
Abstract
Summary
To advance our understanding of how we can best evaluate strengths-based approaches, we aimed to establish: (1) What the relevant outcomes are in strengths-based approaches in adult social care and social work in England; (2) How feasible it would be to measure them; and (3) Which tools and methodologies may be used in outcome measurement and evaluation. We used a Delphi consensus exercise to refine and reduce the long list of outcomes which had been identified in previous work as potentially useful in the evaluation of strengths-based approaches. The Delphi process consisted of two rounds (Rounds 1 and 2). The strengths-based outcomes were divided into five levels of measurement: relevant for a person who accesses social care and social work; relevant for unpaid or family carers; relevant for the community; relevant for the workforce in adult social care or social work; and relevant for organizations in adult social care and social work.
Findings
Fifteen experts completed Round 1 and 11 completed Round 2. At the conclusion of the Delphi consensus exercise, the expert panel agreed that 26 outcomes (66.7%, out of 39 considered) were both relevant and feasible to measure as part of an evaluation of strengths-based approaches in adult social care and social work. The panel also identified eight outcomes as relevant but not feasible to measure.
Application
This study provides a set of outcomes that practitioners, researchers, and policy makers can consider when evaluating strengths-based approaches in adult social care and social work.
Background
The adoption of strengths-based approaches in social work and social care for adults in the U.K. has been an embedded dimension of policy and practice (Caiels et al., 2021). This is the case at least since the 2014 Care Act which places a general duty on local authorities to promote wellbeing of people in need of care and support services (Department of Health and Social Care, 2023). Strengths-based approaches are a core part of the Act's statutory guidance; it refers explicitly to “the person's strengths and capabilities” and to “co-producing services with people who are receiving care and support to foster mutual support networks” (Department of Health and Social Care, 2023). Strengths-based approaches have been embraced by the Chief Social Worker for Adults in her 2017–2018 Annual report “From strength to strength” (Department of Health & Social Care, 2018) and are an integral part of the Professional Capabilities Framework for social work (in England) (BASW, 2018) and Social Work England's Professional Standards (Social Work England).
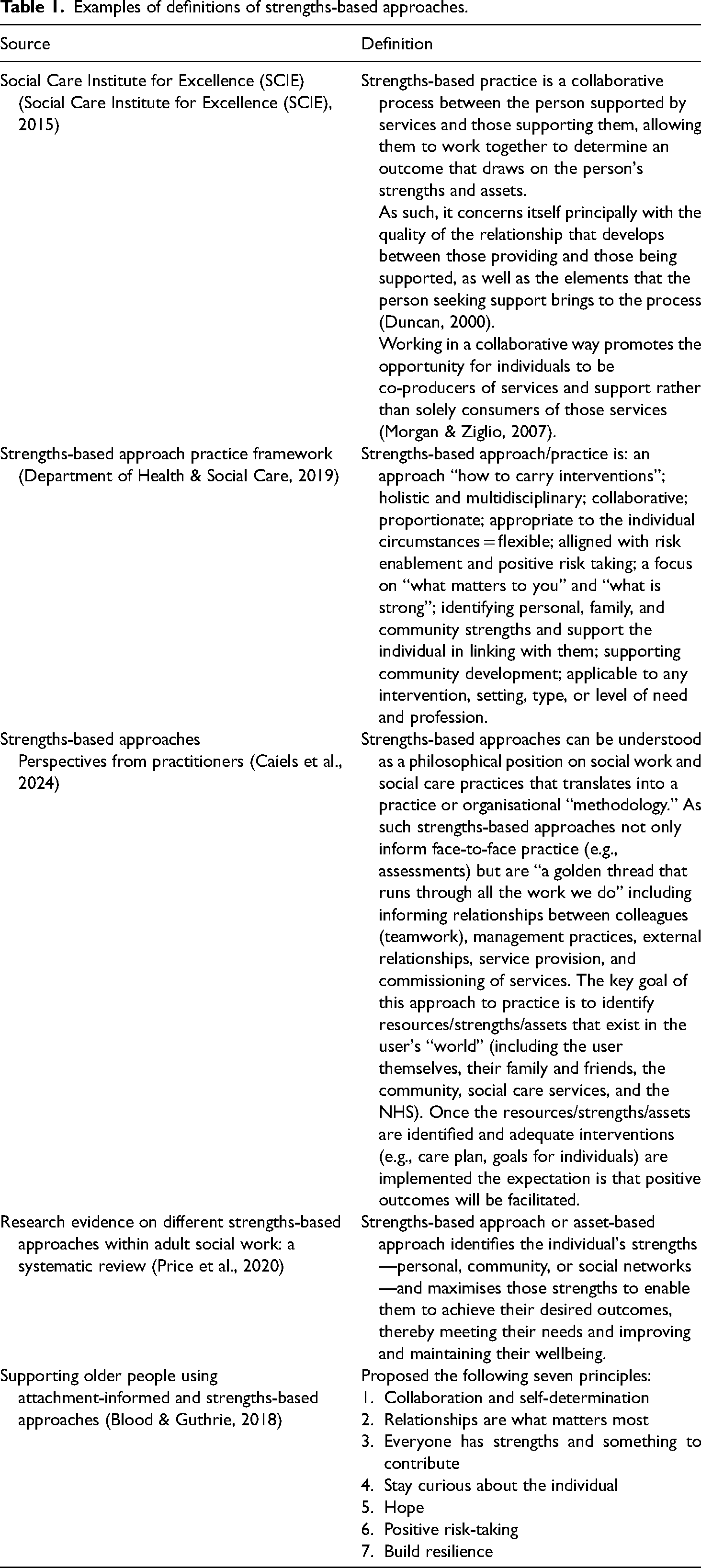
Despite substantial support for strengths-based approaches in both the policy and practice domains, it remains unclear which circumstances and for what groups of users they might be effective with, and precisely what impact they have (Caiels et al., 2021; Caiels et al., 2024; Price et al., 2020). The complexity of strengths-based approaches themselves makes any evaluation of effectiveness challenging (Caiels et al., 2021). This complexity takes a number of forms: including the absence of a clear consensus regarding the definition of strengths-based approaches (see Table 1), target populations, and intended outcomes (Caiels et al., 2021, 2024; Price et al., 2020). As such there is little agreement about how to evaluate the impact of strengths-based approaches, evaluation tools, and criteria regarding what constitutes evidence, and the most effective methods for assessing and measuring outcomes (Caiels et al., 2021, 2024; Price et al., 2020).
Examples of definitions of strengths-based approaches.
A recent systematic review (Price et al., 2020) confirmed the limited evidence base around the “effectiveness” of strengths-based approaches and the extent to which improved outcomes for people using social care and social work services, their families, and communities could be attributed to strengths-based approaches as compared to “usual services or approaches.” Although the review identified 15 U.K. studies, their quality was considered poor (Price et al., 2020). For strengths-based approaches to gain purchase in the adult social care field it is critical that work exploring the shape, nature, and effectiveness of strengths-based approaches is done and that confidence about what constitutes evidence is built (Stevens et al., 2024). There is therefore a need to develop appropriate methods, frameworks, and strategies for evaluation of the implementation (process evaluation) and effectiveness (outcome evaluation) of strengths-based approaches in adult social care and social work.
Aims
As a first step in advancing our understanding of how we can best evaluate strengths-based approaches, we aimed to establish:
what the relevant outcomes are in strengths-based approaches in adult social care and social work in England; how feasible it would be to measure them; which tools and methodologies could be used in outcome measurement and evaluation.
Methods
Study design
This study is the third stage of a larger project that focused on strengths-based approaches in adult social care and social work in England. The first stage included a scoping review of 72 sources that highlighted how strengths-based approaches have been embraced by policy makers and practitioners and widely adopted in practice, but also that questions remained about their definition, effectiveness, feasibility, and how they should/could be evaluated (Caiels et al., 2021). The second stage included analysis of free-text answers collected via an online survey completed by 32 participants (social workers, managers, and commissioners). Of these, 10 participants also took part in one-to-one interviews to gain further insight into their answers. The study concluded that strengths-based approaches had been adopted in a fluid, flexible way and are relevant for everyone involved in or in receipt of social care or social work. Participants also identified a range of outcomes they perceived as resulting from strengths-based approaches in their area of work. Evaluation varied and included small-scale qualitative and quantitative data collection within local authorities (in England local authorities are responsible for adult social care) (Caiels et al., 2024). In the third stage (of this study) we used a Delphi consensus exercise (Hasson et al., 2000) to refine and reduce the broad list of outcomes identified in the previous work (Caiels et al., 2021, 2024; Price et al., 2020; Sugavanam et al., 2021) to a “core set of outcomes” which, longer term, could potentially be used in the evaluation of strengths-based approaches. It consisted of two rounds (Rounds 1 and 2) (see Figure 1). Whilst we originally planned to capture strengths-based approaches in both adult social care and social work, all three stages of the project, including the present study, primarily captured approaches as applied in social work rather than in wider social care. This is because strengths-based approaches are being applied much more explicitly in the adult social work arena.
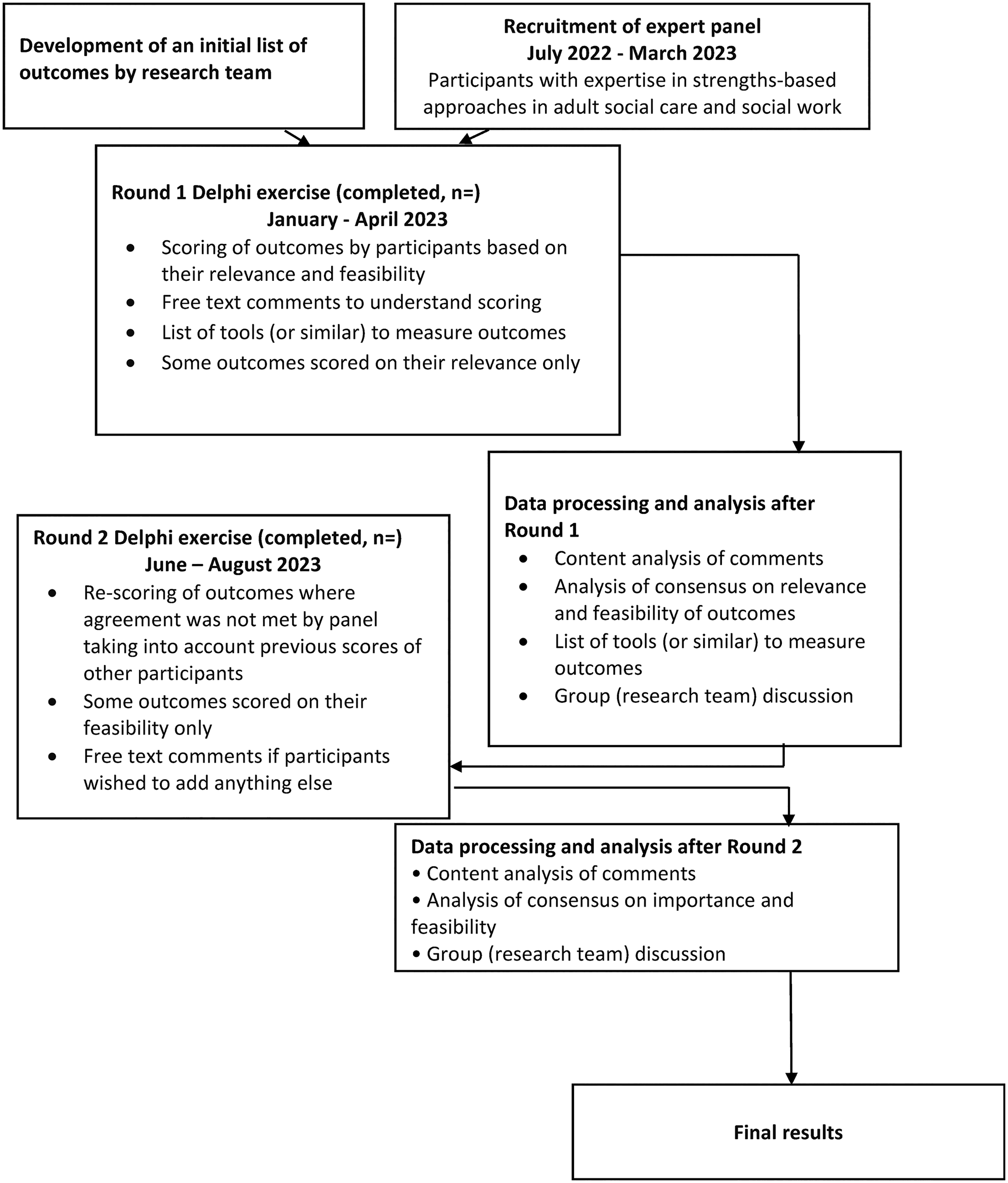
Summary of the Delphi exercise.
The Delphi consensus exercise is designed to elicit a “consensus of opinion” from a group of experts. Participants remain anonymous and provide feedback as part of the iterative process (Hsu & Sandford, 2007; Keeney et al., 2006). The initial list of outcomes for the expert panel to consider included outcomes identified in our previous work (Caiels et al., 2021, 2024). We combined them with outcomes drawn from two studies that were published since 2021: a core outcome set for trials and evaluative studies in adult social care (Sugavanam et al., 2021); and a systematic review of research evidence on different strengths-based approaches within adult social work (Price et al., 2020). Therefore, the initial step in the standard Delphi consensus exercise to identify the “items for inclusion” was not considered to be relevant as, in effect, this groundwork was completed as part of our previous work on strengths-based approaches (Caiels et al., 2021, 2024). Currently, there is no clear agreement on how many rounds of Delphi consensus exercise need to be held (Rowe & Wright, 2001) but the majority of the studies we reviewed conducted two to three rounds (Belton et al., 2019). We decided that the Delphi consensus exercise would be conducted across a maximum of two rounds (Pandor et al., 2019; Woodcock et al., 2020). These enabled us to have adequate reflection on group responses and to incorporate free-text responses from Round 1 to 2. We also recognized that the Delphi process places demands on already busy and time-constrained professionals, and we wanted to ensure maximum participation.
Participant recruitment
Figure 2 shows the flow of participants through the Delphi consensus exercise. For our panel “expert” was defined as: “an individual familiar with strengths-based approaches as well as (the concept of) measurement / evaluation of social care and social work in the adults’ field.” They were all located in England. Participants were identified using a purposive sampling strategy. This included drawing on our existing networks, for example, the Project Advisory Group that was established as part of the first and second stage of the larger project detailed above, and authors of key papers on strengths-based approaches. Potential participants were initially approached informally via email. This was followed up by two reminders (first after 4 weeks, second after 6 weeks) if they did not respond to the initial contact.
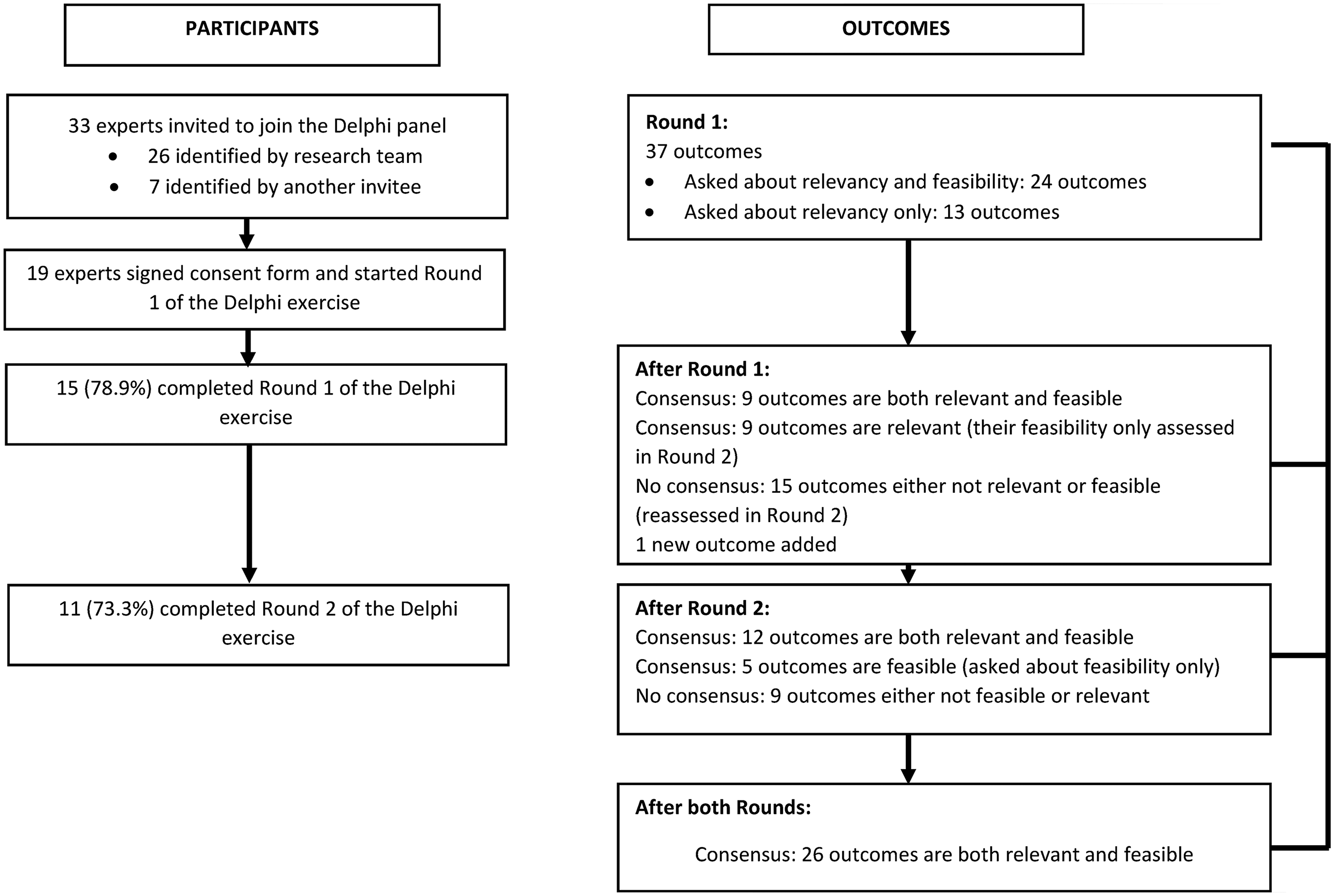
Flow of participants and questions through the study.
Once we had established a group of potential panel members, we sent them a formal invitation to take part in the consensus exercise: this explained the purpose of the study, how the Delphi process would work and the expected time commitment.
Data collection
All data were collected online using the Qualtrics XM Platform. Prior to beginning data collection, we piloted the questionnaire with four researchers working in adult social care from the University of Kent. None of these researchers were involved in the development of the questionnaire. We also piloted the questionnaire before Round 1 with a public and patient involvement member. We recruited the public and patient involvement member from the Public Involvement and Engagement Group that was set up as part of the NIHR Policy Research Unit in Adult Social Care. This member supported all three stages of the larger project described above and was involved in a range of activities including membership of the Project Advisory Group.
Prior to the commencement of each round, we sent participants an email outlining the tasks for the upcoming round, along with a web link to the online consensus exercise. Additionally, prior to Round 1, we provided to the participants a brief summary detailing the current perspectives on evaluating strengths-based approaches in social care and social work. To ensure active participation, we utilized the Qualtrics XM Platform™ to send two reminders at 2-week intervals during each of the two rounds. We also followed these up with emails to maximize opportunities for engagement.
Round 1
The Round 1 questionnaire consisted of two parts. In the first part, we asked participants to provide background characteristics (e.g., job title, gender, regional location, area of expertise, and experience with strengths-based approaches).
The second part of the Round 1 questionnaire focused on five different levels of measurement:
Strengths-based outcomes relevant for a person who accesses social care and/or social work; Strengths-based outcomes relevant for unpaid or family carers; Strengths-based outcomes relevant for the community; Strengths-based outcomes relevant for the workforce in adult social care or social work; Strengths-based outcomes relevant for organizations in adult social care and/or social work.
Each level of measurement included a different set of questions—this reflected the quantity and status of evidence. For example, service user outcomes have been more extensively researched, resulting in a greater number of identified outcomes compared to those for the workforce or for communities.
For strengths-based outcomes relevant for a person who accesses social care and social work, we included the following outcomes: resilience; sense of empowerment; sense of hope, possibility, or optimism; goal attainment; self-esteem; self-efficacy; sense of independence; feeling of control/ability to make choices; dignity; feeling of belonging/connection; quality of an interpersonal relationships; participation in community activities or resources; life satisfaction; wellbeing; functional ability; health-related quality of life; trust in social work and/or social care; an individual's needs are met; and level of satisfaction with a service. We asked participants to rate the relevance of each outcome on a 5-point Likert scale from “not at all relevant” to “very relevant.” In addition, we asked how feasible or difficult it would be to measure this outcome (e.g., using existing tools) on a 5-point Likert scale from “very difficult” to “very feasible.” Lastly, we asked whether the participant was aware of any tools to measure the outcome, and if so, to provide details of these. Each question included space for free-text comments in which participants could explain the rationale for their rating. At the end of this section, we offered participants an opportunity to add anything else about strengths-based outcomes relevant for a person who accesses social care/social work services.
For strengths-based outcomes relevant for unpaid or family carers, we asked participants to rate each outcome (burden placed on carers; carer's quality of life) in the same way as described for strengths-based outcomes relevant for a person who accesses social care and/or social work. Additionally, we asked participants about how they think family carers are conceptualized or viewed by strengths-based approaches. We asked them to rate the following statements on a 5-point Likert scale from “strongly disagree” to “strongly agree”: (1) “Unpaid (or family) carers will be considered as a resource (or strength) when the person they care for is assessed using a strengths-based approach”; (2) “There is a risk that more will be expected of unpaid (or family) carers when the person they care for is assessed using a strengths-based approach”; and (3) “Unpaid (or family) carers are likely to gain access to higher levels of support from social care services for themselves when the person they care for is assessed using a strengths-based approach.” Each question included space for free-text comments, in which participants could explain the rationale for their rating. The foundation for asking these questions is the ambiguous status of family carers in relationship to strengths-based approaches (Bolton, 2019). On the one hand, there exists a policy expectation that carers will not be exploited as a “free resource” (Department of Health & Social Care, 2019) and on the other hand, there are concerns that this is precisely what is happening in many situations (Bolton, 2019). At the end of this section, we asked participants whether they would like to add anything else about strengths-based outcomes that may be relevant for unpaid or family carers.
Regarding strengths-based outcomes relevant for the community, we asked participants to rate one question on a 5-point Likert scale from “not at all relevant” to “very relevant.” This was “Given the emphasis strengths-based approaches have on the use of community resources, how relevant do you think it is to include the availability and range of resources as an outcome of strengths-based approaches in adult social care and social work?.” The question also included space for free-text comments, in which participants could explain the rationale for their rating. They could also add free text relating to anything else about strengths-based related outcomes that they considered relevant for the community level.
Strengths-based outcomes relevant to the workforce in adult social care or social work included two subsections. First, we asked participants to rate the relevance of each outcome (worker's autonomy; level of trust; level of bureaucracy and paperwork) on a 5-point Likert scale from “not at all relevant” to “very relevant.” In addition, we asked how feasible or difficult it would be to measure these outcomes on a 5-point Likert scale from “very difficult” to “very feasible.” Lastly, we asked whether the participant was aware of any tools to measure the outcome, and if so, to provide information about these. Once again, each question included space for free-text comments, in which participants could explain the rationale for their rating. Second we asked participants to select which of these (if any) they think should be considered as outcomes of applying strengths-based approaches for the social care or social work workforce: staff morale; professional identity; job satisfaction; sickness levels and turnover of the staff; relationships and connections; awareness of available resources; and public perceptions of social work and social care. At the end of this section, we asked participants whether they would like to add anything else about strengths-based outcomes relevant to the social care or social work workforce.
Lastly, for strengths-based outcomes relevant for the organization in adult social care or social work, we asked participants to rate the relevance of each of the following outcomes on a 5-point Likert scale from “not at all relevant” to “very relevant”: preventing or delaying the need for more costly/statutory service; service users can have easier, quicker access to the right support; cost-effectiveness; level of complaints from people with care and support needs and families; and cultural shift as evidenced by different use of language (e.g., in organizational mission statements, purpose and value statement, with service users, between colleagues, etc.). The question included space for free-text comments in which participants could explain the rationale for their rating. We also asked participants whether they would like to add anything else; we were particularly interested to hear whether it is useful to capture organizational dimensions when evaluating strengths-based approaches in adult social care or social work and how we might capture related outcomes.
Initially, Round 1 was open for completion over a 4-week period, accompanied by two reminders at 2-week intervals. We extended the deadline for an additional month and sent a reminder at the 2-week point.
Consensus of opinion/agreement
The ultimate goal of the Delphi exercise was to elicit a “consensus of opinion” from a group of experts. Given the absence of a universally agreed-upon threshold for measures of consensus, we established a consensus level a priori (Hasson et al., 2000), following a similar approach in other studies. Each outcome required a minimum agreement of 70% (Pandor et al., 2019) in both relevance (combined scores of relevant and very relevant), and feasibility (combined scores of feasible and very feasible) to achieve consensus. Only the outcomes that had not achieved consensus for both relevance and feasibility in Round 1, as per the defined criteria, were asked about again in Round 2 (Helms et al., 2017; Lau et al., 2022). As is consistent with the Delphi consensus exercise process we revisited questions about both relevance and feasibility for outcomes where consensus had not been reached in one or both of these dimensions. However, as described in Round 1, we did not ask about both relevancy and feasibility for all outcomes. For strengths-based outcomes relevant for the community (one outcome) (Table S1 in the supplemental material) and those relevant for organizations in adult social care and social work (five outcomes) (Table S2 in the supplemental material), we asked about their relevancy only in Round 1. This is because the evidence on outcomes relevant for communities and for organizations is limited, and we wanted to first ascertain whether the expert panel considers these two sets of outcomes relevant before asking about feasibility. These outcomes required a minimum agreement of 70% in their relevancy in Round 1 (combining scores of relevant and very relevant) to achieve consensus in Round 1.
Round 2
At the beginning of Round 2, we provided participants with a document that included all the outcomes assessed in Round 1, along with an indication of whether consensus had been reached for each outcome. Additionally, we shared with them a list of tools or frameworks recommended/suggested by panel members in Round 1 for measuring each outcome.
We then asked participants about the outcomes for which consensus had not been reached in Round 1. For each outcome asked about in Round 2, we provided participants with two scores: the median score calculated based on responses from the expert panel in Round 1 and with the participant's own individual score. They were given the opportunity to revise their previous response if they wished.
For strengths-based outcomes relevant for the community (one outcome) (Table S1 in the supplemental material) and strengths-based outcomes relevant for organizations (five outcomes) (Table S2 in the supplemental material), we only asked about their feasibility in Round 2 rather than asking about both relevance and feasibility. This was because at Round 1 the panel agreed they were all relevant (combining scores of relevant and very relevant). This approach aimed to minimize the burden on participants by avoiding repetitive questions for outcomes where consensus had already been reached in Round 1 (for a complete list of details, please see Tables S1,S 2, and S3 in the supplemental material).
Round 2 was open for participants over a 4-week period in the first instance, with two reminders sent automatically at 2-week intervals. We extended this period for an additional month with one fortnightly reminder. No further rating rounds were conducted even if consensus was not reached following Round 2. This is because the aim of the exercise was not to achieve consensus on all outcomes but rather to refine, reduce, and distil the broad list of outcomes identified in previous work (Caiels et al., 2021, 2024; Price et al., 2020; Sugavanam et al., 2021).
Analysis of data
We used descriptive statistics to present quantitative data collected in Rounds 1 and 2. Descriptive statistics (e.g., median and frequencies) are reported for representing the group opinion. The analysis from free-text responses will be reported and discussed in a separate article. To achieve final consensus each outcome required a minimum agreement of 70% (Pandor et al., 2019) in both relevance (combined scores of relevant and very relevant) and feasibility (combined scores of feasible and very feasible).
Results
Characteristics of participants and response rates
We initially invited 33 experts to participate in the consensus exercise. Twenty-four (72.7%) agreed to participate in Round 1. Out of these, 19 began the survey, and 15 (78.9%) completed it. Only those who completed Round 1 were able to participate in Round 2. Of the 15 participants who completed Round 1, 11 participants (73.3%) started and completed Round 2. Figure 2 shows participants’ journey and the questions in Rounds 1 and 2. Table 2 shows the participant profiles for each round.
Characteristics of the participants in the expert panel for Round 1 and Round 2 respectively.
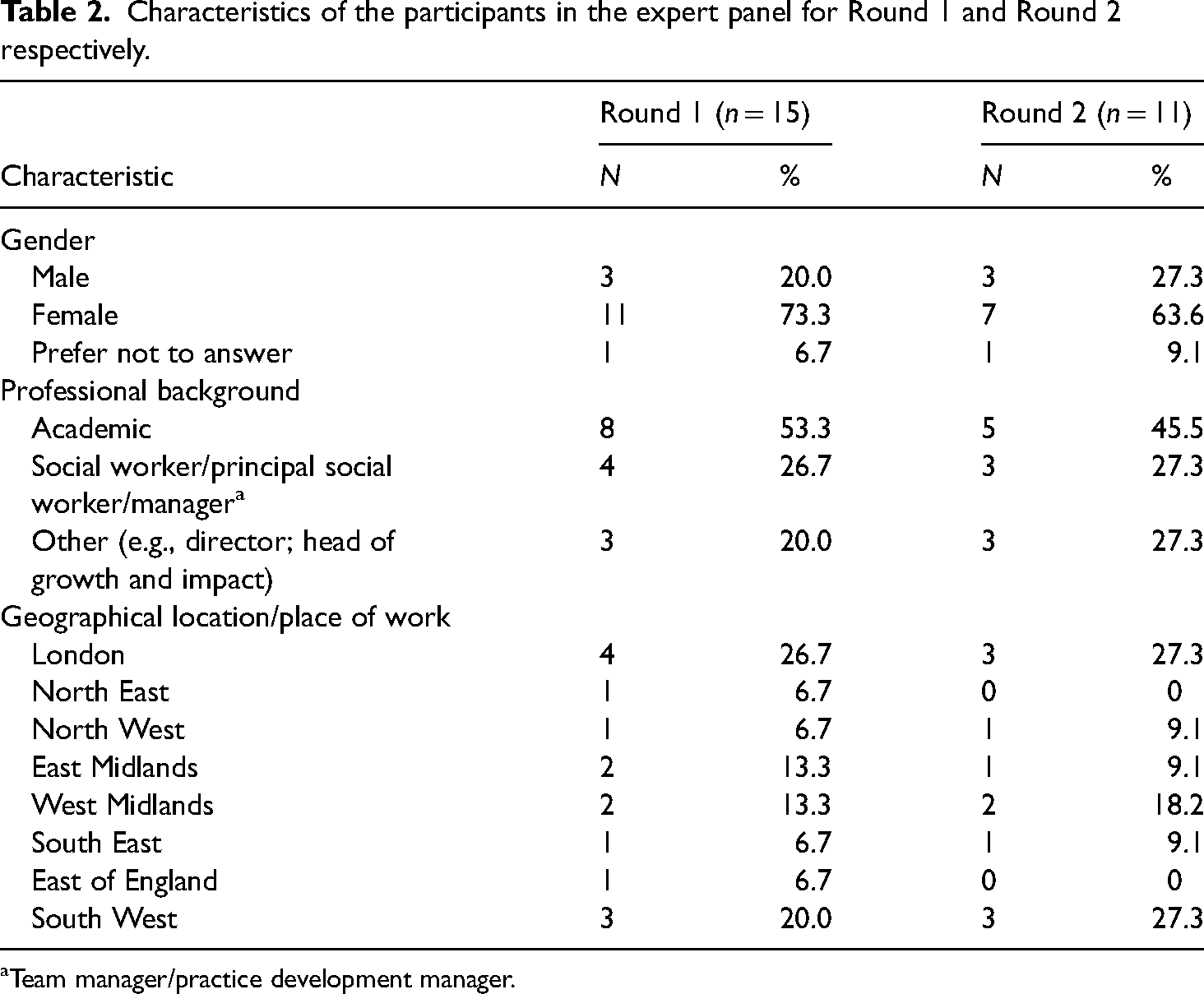
Team manager/practice development manager.
Twelve out of 15 participants indicated their area of expertise as “adult social care and social work,” with some providing additional information about their specific areas of work or role. These included: older adults; impact assessment; homelessness; special education needs; Housing First; direct payments; safeguarding; knowledge mobilization; integrated social care; mental health; family/network approaches; and leadership.
Participants had a range of experience in relation to engagement with strengths-based approaches. These included: conducting research on strengths-based approaches; delivering presentations on strengths-based approaches; developing and delivering training; creating practice handbooks and strengths-based frameworks; integrating strengths-based approaches into social care practice (e.g., during assessments, reviews, support planning, and working in partnership with people); consultancy work; assisting social care organizations in enhancing their practice and leadership through strengths-based approaches; and assessing social work effectiveness reviews. Given the participants’ background and expertise, it is important to highlight that the vast majority of the data gathered from participants related to social work rather than social care more broadly.
Reaching an agreement on outcomes and their feasibility for evaluation of strengths-based approaches in adult social care and social work in England
The full list of outcomes considered in Rounds 1 and 2, and the level of agreement per outcome, is shown in the in the supplemental material (Tables S1‒S3).
At the end of Round 1, the panel had reached consensus on the relevancy and feasibility of nine out of the 24 outcomes identified for evaluating strengths-based approaches in adult social care and social work (Table S1 in the supplemental material). These nine outcomes were integrated into the final list (Table 3) and were not considered in Round 2. The remaining 15 outcomes were amended based on suggestions from the expert panel and entered into Round 2. Amendments included: (a) relabeling the term “burden placed on carers” to “demands placed on carers”; (b) evaluating “the level of bureaucracy and paperwork” as two separate outcomes in Round 2; and (c) providing additional definitions for some outcomes where the panel indicated a need for further clarity, for example, for “sense of independence” we added the following definition as suggested by a member of the expert panel: “being enabled and having the support in order to live a self-directed life.” Based on feedback received in Round 1, we included “social isolation of unpaid (family) carers” as an additional outcome to be assessed in Round 2.
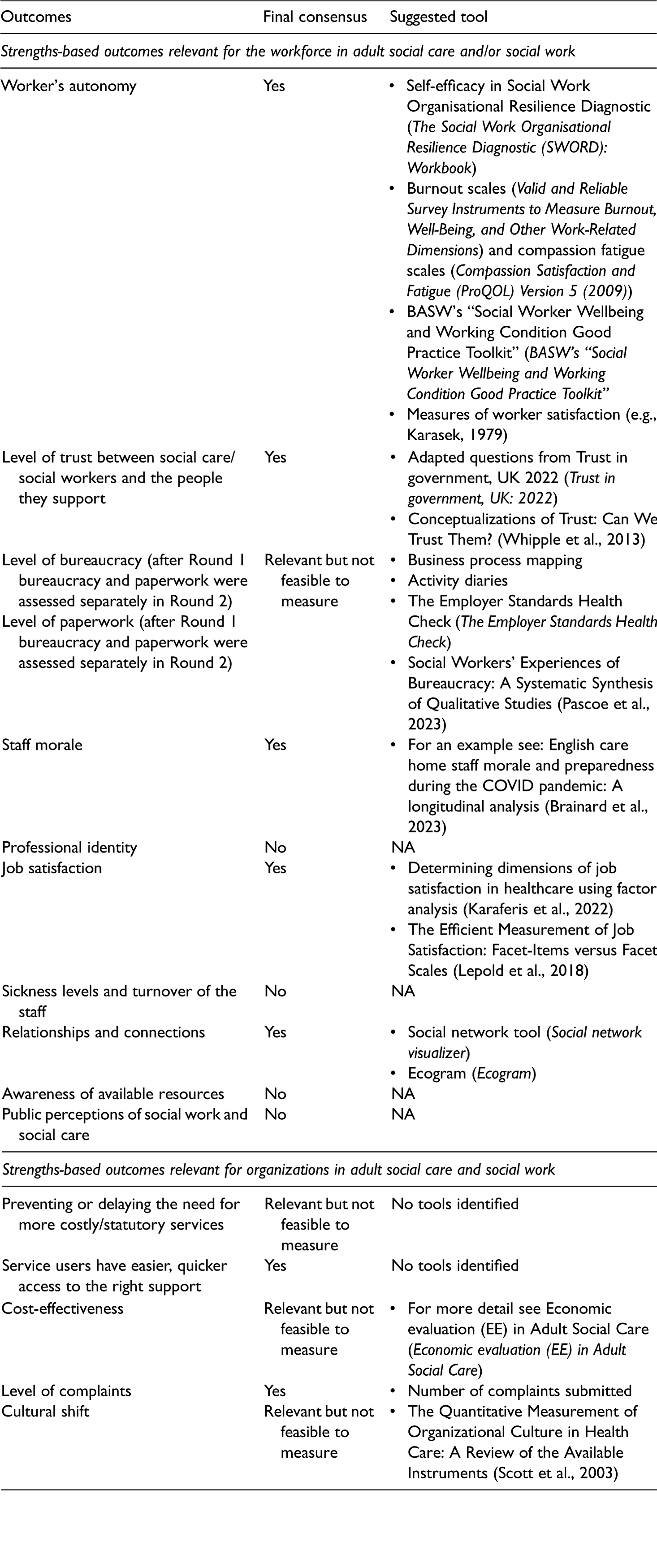
Final list of outcomes that are relevant and feasible to measure as part of the evaluation of strengths-based approaches.

In the case of strengths-based outcomes relevant for the community (one outcome) (Table S1 in the supplemental material), and strengths-based outcomes relevant for organizations in adult social care and social work (five outcomes) (Table S2 in the supplemental material), the panel reached a consensus that all of these outcomes were relevant. Thus, in Round 2, we focused solely on assessing their feasibility.
In Round 1, we asked the panel whether the following should be considered as strengths-based outcomes relating to the social work or social care workforce: staff morale; professional identity; job satisfaction; sickness levels; turnover of staff; relationships and connections; awareness of available resources; and public perceptions of social work and social care. As 70% of the panel membership selected staff morale, job satisfaction, and relationships and connections in Round 1, we proceeded only to assess their feasibility in Round 2.
At the end of Round 2, the expert panel reached consensus on the relevance and feasibility of 12 out of 16 outcomes for evaluating strengths-based approaches in adult social care and social work (Table S1 in the supplemental material). Regarding the outcomes exclusively assessed for feasibility in Round 2 (Tables S1 and S3 in the supplemental material), the panel reached agreement that five out of the nine outcomes are feasible to measure.
At the conclusion of the Delphi consensus exercise, the expert panel agreed that 26 outcomes (66.7%, out of 39 considered) were both relevant and feasible to measure as part of an evaluation of strengths-based approaches in adult social care and social work (Table 3). The panel also identified eight outcomes as relevant but not feasible to measure. These were: (a) for a person who accesses social care and social work: resilience; dignity; (b) for the community: the availability and range of community resources; (c) for the workforce in adult social care or social work: level of bureaucracy; level of paperwork; and (d) for organizations in adult social care and/or social work: preventing or delaying the need for either more costly and/or statutory services; cost-effectiveness; and cultural shift as evidenced by different use of language. The panel did not reach consensus on the relevance or feasibility of measuring five outcomes related to strengths-based approaches. These were: (1) functional ability for a person who accesses social care and social work; (2) professional identity; (3) sickness levels and turnover of staff; (4) awareness of available resources; and (5) public perceptions of social work and social care.
Tools to measure outcomes for evaluation of strengths-based approaches in adult social care and social work in England
As part of Round 1, we asked panel members if they knew of examples of any tools that could be used to measure outcomes as part of evaluating strengths-based approaches. Participants were encouraged to consider all types of approaches or tools (both qualitative and quantitative) when responding.
The examples listed by the expert panel are included in Table 3. These also include other tools known by the research team.
Conceptualization of unpaid or family carers in strengths-based approaches
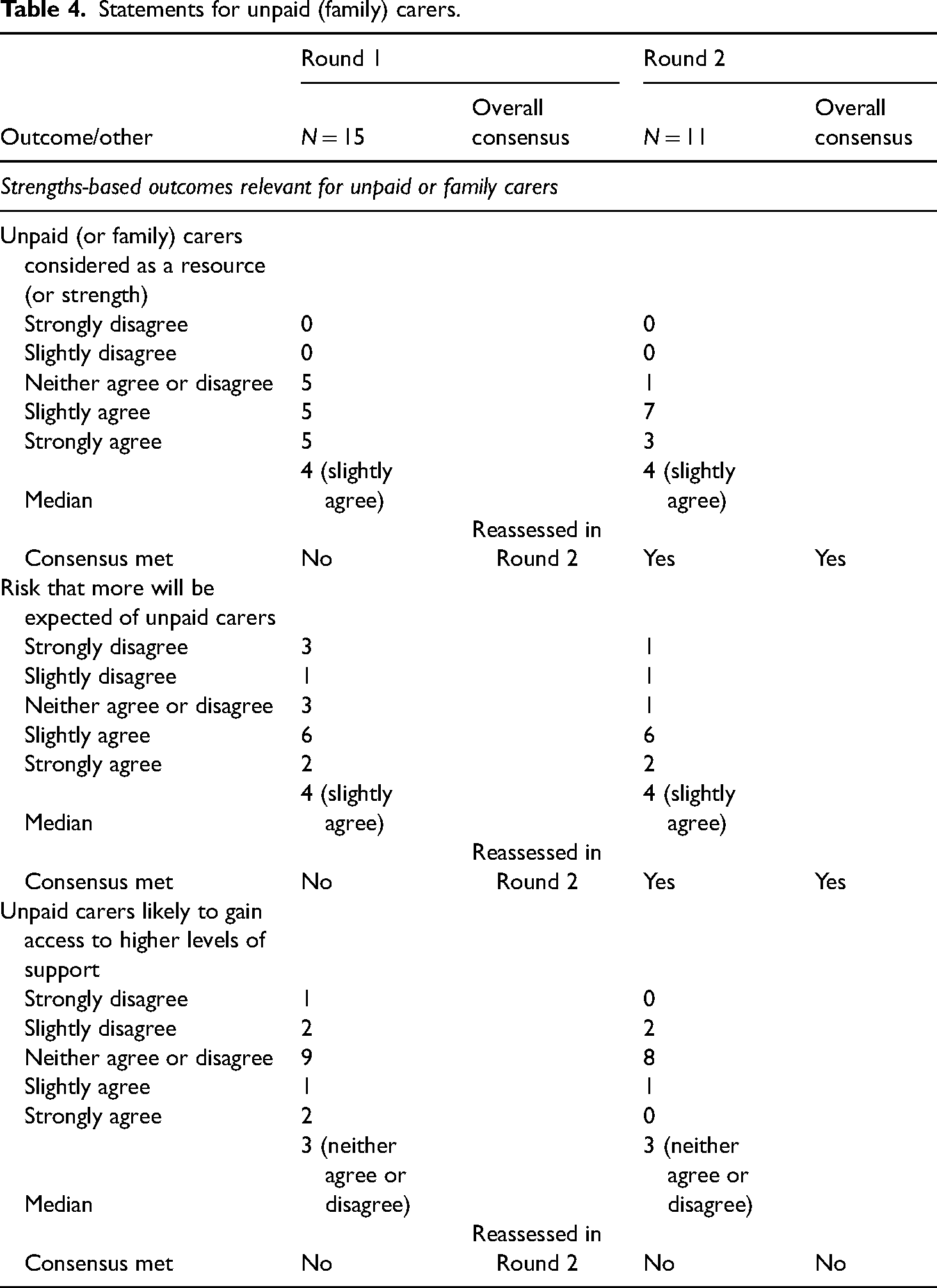
Following Round 2, the expert panel reached consensus (at least slightly agreed) around two carer-related statements: “Unpaid (or family) carers are considered as a resource (or strength)” and “There is a risk that more will be expected of unpaid carers” in the context of strengths-based approaches. The panel neither agreed nor disagreed about the third statement that, “Unpaid carers are likely to gain access to higher levels of support” when applying strengths-based approach (Table 4).
Statements for unpaid (family) carers.
Discussion
The aim of this article was to advance our understanding of how we can best evaluate strengths-based approaches in adult social care and social work. We used the Delphi consensus exercise to elicit agreement among 15 experts in strengths-based approaches in adult social care and social work on what the relevant and feasible outcomes are in strengths-based approaches in adult social care and social work in England. In addition, the expert panel suggested tools and methodologies that may be used in outcome measurement and evaluation.
As emphasized above, practitioners (Caiels et al., 2024), professional bodies (BASW, 2018; Social Work England), and policy-makers (Department of Health & Social Care, 2018, 2023) widely embrace strengths-based approaches in adult social care and social work. Despite this, the current evidence base supporting improved outcomes for adults using social care services, their families, and wider communities relating to the adoption of strengths-based approaches remains limited (Caiels et al., 2021; Price et al., 2020). This paucity of evidence is attributed to the numerous challenges relating to evaluating strengths-based approaches in adult social care and social work (Caiels et al., 2021, 2024; Price et al., 2020). These challenges include a lack of consensus about the definition of strengths-based approaches and the difficulty of attribution, that is, knowing whether improved outcomes for the service user were a result of the strengths-based approach, and if so which elements of the approach used accounted for the improvement in outcomes. There is also confusion about whether a strengths-based approach is an intervention, a conceptual model, and/or an ideological position (Caiels et al., 2021). Another challenge relates to determining who the beneficiaries of strengths-based approaches are: individuals who draw on social care and social work services, their families, the wider community, practitioners, and/or social care organizations.
Given the importance of evaluation studies as foundational sources of evidence for policy-makers, commissioners, and funding organizations, there is a pressing need to delineate what outcomes the adoption of a strengths-based approach can reasonably be expected to deliver for which beneficiary/ies and how feasible these outcomes are to measure. This study sought to establish agreement on which outcomes are both relevant and feasible to measure for individuals who draw on social care and social work services, their families, the wider community, practitioners, and/or social care organizations to inform the design of studies to evaluate strengths-based approaches. Using a Delphi process, an expert panel achieved consensus on 26 outcomes deemed both relevant and feasible for measurement across individuals who draw on social care and social work, their family carers, communities, workforce, and organizations. The study also offered insight into how these outcomes could be measured, using both qualitative and quantitative methods.
In addition to specific evidence about outcomes, our study offers some other interesting new findings. Whilst confirming that individuals who draw on social care and social work can benefit from the adoption of a strengths-based approach, we also identified that family carers, wider communities, social workers, and social care organizations can be positively impacted too. We have also highlighted how family carers are conceptualized in strengths-based approaches, an issue that is rather opaquely referred to in existing literature.
While this study was conducted in England, the shared policy and practice context of the rest of the U.K., and similar contexts in other countries in Europe and beyond, make it very likely that our findings will have resonance beyond the English context. In addition, as the majority of the outcomes that the experts considered as part of this Delphi study were identified in a previous scoping review of international literature (Caiels et al., 2021), this increases the likelihood of wider relevance.
Limitations of the study
The study has a number of limitations. We did not attempt to preference weight the 26 outcomes, that is, some being more relevant than others; neither did we analyze what relationships may exist between outcomes. Also, while we included all tools and methodologies suggested by the expert panel, we did not assess their psychometric properties—specifically their feasibility, reliability, and validity for application in adult social care and/or social work. We did not explore the potential costs of conducting an evaluation. These issues need to be explored in future research.
It is noteworthy that the majority of participants, due to their background and expertise, were associated with social work rather than social care more broadly. This observation mirrors our previous work (Caiels et al., 2021, 2024) which highlights how social care is a very broad and multi-dimensional and multi-disciplinary field. Strengths-based approaches are more easily conceptualized in one-to-one social work encounters; they have also been embraced by social workers (BASW, 2018) in a way that is much less visible in the wider field of social care. Consequently, we suggest that the outcomes established in this study are considered in the context of social work with adults rather than social care more broadly.
We acknowledge that the size of the panel was modest and that, despite several reminders, there was some attrition in participation. This is not surprising given the immense pressure on the social work sector, where individuals often have very limited time. In response to feedback during Round 1, which highlighted the length and time-consuming nature of the Delphi consensus exercise, certain adjustments were made for Round 2. Specifically: free-text questions; questions about outcomes already achieving consensus in Round 1; and queries regarding potential tools for outcome measurement were omitted. However, it is also important to note that there is no agreement on the minimum panel size required for content validity in Delphi studies. Recommendations vary from 5 to 30 participants (Bolton, 2019; Lau et al., 2022; Woodcock et al., 2020), but in general it is agreed that the response rate of each Delphi round should not fall below 70% which this study achieved (Kilroy & Driscoll, 2006).
Conclusion
In conclusion, this study provides a set of outcomes that practitioners, researchers, and policymakers can consider when evaluating strengths-based approaches in adult social work, and with some additional work, adult social care too. These outcomes are categorized into five levels of measurement, these being strengths-based outcomes relevant for: individuals accessing social care and social work; family carers; the community; the workforce in adult social care or social work; and social work/care organizations.
The study represents a first step in advancing our understanding of how we can best evaluate strengths-based approaches, particularly in social work with adults. Future research should establish whether the tools and methodologies proposed by the expert panel are feasible, reliable, and valid. It should also explore the relative significance of the 26 identified outcomes, the interrelationships between these outcomes, and the potential costs associated with any evaluation. While this study focuses on one part of the overall evaluation process—outcome evaluation, there is also a need to develop appropriate methods, frameworks, and strategies for evaluation of the implementation (process evaluation) of strengths-based approaches, and find ways to include the perspectives of people who use adult social care and social work and their family carers.
Footnotes
Ethical approval
Ethical approval for this project was given by the University of Kent Research Ethics Committee (Ref: SRCEA 0278) and e-consent was obtained at the beginning of data collection.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute for Health and Care Research (NIHR) [grant number: PR-PRU-1217-21101]. This paper reports on independent research commissioned and funded by the National Institute for Health and Care Research's (NIHR) Policy Research Unit in Adult Social Care (ASCRU). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, the Department of Health and Social Care or its arm's length bodies, and other Government Departments.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ contributions
All authors contributed to developing and testing the Delphi survey. BS analyzed the data. All authors reviewed and interpreted the results. BS wrote the manuscript with input and final review by JC, AM, and JB-B. JC led the overall study.
Acknowledgements
The authors acknowledge the following for their contribution to this article: a Project Advisory Group for their time and contributions to producing this research, they are: Peter Atkins; Sam Baron; Carmen Colomina; Carla Fourie; Liz Greer; Liz Howard (from British Association of Social Workers England); Jo Moriarty; Tricia Pereira; Jenefer Rees; Kate Sibthorp; Julie Statton; and Madeleine Stevens. Additionally we would like to thank the expert panel who took part in the Delphi consensus exercise—they shared their time and expertise with us generously.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.