beyond mere financial support many SAPs are accompanied by advisers, training programmes and so on, which also play an important role in the design of national social policies. Thus, IOs have increasingly become the focal points of a global exchange of ideas on social policies (cf., for example, Liu, 2015; Ozkan, 2013; Seekings, 2010). In the post-socialist context, for example, IOs have played a prominent role in directing and shaping social policy (cf., for example, An, 2014; Cerami, 2006; Deacon, 2000; Lehrer and Korhonen, 2004). Thereby, IOs ‘help transfer the intellectual matter that underpins policies. They can provide the rhetoric, the language and scholarly discourse to give substance and legitimacy to certain preferred positions’ (Stone, 2002a: 6).
Most of these studies perceive IOs as the drivers of neoliberal reform policies using loan conditionality as a means to force their ideas upon the receiving (mostly ‘unwilling’) countries. This strand of literature emphasises the power of loan conditionality and, therefore, the inevitability of knowledge transfer from powerful IOs to countries in need of (financial) assistance. However, this neglects the stages of perception, adaptation and translation (i.e. modification) of knowledge on the national/domestic level: ‘Policies are not merely transferred over space, but their formats and their effects are also transformed by their journey through professional communities, and through time’ (Stone, 2017: 66). Weyland (2006) does not consider the mere existence of a loan agreement with an IO as a ‘proof of external imposition’ (p. 14). Upon arrival at the national level, global influences often create structures for contestation, resistance and opposition; governments and other interest groups act through their own diverse strategies to determine the pace, course, timing and effects of these influences. Yeates (2002) argues that the outcomes of these struggles for social and economic welfare depend, crucially, on the context in which they are negotiated.
In a related argument, Appel and Orenstein (2018) describe the willing adaptation of the transferred knowledge and even exceedance of advice, the neoliberal ideas of the ‘Washington Consensus’, in Central and Eastern Europe. The ‘Washington Consensus’ prevailed in various forms and to varying degrees across the post-socialist world for nearly two decades independently of the political orientation of the respective governments. Using the examples of flat tax and pension privatisation, the authors assert that post-communist countries went even further with their neoliberal reforms than countries in Western Europe and North America were able and/or willing to (what they call the ‘avant-garde’ phase exceeding a first wave of neoliberal reforms). This enthusiasm for neoliberal reforms ended only in 2008 with the global financial crisis.
Believing that neoliberal economic reforms would generate growth and investment, many governments went beyond required policies and adopted ‘avant-garde measures’, such as pension privatisation and the introduction of a flat tax, which ‘were not required by the IMF, but rather opposed or treated ambivalently’ (Appel and Orenstein, 2018: 26). The dynamics of avant-garde reforms were different from those of earlier neoliberal reform phases. The competition among post-socialist countries for foreign investments
created opportunities for policy entrepreneurs to define and adopt those policies that best appealed to and captured the attention of foreign investors. International actors such as the World Bank and neoliberal think tanks became knowledge resources for innovative neoliberal thinking, rather than enforcers. (Appel and Orenstein, 2018: 92)
Most of the literature on knowledge transfer through IOs has painted a rather broad picture and based its results on a rather limited empirical basis. Inspired by Kuhlmann et al. (2020), the following article analyses the IOs’ agendas on a detailed empirical basis and over time, in order to identify and interpret the shifts and nuances in positions and recommendations. In particular, it tests the assumptions of the literature regarding the neoliberal agenda (‘Washington Consensus’) promoted by IOs through knowledge transfer and about the power they supposedly have through loan conditionality to impose their will on countries in financial need. In addition, it examines ‘avant-garde measures’ (Appel and Orenstein, 2018) of neoliberal reforms exceeding the requirements from IOs. Starting at the beginning of the knowledge transfer process (i.e. with the advice IOs hold in store), this article is primarily a (descriptive) text analysis using qualitative content analysis to test assumptions of the literature on a detailed empirical basis. Thus, it advances the understanding of IOs by subjecting prominent claims in the literature to empirical scrutiny. Therefore, it looks at only one policy field for which there should be a clear domestic demand for reform and policy advice, and which should also be complex enough to ensure that the transferred ideas structure the country’s governance and become institutionalised.
There was a clear demand for reform in the FSU as the inherited Soviet healthcare system, the so-called Semashko system, had been deeply discredited. Originally, it envisioned a comprehensive, qualified medical care available to everyone in the population free of charge and organised as a single, unified service provided by the state (George and Manning, 1980: 105–106). However, the health system had been chronically underfunded, resulting in, for instance, a general lack of pharmaceuticals and a poor quality of services. Consequently, health conditions had deteriorated, with stagnating life expectancy, high mortality rates, and large disparities in health status and outcomes among the 15 Soviet republics (Rowland and Telyukov, 1991: 71–72, 77; Williams, 2006: 217). Thus, in the mid 1980s, the Soviet leadership had begun to reform the Semashko system through the introduction of quasi-market elements (the so-called New Economic Mechanisms, NEM). These efforts had resulted in several regional pilot projects introducing a mandatory health insurance (MHI) scheme to improve the financial situation of the healthcare sector in the late 1980s (Twigg, 1998: 585–586).
The break-up of the Soviet Union in 1991, however, prevented the wider expansion of these pilot projects leaving the Semashko healthcare system mostly unreformed. Thus, this article utilises the example of healthcare reform, especially the introduction of an MHI system, which is considered as a way to put healthcare finance on a solid footing while simultaneously improving the healthcare sector’s efficiency and quality of service.
In order to evaluate the position of IOs towards the introduction of an MHI in the FSU over time, their documents have been analysed by looking at three aspects: (1) the financing of healthcare (out-of-pocket payment; private, for-profit insurance; social insurance; and/or tax funding); (2) the promotion of neoliberal reforms (‘Washington Consensus’); and (3) the IOs’ evaluation of the countries’ (degree of) collaboration, their behaviour towards reform advice. This article does not assume a constant knowledge transfer over the whole time period under study; rather, IOs put their ideas at public disposal to be requested by countries in need or applied to countries on the IOs’ own initiative. These ideas might evolve and/or change over time.
Literature review
There is a multiplicity and variety of actors involved in the field of healthcare reform with no clear division of labour, a certain degree of competition and various forms of collaboration (Kaasch, 2013: 52, 54). The literature has provided leads to which IOs are involved in the FSU (cf., for example, Deacon, 1998, 2003). However, the only IOs actively involved in complex, systemic healthcare reform in the FSU (which has been checked on their websites) are the IMF, the WB and the WHO. 1
The WHO introduced a new approach of primary healthcare (PHC) for the creation of minimum basic health services in the mid 1970s. The PHC approach includes the concept of universal coverage of health services, which aims at granting all people access to needed health services without the risk of severe financial consequences. While the PHC was considered a cost-effective strategy, it still demanded large resource commitments. This started a debate about comprehensive versus selective healthcare services and, consequently, about reforming healthcare financing (HCF), understood as ‘mobilisation and use of financial resources in the health sector’ (Lee and Goodman, 2002: 99, quote 98), and the introduction of user fees for healthcare services.
The WHO, as the most prominent supporter of universal health coverage, considers ‘finding ways to move away from out-of-pocket payments toward some form of prepayment’ essential because out-of-pocket payments, which can take the form of fees for services, co-payments or direct expenditures, create a financial barrier of access and compromise equity (Carrin et al., 2008: 858). Thus, the introduction of user fees in healthcare ‘remained anathema to traditional attitudes within WHO that PHC should be funded by public financing’ (Lee and Goodman, 2002: 109).
Since the 1980s, the WB has increased its activity in the global health policy discourse. Despite its lack of expertise regarding health systems, the Bank became the most important global health actor in terms of financial resources. Loan conditionalities provided the WB with powerful means to disseminate its ideas and to influence ministries of finance as well as of health (Abbasi, 1999: 866; Kaasch, 2013: 52, 58; Tichenor and Sridhar, 2017: 1). In the 1990s, the WB shifted its approach ‘to development assistance, which sees systemic reform as a way to improve the impact and sustainability of investments in health’ (De Beyer et al., 2000: 169). This includes securing sustainable HCF.
The Bank has taken a leading role in influencing HCF debate by arguing for a user-fee approach, while also advocating the establishment of pre-payment insurance schemes where appropriate, opening markets to private healthcare providers and generally increasing the use of market mechanisms. The introduction of user fees in government health facilities was strongly supported in WB-financed projects (Lee and Goodman, 2002: 99–100, 107). With the introduction of user charges, the Bank hoped to make ‘health systems more equitable, considering that the rich – who benefit most from public services – would have to pay. This would theoretically free up government resources that could be directed to programmes and facilities for the poor’ (Tichenor and Sridhar, 2017: 3).
There seems to be agreement that, in reaction to growing protests against its insistence on the universal applicability of market-oriented development programmes (the ‘Washington Consensus’), the WB has tried to change its image (Abbasi, 1999: 866). The Bank reinvented itself as a ‘global knowledge bank’ trying to improve and decentralise its knowledge management, to increase sensitivity and responsiveness. However, it has been argued that this new strategy is a way to ensure the reinforcement of disciplinary neoliberalism rather than to improve the prospects for development as such (Plehwe, 2007). The WB
turned away from an aggressive and coercively conditional neoliberal approach towards a flexible, collaborative, and comprehensive neoliberal approach. The organisation has attempted in recent years to renew the legitimacy of its developmental mindset, while maintaining a market-centric mentality. Thus, the World Bank evolved in rhetoric and practice [. . .] to revitalise its widely condemned (yet stalwartly maintained) neoliberal discourse. (Bazbauers, 2014: 91)
According to the ‘division of labour’ between the twin organisations, the IMF delegated the issues ‘health’ and ‘education’ to the WB because the IMF was ‘not qualified to advise on the health and education sectors’ (Odling-Smee, 2006: 182, FN 53; see also Orenstein, 2008a: 84–85). 2 However, the IMF is an important actor insofar as its loans, coupled with SAP, often include the policy condition to reduce public expenditure on the social sector, including spending on public health and healthcare delivery (Lee and Goodman, 2002: 99). This typically involves a mix of privatisation, liberalisation and fiscal austerity programmes. Several authors see sufficient evidence to indicate that these programmes, contrary to non-IMF lending, have been significantly associated with weakened healthcare systems, reduced effectiveness of health-focused development aid, and increased mortality rates in FSU countries (cf., for example, Stuckler and Basu, 2009; Stuckler et al., 2008).
Vetterlein (2012) considers this common critique, which has also been levelled at the WB (Armada et al., 2001), as overstated. Comparing the discursive level with developments on the policy and operational levels reveals that the social agenda has grown incrementally since the late 1960s, even in times when neoliberalism was the dominant paradigm. She states that both organisations have overcome their tendency to provide standardised responses that ignore local social knowledge. Since, at least the early 2000s, the WB’s emphasis on education and health care received ‘operational significance’ (Vetterlein, 2007) and the Bank retreated from the widely criticised programme of conditionality (Cormier and Manger, 2020). In a similar vein, Broome (2015) and Schlaufer (2019) argue that the IMF has moved to a model of avoiding a one-size-fits-all solution and increasingly tailors its advice to the advised country’s context and policy capacity.
Using data on post-communist IMF programmes for the period 1994–2010, Beazer and Woo (2016) argue that, rather than universally benefitting or harming reforms, the effects of stricter IMF conditionality depend on domestic partisan politics. For the FSU, Stone (2002b) finds that the IMF and its loan conditionality is not as powerful as some critics fear; its power depends on how much credibility it can muster from country to country (see also Pop-Eleches, 2009; Weyland, 2006).
Due to a lack of resources, the WHO and its regional organisations have lost their dominance in the healthcare sector and ‘remained [. . .] a relatively low-key player[s]’ (Lee and Goodman, 2002: 109). While the formerly secure funding from its member states has stagnated, the WHO ‘has become reliant on voluntary contributions from governments and other actors usually earmarked for particular activities favoured by the donor’ (Clift, 2013: 6). In addition, the WHO ‘was accused of cronyism, a lack of direction and cohesion, a reluctance to shift its focus away from prevention of infectious diseases, and a reluctance to tarnish its image with governments’. Consequently, the WHO was left with providing medical expertise or technical support to WB projects (Abbasi, 1999: 868). Eventually, it began to refashion itself as the coordinator, strategic planner and leader of global health initiatives as a strategy of survival in response to this transformed international political context (cf., for example, Brown et al., 2006; Fee et al., 2016; Gautier et al., 2014; Ruger, 2014).
Overall, in the policy field of healthcare, different IOs ‘promote different, contradictory policy models, generating global discourses about desirable national social policy’ (Kaasch, 2013: 49). However, there are some general lines of recommendations among all IOs working on healthcare in the FSU. Lee and Goodman (2002: 101) argue that, by the late 1990s, the debates over public versus private financing had been replaced by a widespread acceptance of the need for multiple sources of HCF, including a public-private mix. While IOs and donors certainly played a part in this process, their contribution to the introduction of market elements in healthcare should not be overstated (Barr and Field, 1996: 308). The desire for complementary sources of healthcare financing has been partly driven by particular ideas and values about the role of the state in many FSU countries (Lee and Goodman, 2002: 97); this resulted in a conscious decision to ‘go “back to Bismarck” [through] re-establishment of pre-Soviet structures and institutions’ (Rechel and McKee, 2009: 1187). The introduction of health insurance schemes was thus widely favoured.
Within these IOs there is no predominant position or coherent (theoretical) model of an ideal healthcare system but rather ‘a high level of uncertainty about best models, coming with vague positions and consensual knowledge’ (Kaasch, 2013: 52). Therefore, it is important to look at the many publications of the involved IOs in detail, and over time, in order to identify and interpret the shifts and nuances in positions and recommendations for the reorganisation of the healthcare system and the introduction of an MHI in the FSU.
Methodology
To do so, the publications and internal documents of the involved IOs covering the period from 1991 to 2018 have been scrutinised. Earlier empirical investigations of the scope of the World Bank’s scientific activity have analysed the IO’s publication including works of World Bank staff in other media, scientific journals and books (Ravallion and Wagstaff, 2012). However, I have used only the IOs’ own publication series and project documents because publications authored by the IOs’ staff carry the caveat that the publication represents the opinion of the author(s) and not necessarily that of the IO. Thus, I use a narrow definition of IOs publication in order to guarantee capturing the IOs’ position on the issues under study.
Appel and Orenstein (2018) claim that ‘[a] number of former Soviet republics, particularly resource-dependent and Central Asian states, exhibited limited enthusiasm for many elements of the neoliberal reform package’ (p. 62) and often had to be pushed to reform. This article looks at three ‘resource-dependent and Central Asian states’ in a most similar cases design, namely Kazakhstan, Kyrgyzstan and Russia (with Kazakhstan fitting both criteria), to examine the advice given by these IOs for the reorganisation and management of these countries’ healthcare systems between 1991 and 2018.
While these supposedly reluctant reformers under study are similar, they reacted rather differently to the advice given. After the disintegration of the Soviet Union in 1991, all of the newly founded states were in a vulnerable financial position and had to simultaneously reconceptualise their entire welfare system from the same starting point of the Soviet model. In the beginning, all selected countries were willing to accept international knowledge transfer. However, over time, Kazakhstan and Russia changed their attitude. While Russia aimed to emancipate itself completely from foreign support and international knowledge transfer by IOs (cf., for example, Belyaeva, 2019), Kazakhstan began to insist on being treated as an equal partner, leading to a more selective process of knowledge transfer (cf., for example, Ambrosio and Lange, 2014; Schatz, 2008).
For the countries under study, the search in the IMF archives (http://archivescatalog.imf.org), including both the institutional archive and the Executive Board documents, and on the IMF’s website (www.imf.org) resulted in 2259 documents. Here, the country names were used as the keyword/search term.
In the case of the WB, its flagship publication, the World Development Report (WDR), has been analysed. Ravallion and Wagstaff (2012) regard the WDR as having had considerable impact on policy and practice by connecting existing knowledge to policy-makers and their advisors. A total of 10 WDRs (for the years 1988, 1991, 1993, 1996, 1997, 2001, 2003, 2005, 2012 and 2013) have dealt with MHI. A general search for other WB publications and documents was also conducted on the Bank’s website (http://documents.worldbank.org/curated/en/docadvancesearch), resulting in 417 documents.
In addition, WB projects relevant for the introduction of an MHI in the countries under study have been scrutinised (www.projects.worldbank.org). A total of 16 projects dealing with the introduction of an MHI have been conducted by the WB in the countries under study (five in Kazakhstan, six in Kyrgyzstan and five in Russia). The examination of the project documentation resulted in 215 documents.
The search through the WHO’s search platform (https://apps.who.int/iris/) included the WHO general programme of works, documents of the Regional Committee for Europe, World Health Reports (WHRs) for the years 1995–2013, and the Reports of the Director-General. Here, the country names were used as keyword/search term. This resulted in a total of 87 documents.
In order to manage the huge number of documents, the text analysis software MaxQDA was used for a first selection of potentially relevant documents (as most document titles were all but instructive). A ‘simple keyword search’ was applied; as keywords were chosen ‘health’ (this keyword has not been applied to the WHO as this organisation is obviously concerned with health-related issues) as well as ‘health insurance’ and ‘insurance’ (as health insurance might be labelled differently, for example as ‘medical insurance’) and common abbreviations (such as SHI, MHI, MHIF). In the case of the WDRs and documents of the WHO, additional search terms were used: the single country names (and their common misspellings, like ‘Kazakstan’) as well as ‘Soviet’, ‘transitional’ and ‘socialist’ in order to increase the relevance of research results. For the search of WB publications and documents, the single country names, their common misspellings and the term ‘Europe and Central Asia region’ was used.
The results of the keyword search were automatically coded. Documents that did not yield any results were deleted, while the rest had been manually selected for relevance (see Table 1).
Number of analysed documents.
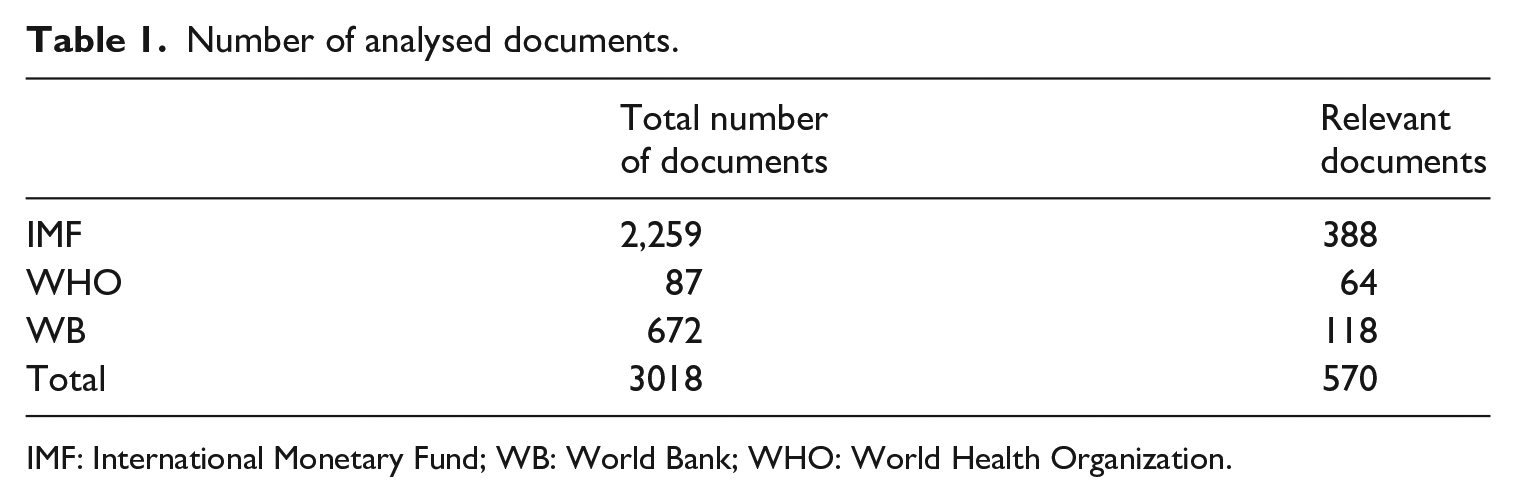
IMF: International Monetary Fund; WB: World Bank; WHO: World Health Organization.
The 570 relevant documents have been included in the following analysis on the attitude of IOs towards the introduction of an MHI in the FSU. The qualitative content analysis is based on manual coding whereby the researcher reads all 1149 text segments coded ‘health insurance’ (the code ‘insurance’ was, if relevant, re-coded to ‘health insurance’) and draws conclusions regarding the research questions: (1) the position of the respective IO on the financing of healthcare (out-of-pocket payment; private, for-profit insurance; social insurance; and/or tax funding); (2) the supposed promotion of neoliberal reforms (‘Washington Consensus’) which manifests itself in advertising spending cuts and privatisation (i.e. a reduced role of the state) in the healthcare sector; and (3) the IOs’ evaluation of the countries’ degree of collaboration, their behaviour towards reform advice (resistant, reluctant, cooperative, pro-active or over-zealous introducing ‘avant-garde measures’).
Results
While all IOs working on systemic healthcare reform in the FSU support health insurance schemes as an additional source of HCF, there are divergences, especially regarding the question of out-of-pocket payments. The WB argued for a health insurance scheme in the countries under study because competition should lead to better healthcare quality and a more efficient use of resources. On the question of out-of-pocket payments, the WB has changed its position; it recognised their regressive nature and now argues for an only limited use of user fees. The WHO did not take an official position on insurance-based health systems. However, it supported health insurance schemes introduced by the WB, for example in Kyrgyzstan. Nevertheless, the WHO has been consistently against out-of-pocket payments.
Using the empirical material to test the assumptions of the literature regarding the neoliberal agenda (‘Washington Consensus’) promoted by the WB and IMF reveals a more detailed, and therefore nuanced, picture. The empirical results make some revisions with regard to spending cuts and the role of the market necessary, and also support the strain of literature that qualifies the power of loan conditionality. In addition, the material indicates ‘avant-garde measures’ of neoliberal reforms exceeding the given advice.
Spending cuts
The IMF’s neoliberal recommendations for all FSU countries typically involve the reduction of staff and overcapacities in the healthcare sector and increased efficiency. Healthcare spending should focus on specific aspects and target the most vulnerable groups, as well as introduce structural reforms and market elements (cf., for example, Horton, 1996; International Monetary Fund (IMF), 1997b: 29, 1997d: 87–88, 2000: 20).
By the end of 1992, concerns in the countries about the hardship the IMF’s austere budgetary policy imposed on social sectors (in particular, the health sector) began to grow (International Monetary Fund (IMF), 1993a: 31). In 1993, the IMF (1993b) started to recommend as a remedy
[s]trengthening the social safety net to address the needs of households adversely affected by economic reforms and ensure a minimum standard of living. This includes support for critical social services such as health and education where service delivery and quality are at risk. (p. 47)
IMF Director Kiekens admitted in 1995: ‘The sequestration of expenditures had been clearly unsustainable, and had been highly detrimental to the necessary public investments for infrastructure, health care, and education’ (International Monetary Fund (IMF), 1996a: 37). The IMF also became concerned with expenditure prioritisation of national governments; it considered the declining expenditures on education, health and social protection as troubling, particularly considering increasing poverty levels (International Monetary Fund (IMF), 2001: 42). Instead, ‘[e]xpenditures on health, education, and other social services are expected to be protected to provide for an effective social safety net and for the investment in human capital necessary for longer term economic growth’ (IMF, 1997a: 7).
In 1997, the IMF ‘was trying to correct a formidable accumulation of misrepresentation’: the United Nations Children’s Fund (UNICEF)
had reiterated in its annual report that structural adjustment programs were harmful to children. With statistics, the Fund had to explain that its programs led to significant increases in education and health, among other areas. [. . .] Even though it was in a continuous state of dialogue with institutions such as UNICEF, and those institutions were currently more aware and supportive of the Fund’s activities than before, they tended to continue to issue their old critical views of the Fund, which they had held more than a decade previously. It was partly a function of the ease with which organizations could issue recycled press releases. The Fund had to oppose vigorously the tendency of other organizations, including nongovernmental ones, to reiterate outdated views of the Fund. (IMF, 1997c: 49)
Overall, the IMF considers healthcare as important for growth and social stability. Regarding Kazakhstan, Director Ngumbullu stated, ‘We are encouraged by the authorities’ commitment towards [. . .] the importance of instituting reforms in the health and education sectors which are essential for sustained economic development and social stability’ (International Monetary Fund (IMF), 2003b: 17).
The WB has made similar recommendations: Within the Second Health Sector Reform Project 3 (2001–2006) in Kyrgyzstan, the Bank pro-actively conducted a dialogue with the Ministry of Finance on budget problems in the health sector and ‘[a]s a result of the Bank’s intervention, key programs for vulnerable groups (health insurance programs) received expected funding’ (World Bank (WB), 2007a: 8). Another decline in healthcare spending in the 2000s could be rolled back with support from the World Bank (WB, 2014b: 20). These spending cuts considered excessive by the IOs can be interpreted as ‘avant-garde measures’ by the countries under study.
Involvement of the private sector
The literature assumes that most IOs generally prescribe only a limited role of the state in healthcare, while stressing the role of the market and of individual responsibility. One exception is the WHO, which traditionally has been sceptical of private involvement in the healthcare sector. In its 1998 WHR, it raised concerns about both equity and allocation issues and about the quality of care considering the significant increase of the role of the private sector in the delivery of services:
The quest for cost-containment and more efficiency, and the imperative to identify more resources, frequently take precedence over the health-for-all principles and values. Consequently, from the patient’s point of view, often what is referred to as ‘reform’ does not contain any elements of improvement. Patients are asked to pay more and receive less. (World Health Organization [WHO], 1998: 145)
The WHR 1999 doubts that ‘market forces which have increased productivity in many sectors of the world economy’ can ‘achieve similar success in health services or health insurance’ (World Health Organization (WHO), 1999: xiv). Instead, governments need to exercise strong stewardship:
taking the lead in explicitly stating societal objectives for health systems, establishing the roles of the public and private sectors in pursuing them, regulating and managing systems and assessing performance to guide future decision-making. When government stewardship was weak, privatization failed to meet societal objectives. (WHO, Regional Office for Europe, 2002: 19)
More surprisingly, the WB makes similar arguments. In order to protect individuals from large and unpredictable health expenditures, the WDR 1988 considers risk-sharing through health insurance as desirable. It assigned an important role in setting up these schemes to national governments (World Bank (WB), 1988: 137). For some time, the WB did not think that the private market could be trusted with the task of providing widespread access to healthcare for the poor: ‘Private markets will not give the poor adequate access to essential clinical services or the insurance often needed to pay for such services. Public finance of essential clinical care is thus justified to alleviate poverty’. Government action needs to compensate for problems generated by insurance market failure and to foster the reduction of poverty: ‘Governments have an important role to play in regulating privately provided health insurance, or in mandating alternatives such as social insurance, in order to ensure widespread coverage and hold down costs’ (World Bank (WB), 1993c: 5, 57, quotes 5; see also Klugman and Schieber, 1999: 35–36).
The 1996 WDR especially advised countries in transition that the state needs to guarantee access to PHC and cost containment (World Bank (WB), 1996: 131). In its Health Reform Pilot Project
4
(1997–2004) for Russia, the Bank takes a critical position on private sector involvement:
The health service sector, with its dual objectives of efficiency and equity and its inherent market imperfections, is not a typical economic sector. Its development requires a balance between public sector involvement and market-type operations that is difficult to achieve. (World Bank (WB), 1997: 12)
The involvement of the private sector needs guidance through a regulatory framework: ‘Many personal health services can be provided efficiently by the private sector once an appropriate incentive structure and regulatory framework are in place’ (WB, 1997: 55).
Repeatedly, the WB has made a case for government intervention as a corrective in order to reduce out-of-pocket payments through pre-payment insurance schemes (including subsidies; World Bank (WB), 2005b: 145). Thereby, the state should support ‘the contributions of all social and economic systems to people’s risk management’ (World Bank (WB), 2013: 38). The IMF has also argued against a rapid privatisation of the healthcare sector in Kyrgyzstan stating that ‘before embarking on promotion of privatization in health care, authorities should consider introducing an adequate regulatory framework for private health care and tackle the issue of streamlining the public health facilities’ (IMF, 2003a: 8).
The loan conditionality and ‘avant-garde measures’
The IMF has complained that after the introduction of market reforms in FSU countries ‘[t]here has been little attention paid so far to the question of “optimality” of such institutional arrangements’ (Lorie, 2003: 8). It has argued that a successful devolution of responsibilities for HCF requires institutional capacities on the national and subnational level and robust revenue sources or effective fee arrangements (Lorie, 2003: 29, 33). For the same reasons, ‘the World Bank expressed concerns about premature establishment of health insurance systems in countries such as Bulgaria, Kazakhstan, Kyrgyzstan, Romania, and Ukraine’ (Rechel and McKee, 2009: 1187).
In the early 1990s, Kazakhstan and Kyrgyzstan showed much enthusiasm for health insurance schemes. Both countries, after experimenting with insurance and provider payment reforms in selected regions, had proceeded the furthest in terms of introducing health insurance funds, loosely based on the Russian model. However, they had little understanding of the basic underlying concepts, the range of options and the steps for implementation. As they did not want to borrow for health expenditures, this resulted in ‘a tendency to apply OECD models and standards with only one-fifth to one-tenth the level of resources’ (Staines, 1999: 36). Consequently, a nationwide implementation of the health insurance legislation in Kazakhstan and Kyrgyzstan had been delayed due to depressed economic conditions (Klugman and Schieber, 1999: 34).
Russia resorted to its NEM pilot projects of the late-Soviet era for the introduction of its MHI and had the relevant legislation in place in 1991. Thus, IOs aimed at improving the already established system.
Kazakhstan
Kazakhstan, ‘taking the lead in health insurance’ (Rose, 1999: 4) and introducing ‘the idea of health insurance [. . .] more quickly and comprehensively’ (World Bank (WB), 2000: 121, FN 146) than any other FSU country, has been an unlikely trailblazer. While the Soviet Republic participated in reforms to the Semashko system, it unilaterally cancelled its NEM pilot projects in April 1990. After independence in 1991, the Semashko healthcare system in Kazakhstan initially did not change significantly, as the government gave priority to political and economic reforms (Kulzhanov and Healy, 1999: 10, 54).
Nevertheless, the general principles of NEM had taken root. In early 1992, Kazakhstan’s parliament enacted a law to fundamentally change the existing Semashko system both in the management and financing of care:
A new employer-based payroll tax [. . .] is to finance the system, with monies coming from the government for special populations such as the elderly, the unemployed, and the disabled. The insurance is to cover a basic package of services. (Langenbrunner et al., 1994: 6–8, quote 7)
A so-called MHIF was to be set up by each region which was ‘protected from and independent of the annual budget process [. . .] to collect contributions and to allocate them to local health insurance organizations’ (Langenbrunner et al., 1994: 7). This raised the expectation that the new health insurance scheme would be implemented in 1993. However, the law had been under discussion by parliament for several years.
In the meantime, a number of regions went ahead and established in 1992 several pilot projects extending greater flexibility in terms of financing, payment and organisation of healthcare delivery. The pilot projects tested new approaches such as restructuring PHC, insurance funding, new provider payment mechanisms and user fees (Kulzhanov and Healy, 1999: 10; Langenbrunner et al., 1994: 6–8). These projects initiated a national debate about healthcare reform supported by the WB: As early as 1993, the WB wanted to use Kazakhstan’s strong motivation for reform as
starting [points] for restructuring the health system, including privatizing some services and introducing medical insurance. [. . .] Given the strain on the budget, it is unrealistic to assume that the Government can continue to sustain health care through direct budget transfers. Alternative forms of financing and cost recovery will be needed. (WB, 1993b: 11)
In order to establish an additional and stable source of financing, the insurance experiment was extended nationwide in June 1995, which guaranteed health insurance for all citizens. Kazakhstan ultimately opted against a single-payer system (recommended by international advisors) and chose to adopt the Russian model of health insurance, which created overlapping financial responsibilities, a fact the WB considered ‘unfortunate’ (Kulzhanov and Healy, 1999: 10, 53; Wickham et al. 1999: 12–13; quote World Bank (WB), 2001: 8).
The MHIF was finally implemented in 1996 as an extrabudgetary fund, which operated as a parallel structure alongside the previous system of budgetary funding (Katsaga et al., 2012: xviii). According to the Vice Minister for Health, Aikan Akanov (1999), Kazakhstan wanted to apply market mechanisms and decentralisation to the healthcare system as well:
As Kazakhstan moves further away from comprehensive state control of the economy, centralized financing of the health sector will be less consistent with economic conditions. [. . .] This requires [. . .] encouraging mixed sources of financing, introducing economic methods of managing health service providers, encouraging competition and [. . .], developing various forms of ownership, and implementing a program to privatize health care provision. [. . .] Health will be placed in direct relation to the costs that poor health incurs to society, and economic incentives to promote good health will emerge. (p. 111)
The MHI introduced the principle of payment for work done. For Akanov (1999), the healthcare finance reform
is intimately related to the introduction of improved methods of economic management of health services at all levels. [. . .] The main effort in this area is directed toward promoting different modes of ownership and privatization and reducing state involvement. (p. 111)
Overall, the reform process has been characterised by considerable fragmentation because implementation at regional level varied extremely: around one-quarter of the population was left without coverage. In addition, the Kazakh healthcare system has remained severely underfunded (Kulzhanov and Healy, 1999: 18, 55, 57). Consequently, the MHIF had large revenue shortfalls and in 1998 defaulted on some commitments as Kazakhstan was hit by repercussions of the Russian financial crisis. The IMF and WB recommended closing down all extrabudgetary funds, including the MHIF, and to revert to the previous tax-based system with budgetary health financing (Kulzhanov and Rechel, 2007: 42).
This short intermezzo of an MHI in Kazakhstan between 1996 and 1998 was not favoured by the WB, which considered it an ‘ill-conceived health insurance experiment’ (WB, 2007b: 7). Despite an ongoing project, the WB was not able to stop the Kazakh government from introducing an MHI for which it considered the institutional framework insufficient. The IMF experienced similar behaviour in 1998 stating its ‘impression from previous meetings on Kazakhstan, that it was a political choice of the authorities to drastically and quickly reduce the role of the government in the economy’. Under Kazakhstan’s special circumstances, the IMF doubted the feasibility of such a strategy (International Monetary Fund (IMF), 1998: 9). With the Social Health Insurance Project 5 (2016–2021), however, the WB supports the design, implementation and management of the national mandatory Social Health Insurance System (SHIS), which it considers better designed than its predecessor. Thus, Kazakhstan undertook ‘avant-garde measures’ against the advice of IOs demonstrating the limited power of loan conditionality.
Kyrgyzstan
Kyrgyzstan too ‘is regarded as a pioneer in health system reforms among its peers’ in the FSU. Since the early 1990s, the country has adopted successive health reforms and has introduced significant changes in financing and service delivery arrangements (Nguyen and Strizrep, 2019: 1).
Responding to financial problems in Kyrgyzstan’s health sector in the early 1990s, the government ‘has started to plan for, and implement, an extremely ambitious reform of the health system in order to encourage the private sector, change patient and provider incentives, modernize and generate additional revenues’ (WB, 1993a: 133). The Health Insurance Law of 1992 introduced a payroll-financed MHI. While these plans were at very preliminary stages, the WB voiced
concerns in principle about the Government’s health care reform plans: first, whether an insurance-based system for the health sector would lead to gaps in coverage; second, whether the introduction of health insurance would encourage cost containment; and third, whether the proposed payroll financing arrangements are efficient. There are also some major practical problems relating to the new proposal: whether the reforms could be supported in view of the lack of appropriate institutional systems, and whether attempts to implement the reforms would divert attention from more urgent problems facing the sector. (WB, 1993a: 134–135)
Beyond the economic crisis the country was suffering, the WB considered it
clear that the preconditions for implementation of the recently enacted health insurance law do not currently exist in Kyrgyzstan. Improvements in the banking system, information system, and tax collection mechanisms are needed before drastic and fundamental changes should be implemented. (WB, 1993a: 137)
Thus, the WB advised that ‘the Government should rethink its plans for the introduction of health insurance and at least delay the implementation of the new law’ and offered technical assistance to assist the government to develop its reform plans further (WB, 1993a: 137, quote 144).
Unlike in the case of Kazakhstan, the IOs were successful in reining in Kyrgyzstan’s move towards ‘avant-garde measures’ and in sustaining their supervisory capacities. In 1994, the Kyrgyz government signed a Memorandum of Understanding with the WHO Regional Office for Europe to implement a comprehensive, national health reform programme called ‘Manas’. Within this framework, the government implemented a health insurance pilot project in the Issyk-Kul region (WB, 2005a: 10).
With the approval of the ‘Manas’ programme in 1996, the Kyrgyz government started a two-phased health sector finance reform. The first phase, from 1997 to 2001, focused on restructuring the inherited Semashko system and obtaining additional revenues through the introduction of a payroll-financed MHI. HCF was changed to capitation- and output-based payment mechanisms and the established MHIF led to a progressive centralisation of the purchasing function of health services and the pooling of funds (WB, 2007a: 43, 289, 2014a: 3–4). The WB (2007a) supported ‘Manas’:
The real significance of this reform period was to create the foundation for the second phase by creating the new institutional structure[,] the MHIF[,] and allow it to learn purchasing and the use of prospective provider payment mechanisms using small amounts of funds. For these contracted facilities, the MHIF introduced new reimbursement procedures: case-based payment to hospitals and capitation-based payment to primary level health facilities. (p. 295)
Since 2001, in the second reform phase, a single-payer system was gradually introduced in Kyrgyzstan as well as an explicit specification of the benefit package through the so-called State Guaranteed Benefit Package (SGBP) and a restructuring of the service delivery system. The SGBP clearly defined the rights and obligations of patients and the state with regard to provision of health services and clarified the entitlements of different population groups (WB, 2007a: 43–44, 292, 2014a: 3–4). In 2001, the SGBP and the pooling of budget funds and insurance contributions were introduced in two pilot regions. Each year, two additional regions established regional health financing pools until the entire country was covered by 2005. The regional pools were merged at the national level in 2006, ending fragmentation of health resources and duplication of services (Giuffrida et al., 2013: 5; WB, 2014a: 4). Beyond the financing mechanism, these reforms had important institutional dimensions. The MHIF was established as a parastatal organisation under the Ministry of Health outside the core public bureaucracy, freeing it from the Soviet-era input-based budgeting mechanisms creating incentives for downsizing and savings (WB, 2007a: 297).
During 2002, implementation of health reforms slowed down, seriously jeopardising the single-payer system. These problems have been discussed at the highest levels of the Kyrgyz government. At a roundtable in February 2003, the President of Kyrgyzstan expressed his strong support for the reforms. The resolution based on this roundtable has been adopted by the government and developed into a time-bound action plan. Thereby, the Kyrgyz government entered into a self-commitment to implement the action plan (World Bank (WB), 2003: 57).
Overall, the WB considers the Kyrgyz reforms successful and replicable in other transition economies because the chosen comprehensive approach included careful sequencing of various reform steps and step-by-step implementation and attention to institutional aspects (i.e. MHIF as a parastatal agency). This was ‘an effective implementation approach and helped build capacity and stakeholder support as well as learning by doing’ (WB, 2007a: 44–45, quote 44; see also Giuffrida et al., 2013: 4).
In Kyrgyzstan, IOs were able to curtail ‘avant-garde measures’ in the healthcare sector. The country followed the advice and chose a more incremental approach for the introduction of an MHI. Similarly, despite political momentum and parliamentary support for the introduction of a flat tax in 2001, the Kyrgyz President ‘responded to IMF pressure and thwarted it’ (Appel and Orenstein, 2018: 104). The IMF considered Kyrgyzstan’s tax base inadequate for such a reform and was able to stop this neoliberal reform project.
Russia
Even though Russia experimented with voucher privatisation in the mid-1990s, an in the West unproven ‘avant-garde measure’ (Appel and Orenstein, 2018: 22), it did not use ‘avant-garde measures’ in the healthcare sector. Instead, Russia fell back on the reform efforts of the late Soviet period 6 and adopted on this basis the Health Insurance Law in 1991, which was amended in 1993. In the beginning, the WB had no formal health sector strategy for Russia; thus, it aimed to help the country rehabilitate and reform the health sector and build an effective and efficient insurance scheme through three health-related projects in the mid-1990s (Twigg and Skolnik, 2005: 20). However, the Health Insurance Law was never fully implemented due to ‘opposition within government and by powerful factions’ (IMF, 1996b: 33).
The IMF noted that in the early 2000s most of the government’s reform objectives were not new, but that preparation and implementation of reforms ‘have been stalled for some time because of resistance from vested interests’. In some areas there was disagreement about the basic concept, and in others – like the health sector – there was consensus on broad objectives but disagreement on the detailed planning (International Monetary Fund (IMF), 2005a: 13, quote IMF, 2004: 24; Klugman and Schieber, 1999: 35).
In addition, in 2005, ‘the unexpectedly strong opposition to the social benefits reform appears to have reduced the resolve to move ahead with health and education reforms’ (IMF, 2005c: 16). This resistance was one of the main reasons for delays in health reform:
Key officials stressed that concerns about the social impact of reforms were now clearly weighing more on policy makers and that reforms in this area were not only going to be slower than foreseen [. . .], but also require more budgetary resources than previously expected. (IMF, 2005c: 25)
IMF Director Mozhin added, ‘In the tense political environment that emerged in the aftermath of this major reform effort, the postponement of other painful reforms was unavoidable’ (IMF, 2005b: 8). Furthermore, ‘health and health care remain a relatively low priority on the national agenda’ (Twigg and Skolnik, 2005: 8).
In 2007, Director Kremers diagnosed a lack of vigour on the part of the Russian government: ‘It is unfortunate that the authorities’ resolve and the public’s support for further structural reform have weakened, well ahead of forthcoming elections. Delays in reforms of the health and education sectors [. . .] are regrettable’ (International Monetary Fund (IMF), 2007: 26). Instead, in an attempt to facilitate reforms through increasing social spending, the Russian authorities disputed with the IMF over budget discipline and expenditure priorities (IMF, 2007: 31).
Due to the global financial crisis of 2008, the Russian budget became less flexible, with an increase in permanent spending. In 2009, the IMF summarised,
Most of these reforms are technically well-advanced, not least health and education reforms. However, the reforms are socially sensitive and had little political support during the period of high oil prices and robust economic growth. The authorities explained to the mission that, among the key reforms still ahead, they would want to give priority to health and education. However, we also sensed a clear realism on the part of senior officials that there is still no strong political momentum behind such reforms. (International Monetary Fund (IMF), 2009: 53)
Conclusion
Based on a qualitative content analysis of 570 documents produced by the three IOs analysed here, it can be clearly shown that while all IOs support health insurance schemes as an additional source of HCF, there are divergences, especially regarding the question of out-of-pocket payments. The WHO has been consistently against out-of-pocket payments. The WB, however, has changed its position; it recognised the regressive nature of user fees and now argues for limiting their use.
Nevertheless, the IOs’ advice for healthcare reform in the FSU seems less heterogeneous than one might have expected. There are no country varieties; all countries under study receive similar advice, even though Broome (2015) and Schlaufer (2019) argue that IOs have moved away from one-size-fits-all solutions. This might be explained by their similar starting conditions after the break-up of the Soviet Union and the fact that systemic healthcare policy did not belong to the IOs’ core competences. While IOs such as the WB and the IMF argue for the introduction and strengthening of market elements in the healthcare sector (including spending cuts), they simultaneously stress the overall importance of the sector and urge sufficient and effective institutional regulations. Appel and Orenstein (2018) claim that the IMF became ‘more supportive of welfare spending than in past’ (p. 170) after the global financial crisis of 2008. However, as the analysis reveals, the IMF has tried to offset adverse effects of its neoliberal reform concepts on the social sector since the mid-1990s. However, it cannot surprise that these IOs have maintained ‘a market-centric mentality’ (Bazbauers, 2014: 91) and rhetoric, as this is consistent with the aim and scope of the IOs in question. Nevertheless, this rhetoric is more nuanced and reflective than often described in the literature.
Notwithstanding, Farnsworth and Irving (2018: 137) argue that social policy is still considered a basic economic function. Therefore, variety in advice indicates ‘a change in political strategy, rather than technocratic epistemology, and one that has not been accompanied by an intelligible revision to thinking on social spending or the wider purpose of social policy in global stability’ (Farnsworth and Irving, 2018: 136). Kentikelenis et al. (2016) go even further, arguing that multiple layers of rhetoric and ceremonial reforms have been designed to obscure the actual practice of adjustment programmes. They find little evidence of a fundamental transformation of IMF conditionality.
This leads one to question the relationship between rhetoric and practice: do these IOs actually practice moderation in the projects they fund or are they engaging in deception? The discrepancy between IOs’ rhetoric and practical policies might be caused by the IOs’ inability to moderate or constrain countries willing to reform. While the limited power of conditionality has often been discussed in connection with a country’s resistance towards proposed reform measures, Appel and Orenstein (2018: 26) coined the term ‘avant-garde measures’; neoliberal reform efforts that exceed required policies and were ‘rather opposed or treated ambivalently’ by the IOs. As this study has shown, the IOs under study have objected to both a rapid and unprepared introduction of MHI schemes and excessive spending cuts in the welfare sector. While the IOs have been successful in preventing or modifying reform concepts in Kyrgyzstan, the introduction of an MHI in Kazakhstan in 1996 provides an example of the fact that in some circumstances the IO cannot or did not try hard enough (i.e. maybe not using conditionality but just advice) to moderate the neoliberal zeal of the national government. Kazakhstan has enacted ‘avant-garde measures’ and has not heeded the IOs’ advice rendering their intervention unsuccessful. The MHI experiment ended in failure; in the end, Kazakhstan had to follow the IOs’ advice and closed the MHIF.
In Kyrgyzstan, the IOs were successful in their intervention against ‘avant-garde measures’ regarding the introduction of an MHI and a flat tax (i.e. preventing knowledge transfer by stopping the institutionalisation of the policy transfer). The Kyrgyz government has been working closely with the WB. It seemed continuously willing to accept international knowledge transfer and chose a pro-active, reform-oriented approach.
Russia, however, had an MHI legislation already elaborated and in place. The IOs had not developed a health strategy for Russia and, therefore, engaged merely in the optimisation of the existing healthcare system. Overall, Russia has shown neither much pro-activeness and collaboration nor outright resistance against international advice. Russia did not commit to recommended structural reforms; instead, it chose to throw money at the problem, causing disputes with the IMF. However, it has not become clear from the analysed documents that Russia aimed to emancipate itself completely from foreign support and international knowledge transfer by IOs as claimed in the literature. There was not resistance, but rather a lack of vigour on the part of the Russian government.
While Appel and Orenstein (2018: 62) claim that resource-dependent and Central Asian FSU countries exhibited only limited reform enthusiasm, this analysis shows that some of these countries have indeed shown enthusiasm by even applying ‘avant-garde measures’ to their healthcare sectors exceeding the required policies. Thus, when judging the work of IOs, one should keep in mind that IOs might be the provider, but not necessarily the enforcer of knowledge and, thus, not neglect the agency of the countries receiving advice. These countries are more than mere recipients of international knowledge transfer, sometimes themselves becoming the drivers of neoliberal reforms (against the advice of the IOs).
Footnotes
Funding
The author disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) in the context of the Collaborative Research Centre 1342 ‘Global Dynamics of Social Policy’ (Project No. 374666841) as subproject B06 ‘External reform models and internal debates on the new conceptualization of social policy in the post-Soviet region’.