
Abstract
Summary
The COVID-19 pandemic and subsequent public health restrictions caused an unprecedented impact on long-term care services in the United Kingdom (UK). A qualitative study was conducted in the East Midlands, UK, to explore how home care provision was perceived and experienced, by those organizing, commissioning, or providing care, and those receiving care, during the pandemic. Fifteen semi-structured telephone interviews were conducted between September to December 2020 with people who organize, commission, or provide home care (n = 9), recipients of home care (n = 3), and their informal carers (n = 6).
Findings
Three broad themes were constructed through a thematic analysis: (1) positive about home care; (2) fear of infection; and (3) social isolation. In addition to these overarching themes, specific group themes were identified amongst group one: those organizing, commissioning, or providing care, and group two: those in receipt of the care and informal carers. Those in group one spoke about the pandemic creating stressful working conditions, regardless of whether organizing, commissioning, or providing care. Despite working throughout the pandemic, they felt a forgotten part of the essential workforce, when compared to those employed in the National Health Service and institutional care. Those in group two experienced a loss of control with visits cancelled or frequently occurring outside of scheduled times. Dissatisfaction with the visits was directed at the management level, rather than at the staff visiting the homes.
Applications
Awareness and understanding of the experiences of home care will provide useful knowledge when commissioning future services.
Introduction
On March 23, 2020, in response to the growing COVID-19 pandemic, the British government introduced a nationwide lockdown in England with associated public health measures. The population were obliged to remain in their own home except for essential trips and once-daily exercise (Giebel et al., 2021a). People aged 70 and over with underlying health conditions, were identified as being at greater risk of mortality from the virus (Sepulveda-Loyola et al., 2020), and were subsequently advised to shield, avoiding all face-to-face contact, except for carers. A narrative review exploring the impact of social distancing policies concluded that the mental health of older people was affected negatively with higher levels of depression and anxiety identified (Sepulveda-Loyola et al., 2020).
The government restrictions placed an unprecedented impact on social care services. Many of these services, such as day and respite care, closed during lockdown. A national United Kingdom (UK) survey conducted with older people and informal carers during the lockdown concluded that reduction in social support was significantly associated with reduced levels of well-being and increased anxiety in older adults. One service that continued, albeit at a reduced level, was the formal home care service (Giebel et al., 2021b). The term home care in the UK covers a wide variety of care provision and tasks, these range from assistance with instrumental activities of daily living, such as shopping and food preparation, to basic activities of daily living such as bathing, toileting, and dressing (Giebel et al., 2020a).
Studies conducted during the UK lockdown with people living with dementia and their informal carers reported that those in receipt of care were fearful of catching COVID-19 from those providing their care, recognizing the risk that home care workers might spread the virus from household to household (Giebel et al., 2020; Giebel et al., 2021a). At the time of the lockdown home care recipients had to decide whether to continue with the service, and risk possible infection from visiting staff, or reduce or cancel it (Giebel et al., 2020).
An additional or alternative source of support in the home is provided by informal carers. Defined as family or friends who provide unpaid care for older people, or people with disabilities and/or long-term health conditions (Carers, 2020a). There are 6.5 million informal carers in the UK (Carers, 2020a), and this number increased by an additional 4.5 million during the lockdown (Carers, 2020b). Furthermore, those already providing informal care increased their input during the pandemic due to reduced or cancelled community services (Carers, 2020a; Lorenz-Dant & Comas-Herrera, 2021). Many of these informal carers provided care alongside their own work commitments (Carers, 2020b). This was made possible due to furloughing and working at home arrangements during lockdown. However, similar to the homecare workers, informal carers feared catching and spreading COVID-19 to the person they cared for (Lorenz-Dant & Comas-Herrera, 2021).
A rapid mapping review of measures taken to mitigate the impact of COVID-19, on people receiving or providing long-term care, found only eleven studies covering home care services. This review identified an evidence gap around home care during the COVID-19 pandemic (Byrd et al., 2021).
Studies on home care conducted in the USA and Norway have been identified (Cabin, 2021; Eide et al., 2021; Markkanen et al., 2021; Osakwe et al., 2021; Sterling et al., 2020). Perhaps, unsurprisingly, they report participants, regardless of whether providing or receiving home care, feared catching COVID-19 (Osakwe et al., 2021; Sterling et al., 2020), and problems around accessing personal protective equipment was reported (Osakwe et al., 2021; Sterling et al., 2020). The home care workers spoke of being inadequately supported with training, information, and resources (Osakwe et al., 2021; Sterling et al., 2020). A range of concerns was expressed for those in receipt of home care including isolation, loneliness, depression, and anxiety (Cabin, 2021; Markkanen et al., 2021). These were psychological problems that often existed as the norm before the pandemic but became exacerbated by COVID-19 (Cabin, 2021). An increased burden on informal carers was also reported with family members taking on more day-to-day care (Eide et al., 2021).
There were problems with home care prior to the pandemic. Frustration has been voiced by home care recipients and their informal carers around reliability, flexibility, poor communication, and continuity (Francis & Netten, 2004; Fraser et al., 2014). COVID-19 brought new pressures and challenges to the home care service, and it is unknown if these issues were compounded further during the pandemic.
In the UK, Giebel et al. (2020) focused on home care provision during the national lockdown. This study involved interviewing informal carers of people living with dementia. It highlighted the distress of maintaining home care due to the risks of infection, the difficult decision of whether to continue to allow multiple carers to enter the home and the increased burden on carers taking on extra carer responsibilities.
It is recognized, within the limitations of the Giebel et al. (2020) study that paid carers were not interviewed. Equally, the sample was limited to carers of people living with dementia whereas home care is provided to a much broader group.
Therefore, the aim of this study was to explore the experiences of those organizing, commissioning, or providing care, and those receiving the home care service in two geographical areas of the East Midlands, UK, during the COVID-19 pandemic, and to use this learning to inform future practice.
Design
The stakeholders wanted to approach the service with an appreciative eye (Hammond, 1998), therefore an exploratory qualitative approach was adopted utilizing a modified form of Appreciative Inquiry (Carter, 2006; Postma, 1998). This approach begins with an appreciation of the “best of what is” in order to articulate “what might be” (Bushe, 1995). The positive focus of Appreciative Inquiry reduces defensiveness and encourages open discussion.
However, the authors had concerns that Appreciative Inquiry had the potential to “brush under the carpet” what doesn’t work (Reed et al., 2002) and prevent learning from the experience. Indeed, it has been found that examples of poor practice can provide understanding of what constitutes good care (From et al., 2009). This study therefore explored examples of both what worked and what did not work during the pandemic.
Participants
Four groups of participants were recruited:
Paid social care workers who were organizing, commissioning, or providing home care. Home care recipients who received a package of care prior to UK lockdown on 23rd March 2020. Family, friends, or neighbours of individuals who were receiving home care and who also assisted with care tasks. Volunteers who had taken on caring tasks during the COVID-19 pandemic. It transpired that this group were not involved with the home care service. The findings in relation to this group will therefore be presented separately in a future paper. Aged over 18 years. Lived within two geographical locations in the East Midlands, UK, or organized, commissioned, or provided home care in these regions. Lacked capacity to consent and engage with the interview process. Unable to participate in a telephone interview. Unable to understand written or spoken English. Individuals receiving care whom the Local Authority Adult Care Service cited as inappropriate to recruit (e.g., those with a history of aggression).
Participants from both genders, different ethnicities, and a mix of ages were purposively sought. The inclusion criteria for participants were individuals who were:
The exclusion criteria for participants were individuals who:
Recruitment
Potential participants were identified by the Local Authority databases and sent an “Invitation to Participate” and participant information sheet (PIS) via post and email. This outlined the reason for the research and asked interested individuals to contact the researchers (details were provided). Once contacted the researchers again explained the study and arranged a telephone interview. All recruitment conversations took place either over the telephone or via email.
Data collection
Telephone interviews took place from September to December 2020. Verbal consent was obtained from participants at the start of the interview and was recorded. Two experienced qualitative researchers (JD and FA) conducted the interviews. Thirteen interviews took place between one researcher and one participant. Two interviews were conducted with multiple participants involving both the home care recipient and their informal carers.
Interviews were semi-structured and used specific interview schedules which asked participants for examples of what had worked well, and conversely what had not worked well, during the lockdown. The schedules were discussed amongst the stakeholder group but were not pilot-tested due to time constraints.
Audio recordings of interviews were kept securely in encrypted and password-protected files on university computers. Interview data was transcribed verbatim and anonymized at point of transcription. Field notes were made by the researchers following each interview to identify initial thoughts and assumptions. These were discussed amongst the team in analysis meetings.
Data analysis
Two researchers (JD), an occupational therapist, and (FA) a physiotherapist, completed the analysis. In recognition that therapists work within a particular theoretical framework, and that this shapes their interpretation of the data (Braun et al., 2022) a Patient and Public Involvement (PPI) partner (CK) also analyzed some of the transcripts. This provided an alternative perspective upon the emerging themes. This partner was trained in the analysis process. The researchers completed a reflexive diary and discussed their reflections alongside their analysis (details on analysts’ backgrounds supplied at the end of the paper).
The data was analyzed using the steps of thematic analysis (Braun & Clarke, 2006). This involved the analysts familiarizing themselves with each transcript before completing a line-by-line inductive analysis to identify codes. This was repeated for each of the transcripts. The initial codes were applied to subsequent transcripts alongside newly identified codes. The researchers and Patient and Public Involvement partner met regularly to discuss their coding. Once all transcripts had been coded they met again to discuss their reflexive notes and together constructed the themes. One set of themes spanned all the participant groups, and another set were focused on those organizing, commissioning or providing care (group 1) and those in receipt of care and their informal carers (group 2).
Findings
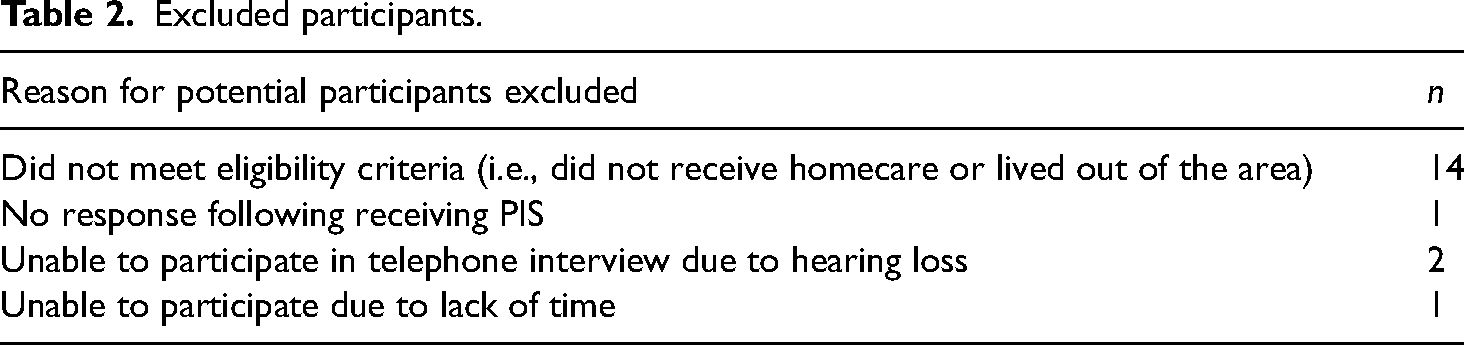
A total of 18 participants were interviewed. Nine participants (those organizing, commissioning, or providing care) were grouped together as formal carers in group one. Group two was composed of those receiving the home care service: six informal carers, and three home care recipients. Demographic information on the 18 participants is provided in Tables 1 and 2 provide details of excluded participants.
Sample demographic.
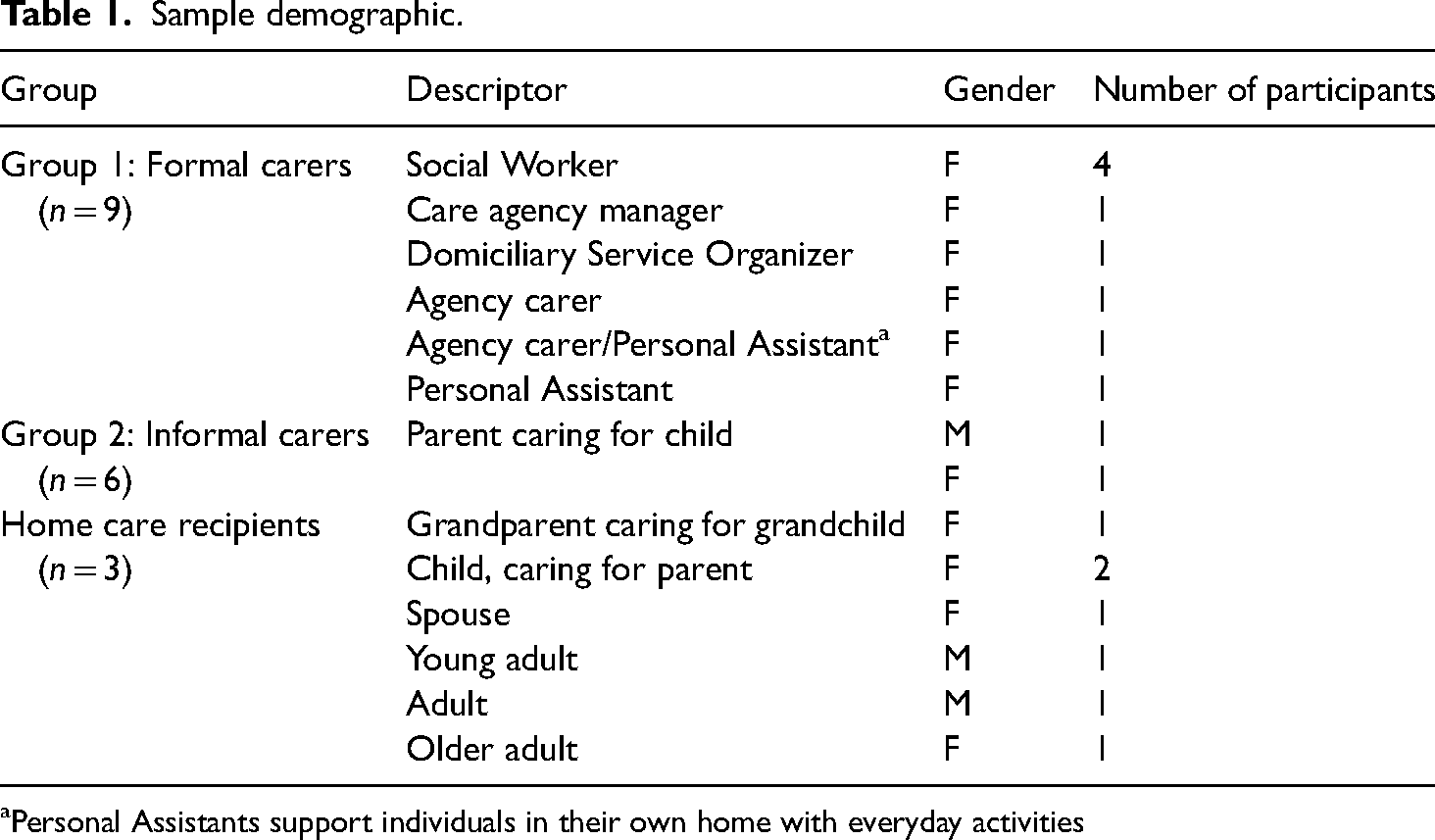
Personal Assistants support individuals in their own home with everyday activities
Excluded participants.
Interviews ranged in length from 21 min to 83 min (average length 48 min).
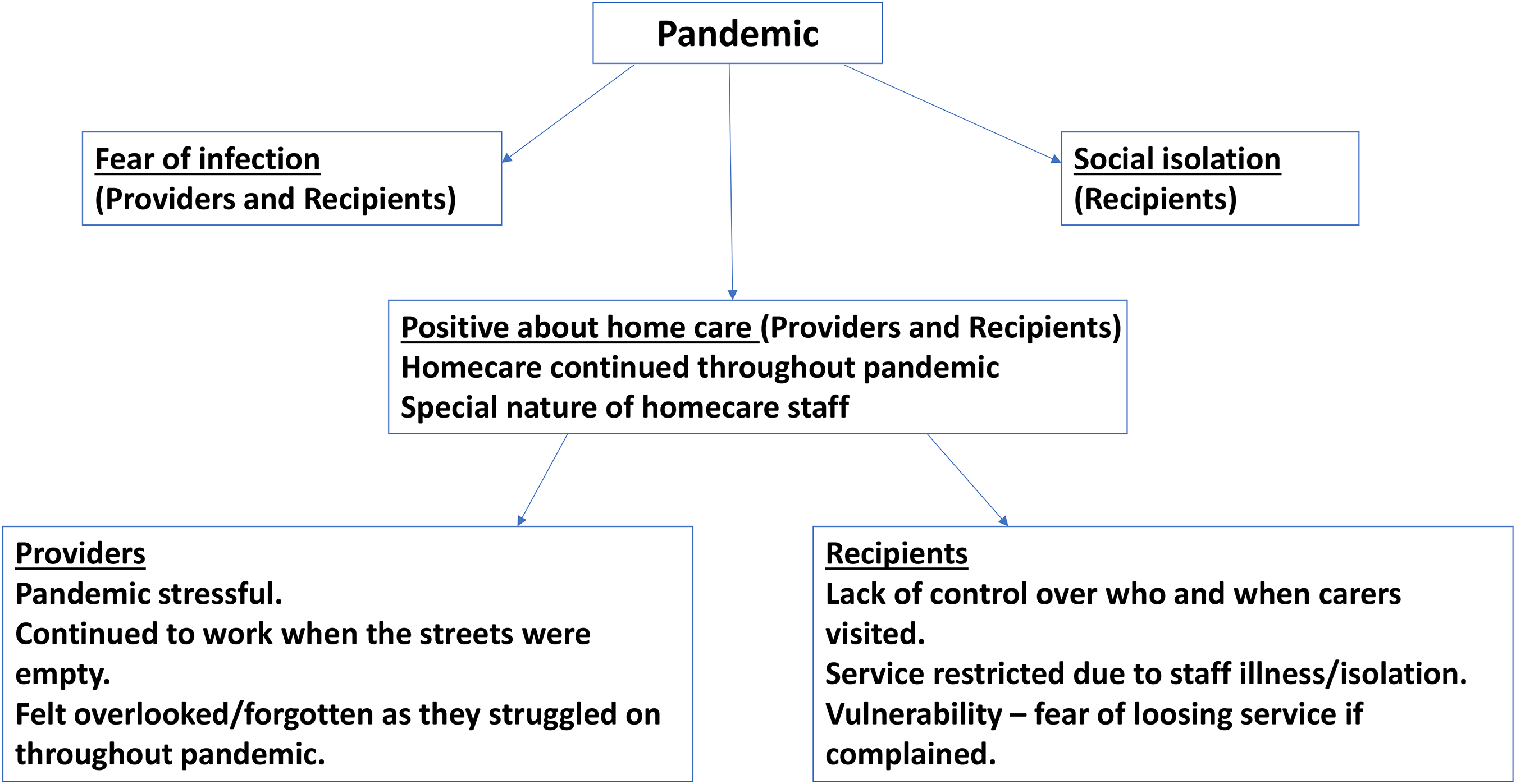
The analysis identified three broad themes across all the participants: positive about home care, fear of infection, and social isolation. Following this, a sub-analysis describing the experience from group one (those organizing, commissioning, and providing care) and group two (those in receipt of the care) perspective is provided.
Broad over-arching themes
Positive about home care
There was an overriding feeling of positivity about the home care service, regardless of whether the participants were recipients, informal carers, or those organizing, commissioning, or providing the care. This was largely attributed to the fact that the home care service, unlike other services—colleges, day care, and respite—continued throughout the pandemic. Some complaints were made about the timing of visits, but even those participants who made complaints were at pains to express appreciation and gratitude for the ongoing service.
Those who organized, commissioned, or provided the home care services—the Social Workers, homecare manager, and Domiciliary Services Organizer also expressed appreciation for the home care workers: And they do an amazing job. And they do provide a service that I wouldn’t want to provide for their level of pay at my current level of pay. But they are absolutely essential. (Formal carer 4, social worker)
They spoke about the home care staff going above and beyond their role, taking on extra tasks, many of which had previously been completed by family members before lockdown. Often these extra tasks, such as shopping, were completed outside of their paid hours.
The recipients and informal carers were not only positive about the continuation of the service in such difficult times, but were also positive about the individual carers that visited. They talked about the “fantastic” and “lovely” home care staff. Many spoke about the special nature of the carers whom they described as kind, supportive, and encouraging. They outlined how the carers spent time interacting with them and how they got a difficult job done with minimal fuss: They … don’t just come in and, robotics. Just do this, do this, I’m off. They’ll sit down and they’ll … it's just you know when you get somebody that's kind. Somebody that's just a good laugh, you know. (Home care recipient 3)
Fear of infection
It is perhaps unsurprising that fear of infection was a strong theme amongst those organizing, commissioning, or providing care and those in receipt of the care. Concerns were expressed about spreading and catching the virus: Because they would be going to other people's home[s] and then there was a chance that they could be bring COVID-19 into the home. (Formal carer 2, Social Worker) I feel like it should be more sort of a smaller team who deals with you and they send on a regular basis. That's personally how I feel … but there's definitely a lot of different people. Whereas me, especially with COVID, I think it should have dropped to a smaller bubble if you get me. (Informal carer 5) …one thing that [our son] needs to have is regular carers, because otherwise he struggles. So he … like we said at the beginning of the discussion, we’ve got a core set of carers who come regularly … and a few more that are starting to come, but having … having that core caring group has been harder over COVID obviously because people have their own … they have to look after themselves, and obviously they have their own … they have to look after their own health and everything else. (Informal carer 4)
Social isolation
Participants identified social isolation as an issue associated with the COVID-19 pandemic. During the lockdown, many of those using the home care service were in the shielding category and were not going out or having visitors into their homes, and this often included visits from family members. They were however still having contact with the home care staff, but this service was often over-stretched with staff off sick, isolating, or shielding. Consequently, visits during lockdown were often focused on the provision of personal care rather than social interaction: …so I think that affected people's wellbeing because they were getting the basic care needs met, but not having any social interaction or social support, so that … that was what didn’t go so well. (Formal carer 9, Social Worker) So I … when I’ve gone round, I’ve said come on let's go and have a coffee in the garden. And we’ve walked out and sat in the chair. But she's frightened to go out on her own. And she knows she needs to exercise. But she's … she's frightened. (Informal carer 2)
Provider perspective (group 1)
In group one, nine social care workers were interviewed: Six arranged or commissioned the care (Social Workers, Domiciliary Services O-rganizer, and care agency manager), and three provided direct care in the home (carers and Personal Assistants).
Pandemic stressful for formal carers
The lockdown created specific challenges for the home care service. The majority of formal carers spoke about the pandemic causing them stress, some in their working lives and some in their home lives, and in many cases in both. This spanned across the entire field of workers, including those directly providing the care, and those organizing and commissioning home care services:
The Social Workers spoke about the stress of organizing home care services without seeing the recipients face-to-face. This lack of face-to-face contact challenged their professional values and ethics: …but I think the fact is that a Social Worker by it's very nature is to be social and be … be there. We … we’re not being allowed to be there. And I think we … we … we worry that the power we have as a Social Worker, which we often use to engage those vulnerable people is being … well is … it's not important right now. And it's been … it's been hard. It's been very hard, emotionally. (Formal carer 1, social worker) Do you know what scares me? I … I keep … I kept saying that if I felt that one of mine passed away due to catch … if I caught it and not known that I’d got it and … and then I found out I did have it, it would make me feel awful thinking was it my fault? Did I kill them?… And that was always in the back of my head. And there were moments, you know, I just remember sitting down a few times, getting myself all upset thinking you know if … if they was to get it, you know, that would make me feel awful if it was my fault. (Formal carer 7, personal assistant)
Carers felt forgotten/overlooked during lockdown.
Despite working in stressful conditions throughout the lockdown the majority of the formal carers spoke about feeling forgotten or overlooked. They contrasted this oversight with the public recognition given to National Health Service (NHS) and residential care staff: …and I felt a bit annoyed that it was about protect the NHS. Well actually, the NHS was exceptionally protected. But social care not so much. Not so much. So again it … you know, I think you know sadly social care is … is known as a poor cousin of the Department of Health. You know, the NHS is … is a big monster. One we do try to work with, but ultimately the NHS will … will you know … takes a bigger part of people's perception. (Formal carer 1, Social Worker)
Recipient perspective (group 2)
Loss of control
The home care recipients and informal carers experienced a loss of control over their daily lives in relation to their reliance upon the home care service. They spoke about a lack of control over the safety precautions being taken by staff visiting their homes: I mean not even wearing aprons and stuff, you know what I’m saying? I could see, because they’re obviously coming into your house without an apron on and stuff. (Informal carer 5) …they came at tea time which is one of the comments my Mum made was, that was to put her to bed and they wanted her to go to bed at six o’clock at night. She's a bit of a night bird. So they were trying to get her ready for bed at six o’clock and she didn’t want it…. (Informal carer 2) …it's just stress and worry, because today I … I’ve not felt like I can go out, you see, because it's happened. I know all the toileting you see, will be out of synch, you see. So today I don’t feel like I can nip anywhere, because I know probably outside of time calls, you know what I’m saying, she’ll be wanting the toilet. She’ll want … which will mean I don’t feel that I can go out today you see. (Informal carer 5) But it's very restricting because you can’t … if you go out, you’ve got to be back. They were coming in at six o’clock to put her to bed. Six o’clock in the evening. And … and it's quite early, and they weren’t very flexible, so it was … I was a bit disappointed about that but we worked round it. (Informal carer 6) …the last time they (Social Worker) said, oh, give them a bit more time. Give it two weeks. But they … I get the impression they don’t really want to do anything … that's why I’m going to try and take this formal complaint and see where I stand. Because I don’t want to shoot myself in the foot by going off on one, and them just cancelling the care. (Home care recipient 3) And as soon as you decide if you’re not happy with something it's like they … they punish you in other ways for saying speak up sometimes, as silly as it sounds. We’ve noticed, haven’t we? They’ll do something like, your times the next week. I’ve found that before, if they say where they’ve done it to be like a bit vindictive, to be honest. You know what I’m saying? (Informal carer 5)
Themes.
Participant recommendations
Finally, the participants in both groups were asked, based on their experience of practices that worked well or less well during lockdown, for their suggestions and recommendations on how to improve home care practice. Their recommendations were focused at service and management level and included the need for more investment in home care. This investment included the need for staff training, to improve job satisfaction, retention and care: So you have to look after your staff. Invest and value them. And that is the starting base, or the starting baseline, to deliver good care. If your staff members feel valued, that their pay reflects what they do, work life balance is balanced … that's a good place to start, you know, to be reassured as an organisation or a provider that you’re going to … that the end place, the delivery of care, the person that's receiving care, is going to get some good quality care. (Formal carer 3, care agency manager)
Discussion
This study managed to record real-time experiences of those organizing, commissioning, providing, and receiving home care during the COVID-19 pandemic. It is perhaps not surprising that participants were fearful of catching the virus from home care staff. To put this into context, at the time of this study, England was experiencing the second wave of the pandemic. The East Midlands, the focus of this study, had the third highest rate of deaths across England and Wales (Office for National Statistics, 2020). The health service was under enormous pressure with rocketing emergency department waiting times and increased patient admissions to intensive care units (BMA, 2023). An earlier UK home care study, conducted during the first wave, similarly found that people living with dementia and their informal carers feared the risk of transmission from paid carers coming into the home (Giebel et al., 2020). The current study supports this, whilst showing that fear amongst home care recipients is present on a much wider scale.
The home care recipients spoke about the lack of control they perceived in relation to the timing of visits. Unreliable visits can affect the home care recipient's plans for the day (Hughes & Burch, 2020). Other studies have similarly identified that reliability and punctuality are attributes valued by home care recipients and their informal carers (Francis & Netten, 2004; Fraser et al., 2014; Pollock et al., 2020). During the pandemic, this loss of control was not unique to those receiving home care services. Giebel et al. (2021a) examined the effect of social support closures, and similarly found that the recipients, people living with dementia and their informal carers, experienced a loss of control. The current study reveals that even when services continued, such as the home care service, the interruptions to the service still resulted in feelings of loss of control.
Perceived control relates to how much an individual feels that they are in control of their own actions and have influence over events around them (Robinson & Lachman, 2017). This perceived lack of control, by those in the current study, is not unique to the pandemic. Studies prior to the pandemic have found that older people struggle to maintain control over their own environment when receiving home care (Hughes & Burch, 2020; Jarling et al., 2018). One study found that older people, receiving home care, felt like a guest in their own home, and had needed to adapt their own routines around the caregivers. Their daily routine became structured and inflexible with no control over when to complete daily activities (Jarling et al., 2018).
The home care recipients in the current study were already fearful of catching COVID-19 and were socially isolated. Both were likely to affect their mental well-being. A perceived loss of control has been associated with increased rates of depression and low mood (Halse et al., 2021), as well as decreased levels of social interaction in older adults (Curtis et al., 2017). Therefore, the inability of participants who receive care to control the time of carer visits or routines may lead to worsening health, social interaction and independence. This is an area that home care needs to focus on. Indeed, in the UK, the National Institute for Health and Care Excellence (NICE) which publishes guidance for health and social care services has highlighted the importance of reliability in its 2015 guidelines for home care providers.
The unreliability of visits also had an impact upon the informal carers, creating rather than reducing informal carer stress. Increased burden has been shown to have an impact on informal carer health and well-being (Carers, 2020a; Eide et al., 2021; Giebel et al., 2020, 2020b, 2021; Lorenz-Dant & Comas-Herrera, 2021).
The home care recipients and their informal carers not only valued reliability, but also highlighted the importance of a small number of staff visiting them, and it was one method suggested to reduce the risk of catching COVID-19. This strategy also has the advantage of providing continuity of care which has been identified as an important attribute of good home care prior to the pandemic (de Sao Jose et al., 2016; Edebalk et al., 1995; Francis & Netten, 2004; Fraser et al., 2014; From et al., 2009; Hughes & Burch, 2020; Lorenz-Dant & Comas-Herrera, 2021; Pollock et al., 2020).
One advantage of staff continuity is that familiarity with recipient routines has been found to free up time for social interaction (Hughes & Burch, 2020). Socialization has been recognized as an important element of home care visits (Fraser et al., 2014; Hemberg et al., 2019; Hughes & Burch, 2020; Pollock et al., 2020) and is often valued as much as the practical tasks being completed (Hughes & Burch, 2020; Pollock et al., 2020). Participants in the study spoke about the special nature of home care staff and particularly valued those who spent time talking to them. Allocating consistent carers has the advantage of enabling relationships to develop, and ultimately this leads to the home care recipient having a greater sense of control (Hughes & Burch, 2020).
The pandemic was also stressful for those organizing, commissioning, and providing care. Many of those continued to go into recipients’ homes during the nationwide lockdown. Although they were valued by those in receipt of their services, they felt undervalued by the public. Their front-line role made them vulnerable to infection and death (Nyashanu et al., 2022; ONS, 2020), and even if working remotely, such as Social Workers, their relationship-based practice was affected (Ravalier et al., 2023). These staff have continued to experience increased levels of stress and poorer psychological well-being since the pandemic (Ravalier et al., 2023). Despite the stress of continuing to work through the pandemic, the formal carers in the current study felt overlooked compared to their NHS counterparts. This has been reflected in another UK study of private care home workers and home care workers (Nyashanu et al., 2022).
Limitations
The findings need to be viewed within the limitations of the study. It was completed in one geographical location of the UK and there were recruitment difficulties. The sample size was small with only nine formal carers (split between those organizing or commissioning care and those providing the care), six informal carers, and three homecare recipients. This necessitated utilizing a convenience sample. Temple (2002) argue this is an acceptable method of sampling for hard-to-reach groups. None of those interviewed were from ethnic minority backgrounds, and this has been recognized as a limitation in other home care studies (Giebel et al., 2021b, 2021; Hughes & Burch, 2020). Furthermore, many of the interviews were short and this would have reduced the depth of information gleaned.
Telephone interviews further restricted access to home care recipients with hearing loss quoted as a reason for declining interviews. The use of Voice over Internet Protocol technology (VolP) may overcome these problems and is recommended for any such future research.
Implications and future research
The findings of the study highlight the importance of continuity of staff in home care services. This has long been recognized as an important element of the home care service (de Sao Jose et al., 2016; Edebalk et al., 1995; Francis & Netten, 2004; Fraser et al., 2014; From et al., 2009; Hughes & Burch, 2020; Lorenz-Dant & Comas-Herrera, 2021; Pollock et al., 2020). However, in any future lockdowns, continuity also has a part to play in reducing the number of staff visiting home care recipients and thus reducing the risk of infection. This may encourage recipients, fearful of infection, to continue with their service during such a crisis. This will ultimately reduce the burden on informal carers. Also highlighted was the frustration around the timing of home care visits. This led to home care recipients, and their informal carers, feeling that they lacked control over their daily lives. During a national crisis, it is difficult to maintain a service, especially when staff are off sick or isolating, however, communication needs to be improved so that recipients and informal carers can make plans around any changes to their service.
The formal carers felt overlooked and poorly credited for their efforts, compared to NHS staff. This reflects a larger problem in social care. In the UK, the public holds a negative perception of social care, perceived as second class to the NHS. The Institute of Health and Social Care Management (2021) has recognized this issue in its People Plan. They have put forward a series of recommendations to raise the public profile of social care. Increased awareness and understanding of social care is necessary to improve recruitment and retention of staff. Ultimately, increased staffing levels will enable home care services to provide continuity of staff and a reliable service.
Finally, social care in the UK has recognized the importance of drawing upon research evidence, both the lived experience of those using the services, and also the practice wisdom of those providing the care, through the development of IMPACT, a UK center for implementing research (Health Foundation, 2021). The current study focused on the experiences of those arranging, commissioning, or providing home care and those in receipt of the service during the pandemic. It identified what was important to these groups during a time of crisis. There is a need for research now to identify what home care should look like during times that are more “normal.” However, the current study experienced recruitment difficulties. The challenge will be to hear the voice of this hard-to-reach group.
Conclusion
Providing home care services was difficult during the COVID-19 lockdown period in the UK. Whilst the extent of these pressures was new, the pandemic compounded challenges that were already within the sector. In this study, home care recipients were seeing multiple care workers and often receiving visits at inappropriate times. The pandemic resulted in visits being rescheduled or cancelled due to a lack of staff availability, worsened by sickness and the need to isolate. Continuity of care is recognized as important in the NICE Guidelines (2015), but this is a sector that struggles with recruitment and retention of staff, and this needs to be addressed, especially in times of crisis, if continuity of staff is to become a reality. However, recruitment will only improve if the negative image of social care is addressed.
Footnotes
Ethical approval
Ethical approval for the study was provided through the West Midlands-Black Country Research Ethics Committee 20/WM/0218 on July 27, 2020.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the NIHR Applied Research Collaboration East Midlands (ARC EM), Building Community Resilience and Enabling Independence (BCREI) theme. Project number C4. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Declarations of conflict of interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ contributions
Janet Darby and Fran Allen were responsible for the day-to-day progress of the study. They devised the interview schedules, conducted the interviews and data analysis, and drafted the paper. Cate Bennett was the Local Authority stakeholder, contributed to the stakeholder meetings, accessed the Local Authority databases, and assisted with recruitment. She also contributed to the draft papers. Chibeka Kasonde completed data analysis, contributed to the stakeholder group and to the drafts of the paper. Pip Logan was the Principal Investigator, contributed to the stakeholder group and edited the paper.
Acknowledgements
The authors acknowledge the following for their contribution to this article: We would like to acknowledge Anita Pashley, PPI partner, who provided advice in our stakeholder group.