
Abstract
The importance of mutual learning between providers and recipients of development assistance has been emphasised for decades. Nevertheless, its practical implementation remains limited, primarily due to organisational issues and unequal power relations in development aid. Using the ‘design-thinking’ approach, this study demonstrates the possibility of mutual learning utilising the example of the Swiss Red Cross and the Village Health Committees in the Kyrgyz Republic. Based on the related project documentation and interviews with relevant partners, this article provides an insight into the factors enabling mutual learning in practice. It suggests that decentralisation of the organisation, its leadership and response to failures, continuous contact between provider and recipient of development assistance, and emphasis on local expertise contribute to learning. Although context-specific, these findings are essential to understanding the mutual learning in general and taking this phenomenon from theory to practice.
Keywords
Introduction
International aid-providers have aspired towards community participation in development programmes or community-driven development (cf., for example, Bamberger, 1986; Binswanger-Mkhize et al., 2010; The Global Fund to Fight AIDS, Tuberculosis and Malaria, 2014), highlighting a mutual learning process between the two (or more) partners (Buchert, 1998: 353–354). Although emphasised ‘in the post-2015 agenda’ (Organisation for Economic Co-operation and Development [OECD], n.d.), mutual learning remains ‘ad hoc’ rather than ‘systematic’ (Buchert, 1998: 361), mainly because of the hierarchy between the actors. A recent study on ‘partnership’ between donor and non-governmental organisations in the Pacific highlights power imbalances between actors (Moloney, 2019: 9). Despite the emphasis on ‘ownership’, placing the beneficiary ‘in the driver’s seat’ (Ellerman et al., 2001: 175–176) and attempts over the last 20 years to make the assistance ‘more participatory’, aid-recipients have remained ‘program takers’ rather than ‘program makers’ (Flint and Meyer zu Natrup, 2019: 211). Putting the donors’ aspirations and rhetoric into practice, however, requires acknowledging the differences between the actors and changing their ‘power relationships’ (Kontinen, 2018: 28, 34–35). Focusing on ‘transformative development’, the United Nations’ Sustainable Development Goals 1 ask for ‘specific kinds of learning’ (Kontinen, 2018: 29–30) with the rationale for the mutual learning being ‘more powerful than ever’ (Constantine and Shankland, 2017: 117).
Thus, this study focuses on mutual learning between providers and recipients of development aid using the example of the Swiss Red Cross (SRC) and the Village Health Committees (VHCs) established through the Community Action for Health (CAH) project in the Kyrgyz Republic.
The CAH (2001–2017), formerly known as the Kyrgyz-Swiss Health Reform Support Project and Kyrgyz-Swiss-Swedish Health Project (Schüth et al., 2014: 7), was implemented by the SRC. It was financed by a number of international organisations (IOs), including the Swedish International Development Cooperation Agency (Sida) and the United States Agency for International Development (USAID), but the main one being the Swiss Agency for Development and Cooperation (SDC). The overall budget of the project for 17 years amounted to CHF24.5 million (around €21.7 million; Gotsadze and Murzalieva, 2017: vi). CAH had two objectives: to ‘enable rural communities to act on their own for the improvement of their health’ and support the state healthcare system ‘to work in partnership with communities for improving health’ (Schüth, n.d.: no page number). In other words, the project aimed to promote community participation and collaboration between the state healthcare system and local communities. For this reason, it established the VHCs.
VHCs are community-based organisations composed of volunteers, mostly local residents. Depending on the size of the village, organisations have around 5–10 members (Interviewee A, 18 July 2016, personal communication, Bishkek: para. 7; Interviewee E, 22 January 2018, personal communication, northern province: para. 37–38; Kickbusch, 2003: 18). The VHCs help identifying healthcare problems in their villages and implement the relevant solutions. Its members are community volunteers who conduct awareness-raising and health promotion activities throughout the project and beyond it. One interviewee who worked closely with the VHCs suggested that, of the original 1612 organisations, around 70–80% were still working (Interviewee H, 30 January 2018, personal communication, Bishkek: para. 125–138). Thus, despite the project ending, the majority of the VHCs continued their existence, echoing similar findings in other countries (cf. Glenton et al., 2010).
The CAH targeted rural areas of the country because of the problems with access to healthcare and poverty. The initial study conducted within the project showed unequal access to healthcare among the rural population. Although the local health facility was the first point of contact for most, poor households went to the local traditional healer due to affordability concerns (Schüth, 2000: 7). The Government initiated the Manas (1996–2006), Manas Taalimi (2006–2010) and Den Sooluk (2012–2018) programmes to reform the healthcare system, strengthen primary healthcare (PHC) and ensure its accessibility to the population. An interviewed community representative noted that the CAH commenced at a time of extreme impoverishment after independence (Interviewee E, 22 January 2018, personal communication, northern province: para. 6). It is difficult to obtain the data for early years or ensure its comparability, but according to estimates in 1999, the poverty rate reached its zenith, with 55.3% of the population living below the poverty line (UNDP and ILO, 2008: 25). Poverty gradually decreased thereafter but remained an issue, particularly in rural areas. In 2019, about 20% of the population, or 1,313,000 persons, lived below the national poverty line, 2 and 73.8% of them resided in rural areas (National Statistical Committee of the Kyrgyz Republic, 2020: 1).
The participation of individuals and communities in the health system complies with the World Health Organization’s (WHO) Alma-Ata Declaration (1978) 3 and the Ottawa Charter for Health Promotion (1986). 4 While the Alma-Ata Declaration viewed participation as a ‘right’ and ‘duty’, the Ottawa Charter went further by suggesting supportive actions, such as access to information, learning and funding. Both documents called for greater individual and community involvement in PHC and health promotion. Accordingly, community participation materialised in various forms in different settings. In some countries, such as Peru, Zimbabwe, Kenya and Burundi, it took the form of health committees, monitoring health facilities, participating in their administration, evaluating community needs, etc. (cf., for example, Falisse et al., 2012; McCoy et al., 2012). In this way, the committees contribute to accountability of healthcare providers to the population and serve as a link between the two. In other cases, for instance in the Philippines, communities were involved in decision-making processes through representation in local health boards, serving alongside state and healthcare officials (Ramiro et al., 2001). Furthermore, community involvement also resulted in extending the outreach of the state healthcare system. For example, multiple community organisations in Cuba participate in awareness-raising, health situation analysis and health promotion activities (Greene, 2003). In India, community members take part in Village Health Sanitation and Nutrition Committees planning sanitation improvements, organising health promotion activities and supporting villagers’ access to healthcare by arranging transportation to hospitals (Kumar and Mishra, 2016). Overall, there is no single scenario or template for community participation.
At the same time, the multiplicity of engagement forms makes evaluating the impact of community participation in practice difficult. A systematic review of relevant studies indicates problems with operationalising the participation and linkage between community involvement and health outcomes (Rifkin, 2014). Yet, some authors stress the relevance of this participation by pointing out that the lack of evidence does not invalidate its impact on outcomes (Haldane et al., 2019; Preston et al., 2010: 14). Other studies emphasise the positive role of community engagement in maternal and new-born health (Marston et al., 2013), healthy living, prevention and treatment of some parasitic diseases (Haldane et al., 2019), fighting malaria (Atkinson et al., 2011: 30), among others.
The concept of community participation is rather new to the Kyrgyz Republic. The country, similar to other countries in the post-Soviet region, inherited the hierarchical Semashko healthcare system in which the state was responsible for financing, regulating and providing healthcare services. After the collapse of the Soviet Union, the Kyrgyz Republic implemented a number of reforms to optimise and decentralise the healthcare system (Isabekova, 2019a). The establishment of VHCs represents one form of decentralisation of healthcare services. As local institutions at the village level, the VHCs plan and implement activities to address broader issues pressing to the local population (Smith, 1997: 402–403). In this way, community participation is seen ‘as part of wider community development programs’ rather than engagement ‘in health services alone’ (Rifkin, 2009: 33). This also complies with the WHO emphasis on social determinants of health, including, but not limited to the healthcare system. 5
This study explores the learning between aid-providers and recipients using the example of the SRC and VHC members. The section on methods is followed by the analytical framework, which integrates the concept of mutual learning into the ‘design thinking’ (Flint and Meyer zu Natrup, 2019) approach. By doing so, this study aims to benefit from practical applicability of the ‘design-thinking’ and theoretical strength of the mutual learning concepts. The analysis is followed by discussion of results and concluding remarks. Although context-specific, the issues highlighted in this study, namely the hierarchy among stakeholders and their knowledge, are relevant beyond the selected case. Therefore, the analytical framework used in this study can serve as guidance for development policies and assistance incorporating local communities into the process and moving beyond the traditional ‘top-down’ approach.
Methods
This study is based on project-related documents, academic literature and nine semi-structured interviews with development partners, state organisations and the VHCs conducted by the author between 2016 and 2018 in Russian, English and Kyrgyz. 6 The interviews took place in the capital Bishkek and two other provinces in the north of the Kyrgyz Republic. Accessibility of the interviewees and the author’s personal networks were the primary reasons for selecting the north. Other provinces were not included mainly due to feasibility concerns. The interviews were analysed by the author using the MaxQDA software following descriptive content analysis (Kuckartz, 2014). According to this approach, questions of the semi-structured interviews are used to make an initial categorisation of the material, followed by more detailed content-driven analysis and categorisation based on the material itself. This approach ensures accuracy and comprehensiveness of the interview analysis. At the same time, the analysis has some limitations. Based on accessible information, the analysis certainly represents part of, but not the whole picture. Although the interviewed development partners and state organisations worked with and were aware of the VHCs in the entire country, this study does not aim to generalise the interviewees’ experiences but rather explores the mutual learning between the SRC and selected VHCs.
Analytical framework
This study operationalises (mutual) learning as a continuous process of action and reflection by relevant actors based on the knowledge received by them. For clarity purposes, it explains the mutual learning by specifying ‘who learns, what and to what effect’ (Bennett and Howlett, 1992: 278).
First, who learns? Kontinen (2018) distinguishes various levels on which learning occurs, whereby this study focuses on organisations as learning entities. Organisations in this study are ‘constellations of people, material artefacts and structures gathered together to do something’ (Kontinen, 2018: 36). In other words, these are people representing ‘donor’ and ‘recipient’ of assistance in a specific area at a given period of time. Donor–recipient affiliation simplifies ‘a considerably more complex reality’ (Carlsson and Wohlgemuth, 2000: 8), and yet, it is important for understanding the factors relevant to mutual learning.
In their approach to knowledge, organisations can be separated into two types. ‘Action’ organisations use knowledge ‘instrumentally’ to improve ‘quality of their outputs’ and achieve ‘the relevant social impacts’, as these organisations acquire legitimacy based on their ‘output, or societal impact’ (Boswell, 2009: 13, 47). In contrast, ‘political’ organisations approach knowledge in a ‘symbolic’ manner, since their legitimacy is based on ‘formal structures and decisions, rather than social impact of their policies’ (Boswell, 2009: 13, 48). In practice, organisations combine both types (Boswell, 2009: 48), but this distinction is useful to differentiate their attitude to knowledge. Overall, organisations engaged in development assistance are ‘slow’ learners (Berg, 2000: 26–29) because of structural issues and donor-recipient relations.
The structural factors preventing organisations from learning include division of labour, reliance on ‘conventional wisdom’ (Edgren, 2000: 43–46) and routine, ‘budgetary pressure’ (Suzuki, 2000: 100), fragmentation and quality of information (Carlsson and Wohlgemuth, 2000: 9), and compliance with pre-defined agenda (a ‘blueprint approach’) (Berg, 2000: 35; Flint and Meyer zu Natrup, 2019: 214–215). Staff composition and turnover, incentives, organisational goals and leadership are also relevant (Berg, 2000: 34–35; Cheng, 2000: 140; Edgren, 2000: 48–50; Kontinen, 2018: 39–40; Salem et al., 2018: 603). Notably, decentralisation of an organisation contributes to mutual learning (Constantine and Shankland, 2017: 103). Decentralisation increases authority of the ‘field’ offices and their responsiveness to ‘what is happening on the ground’. Another relevant factor is organisational response to failures, varying between denial, acknowledgement with attribution to external factors and treating ‘error’ as an opportunity to improve compliance with beneficiaries’ interests (Korten, 1980: 498). The first two options are more likely to take place in practice. Project failure is often attributed to ‘a mistake in the local culture’, instead of not ‘understanding’ this culture (Cheng, 2000: 140). Organisational staff is discouraged from acknowledging problems. If project ‘mistakes’ represent the ‘lessons learnt’, administrative failures are taken ‘more seriously’ and employees do not admit the issues ‘unless they have to’ (Suzuki, 2000: 95). All these structural factors may discourage or facilitate organisational learning.
Furthermore, relations between aid-providers and recipients are relevant to learning. As a ‘two-way process’ (Constantine and Shankland, 2017: 116), mutual learning highlights multiplicity of sources in exchanging knowledge and expertise (Buchert, 1998: 353). Continuous contact between aid-providers and recipients is essential. If a programme aims to fight poverty, learning presumes living among ‘poor’ people, and yet, practitioners in development organisations tend to spend more time in the capital (Eyben, 2005: 104). Mutual learning requires spending more time with those who ultimately receive the aid. Understanding the local culture is more than ‘identifying a few indicators’ or making ‘blitzkrieg’ visits to project beneficiaries (Cheng, 2000: 139–140). In addition to continuous contact, mutual learning requires its acknowledgement by both aid-providers and recipients. As ‘trainers’, but not ‘learners’, the staff of IOs sees no ‘need for learning’ or identifying ‘themselves as learners’ (Suzuki, 2000: 100). Yet, an ‘expert’ as a ‘saviour’ may have no contextual awareness (Flint and Meyer zu Natrup, 2019: 208–209) or knowledge about beneficiaries’ most pressing issues, or the most fitting solutions to them. The mutual learning for aid-provider demands ‘unlearning the expertise’, ‘truly’ listening (Eyben, 2006: 50) and ‘learning how to learn’ (Cheng, 2000: 132–133). For the aid-recipient, this means expressing their ideas, concerns and solutions, which might be challenging given potential capacity issues and the aid-dependence on the recipient side, aid-uncertainty and the inflexibility of aid programmes on the donor side (Isabekova, 2019b).
Second, learning is defined in relation to knowledge the actors received or ‘what’ is learnt. This study defines knowledge as the expertise held by actors without further geographic (‘local’ vs ‘international’) or content-related (‘specific’ vs ‘abstract’) categorisation. Knowledge is an ambiguous term (Bar-On, 2015: 781), understood as an instrument to achieve goals, response to external factors, ‘lesson-drawing’, etc. (Bennett and Howlett, 1992: 276–277). Knowledge is often discussed in relation to its origin contrasting ‘indigenous’ or ‘local’ with ‘Western’, ‘scientific’ or ‘international’ knowledge (Bar-On, 2015: 781). However, despite the presumable difference in abstraction and analytical strength, ‘indigenous’ and ‘Western’ knowledge are similar (see Agrawal, 1995), as knowledge can be ‘useful or useless [. . .] socially relevant or irrelevant [. . .] without reference to whether it is indigenous or scientific’ (Agrawal, 2009: 157).
Nevertheless, the distinction between the ‘local’ and the ‘international’ is critical to understanding the hierarchy in development assistance. External actors have access to financial resources and expertise; they adapt ‘international principles’ to local realities and ‘define ownership as theirs to give to national or local actors’ (Sending, 2015: 67–69). As donors bring money, beneficiaries do not object ‘even if the project is doomed to fail’ (Cheng, 2000: 140). Inequality between the actors contributes to the hierarchy of their knowledge. ‘Indigenous’ knowledge is ‘rarely seen as an equal’ to the ‘Western’ kind (Briggs, 2013: 235–236). Local expertise is ‘subordinate’ to international, and it is primarily used to implement the ‘international standards’ (Sending, 2015: 55, 65). This hierarchy is also reflected in the acknowledgement of ‘local’ knowledge by international actors. ‘Recognition’ and ‘misrecognition’ are key to authority (Sending, 2015: 12) of ‘international’ knowledge over the ‘local’, as it diminishes (Briggs, 2013: 235) and challenges (Bar-On, 2015: 781) the latter. Recognition authorises external actors to not just ‘instruct [,] but also construct the categories’ (Sending, 2015: 132) the local actors comply with. Overall, subordination to external actors and their knowledge highlights fundamental hierarchies between the actors engaged in development assistance and their knowledge.
Third, learning is closely associated with action. As a continuous and dynamic process (Suzuki, 2000: 97), learning is ‘more than assimilation of information and knowledge’ (Pasteur, 2004: 12) and is commonly associated with change (Grin and Loeber, 2007: 205–210; Kontinen, 2018: 39; Pasteur, 2004: 9; Suzuki, 2000: 88). As argued by Carlsson and Wohlgemuth (2000: 8–9), ‘It is not enough to identify a problem and propose a solution. The solution must be put into practice before learning can occur’ (pp. 8–9). Suzuki (2000) goes even further with the assertion ‘no action, no learning’ (p. 100). Notably, action includes reflection on the knowledge received. Learning implies, ‘achieving new understanding and insight’ (Pasteur, 2004: 12, 17). In development assistance, this implies questioning inherent inequalities; thus, Kontinen (2018) distinguishes various ranges of learning useful to understanding the actors’ reflection. She distinguishes among ‘quite stereotyped responses’ to information without any reflection (‘zero learning’), choices driven by effectiveness (‘conformative’), ‘reflection on organizational values, assumptions and goals’ (‘reformative’) and questioning/changing the ‘alternatives from which the choice is made’ (‘transformative’) (Kontinen, 2018: 23–26). Therefore, reflexivity may vary between reaction, outcome improvement, rethinking organisational goals, questioning both organisational objectives and possible solutions.
This article uses ‘design-thinking’ (Flint and Meyer zu Natrup, 2019) to analyse mutual learning in practice. Driven by process, rather than outcome, this approach ‘embraces uncertainty’ with aid-providers acknowledging incompleteness of their knowledge, as aid-beneficiaries are the ones who know their needs (Flint and Meyer zu Natrup, 2019: 212). The authors suggest that this approach recommended itself in information technology (IT) and engineering, but the ‘end-user’ of aid remains largely excluded from designing development programmes (Flint and Meyer zu Natrup, 2019: 212–213). Although joint planning and engagement of multiple actors is not new (cf. Korten, 1980; Suzuki, 2000), the ‘design-thinking’ addresses inequalities between the actors by ensuring non-dominance of aid-providers in agenda setting (Flint and Meyer zu Natrup, 2019: 217) and stressing engagement of aid-beneficiaries throughout the development assistance. By doing so, it overcomes the hierarchies between the actors and their knowledge, and provides the environment for mutual learning to take place in practice.
As a repetitive process, ‘design-thinking’ is composed of multiple stages, including problem identification, developing potential solutions, testing them and implementing the final solution. Issues and solutions are defined by people affected by them; aid-providers establish the ‘platform’ for discussions and have rather supportive and ‘facilitating’ functions (Flint and Meyer zu Natrup, 2019: 212–216). Potential solutions are evaluated through ‘testing’ and ‘prototyping’. Testing aims to create scientific conditions and involves larger sample sizes (Flint and Meyer zu Natrup, 2019: 216). Notably, ‘failure’ is seen as an indispensable part of the process, contributing to actors’ knowledge, experience and trust (Flint and Meyer zu Natrup, 2019: 215).
This article integrates mutual learning into the ‘design-thinking’ approach by elaborating on who learns, what they learn and what effect this learning has at the problem identification, developing solutions and implementation stages. The two approaches are complementary. ‘Design-thinking’ provides the necessary environment for mutual learning to take place and allows us to follow the learning process throughout the development project. Incorporation of mutual learning into ‘design-thinking’ in turn enriches the original framework by elaborating on the types of actors and knowledge involved, thus linking the framework to the broader literature on learning.
‘Design-thinking’ in the CAH
While design-thinking commences with ‘problem identification’ and ‘developing potential solutions’, the CAH targeted the problems defined by communities. The SRC and the Health Promotion Units (HPUs) conducted a round 3000 Participatory Reflection and Action (PRA) sessions per 100,000 population to identify community issues, covering about 70–80% of households (Interviewee B, 8 December 2017, personal communication, Skype: para. 60). In addition to enabling the communities to act on their own, the CAH intended to support the partnership between communities and the state healthcare system. Therefore, problem identification, developing, testing and implementing potential solutions engaged the local PHC and HPU representatives, who worked closely with the VHCs. Specifically established by the Ministry of Health (MoH) to support the VHCs as part of the PHC initiative (Schüth, 2009: 10), HPUs received extensive training from the SRC and largely complied with its approach to the PRA and work with local communities. For this reason, this study focuses on the SRC as the main actor providing training and support to the VHCs. Formerly known as the Participatory Rural Appraisal, the PRA developed in the early 1990s and it encompasses ‘a growing family of approaches and methods to enable local (rural or urban) people to express, enhance, share and analyse their knowledge of life and conditions, to plan and to act’ (Chambers, 1994: 1253). The PRA sessions followed the principles of ‘non-dominance’ and ‘non-interference’ by facilitating the discussion without influencing it:
[. . .] it is only possible with non-dominant behaviour, because otherwise people, you know, usually view outsiders as more educated, richer, more powerful than themselves, and so they, you know, they tend to be quiet. (Interviewee B, 8 December 2017, personal communication, Skype: para. 133)
In addition, the SRC trained the staff of the local PHC facilities on the principles of ‘non-dominance’ and ‘non-interference’ in order to facilitate the PRA sessions (Interviewee F, 22 January 2018, personal communication, northern province: para. 153). Both PHC workers and the project team conducted discussions ‘without judging’ people’s responses as ‘right or wrong’ (Schüth, 2011: 23–24). The PRA meant to provide the ‘space’ for community members to express themselves; the facilitators showed ‘respect’, ‘seriousness’, interest and learning (Interviewee B, 8 December 2017, personal communication, Skype: para. 133), driven by the assumption that the project team should learn from local people, as they know best (Schüth, 2011: 23–24). The participants were grateful and surprised, and came away with the ‘feeling that they were listened to’ (Schüth et al., 2014: 28):
[. . .] if you come in to local community with a dominant attitude, people [. . .] shut up, agree, and sit and finally, go away, listen because they are nice to you, but not [because they are truly interested]. [. . .] how do you give space when you meet local communities? You shut up and listen, you do not talk, you let them talk, you ask, you listen, you show your respect and seriousness by being interested in what they are saying, by inquiring more, by showing people that you are learning something from them – then it is their space and you are participating in it. And they can come up with that they do, come up and show their knowledge, show their capacity, and then you are in a working relationship, where both sides can contribute to a common goal. (Interviewee B, 8 December 2017, personal communication, Skype: para. 133)
The PRA sessions not only aimed to identify the issues, but also generate the solutions. Community members brainstormed about pressing diseases and how to stay healthy (Interviewee B, 8 December 2017, personal communication, Skype: para. 60). Facilitators compared these lists of ideas to the Alma-Ata Declaration: similarities of the list to the declaration, developed by international experts, ‘encouraged’ the community members (Schüth, 2011: 32). To take action in relation to identified issues, the PRA participants nominated community members to the VHC. The selected members surveyed the local population by asking about their problems and priorities:
Around 10 [VHC] members visited each house and asked for 10 priorities. These were, for instance, iodine deficiency, iron deficiency, hypertension, alcoholism and others, and they decided themselves what should be prioritised. (Interviewee A, 18 July 2016, personal communication, Bishkek: para. 7)
7
The list of pressing issues by local communities in Batken oblast in the south of the Kyrgyz Republic in 2007 for instance, contained among others high blood pressure, anaemia, goitre, influenza, joint diseases, brucellosis and alcoholism. Determinants of health or the conditions to stay healthy in the same oblast included clean water, access to healthcare, improved sanitation, nutrition and others (Schüth, 2009: 7). Similar surveys were conducted in other regions of the country.
Furthermore, the VHCs took action to address the issues identified in the surveys. This corresponds to another stage of the ‘design-thinking’, namely ‘testing’ and implementing the solutions. The Kyrgyz Republic was among the countries with the highest level of human brucellosis in mid 2000s, mainly due to low population awareness of preventive measures. As the disease is largely related to lambing, most cases occurred among men aged 13–35 (Schüth et al., 2014: 7–8, 17). To address this problem, the VHCs conducted outreach campaigns on preventive measures and available treatment (Schüth et al., 2014: 8) by providing brochures to each household (Schüth, 2005: no page number). Similarly, to combat goitre, the VHCs informed local population about the need to consume iodised salt, provided test kits to local retailers and periodically checked salt samples in local shops (Schüth et al., 2014: 23–24). These activities prevented local retailers from selling counterfeit ‘iodised’ salt:
The label says, ‘iodised salt’, but in fact it is not, [it is] technical [salt]. Then people became educated, applied these [tests], [and saw the indicator did] not change: ‘ah, it is a technical salt, we will not buy it’, and all [local] entrepreneurs started selling 100% iodised salt. (Interviewee A, 18 July 2016, personal communication, Bishkek: para. 7)
Likewise, the VHCs conducted activities against hypertension. High-blood pressure ranked third among the risk factors contributing to death and disability in 2017 in the Kyrgyz Republic (Institute for Health Metrics and Evaluation, 2019). Low awareness contributed to the problem: only one-third of the affected population was aware of their high-blood pressure, and less than 3% received treatment for it. During the World Heart Day in September, the VHCs throughout the country screened ‘as many adults’ as they could. The VHCs explained the risks of hypertension, provided brochures to persons with high-blood pressure and compiled a list with their names and addresses, and passed these lists to the local family group practice or feldsher-midwife points (Schüth et al., 2014: 11).
Overall, according to external assessments, the VHCs’ activities contributed to increased awareness of hypertension (WHO, Regional Office for Europe, n.d.: n.p.) and decreasing instances of brucellosis (Schüth et al., 2014: 10), goitre (Schüth, 2009: 30), mortality from cardiovascular diseases (Gotsadze and Murzalieva, 2017: 15) and other health issues in the Kyrgyz Republic. Although cardiovascular diseases remain an issue in the country, the VHC activities increased the awareness of hypertension among the population ‘to a remarkable degree in a relatively short time’ (WHO, Regional Office for Europe, n.d.: n.p.).
The SRC provided technical support, including training and equipment. The VHCs received training on how to organise seminars for their awareness-raising campaigns (Interviewee C, 13 January 2018, personal communication, northern province: para. 9; Interviewee F, 22 January 2018, personal communication, northern province: para. 23) and how to measure blood pressure and test for iodine in salt. The SRC provided blood pressure monitors, kits to test iodine in salt, gloves, vegetable seeds (to increase vegetable consumption) and other relevant supplies. The SRC also supported the VHCs’ organisational capacity by providing office hardware and outreach materials, training VHC members in bookkeeping and budgeting, and writing appeals to local self-governance (LSG) institutions (Interviewee F, 22 January 2018, personal communication, northern province: para. 49–50, 69, 155–162, 189) among others. It should, however, be noted that the VHCs encountered challenges during implementation, such as misunderstanding and resistance from the local population (Interviewee C, 13 January 2018, personal communication, northern province: para. 28–29; Interviewee F, 22 January 2018, personal communication, northern province: para. 124) and LSGs (Interviewee F, 22 January 2018, personal communication, northern province; Interviewee D, 19 January 2018, personal communication, Bishkek: para. 25). There were cases of people throwing away the information materials provided by the VHCs (Interviewee C, 13 January 2018, personal communication, northern province: para. 28–29) or disrupting the seminars:
When we mentioned the toilet bowl, [people] said ‘are you going to build us a toilet?’ And then we said that the toilet needs a pipe, as we have learnt, that it should be this way and to not attract flies, it should be closed, and that it needs to have a hand washer. Some chased us away, disrupting the seminar, [saying]: ‘What toilet can we build? We are barely making ends meet’. (Interviewee F, 22 January 2018, personal communication, northern province: para. 119)
There were misunderstandings with the LSGs as well (Interviewee H, 30 January 2018, personal communication, Bishkek: para. 112), although the initial attitude gradually shifted towards gratitude from the local population (Interviewee F, 22 January 2018, personal communication, northern province: para. 124) and close engagement with the LSGs (Interviewee C, 13 January 2018, personal communication, northern province: para. 9; Interviewee F, 22 January 2018, personal communication, northern province: para. 73, 79–80). The interviewees pointed out the voluntary work of the VHCs (Interviewee F, 22 January 2018, personal communication, northern province: para. 82, 141) and their motivation (Interviewee D, 19 January 2018, personal communication, Bishkek: para. 9) as factors contributing to this change. In addition, this study highlights the broad character of the work conducted by the VHCs.
The VHC activities were not limited to healthcare problems in a narrow sense. The poorest female-headed households received a sack of potatoes, 10 hens, a rooster and training on how to keep chickens, with the VHCs helping build hen houses (Interviewee F, 22 January 2018, personal communication, northern province: para. 6–8; Schüth et al., 2014: 25). The Swiss provided small grants to support the VHC initiatives in solving community issues. These grants were used to build public baths (Interviewee E, 22 January 2018, personal communication, northern province: para. 4; Interviewee G, 22 January 2018, personal communication, northern province: para. 1–3), purchase recreational equipment for schools (Interviewee C, 13 January 2018, personal communication, northern province: para. 9), build sewing shops, etc. In Lahol village of Naryn Oblast, for instance, water pipes were repaired using one of these small grants utilising local labour, thereby solving the problem of access to water, which had persisted for 20 years (Interviewee A, 18 July 2016, personal communication, Bishkek: para. 7). The VHCs conducted a number of social activities to support vulnerable groups, including fundraising activities for a villager in need of medical intervention (Interviewee C, 13 January 2018, personal communication, northern province: para. 35), support for war veterans (Interviewee F, 22 January 2018, personal communication, northern province, Kyrgyzstan: para. 17–22) and children from poor households, covering transportation costs to hospitals for the poor, etc. (Interviewee D, 19 January 2018, personal communication, Bishkek: para. 25). With the technical and financial support from the SRC, the VHCs tackled broader social and economic issues faced by their communities, which also contributed to their legitimacy.
Notably, the solutions mentioned earlier were ‘tested’ by stakeholders before and during the implementation:
[. . .] [the SRC] would hand it [the idea] to the village health committee; to one or two or three [committees], [. . .] find out what they say [. . .], even try it out in a workshop also, and then get feedback from them, find out how does it work and get adjusted [. . .]. (Interviewee B, 8 December 2017, personal communication, Skype: para. 50)
In addition, there was continuous evaluation of the VHCs by their members and the Health Promotion Units (HPUs) working with them. Evaluation took place on an annual basis, based on the criteria the SRC had developed using Labonte and Laverack’s (2001) community capacity-building framework. It emphasised participation, leadership, organisational structure, resource mobilisation and other areas (Labonte and Laverack, 2001: 117), adapted into 15–17 indicators (Interviewee B, 8 December 2017, personal communication, Skype: para. 117–118). These indicators included questions on number of staff, gender composition, presence of relevant documentation, budgeting, etc. (Interviewee H, 30 January 2018, personal communication, Bishkek: para. 123–124, 163–167). VHC members also filled in ‘happiness’ and ‘workload’ indices. The evaluation results of both the VHCs and the HPUs were found to be similar (Interviewee B, 8 December 2017, personal communication, Skype: para. 119).
Overall, the CAH followed the ‘design-thinking’ framework by choosing to ‘embrace uncertainty’ over pre-defined agendas (Flint and Meyer zu Natrup, 2019: 212). Certainly, the project aimed to promote community participation in healthcare and facilitate interaction between communities and state institutions. This agenda complied with the Alma-Ata (1978) and Ottawa (1986) 8 declarations, as well as with the principles of the SDC (financing) and SRC (implementing). The stated aim of the SDC is to ‘strengthen the voice and role of communities and civil society’ by supporting ‘community-based health services’ and initiatives ‘targeting and involving the poor and most vulnerable groups in society’ (SDC, 2003: n.p.). Similarly, the SRC stresses ‘development from below’ and supports ‘grass-roots organizations’ working on awareness raising among the population (SRC, 2006: 6). Thus, both organisations supported civil society and community-based organisations in promoting their interests and needs in health systems. Yet, this agenda was broad and open to interpretation at the local level, with communities identifying their concerns and suggesting their solutions. Despite the presence of organisational objectives, the project was process, rather than outcome-driven, as these objectives were open to interpretation on the ground.
Mutual learning
How does mutual learning take place in the ‘design-thinking’ framework? To understand this, this study elaborates on who learned, what they learned and the action related to it. The SRC, in collaboration with the HPUs, organised PRA sessions and facilitated discussions following the principles of ‘non-interference’ and ‘non-dominance’. Community representatives, for their part, brainstormed about pressing issues and health determinants. They also surveyed the local population and compiled lists of community concerns and priorities. Knowledge transfer in defining community problems and solutions engaged both actors, as illustrated below in Figure 1.
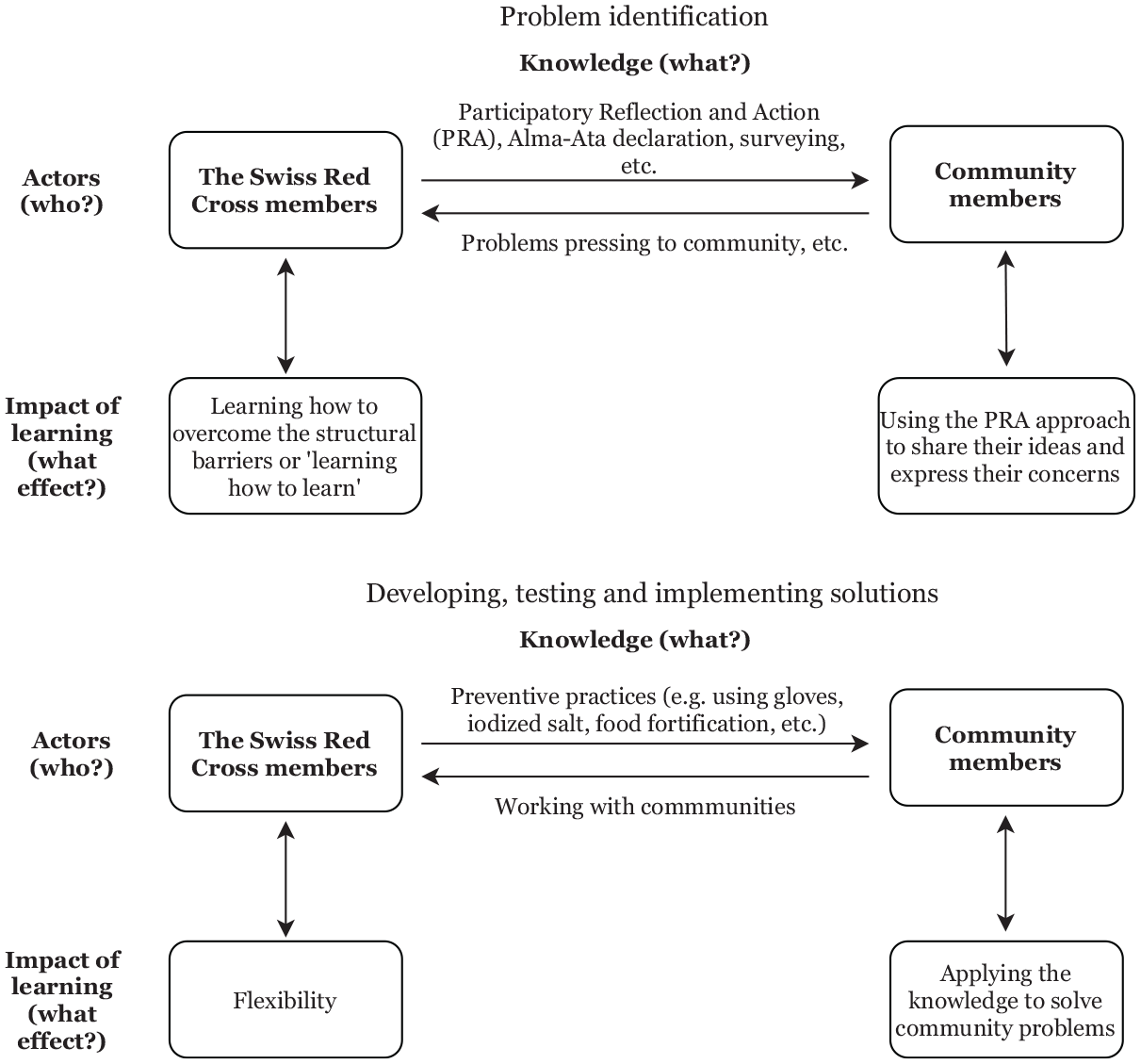
Mutual learning between the SRC and VHCs in ‘design-thinking’.
Yet, mutual learning implies action or change based on knowledge. What kind of actions did the actors take based on the knowledge they received? ‘Surprised’ by the interest in their opinion (see Schüth et al., 2014: 28), community members used the PRA to share their ideas and express their concerns. Similarly, they used knowledge about surveying to identify and prioritise community issues and solutions. The SRC in turn learned to work with local communities, most importantly to overcome structural hierarchies and accept community knowledge without judgement. Learning in the case of the SRC was not related to action, but reflection or ‘learning how to learn’ (Cheng, 2000: 132–133), ‘truly’ listening and ‘unlearning expertise’ (Eyben, 2006: 50). This indicates changes in the hierarchy between the actors and their knowledge of development assistance. Interestingly, the PRA facilitators used the Alma-Ata Declaration to highlight the similarities between the declaration and priorities identified by community members. This supports the hierarchy between the ‘local’ and ‘international’ knowledge, and the authority of the latter in setting the standards for ‘local’ knowledge to comply with (Sending, 2015: 12, 132). This comparison could have also been used to demonstrate the validity of community choices to the project funders by highlighting their similarity to the ‘international’ knowledge level. Yet, in this particular case, the comparison was used to empower community members unaccustomed to being heard by representatives of IOs or the state. Although the emphasis on empowerment and ownership supports the hierarchy between the actors, with external actors defining the ‘ownership as theirs to give to national or local actors’ (Sending, 2015: 67), it may also be the outcome of providing the ‘platform’ for community members to discuss their issues and identify the solutions as part of ‘design-thinking’.
In addition to problems, community members also suggested solutions for staying healthy. They also nominated their members to implement these solutions. The SRC provided technical and financial support, or the ‘ecosystem’ (Flint and Meyer zu Natrup, 2019: 211), for the communities to conduct these activities. One of my interviewees pointed out that flexibility was essential to working with community volunteers. This also required going beyond the standard working hours and reaching out VHCs in the evenings when they were available (Interviewee I, 15 January 2018, personal communication, Bishkek: para. 45). At the same time, these activities were mainly guided by ‘international’ knowledge about preventive practices, such as using gloves against brucellosis, consuming iodised salt, measuring blood pressure, etc. Anaemia among pregnant women and children was targeted through food fortification. Following established international practice, micronutrient powder, composed of 14 micronutrients, was piloted in two provinces, with subsequent adaptation of the package design and instructions and changing the product name to the Kyrgyz-language Gulazyk (Lundeen, 2010). Recalling the discussion of ‘local’ and ‘international’ knowledge, although adapted to the local context, Gulazyk, similar to other ‘solutions’, represented international practice, not a locally generated solution.
The decision to use micronutrient powder, similar to other ‘solutions’ to healthcare issues, does not necessarily neglect the ‘local’ expertise or assert the supremacy of international knowledge, but was rather driven by utility concerns. Anaemia is attributed to multiple factors, including poor nutrition. Another contributing cause is the extensive consumption of black tea among the population (Schüth et al., 2014: 15) and giving black tea to young children (Lundeen et al., 2010: 447). The VHCs conducted awareness campaigns among pregnant women urging abstention from drinking black tea and stressing the importance of giving Gulazyk to their children (Schüth et al., 2014: 16–17). As a result, the rate of tea consumption among pregnant women and children fell (Schüth et al., 2014: 16–17), although overall reduction in anaemia among children was ‘slightly lower’ than in other countries where micronutrient powder was used (Lundeen et al., 2010: 458), which could also relate to tea consumption within the population (Medicus Mundi Schweiz, 2011: 25). Following Agrawal (2009), knowledge can be ‘useful or useless [. . .] socially relevant or irrelevant [. . .] without reference to whether it is indigenous or scientific’ (p. 157). Similarly, Bar-On (2015) highlights that knowledge of the ‘poor’ regarding how to cope with poverty does not ‘draw resources their way’ (p. 786). Similarly, this study argues that the choice to use international practice in targeting community concerns, was neither driven by geographical origin of knowledge nor the aim to prioritise one knowledge over another. The main reason behind it was to pragmatically solve these issues.
This ‘instrumental’ approach to knowledge also relates to the actors engaged in the project. Both SRC and VHCs are ‘action’ organisations (Boswell, 2009) as their existence and legitimacy are based on the results they achieve. As one interviewee mentioned, the VHCs are ‘themselves interested in changing something [. . .] they are not interested in their mere existence. They are not paid for that, they are volunteers [. . .]’ (Interviewee D, 19 January 2018, personal communication, Bishkek: para. 8–9). Although the SRC could also be a ‘political’ organisation with its legitimacy based on its existence (Boswell, 2009), its recognition at the local level and its ability to mobilise local communities required the demonstration of tangible results. Certainly, both the SRC and VHC also approach knowledge in a symbolic manner, as in the case of the Alma-Ata Declaration, in which comparison of the ‘local’ knowledge to ‘international’ was rather symbolic. In practice, the organisations represent a combination of ‘action’ and ‘political’ types (Boswell, 2009: 48), although knowledge in solving healthcare issues was guided by an ‘instrumental’ perspective. The dominance of this approach is illustrated in the interviewee quote about awareness-raising activities and the need to instal toilets, prompting a reaction of local community representatives that economic hardships faced by them have a higher priority than toilet bowls (see above). This clearly illustrates the ‘instrumental’ approach to knowledge, mainly driven by the solving of a specific healthcare problem. As a result, the VHCs implemented a number of activities to support vulnerable groups in their communities. Yet, such single attempts are unlikely to change the general economic and social problems in the country.
Flint and Meyer zu Natrup (2019) stress the necessity of testing potential solutions before identifying the final one. The annual evaluation of the VHCs and HPUs by its members contributed to a continuity of testing of the work conducted. It also contributed to the VHCs’ learning by indicating weaknesses and facilitating reflection on potential improvements (Interviewee C, 13 January 2018, personal communication, northern province: para. 67).
Testing is essential to verify effectiveness (achieving the stated objective), efficiency (value for money) and feasibility of the solution in a given context. ‘Solutions’, such as Gulazyk, in the CAH were initially piloted in several provinces before their broader implementation. Due to time and financial pressure, however, ‘testing’ and implementation in development assistance are often concurrent. In any case, ‘successful’ implementation of activity in one area does not guarantee similar results in other areas. For instance, VHC members in southern regions of the Kyrgyz Republic faced more obstacles related to traditional gender roles (Interviewee D, 19 January 2018, personal communication, Bishkek: para. 25). Organisational activities require continuous revision and adjustment to changing realities. One of the examples is the incorporation of WhatsApp into inter-VHC communication (Interviewee H, 30 January 2018, personal communication, Bishkek: para. 106) or the reduction of outreach campaigns on alcoholism as the alcohol consumption decreased (Interviewee F, 22 January 2018, personal communication, northern province: para. 55). Changes in the overall environment may shape issues and the relevant potential solutions. Therefore, this research suggests that there is no ‘final’ solution, as the process of finding appropriate solutions never ceases.
What factors contributed to the mutual learning between the actors? Among the key factors were decentralisation and leadership. Decentralisation proved an enabling factor for learning. The Swiss Co-operation Offices, representing the Swiss development cooperation system (including SDC) at the field level, are ‘fairly autonomous’ with some flexibility in staff management and fund allocation according to priorities defined by recipient governments (OECD, 2005: 22, 73–74). The SDC enjoyed autonomy in adjusting its activities to the needs of the local population, reflected in the flexibility of the CAH. Leadership was another factor contributing to mutual learning, because leaders occasionally facilitate learning (Salem et al., 2018: 603). The project coordinator promoted the PRA approach among team members, PHC specialists, VHCs and other actors involved in the project. The emphasis on people as ‘the ones who know’, rather than stressing the expertise of external actors, challenged the hierarchies inherent to development assistance by ensuring a respectful and rather equal relationship between the project team and community members. The VHCs recalled the project coordinator warmly (Interviewee C, 13 January 2018, personal communication, northern province: para. 9; Interviewee E, 22 January 2018, personal communication, northern province: para. 4; Interviewee F, 22 January 2018, personal communication, northern province: para. 189) and were ‘upset’ when he was leaving the country (Interviewee H, 30 January 2018, personal communication, Bishkek: para. 104). Overall, staff turnover negatively impedes learning (Berg, 2000: 34–35; Cheng, 2000: 140; Kontinen, 2018: 39–40). The project coordinator spent 13 years in the country, which ensured continuity and consistency of the PRA approach throughout the project. The continuous presence of the coordinator in the country also contributed to trust between the actors, which is essential to learning (Flint and Meyer zu Natrup, 2019).
Conclusion
This study explored the mutual learning between providers and recipients of development assistance using the example of the SRC and VHCs in the Kyrgyz Republic. It demonstrates that decentralisation of the organisation, its response to failures and its leadership can facilitate learning. Thus, increased authority of field offices may potentially contribute to their responsiveness to changes ‘on the ground’ and their flexibility to adjust accordingly. Furthermore, the organisational consideration of failures as inherent to learning (Flint and Meyer zu Natrup, 2019: 215) and increasing compliance with beneficiaries’ interests (Korten, 1980: 498) contribute positively to the learning process, while hierarchy between actors and their knowledge has an adverse effect. However, the focus on local communities and their expertise may alter these hierarchies. The project coordinator and his or her emphasis on the principles of ‘non-dominance’ and ‘non-interference’ were essential to changing the roles of project team members from ‘trainers’ to ‘learners’. Local communities, for their part, learned to express themselves and tackle the issues in the empowering environment provided to them. Overall, continuous contact between the SRC and the VHCs and the presence of the project coordinator in the country for over 13 years contributed to continuity of this environment and trust between the partners. The example of the SRC and VHCs in the Kyrgyz Republic demonstrates the feasibility of mutual learning in practice.
Although context-specific, these findings have broader relevance to programmes aiming to involve the local communities in the development process. The idea of joint planning and engagement of multiple actors is not new (cf. Korten, 1980; Suzuki, 2000), though a number of factors, such as inequality between the actors and their knowledge, remain. The ‘design-thinking’ approach addresses these inequalities by ensuring non-dominance of aid-providers in agenda setting (Flint and Meyer zu Natrup, 2019: 217). This provides a favourable environment for mutual learning to take place in practice. This study integrated the concept of mutual learning into the ‘design-thinking’ approach in order to observe the learning process throughout the assistance period. The combined framework focuses on the types of actors (‘action’ and ‘political’) and knowledge (local and international) involved, and the effect of learning (action or reflection) at problem identification, developing solutions and implementation stages. In this way, it benefits from the theoretical strengths of the mutual learning concept and the practical clarity of the ‘design-thinking’ approach. As this study focused on the learning between the SRC and the VHCs, future research could examine the learning between community organizations and other national (MoH, HPUs, LSGs) and international (Sida and USAID) actors, exploring its similarities and differences from mutual learning and its outcomes found in this study. At the same time, the combined framework suggested in this article is not bound to the specific country context, and could be used by other programmes willing to pursue the mutual learning and community involvement at both local and international levels.
Footnotes
Acknowledgements
The author would like to thank participants of the workshop on ‘International knowledge transfer and learning in social policy: The case of the post-Soviet region’, which took place on 9 November 2019 in Bremen, and particularly Dr. Karolina Kluczewska, for their helpful comments on the early draft of this article. She would also like to thank Dr. Tobias Schüth for his thoughtul suggestions and feedback, Natalia Zakharchenko for her support with data collection and Nathanael Brown for proofreading the final version of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) in the context of the Collaborative Research Centre 1342 “Global Dynamics of Social Policy” (Project No. 374666841) as Subproject B06 “External reform models and internal debates on the new conceptualization of social policy in the post-Soviet region”.