
Abstract
The way in which international actors formulate proposals for reforming or establishing public social policies not only varies between different organisations but is also dependent on the policy field in question. This article compares the positions of two international organisations (IOs), the Economic Commission for Latin America and the Caribbean (ECLAC) and the Pan American Health Organization (PAHO), on the two related social policy fields of health and long-term care in Latin America. We apply qualitative document analysis to reports and strategy articles published by ECLAC and PAHO between 2000 and 2015. The analysis finds that despite some similar proposals by both organisations, there are also clear differences between their positions depending on the policy areas. While both organisations see the need to establish healthcare and long-term care as a human right, they have different ideas on targeted and universal approaches. Moreover, with long-term care as a new and emerging policy field, there is still much more variation in how the IOs address the topic, while proposals on healthcare are shaped by previous debates at international and regional levels.
Introduction
Care provision – both for people with acute health issues and long-term impairments – is a fundamental need in human life. As such, healthcare (HC) and long-term care (LTC) are regarded not only as a matter of private concern but also as crucial fields of social policy (Kaasch, 2015; Österle and Rothgang, 2021). In contrast to long-existing public HC systems, the necessity for social protection for LTC has increasingly surfaced only in recent decades. This development is visible in fast-aging Latin America, where novel LTC systems are being established, for instance, in Uruguay and Costa Rica (Esquivel, 2017; Matus-López and Chaverri-Carvajal, 2022). Parallel to these national developments, LTC systems have recently also been debated at the global and regional level by international organisations 1 (IOs) such as the United Nations (UN) and the World Health Organization (WHO). Following global social policy research, IOs can be key actors in generating and translating ideas that can influence global discourse and initiatives as well as national (social) policy-making (Kaasch et al., 2019; Niemann et al., 2021). So far, however, little is known about the content of IOs’ ideas in the field of LTC and how they are linked to HC discourses, as the policy fields are not only institutionally connected but also share their orientation on service provision for people with physical or mental health care needs. To examine how different IOs address HC and LTC, and also to reveal possible differences in IOs’ approaches across policy fields, we address two main research questions: Do proposals clearly differ across organisations in each policy field, as previously shown, for instance, for discourses on pension policy (Deacon, 2015), or are their assessments rather similar? Do IOs’ principles and recommendations for LTC policy follow those in the more mature but closely-related area of HC policy?
Addressing these questions, this article compares the problems identified, the guiding principles and recommendations on HC and LTC systems in Latin America of two regional, UN-affiliated organisations which are relevant actors in both policy fields: the Economic Commission for Latin America and the Caribbean (ECLAC) and the Pan American Health Organization (PAHO). While ECLAC seems to be particularly involved in discussions on care systems, gender and women’s rights (Esquivel, 2017; Mahon, 2018), PAHO as a health organisation seems to be notably important in HC. Both IOs however publish on both fields and address their recommendations and ideas towards governments. The regional focus was selected because, first, IO engagement in HC has historically been very strong in Latin America (see, e.g. Weyland, 2006), and second, regional initiatives on (long-term) care have recently flourished. In contrast to the majority of previous studies focusing on international financial institutions (IFIs) such as the World Bank in HC reforms in the late 20th century, we analyse prescriptions published in the period 2000–2015 by ECLAC and PAHO as ‘idea-based organisations’ (Mahon, 2015: 5), which do not always attach hard conditionalities and financial incentives. With our dual and twofold comparison – ECLAC and PAHO, HC and LTC – we aim to contribute to a differentiated understanding of IOs’ social policy proposals, in particular with regard to novel policy fields such as LTC, where positions and ideas might not (yet) be polarised or consolidated.
The article is structured as follows: First, we theoretically address IOs’ role in social policy-making and introduce the two regional IOs under study more closely. The next section provides a brief background on HC and LTC as social policy fields, highlighting their interrelations. Third, we describe the process of data collection and analysis; fourth, we compare the main concepts, for example, targeting and universalism, presented by the two IOs for HC and LTC both within each policy field and across policy fields and analyse similarities and differences. We then discuss our findings in light of the literature on IOs as proposal actors, and finally, we address limitations of the study and suggest areas for further research.
IOs in social policy-making
Theoretical background: IOs as soft power proposal actors
While the adoption and implementation of welfare policies, including HC and LTC policies, mostly occur at (sub-)national level, the international and transnational arena can be important for shaping these policies too. One important type of ‘corporate actor’ (Coleman, 1990) in global social policy are IOs such as UN agencies or IFIs operating on a global or regional level (e.g. Deacon, 1997; Ervik et al., 2009). In the discipline of international relations (IRs), where the analysis of IOs is a major field, there has been extensive theoretical debate on the role and autonomy of such organisations vis-à-vis states/governments (see, e.g. Martin and Simmons, 2013). Generally, global social policy studies, in line with constructivist and liberal IR approaches, seem to regard IOs as meaningful actors with a certain degree of autonomy, while they also mostly acknowledge the importance of founding members and donors, that is, (powerful) states, in shaping IOs’ agendas and actions (Béland and Orenstein, 2013: 128; Deacon, 1997: 61; Kaasch et al., 2019: 5–6; Leisering, 2019: 109; Niemann et al., 2021: 11–12). This is also the theoretical stance we take here.
Scholars have identified various means and mechanisms by which IOs influence (national) social policy, some more forceful and binding than others. At times, and particularly in countries of the Global South, more direct policy interventions such as financial incentives (loans, aid) and conditionalities have been employed, one prominent example being the role of the World Bank in HC reform in the 1990s in Latin America (Almeida, 2006). However, this route for IO influence is constrained and contingent. Since IOs do not have formal veto power on domestic welfare policy, they lack hard governance mechanisms (Orenstein, 2008: 127; Schmitt, 2020: 8). Consequently, global social policy research has focused on analysing more subtle and ‘soft’ means of influence. Here, the creation and diffusion of ideas and norms, expertise and knowledge are key tools (see, e.g. Béland and Orenstein, 2013; Leisering, 2019; Niemann et al., 2021). In their seminal study on IO authority, Barnett and Finnemore (1999: 710–715) identify three ways by which IOs exert power (which have since been confirmed in empirical studies on social policy): first, via classification and categorisation, second, by (re-)defining the meaning of concepts, and third, by spreading these established ideas and norms. It is via such mechanisms that, as Orenstein (2008: 57) terms it, IOs act as ‘proposal actors’ who ‘formulate legitimate and well-elaborated policy proposals’ to convince domestic actors of their ‘problem definitions, norms and proposed solutions’.
Following the argument of Béland and Orenstein (2013), IOs’ positions and proposals are subject to change over time. But how and why do they develop, and why do they differ between IOs and policy fields? Generally, IOs can be shaped by multiple internal and external factors such as influential individuals and their (professional) biographies, bureaucratic culture, (formal) organisational structure and membership, external circumstances or events and their relationships with other actors (Barnett and Finnemore, 1999: 706; Deacon, 2015: 108; Vetterlein, 2015: 88–89). For instance, comparing the views on gender equality held by ECLAC and the OECD, Mahon (2018: 280–281) finds that the internal structure (positions held by feminists), the organisational paradigms (neo-structuralism vs neoliberalism) and the regional context in which the organisations operate (Global South vs North) account for differences between both IOs.
Importantly, there can also be differences within IOs, for instance, between different policy fields. Such variance can for example be linked to ‘distinct internal cultures’, as Barnett and Finnemore (1999: 724) posit:
Different segments of the organization may develop different ways of making sense of the world, experience different local environments, and receive different stimuli from outside; they may also be populated by different mixes of professions or shaped by different historical experiences.
However, internal variations are not the only possible reason for differences within IOs. Rather, as Vetterlein (2015: 90) argues, an IO’s position in relationship to other actors within the (policy) field ‘based on its expertise (or cultural capital) in the respective policy area’ shapes its response as well. The position is both dependent on the (past) behaviour and actions of the IO, as well as its recognition by other field actors (Vetterlein, 2015: 91). While Vetterlein applies the theory of field position to explain the degree of change of an organisation in two different crises, it is very well suited to account for the divergent proposals of one organisation in different policy areas, if it occupies different positions in both fields. Building on these theoretical considerations about the development of IOs’ positions, we aim to enhance the existing body of literature on IOs’ social policy proposals by unpacking differences and similarities in two related policy fields in two similar regional IOs. Crucially, this contributes to uncovering and reflecting intra-organisational differences.
The regional IOs under investigation: ECLAC and PAHO
In the growing scholarship on global social policy, heterogenous IOs have been the object of investigation in relation to various policies and regions of interest. Besides the usual suspects on the global level – such as the International Labour Organization or the World Bank – regional organisations which ‘make reference to territorial location and to geographical or normative contiguity’ (Börzel and Risse, 2016: 7) are less but increasingly studied (Bianculli and Ribeiro Hoffmann, 2016: 2; Yeates, 2019). Both, ECLAC and PAHO, are UN-affiliated, regional IOs. While PAHO’s mandate spans the whole American continent, ECLAC’s actions concentrate on Latin America and the Caribbean only. 2 Both organisations joined the UN system in the mid-20th century; ECLAC as a regional commission established by the Economic and Social Council in 1948 (ECLAC, n.d.-a), and PAHO – which had existed already since 1902 – as a regional office of the WHO (Meier and Ayala, 2014: 357–359). From their embedding within the UN system, we can expect that ECLAC and PAHO build on global policy discourses but with a focus on region-specific issues and solutions.
On the ‘continuum between task-specific and multi- or general-purpose’ (Börzel and Risse, 2016: 7–8), both organisations are somewhat task-specific, but PAHO with a much narrower focus than ECLAC. While ECLAC was founded ‘with the purpose of contributing to the economic development of Latin America (ECLAC, n.d.-a), its focus on social development only started in the 1990s (Mahon, 2015). Similarly, PAHO also broadened its focus within the field of health over time: Initially, the organisation had a strong disease and public health–centred approach, which was only complemented by a focus on HC systems and economics in the 1970s/1980s (Almeida, 2006: 134–141). In regards to networks and tools, ECLAC and PAHO can both be characterised as ‘idea-based’ organisations which employ mostly ‘soft’ governance mechanisms such as the compilation and distribution of information (Mahon, 2015: 6–7; PAHO, 2020: x). Consequently, despite emerging from different roots, today both organisations develop and disseminate proposals on HC and LTC system design in Latin America, making them fitting cases for comparison.
There is little previous research on either of the IO’s positions on social policies, including HC and LTC systems. In her analysis on the integration of ‘the social’ into ECLAC’s discourse, Mahon (2015) shows that in recent decades, the IO has shifted from the notion of ‘equity’ to embrace a rights-based, universalist conception of social protection’ (Mahon, 2015: 12). In parallel, ECLAC has also developed a focus on gender equality, including the position that not only childcare services but also ‘the provision of eldercare and support for those with disabilities [are] part of a gendered care economy’ (Mahon, 2018: 280). While there are several studies on PAHO, for instance, regarding the organisation’s historical development or management of epidemics (e.g. Meier and Ayala, 2014; Melo et al., 2020), research on its positions and involvement in HC (yet alone LTC) system design issues seems to be lacking. Before we turn to our empirical analysis, the next section provides a brief background on both social policy fields under study.
HC and LTC as social policy fields
HC and LTC are two service-based social policy fields dealing with the mitigation of and assistance in living with physical or mental impairments. As such, both fields are not only substantively but also institutionally closely connected. In fact, HC and LTC policies and systems are highly entangled in many countries, and the latter often builds on or develops out of pre-existing public HC provisions (Billings et al., 2013; Fischer, 2022). The affiliations between the areas is also visible at the international level, for instance, with WHO health reports incorporating chapters on HC and LTC systems (WHO, 2015). Despite this close relationship, the focus on providing continuous care and social support with daily living, as opposed to HC’s concentration on preventing and curing illness, has propelled LTC along the route to becoming a distinct social policy field next to the contentious and long-existing area of health policy. This development is increasingly evident in Latin America, both at the national (e.g. in Uruguay, Costa Rica) and regional (several UN organisations, ECLAC in particular) levels (see, e.g. Esquivel, 2017; Garay Villegas and Arroyo Rueda, 2022; Matus-López and Chaverri-Carvajal, 2022). It therefore seems worth studying whether and to what extent proposals on HC and LTC system design for the region differ, as they might also influence further LTC policies in the coming years.
In comparative research on HC and LTC systems, a three-dimensional approach has proven useful for describing the crucial elements of such systems (see, e.g. Fischer et al., 2022; Wendt et al., 2009). First, provision – that is the actual delivery of services – constitutes the basic function of any HC/LTC system. However, there is also a crucial difference between both fields in regards to provision: While, due to the necessary expert knowledge, HC is provided exclusively by trained professionals, for LTC, a ‘make or buy’ decision is possible (Rodrigues and Nies, 2013: 195). This means that informal care that is often provided by family members is a major source of LTC provision, making informal care givers an additional target group of LTC policies besides the persons in need of care themselves. Second, (monetary) resources need to flow into the system, constituting the dimension of financing. Third, the complex interaction between financing and provision structures and care recipients needs to be co-ordinated and governed – this is what the dimension of regulation refers to. The design of each of these dimensions has important implications, for instance, regarding equity, efficiency, affordability and (re)distribution. Crucial aspects to address when designing – or analysing – HC and LTC systems are therefore questions such as where and how care is provided (provision), who pays how much for care (financing) and how generous in terms of benefit scope and population coverage the system is (regulation) (see, e.g. De Carvalho et al., 2021; Jenson, 1997: 186; Toth, 2019). The latter issue is often addressed with the dichotomy of ‘universal’ – that is, applying ‘the same standards to all individuals’ – vs ‘targeted’, that is, the selection of certain (vulnerable) groups/persons, for example, based on care needs, economic means, gender or ethnicity (Carey and Crammond, 2017: 303).
As outlined earlier, IOs are engaging heavily in drafting and disseminating proposals on how welfare policies, including HC and LTC systems, should be designed. While research on IOs’ activities in LTC policy is to date largely absent (but see the work of Theobald and Kern, 2009), the influence of IOs on HC policy both globally and in Latin America specifically has been vastly documented. Especially during the 1980s and 1990s, the region acted as a ‘social laboratory’ (Mesa-Lago, 2008: 15) for HC reforms promoted by IOs, in particular, the World Bank and the Inter-American Development Bank (Almeida, 2015; Noy, 2017; Weyland, 2006). This has resulted in several seminal works analysing HC policy in light of a neoliberal framing, in which recommendations argued for a diminishing role of the state and increasing participation by the private sector and encouraged measures such as targeting, user fees and privatisation (Almeida, 2015; Mesa-Lago, 2008; Noy, 2017; Weyland, 2006). Although extant literature mostly focuses on the impact of IFIs on the HC reform wave seen in the last decades of the 20th century, recent research highlights the importance of the WHO and PAHO starting in the noughties, when principles of equity and access were encouraged in view of the Millennium Development Goals (MDGs) and the primary care framework (Almeida et al., 2018; Giovanella and Faria, 2015; Giraldo Osorio and Vélez Álvarez, 2013). While these studies mention some of PAHO’s ideas on HC systems, there is still a lack of a systematic analysis on its proposals. This shortfall is also evident in the case of other non-financial IOs, such as ECLAC. Thus, while our analysis of IOs’ proposals on LTC and the comparative focus are most innovative, we also hope to contribute to broadening the perspective on IOs in HC policy.
Data collection and analysis
In order to analyse similarities and differences in the IOs’ proposals, we collected reports and strategy articles published by ECLAC and PAHO between 2000 and 2015 in English and Spanish. This period was selected because at the beginning of 2000, the UN published seminal international agreements that have had a substantial impact on both fields. The MDGs had an enormous impact on health and, accordingly, HC systems in Latin America (Evans et al., 2005; Torres and Mújica, 2004). In the case of LTC, the UN’s Madrid International Plan of Action on Ageing (MIPAA) in 2002 put the topic of ageing and LTC on the international agenda and initiated successive regional meetings and political frameworks, among others, in Latin America (Garay Villegas and Arroyo Rueda, 2022; Montes-de-Oca et al., 2018). To achieve a relatively stable period of observation, which is not affected by huge changes in the discourse, the period of observation ends in 2015. We assume that certain changes at international and regional levels could have affected the regional discussions after 2015, as this was the year the UN revised the MDGs and introduced the Sustainable Development Goals (SDGs) at the international level, and on the regional level, it was the first time a national LTC system was introduced in Uruguay (Esquivel, 2017; Matus-López and Cid Pedraza, 2016).
After a three-step phase of document selection and collection, we conducted an eight-step qualitative analysis. The steps follow the procedure outlined by Altheide (2000) and Bowen (2009). The data collection and analysis processes are displayed and detailed in the following sections (Figure 1).
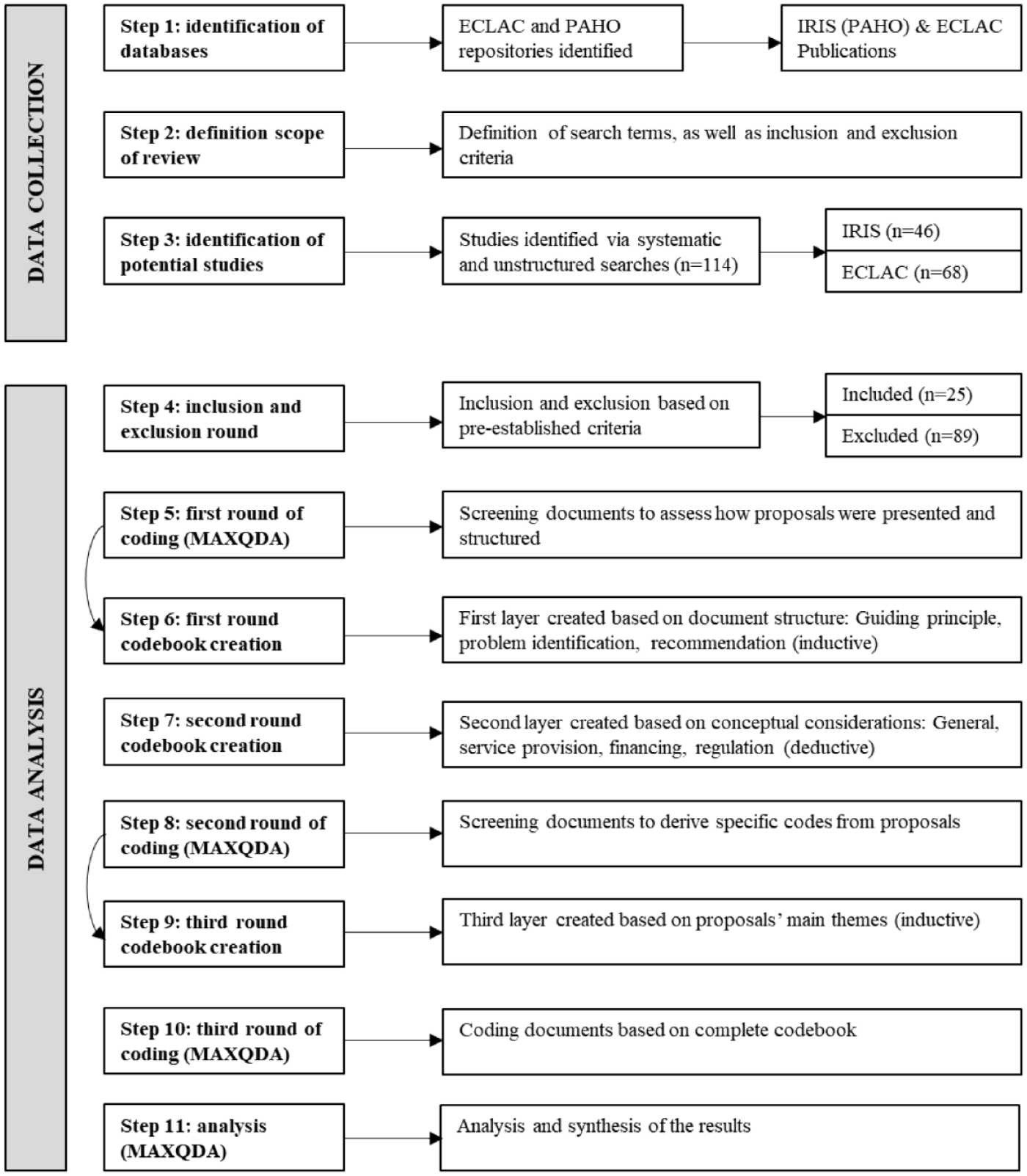
Flow diagram of data collection and analysis processes.
To identify the relevant documents, we performed searches between February and July 2022 in the publicly available databases of each IO. 3 Systematic and unstructured searches were conducted to locate both indexed and non-indexed documents. We also reviewed articles mentioned in the reference lists of the reports identified through systematic searches. Our initial screening retrieved 114 documents, 56 pertaining to the field of HC and 58 addressing LTC. The documents selected for analysis meet five pre-established criteria: They (a) are authored by the IOs or by experts affiliated with the institutions and extend beyond mere resolutions or political agreements between member states; (b) are free from disclaimers indicating that the document does not (necessarily) represent the views of the IO; (c) specifically address the topics of LTC or HC, rather than just general social policies; (d) offer explicit or implicit recommendations on HC or LTC, rather than simply identifying best practices or conducting country analyses and (e) were published within our designated observation period.
The data analysis consisted of eight steps as displayed in Figure 1. After excluding documents not adhering to these criteria, 12 publications related to HC and 13 to LTC were analysed. 4 The processes of coding and codebook creation were iterative. The first round of coding the reports revealed a similar structure that the IOs use in their publications. They first identify current problems within the field. Then, the IOs suggest how these issues could be addressed by setting overarching aims, or guiding principles, that should steer policies at the highest level of abstraction; for instance, the right to HC or LTC. These are often presented in the introduction and first paragraphs of the documents. Subsequently, IOs recommend specific instruments, techniques or settings to achieve these guiding principles and solve the identified problems, that is, establishing a minimum basket of benefits available to the whole population. Therefore, the first layer of our coding scheme refers to the general structure of the IOs’ proposals for countries: Problem identification, guiding principles and specific recommendations.
Adopting a deductive approach, we subsequently created a secondary layer encompassing the three functional dimensions of HC and LTC systems – provision, financing and regulation. However, these dimensions bear no relevance to guiding principles. This is due to the fact that guiding principles do not exclusively refer to any system characteristic but represent general policy objectives. A second coding round was conducted to inductively identify specific codes. This exercise gave rise to the third layer of the coding scheme, which incorporates 101 distinct codes. For instance, ECLAC states that ‘one very common problem, both in the countries of the region and elsewhere, is that of rising health system costs’ (D6: 28). In this case, the specific code related to problem identification and financing was created: Costs LTC/HC, which refers to the high costs associated with the provision of health services. Table 1 presents a simplified version of the codebook. 5
Simplified codebook.
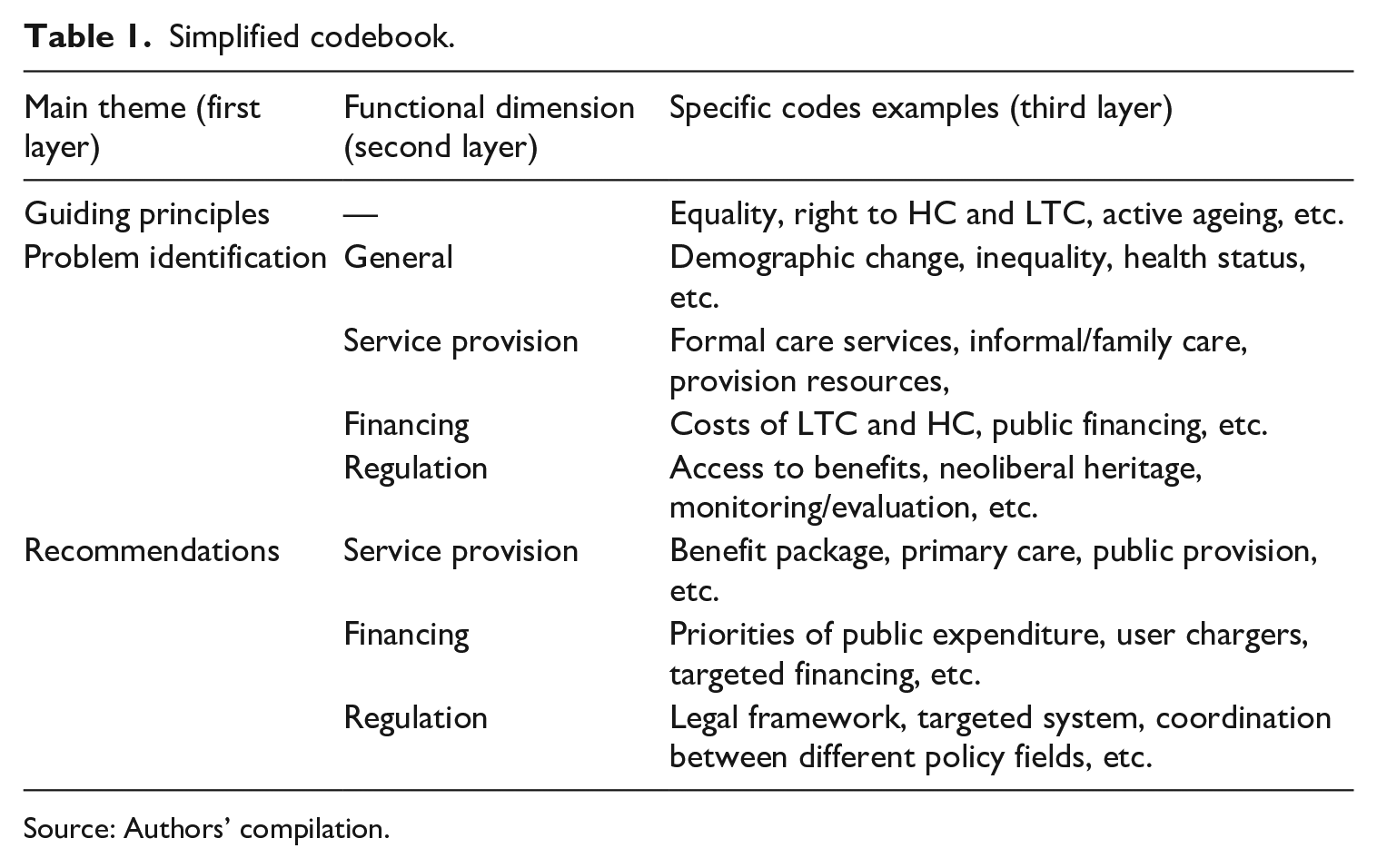
Source: Authors’ compilation.
After constructing the codebook, the IOs’ documents were annotated according to the pre-determined codes. The text analysis software MAXQDA was used for coding and examining the content of the reports; more specifically, the software served for data preparation (i.e. organising and compiling the documents), data coding (i.e. code system management, merging and transforming codes, linking documents and codes, coding the data), data analysis and visualisation (i.e. information retrieval, summary tables and frequencies), as well as data storage. Altogether, 1114 text segments were manually and systematically coded by the authors. The subsequent section presents and synthesises the main results of the analysis. 6
ECLAC’S and PAHO’S proposals for HC and LTC systems
In the following analysis, we delve into the most frequently recurring and striking similarities and differences between the HC and LTC proposals made by ECLAC and PAHO. These comparisons are drawn within the context of their guiding principles, their identification of problems and their recommendations for resolving these.
Proposals for HC policy
With regard to proposals for HC policy, both ECLAC and PAHO aligned on the need for regulatory oversight, service provision and financing reforms to safeguard the right to HC. However, there are distinct divergences in their stance on certain issues, such as the extent of public sector responsibility and especially regarding coverage and financing aspects. The following subsections describe and compare the IOs’ proposals.
Guiding principles
With regard to the principles that should guide policy recommendations, issues related to equality were heavily discussed by both IOs. However, the range of social problems they associated with equality differed. While PAHO positioned equality in a broader context, justifying it as a matter of ‘social justice’ for the whole population (D18:12), ECLAC mostly focused on ethnic equality aimed at indigenous and black peoples (D8; D12; D14). Both IOs also suggested principles of gender equality but to a much lesser extent (D4; D18). Universalism was the main guiding principle for PAHO: ‘universal coverage and access are the root of healthcare systems’ (D18: 25, own translation). The necessity of expanding coverage is also mentioned by ECLAC in two documents (D4; D6), but the organisation emphasised the burden of universalism on expenditure and demand: ‘the imperative to move towards universal HC provision is a factor that is undoubtedly adding to the pressures on demand and expenditure in the sector’ (D6: 23). Issues related to intersectionality (health as cross-cutting policy fields) and integrality (the need to develop policies/systems that provide all the necessary services across the whole life cycle) were emphasised by both organisations (D4; D5; D9; D12; D17; D18; D24). Moreover, the organisations analysed recognised HC as a human right (D18; D24) and asserted that it should be a priority for governments (D4; D18; D24).
Problem identification and recommendations
In discussing specific problems and solutions for HC, the IOs mainly agreed on topics related to regulation and service provision aspects of systems, thereby favouring the right to health(care) and primary care. Substantial differences were observed in financing: Unsurprisingly, ECLAC’s ideas were rooted in economic principles, with some recommendations based on neoliberal, pro-market doctrines widely disseminated during the 1980s and 1990s (Mesa-Lago, 2008), of which PAHO was critical.
The main regulatory themes that ECLAC and PAHO addressed were access to the system, state involvement and the role of the public sector as well as coordination. According to the IOs examined, the main challenges faced by HC systems in the region were not only the low levels of general access but also availability of specific services, as well as a lack of state involvement (D4; D5; D9; D17; D18; D24). The organisations saw these as consequences of segmentation 7 and the neoliberal reforms of the 1980s and 1990s. In addition, these pro-market reforms 8 created or deepened biases towards targeted policies and decreased state involvement, which aggravated the already existing coverage challenges (D18).
In order to address these challenges, recommendations varied from universal to targeted logics. Both IOs argued for the need to facilitate access for the whole population, as health is considered a human right. PAHO, for instance, suggested that emphasis must be placed on universal coverage to remove economic barriers to access (D18). Although both IOs suggested some degree of targeting, ECLAC’s rationale differed from PAHO’s. While the latter suggested targeting as a first step to achieving universal coverage, ECLAC argued for ‘distributive equity’, in which the distribution of resources should not be ‘egalitarian between individuals or groups, but of differential allocation according to the particular requirements of those groups and individuals’ (D4: 66, own translation). The IOs also identified societal groups that should be prioritised, such as women, the elderly, the disabled, indigenous and black populations (D9; D12; D14; D18) and the poor (D4; D17). Interestingly, all reports published by ECLAC after 2006 specifically addressed special health needs of marginalised communities – for example, indigenous adolescents and young adults (D12) and indigenous and black mothers and children (D9).
Recommendations specifically for the public sector were also found across the documents. Greater state involvement in all aspects of the system, such as financing, developing public health programmes or controlling mechanisms were presented (D4; D14; D17; D18). According to ECLAC (D4: 48, own translation), ‘the state must continue to be hegemonic in normative, political, monitoring and controlling aspects’ of the HC system. Moreover, PAHO and ECLAC suggested that states should strengthen the legal framework of the systems to develop oversight mechanisms, increase the efficiency of the public sector to obtain best results with minimum resources and improve HC for marginalised populations. ECLAC published the vast majority of the recommendations on public sector efficiency, and they revolved around cost reduction, resource allocation and management (D4; D6).
Another important aspect raised by the IOs was the issue of coordination between policy fields (D4; D12; D14; D18) and government levels, namely local, regional and national. With regard to the latter, ECLAC pushed for the decentralisation of systems (D4; D6), while PAHO recommended a better integration between government levels (D14; D17; D18). Even though PAHO briefly mentioned the importance of active participation by communities (D18), they suggested that states should be the most important actor in HC. In contrast, ECLAC placed greater emphasis on community involvement, highlighting its role in designing, monitoring and implementing public health policies (D4; D9; D12; D14).
In sum, both IOs agreed in the main regulatory challenges Latin American HC systems face, with an emphasis on low levels of access and availability of services and state involvement. However, the IOs offered different solutions to the issues in terms of coordination (decentralisation vs integration), community involvement (participation vs government oversight) and coverage logic (universalism vs distributive equity).
In terms of service provision, the need to create and define a minimum-benefit package was raised by both organisations. For instance, ECLAC highlighted the necessity of setting criteria to determine the services that need to be covered by health schemes (D6). Even though the IOs agree that each country should decide which services should be included in the minimum-benefit package, it is possible to observe a clear focus on services/treatments related to primary care, prevention and health promotion and for marginalised groups. Moreover, the organisations recommended that governments should prioritise public provision. However, ECLAC suggested that ‘some mixture of private and public provision of services could serve the developing countries of Latin America best’ (D5: 43). In addition to focusing on the services previously mentioned, the IOs prescribed that public delivery must target the provision of essential drugs and treatments that address the epidemiological challenges of each nation and population group (D4; D9; D14; D17; D18). Therefore, we do not observe major differences between the IOs regarding service provision, except for ECLAC’s encouragement of private provision.
In general, the IOs did not discuss financing issues to the same extent as service provision and regulatory matters. The main financing topics discussed by the IOs revolved around the role of the state in funding the system (ECLAC and PAHO), as well as cost-saving measures (ECLAC). To address reduced public funding and the high levels of private financing, in particular, out-of-pocket payments, the IOs advocated for greater state involvement, however, to different degrees. PAHO clearly affirmed that governments should be the main actor responsible for financing HC systems, stating that ‘improving [the HC sector] seems to require the continued political commitment at the national level, including the necessary foresight to ensure that financing meets the needs of the entire population’ (D18: 31, own translation). Contrarily, ECLAC claimed that identifying priorities for state financing, such as targeting specific groups (D4), would combat the inefficient and unequal allocation of public spending.
The high cost of HC seems to be one of ECLAC’s main concerns, and the organisation recommended six measures to tackle the issue: decreasing costs through better allocation of resources and reducing costs in service provision (D4; D6); expanding universal compulsory insurance systems as they ‘can also generate incentives for cost savings through the articulation of public and private providers’ (D6: 29); adopting user fees such as co-payments and minimum charges to save costs 9 ; prioritising in public expenditure to marginalised groups, that is, black and indigenous peoples, considering their specific health needs (D9; D12; D14); increasing competition (D6); finally, ECLAC actively encouraged targeted financing, allocating and prioritising public resources according to needs and economic capacity (D4).
Proposals for LTC policy
Policies on LTC were still under development throughout Latin America in the observed period. Therefore, when comparing general principles, identified problems and recommendations, PAHO’s and ECLAC’s overall approaches were relatively broad, with an emphasis on regulation and service provision.
Guiding principles
The active ageing approach as a guiding principle was emphasised by both organisations (D1, D2, D3, D19, D21). This approach focuses on prevention and keeping older people active as long as possible. However, they had different perspectives on LTC and the way it should be addressed. While PAHO focused on the person in need of care, ECLAC concentrated far more on the needs of informal caregivers, with an emphasis on gender equality and unpaid female care work. Another difference is that, in general, ECLAC had a broader understanding of ‘care’. In their documents, childcare and eldercare were often discussed in the same vein, whereas PAHO discussed care in the context of ageing and care for the elderly. Comparing the guiding principles, ECLAC stressed ‘gender [. . .] equality’ (D10: 207) and ‘co-responsibility’ (D15: 222) – meaning the better distribution of care-related work between men and women – as their main guiding principles, while PAHO focused mainly on ‘active ageing’ and the ‘centrality of the older person’ (D16: 9). These concepts reflect the organisations’ understanding of LTC policies because they underline, in the case of ECLAC, the link between public care policies and informal (female) care work, whereas PAHO argues for LTC policies as an instrument to help older people in need. What is also remarkable is that ECLAC highlighted ‘universality’ and ‘solidarity’ (e.g. D10: 41), while PAHO rarely mentioned these themes. These principles underline ECLAC’s concept of a system that is directed towards the whole population, without prioritising specific social groups, and that is based on solidarity between generations.
Problem identification and recommendations
These differences in the general principles are then also reflected in some of the recommendations on regulation: ECLAC recommended establishing universal systems directed at the whole population, while PAHO argued for targeting services to specific groups. Specifically, PAHO proposed targeting the most vulnerable groups such as poor, uninsured, frail and severely disabled people or people living in rural areas (D21: 2, D25: 6). Targeting people in poverty was criticised by ECLAC, as the organisation stressed the need to address all groups in need, especially middle-income groups, and not only to focus on the poor, as otherwise the costs for care could push these better-off households into poverty (D15: 226). Also, ECLAC was concerned that targeting would rather reinforce inequalities between men and women:
Historically, the State’s role in care provision has not been universal in its focus, but rather has targeted population groups with specific characteristics. The rationale of the support provided through public schemes has tended to assume that caregivers, particularly women, are in the home and have time available. (D10: 216)
Another difference between the organisations regarding the general regulation of the system was that PAHO discussed LTC as part of the HC system, while ECLAC recommended to ‘set up national care systems with public institutions that are capable of integrating care policies and services’ (D15: 44).
Apart from these very striking differences between PAHO and ECLAC, there were also some common recommendations in the regulation dimension, such as the need to establish legal frameworks, improving coordination between policy fields and recommendations on quality and monitoring. The recommendations on legal instruments focused, on the one hand, on the need to establish strategies and legal frameworks that protect the rights of older people (D1, D8, D10, D13, D19, D21, D25). On the other hand, there were more specific recommendations on certain topics related to LTC such as laws regulating the working conditions of domestic care workers and providing them with basic social security rights such as pensions (D15). PAHO and ECLAC also frequently addressed the need to improve coordination between policy fields, as a lack of coordination between the health and social care systems in particular would lead to fragmented coverage of services and thus affect care provision (D7, D15, D25). Moreover, they both also stressed the importance of improving quality and monitoring instruments in LTC (D1, D8, D15, D16, D21, D25).
In financing, the main differences between the two IOs were, firstly ECLAC’s recommendation to finance universal LTC systems preferably through taxes (D15), while PAHO seemed not so clear on a specific financing mechanism; secondly, ECLAC recommended creating distinct LTC systems that are financially independent from other systems such as HC:
In Latin America and the Caribbean, however, the social protection systems for pensions and health are so unequal and have proven so hard to reform that funding for long-term care should not be aligned with existing social security schemes. (D15: 226)
Nevertheless, both IOs addressed the need to allocate sufficient public funds to LTC and even more importantly to consider LTC in the state’s general budget. In response to possible concerns about high expenditure for LTC, the IOs also mentioned the costs that result from not having public care policies. This issue was raised by PAHO:
Can we afford the cost of eldercare in the face of so many other public health priorities? The costs of eldercare should be considered in relation to the cost of prevention versus the cost of treatment and long-term care, and in relation to the cost of mismanagement of primary healthcare. (D16: 14)
ECLAC criticised the high use of private co-payments and the resulting inequalities due to the lack of a system for LTC, as people who are poor or do not have access to services have to find other solutions for care, that is, informal care, which reinforces inequalities as it leads to a loss of income in already poor households (D8: 89).
Regarding provision, both IOs drew attention to changing family structures and informal care provision as main challenges countries should address, but with different emphases (D1; D2; D7; D10; D15; D21; D25). ECLAC, on the one hand, was concerned that persisting gender inequalities associated with informal caregiving might be reinforced as the ageing population increases the demand for (informal) care in the region (D10). PAHO, on the other hand, was rather worried that the supply of informal care (due to changing family structures and ageing populations) might not be sufficient, leading to an ‘increasing demand on social protection systems, and the health system in particular’ (D 25: 2). To strengthen care supply, PAHO argued for offering better services to support formal and informal caregivers (D16; D 25).
One element that was central in both IOs’ documents was community care. The importance of ‘ageing in place’ (D8: 129, own translation) was described as an essential objective to improve availability and access to services and to support informal caregivers. Community care, as proposed by the IOs, comprises the full range of local services, including prevention, primary care and rehabilitation (D1, D16). According to ECLAC and PAHO, social services, such as help with shopping, washing or cleaning, could be provided through different stakeholders within the community comprising a wide range of non-governmental and voluntary agencies or associations (D8, D15, D16). However, the responsibility for developing and coordinating these networks and stakeholders should fall to the state, as its task should be ‘the creation, promotion or consolidation of informal protection mechanisms developed by families and communities to enable people to age in place and feel integrated into the community’ (D8: 125, own translation).
The participation of families was discussed as a crucial element in these community settings, due to the predominance of informal care by family members in Latin America. Consequently, both IOs recommended establishing support services to improve the situation of these caregivers (e.g. D3, D25). These support services should encompass the provision of not only social and HC services for the elderly but also services directed towards the specific needs of caregivers, such as training or mental-health and social support programmes and services (D2, D3, D10, D15, D16, D25).
Summing up, the two IOs differed in particular in their general view on LTC and the main stakeholders, with ECLAC having a stronger focus on informal caregivers and gender inequalities, while PAHO primarily considered the elderly and their (health) needs. The main differences in the recommendations were related to regulation and financing, where ECLAC preferred universal coverage, financed through tax-based systems, and PAHO recommended targeting specific groups with LTC services. However, both organisations agreed that LTC must be equipped with better legal frameworks, that policies should focus on community-based care, and that government accountability should be increased and funding improved.
The IOs’ positioning across policy fields
Comparing ECLAC’s and PAHO’s prescriptions on HC and LTC, they both emphasised a rights-based approach, underlining the state’s responsibility for securing and enforcing their citizens’ rights to HC and LTC, which could be achieved by adopting legal frameworks. They also had similar ideas in more specific recommendations, such as improving access to services or prevention measures. Nevertheless, there were also some differences in the general principles and the recommendations in the two fields.
Comparing ECLAC’s proposals in HC and LTC, equality was mentioned in both fields but with different target directions. While they stressed economic equality in HC, gender equality was addressed as one of the main guiding principles in its documents on LTC. In HC, the focus was on inequalities in access to HC services due to economic status, while in LTC, ECLAC was much more concerned with gender inequalities related to female caregiving. Moreover, one of the most surprising differences within the IO’s proposals is the importance of universalism in LTC in contrast to HC. While, in HC, ECLAC still seemed to follow more neoliberal principles, recommending targeting the poor and user fees, the organisation seemed to follow a different path in LTC, where it was critical of targeting the poor and advocated for universal systems that cover all people in need, independent of their income, preferably financed by taxes. Also, we could observe differences in the recommendations related to governance. In HC, the IO recommended decentralisation, whereas in LTC, probably due to the lack of general policies in the field, decentralisation was not discussed. Here, the recommendations focused more on coordination between policy fields, especially between HC and social services.
Comparing PAHO’s recommendations and principles in the two policy fields, the contrast was not as great as that in ECLAC’s case. However, the striking difference was again on the topic of universalism, as the IO argued for a universal system in HC, while it addressed the need to target specific groups such as the poor in LTC. Also, PAHO emphasised universalism as a guiding principle in HC while it remained silent on this topic in LTC. In other recommendations, there seem to be more common ideas on the policy fields, such as the need for coordination between providers and government levels, improving access or preventive measures. Table 2 summarises these differences between the organisations and policy fields.
Similarities and differences between the IOs and policy fields.
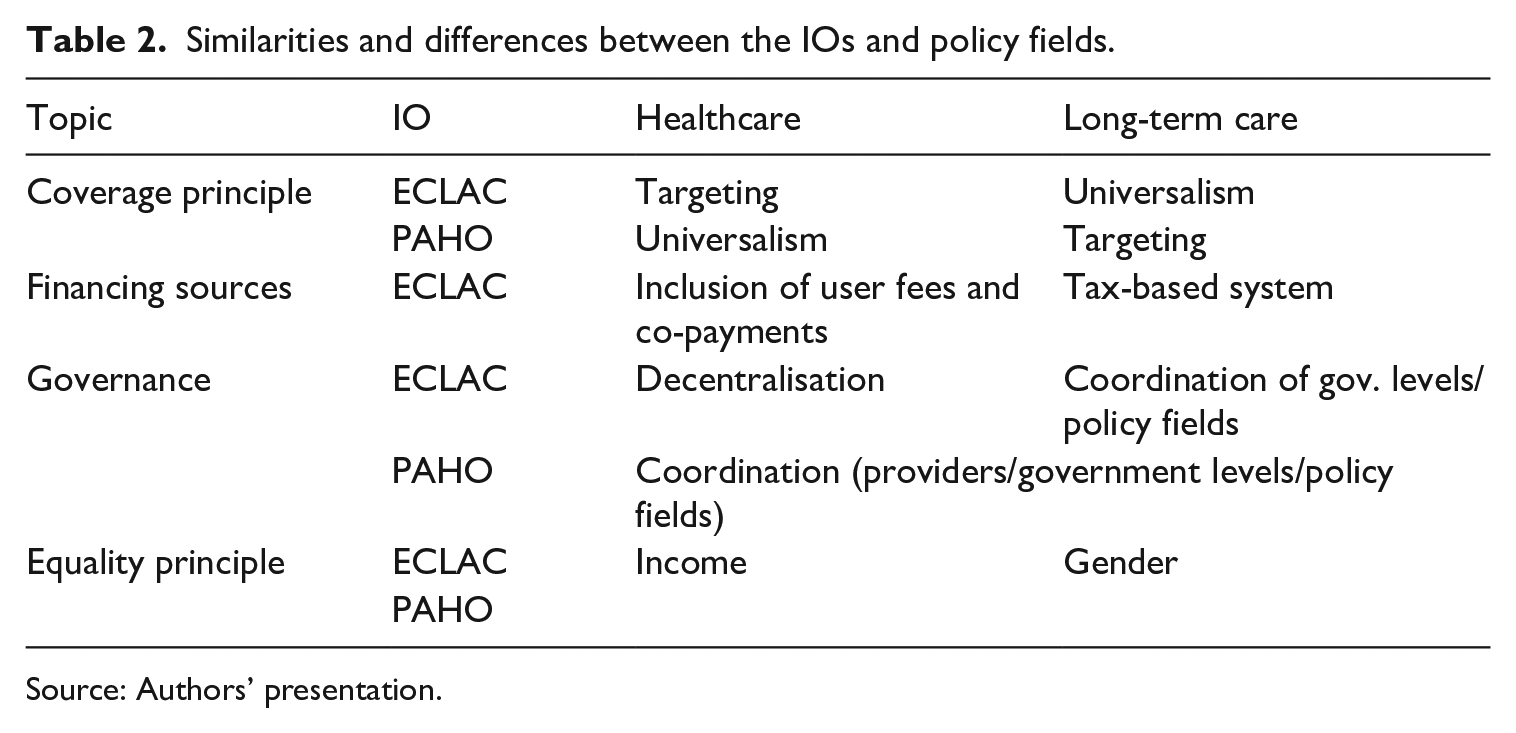
Source: Authors’ presentation.
Discussion
Our analysis revealed some similarities, but also differences both within and between the IOs as well as across policy fields, which were especially noticeable in ECLAC. The differing perspectives on HC and LTC within one and same organisation are all the more surprising given that the majority of the analysed documents were published by the Latin American and Caribbean Demographic Centre (CELADE) – the Population Division of ECLAC. This finding seems contrary to our initial assumption that ‘distinct internal cultures’ (Barnett and Finnemore, 1999: 724) across divisions may be behind shaping different proposals in both policy fields. However, a closer look at the ECLAC staff who co-ordinated the analysed publications reveals that in most documents, different staff members were responsible for each policy field. This could indicate that different staff members might develop distinct internal cultures even within a division. Linking this observation to our empirical findings, this seems to corroborate what has been mentioned in the literature, namely that the (professional) background of staff can play an important role in shaping the agendas of IOs (Barnett and Finnemore, 1999; Mahon, 2018).
Furthermore, ECLAC’s position in the respective policy fields might account for the observed differences (Vetterlein, 2015). While Vetterlein analysed change over time within one organisation, finding that IOs’ policy responses depend on other actors in the field as well as on past behaviours and interactions, our study indicates that differences at the same time within one organisation in different policy fields could also be dependent on field-specific positions of actors and historical developments. ECLAC’s diverging recommendations on HC and LTC could therefore be due to (ideological) heritages in health policy. IOs have a long tradition of championing proposals for HC, as it is one of the pioneer branches of the modern welfare state. During the 1980s and 1990s, neoliberal principles were predominantly advocated within the field, especially by actors with economic/financing expertise such as the World Bank and the Inter-American Development Bank. This may have hindered an abrupt and progressive shift towards more inclusive recommendations, such as universalism, as more recent recommendations still inherit aspects of previous periods. In LTC, there are no such dominant IOs that have shaped the discourse either in the past or in current years, nor did ECLAC define the policy field previously. ECLAC’s position in LTC can thus be characterised by a certain autonomy, without external influences or a previous ideological heritage from other major international players. This also opens up the possibility for other actors and disciplines, such as feminist and gender research, to contribute to the agenda, which seems to be the case with the IO’s focus on gender equality (Mahon, 2015, 2018). The emphasis on gender equality may also be explained by the particularities of LTC, as the role of female informal care is a crucial element in LTC provision, in contrast to formal, professionalised provision structures in HC systems. Similarly, the different recommendations on the financing mechanism, where ECLAC promoted – especially in the earlier documents – user fees and co-payments in HC, while co-payments were criticised in LTC, could be due to certain field-related particularities: Generally, HC systems are more cost-intensive for states, leading to the need to control costs, while LTC is (currently) characterised by informal care provision and a lack of public policies and, hence, lower expenditures. Consequently, the organisation might not focus on cost-sharing for LTC systems as this does not seem urgent with current arrangements.
In the case of PAHO, different perspectives on the two fields are not as prominent in its recommendations, which could be explained by our observation that the organisation mainly perceived LTC as part of the HC system rather than a distinct policy field, whereas in its documents from 2010 onwards, ECLAC clearly argued for the creation of ‘a new pillar of social protection’ for LTC (D10: 211). These differences regarding the framing of LTC can be related to the different foci of the IOs, with PAHO being an IO specialised in HC, while ECLAC is leaning towards a multi-purpose organisation. Consequently, PAHO’s recommendations on LTC were thus closely linked to HC, which also explains to some extent the differences we observed in the recommendations on targeting, as the organisation identifies older people, and particularly vulnerable groups among them, as a specific group requiring special attention, but within a universal HC system.
While the differences between PAHO and ECLAC in their recommendations on LTC may be explained by their general view on LTC as either a distinct field of social policy with its own logic or as a subfield within HC, the differences between PAHO and ECLAC in HC are more puzzling, as the latter seemed to follow more closely the narrative of past discourses, while PAHO had a progressive approach. One possible explanation could be that as a health organisation, PAHO has a stronger position in the policy field and was therefore also more open to new perspectives and ideas, while previous debates drawing on neoliberal ideas were more internalised in the HC discourse at ECLAC. Moreover, past experiences not only from HC but also from other policy areas in which the organisation was heavily involved, such as pensions – which were grounded in neoliberal principles during the Washington Consensus era – may have continued to inform HC discourses in a kind of path-dependent trajectory. Interestingly, in LTC, these principles did not shape the discourse strongly. One potential explanation for this difference could be that the policy field only emerged in the early 2000s, ‘freeing’ it somewhat from the ideological heritage of past debates.
Conclusion
This article aimed to answer the question to what extent proposals for LTC and HC policies differ between and within ECLAC and PAHO. As shown earlier, there are clear differences not only between the two organisations and how they position themselves in each policy field but also within the same organisation. This is particularly evident in ECLAC, which stands out as the main agenda-setter in care policies in Latin America in the analysed period. While the proposals in the health sector seem to be shaped by past debates and also other international players in the region, the IO’s discourse on LTC is currently in the process of unfolding and establishing its own agenda. In the case of PAHO, it can be seen that the policy fields are not so clearly separated, as LTC is understood as a part of HC. These interrelations between the policy fields show that even on the level of IOs, the question on how to organise LTC in relation to HC is not uniform and that addressing LTC as a policy field in its own right is still a fairly recent phenomenon.
This article therefore contributes not only to a better understanding of IOs’ positionings in different policy fields but also to how their ideas and proposals in HC and LTC evolve vis-à-vis each other and how actors and field dependencies add to these differences and interrelations. This is particularly relevant as IOs’ proposals could influence how countries in the region approach care when introducing or reforming respective policies in the future. For instance, the strong focus of ECLAC’s regional discourse on gender inequalities in LTC could lead countries to underestimate other potential access barriers such as income, which have been shown to be important in HC systems, when designing novel LTC systems.
However, this study is not without limitations. First, the choice of the two policy areas brings its own challenges, as they both have different preconditions in terms of their historical traditions and general developments at the country level, which makes comparison challenging. And second, by focusing on IOs relevant to both policy fields, we excluded other actors that could potentially play a more central role in policy debates for HC or LTC, such as the World Bank (HC) and UN Women (LTC).
Our analysis offers new research avenues. First, as this article only examines the positioning of IOs, it is necessary to investigate whether and how these ideas are reflected in and translated into policy-making at the country level as well as in what way developments in countries shaped the international and regional discourse, such as the ‘pink tide’ 10 or the commodities boom in the early 2000s. Second, it could be interesting to shift the perspective from the discourse of regional UN organisations within Latin America to other types of IOs – regional (UN) agencies in other parts of the world, organisations at the global level such as central UN bodies or regional integration organisations such as MERCOSUR (Southern Common Market) or the European Union.
Supplemental Material
sj-docx-1-gsp-10.1177_14680181241254087 – Supplemental material for New agendas and old legacies? Comparing international organisations’ proposals on health and long-term care systems in Latin America
Supplemental material, sj-docx-1-gsp-10.1177_14680181241254087 for New agendas and old legacies? Comparing international organisations’ proposals on health and long-term care systems in Latin America by Meika Sternkopf, Gabriela de Carvalho and Johanna Fischer in Global Social Policy
Supplemental Material
sj-docx-2-gsp-10.1177_14680181241254087 – Supplemental material for New agendas and old legacies? Comparing international organisations’ proposals on health and long-term care systems in Latin America
Supplemental material, sj-docx-2-gsp-10.1177_14680181241254087 for New agendas and old legacies? Comparing international organisations’ proposals on health and long-term care systems in Latin America by Meika Sternkopf, Gabriela de Carvalho and Johanna Fischer in Global Social Policy
Supplemental Material
sj-docx-3-gsp-10.1177_14680181241254087 – Supplemental material for New agendas and old legacies? Comparing international organisations’ proposals on health and long-term care systems in Latin America
Supplemental material, sj-docx-3-gsp-10.1177_14680181241254087 for New agendas and old legacies? Comparing international organisations’ proposals on health and long-term care systems in Latin America by Meika Sternkopf, Gabriela de Carvalho and Johanna Fischer in Global Social Policy
Footnotes
Acknowledgements
We would like to thank Heinz Rothgang, Simone Leiber and the participants in the doctoral colloquia held by the University of Bremen for their comments on early versions of this research, and Max Henke for editorial support.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article is a product of the research conducted in the Collaborative Research Centre 1342 “Global Dynamics of Social Policy” at the University of Bremen. The centre is funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation)—project number 374666841—SFB 1342.
Supplemental material
Supplemental material for this article is available online.
Notes
Author biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.