
Abstract
Summary
Mentoring is an intervention aimed at strengthening social networks of individuals by providing one-to-one support to develop a social network. While there is a lack of insight into how the social network intervention “mentoring” affects health outcomes, we used a realist evaluation approach to find out for whom and under what circumstances mentoring affects health. The study was conducted in the Netherlands. In phase 1, an initial program theory of mentoring was developed based on a group interview with participants and professionals engaged in mentoring, complemented by documents (previous studies, descriptions of interventions). In phase 2, the program theory was tested using interviews with 23 participants before and 16 after mentoring.
Findings
Mentoring strengthened the social network when two conditions were met. Firstly, mentoring coaches needed to be trained. Secondly, participants needed to have a pre-existing—albeit small—network and need to have some social skills. If the social network was strengthened, mentoring increased self-esteem and self-confidence and decreased experiences of depression and loneliness of participants through three mechanisms: (1) participants were acknowledged and their individual needs were accepted; (2) individual coping resources were improved; (3) capabilities to initiate the search for a social network and to be involved in a social network were realized.
Applications
Mentoring is a useful intervention to increase self-esteem and self-confidence and decrease experiences of depression and loneliness of participants if the two conditions are met. Therefore, mentors should be carefully trained to acknowledge and respond to participants’ individual needs for social bonds.
Introduction
Having a strong social network is associated with good health as it impacts favorably on longevity (e.g., Holt-Lunstad et al., 2010), self-rated physical health (e.g., Cornwell & Waite, 2009), and mental health (such as fewer symptoms of depression; e.g., Cornwell & Laumann, 2015), well-being, and quality of life (e.g., Tomaka et al., 2006). In contrast, a lack of social ties is associated with poorer physical and mental health and unhealthy lifestyles (e.g., Richard et al., 2017). These empirical findings are confirmed by theoretical models of how social networks impact health, in which not only the provision of social support through the network plays an important role, but also social influence, attachment, and access to resources through the network (Berkman & Glass, 2000). These empirical findings as well as the conceptual models imply that developing and maintaining a social network can be an important strategy to improve health. However, building and maintaining a social network is difficult for many people. For example, 10–30% of the population in Europe report feeling lonely and being in need of connection with others (e.g., Richard et al., 2017). In the Netherlands, 10% of the population feel very lonely (CBS, 2020).
The potential of social networks to improve health behaviors and outcomes is still “largely untapped” (Hunter et al., 2019), and researchers are increasingly interested in understanding the effects of interventions that can change networks and thereby change health behavior and health (Hunter et al., 2019; Valente, 2012).
Social network interventions are interventions that use social network characteristics to change or enhance health behavior and favorably influence health outcomes (Valente, 2012). There is some evidence of the effectiveness of social network interventions for some specific health outcomes, for instance, social support, glycemic control, and quality of life in patients with type 2 diabetes (Spencer-Bonilla et al., 2017), and for general health outcomes including sexual health, well-being, and smoking cessation (Hunter et al., 2019).
However, to understand the full potential of social network interventions, there is a need to further explore the effectiveness of such interventions for other health behaviors and outcomes (Hunter et al., 2019), such as mental health or quality of life. There is also a need to further investigate the mechanisms by which social network interventions work and to understand why they work and for whom, to maximize their effectiveness so that they can be effectively implemented, for example, in the community (Hunter et al., 2019).
One promising intervention that aims to improve people's social networks is mentoring. Mentoring is the provision of one-to-one support by a volunteer to a community member to help this person strengthen their social network. The level of support offered by the mentor is generally variable and responds to the participants’ perceived needs. It has been defined as a “unique learning partnership” offering either emotional or instrumental support, with mentors reducing the level of support over time as appropriate (see Dickens, Richards, Hawton, et al., 2011; Dickens, Richards, Greaves, et al., 2011). Mentoring is often initiated, supported, and monitored by an agency in the community, and usually lasts about 1 year (Thompson et al., 2016). In the Netherlands (Goede & Kwekkeboom, 2013) as well as in the United Kingdom (Dickens, Richards, Hawton, et al., 2011; Dickens, Richards, Greaves, et al., 2011; Philip & Spratt, 2007), mentoring is used by social work organizations, such as charitable and voluntary sector organizations.
Quantitative evaluation studies of mentoring have predominantly focused on people with severe mental health problems (Anderson et al., 2015; DuBois et al., 2011; Mann et al., 2017; Webber & Fendt-Newlin, 2017) and showed that mentoring has a moderate effect on physical health and a modest effect on depressive symptoms and emotional distress in mentoring participants. There are indications that mentoring works for older, socially isolated people (Dickens, Richards, Hawton, et al., 2011; Dickens, Richards, Greaves, et al., 2011) when it is tailored to participants’ needs, a key underlying process being the building of confidence and self-efficacy. These results were found only in the pilot study and were not replicated in a follow-up study.
We thus generally do not know whether mentoring works for people who are not in professional mental health care, but who still present with distress because of social, physical, and economic problems. This is an important issue, as these individuals may particularly benefit from mentoring by charitable and voluntary sector organizations, supporting them to develop a social network within their local community, without medicalizing their difficulties (Middleton & Shaw, 2000). Mentoring in the daily context of social work aims to assist people who are in temporary need of support, including family caregivers, single parents, bereaved spouses, or unemployed persons who find themselves without a social network because of the social or economic conditions they are in. Mentoring schemes may even be more important during and after the COVID-19 lockdown, as the lockdown has increased feelings of loneliness in the Netherlands, and most likely in other countries as well. For example, the number of elderly people who feel lonely in the Netherlands has doubled since the lockdown (SCP, 2020).
In this article, we therefore want to address the following questions: what are the possible mechanisms that explain the effect of mentoring on experienced health, and for which populations is mentoring most effective in the daily context of social work?
Methods
The mentoring intervention
In the Dutch intervention called “Of course a network mentor!” (in Dutch: “Natuurlijk een netwerkcoach!”), participants are matched for a period of 9–12 months with a voluntary mentor who helps them strengthen their social network. The intervention generally targets all vulnerable citizens in the communities addressed by the social work organizations who wish to strengthen their social network. The intervention is described in the Dutch databank “Effective social interventions” (see https://www.movisie.nl/interventie/natuurlijk-netwerkcoach [only in Dutch]).
The ultimate aim of mentoring is a stronger social network as perceived by the participant. Social networks are generally defined as the web of ties that surrounds a person and the characteristics of those ties, such as frequency, size, density, and heterogeneity (Berkman & Glass, 2000). Thus, social networks may include close, supportive relationships with family and friends, as well as more spontaneous, casual interactions with persons in the community. The key feature of the mentoring intervention is self-regulation (Storms, 2016), which means that the mentor supports the participant during the mentoring period, but the participant decides which actions will be taken and when. This also means that it is the participant who decides whether the social network has strengthened after the mentoring intervention.
The mentoring intervention starts with an intake interview by a social work professional, often the coordinator of the program in a social work organization (Storms, 2016). The coordinator matches the participant with a volunteering mentor. The coordinator also supports the volunteering mentors by means of periodical supervision. During mentoring, participant and mentor generally meet for 1–2 hours every week or every fortnight.
Mentors are generally volunteers from the community with an interest in helping others. Sometimes mentoring is also done by social work students during their internship at the organizations. Mentors do not need to have a particular level of previous education or training but are selected if they are motivated and if, in the eyes of the coordinator, they possess competencies such as being able to listen and being able to coach rather than trying to solve problems themselves. Other competencies that coordinators take into account when engaging mentors are patience, resilience, openness to people from different backgrounds, and being able to work together with professionals. Once selected, mentors receive a training course by the coordinator or from the organization that developed the intervention. In this course, mentors are taught 10 steps to guide participants in strengthening their network, using several techniques, including communication techniques, which, for example, help to describe the participant's network or enable the mentor to listen to the participant without judging. These 10 steps take the participant through three phases. In the first, the mentor helps the participant describe his or her existing social network. In the second, the mentor helps to identify activities, interests, or needs that the participant thinks may help to enlarge the social network. Finally, the participant engages in the activities or interests thus identified, while being coached by the mentor.
Design
The difficulty of evaluating mentoring is that, like most social network interventions, it is highly context-dependent. Whether mentoring works to strengthen a social network and whether it has an effect on health is closely related to the decisions and actions taken by the participants, as well as to their needs and the activities they would like to engage in during the mentoring period. Therefore, we used a realist evaluation to evaluate mentoring. Realist evaluation is a theory-driven method of evaluating complex interventions and is based on the idea that an intervention works because participants make certain decisions or act in a certain way in response to the intervention. This research approach offers a useful framework as it aims to answer the question “What works, for whom, in what respects, to what extent, in what contexts, and how?” (Pawson & Tilley, 2004), whereas the usual evaluations merely aim to investigate whether the intervention works. Realist evaluation explicitly uses existing theoretical knowledge to build upon, and starts from a set of hypotheses which is called the initial program theory. We conformed to the RAMESES standards for reporting about realist evaluation (Wong et al., 2016).
Phase 1: Initial program theory
In the first phase of our realist evaluation, we developed an initial program theory to explain what makes an intervention work (mechanism), under what conditions (context), and what the effect is (outcome). As some contexts will be supportive while others will not (Pawson & Tilley, 2004), an initial program theory is able to describe different context–mechanism–outcome configurations (CMO). Context refers to the features of participants, organizations, staffing, etc. (i.e., “for whom” a program works as well as a specific organizational setting or key attributes of mentors) that are required to “fire” the mechanism. As a consequence, countervailing mechanisms can also be distinguished, that is, specific aspects of the context that prevent the mechanism from “firing.”
To develop our initial program theory, we scoped published and gray literature and interviewed several stakeholders in two group interviews in March 2015: one interview with a convenience sample of four participants of mentoring and one interview with a convenience sample of four providers of mentoring (one mentor, two coordinators, and the developer of the intervention). All respondents were from the same welfare organization in a small town in the Netherlands, and the coordinators were approached through the network of the developer of the intervention. The coordinators in turn approached the mentor and the participants. Respondents were selected because of their willingness and capability to reflect on the mentoring intervention.
The literature and the interviews were qualitatively analyzed, allocating codes to fragments and comparing and combining codes into meaningful patterns (Miles et al., 2019). From these data sources, we iteratively identified three key mechanisms: personal contact, coaching contact, and exploring and maintaining a social network.
The first CMO was based on the theory of Honneth (1995), who hypothesized that the extent to which an individual is included as a unique and irreplaceable member of a social community results in human flourishing and personal well-being. The mentor can enhance well-being (Heaney & Israel, 2008) and reduce loneliness by meeting basic human needs for recognition, companionship, intimacy, a sense of belonging, and reassurance of one's worth as a person. We based the second CMO on the coping theory of Lazarus and Folkman (1984), who hypothesized that supporting people to improve their individual coping resources can enhance their ability to access new contacts and information as well as to identify and solve problems. These improved coping resources may have direct health-enhancing effects (e.g., a sense of personal control) and may also diminish stress (Heaney & Israel, 2008). The third CMO was based on the capability approach, hypothesizing that when voluntary mentors recognize and cultivate participants’ capabilities to search and experience inclusion in a new social network, capabilities such as being self-aware and self-directing, and participating socially in a group or community, can enhance mental health (Entwistle & Watt, 2013).
Phase 2: Testing the program theory
In the second phase, we tested which CMO configurations offered the most robust and plausible explanation of the observed effects. In addition, in this phase, we also studied for which groups the intervention was most effective. We used a convenience sample to recruit respondents in the 2015–2017 period. From the developer of the intervention, we received a list of about 20 welfare organizations that were using the mentoring intervention. We invited them by mail, and five welfare organizations agreed to join the study, one of them being the organization that participated in phase 1. Four of the five welfare organizations were based in large cities in the Netherlands, one in a small town. The five welfare organizations implemented the intervention as described above with a coordinator and trained volunteers, all using the same methodology. One welfare organization specifically focused on individuals with psychiatric problems, the others focused on all citizens who felt a need to strengthen their network.
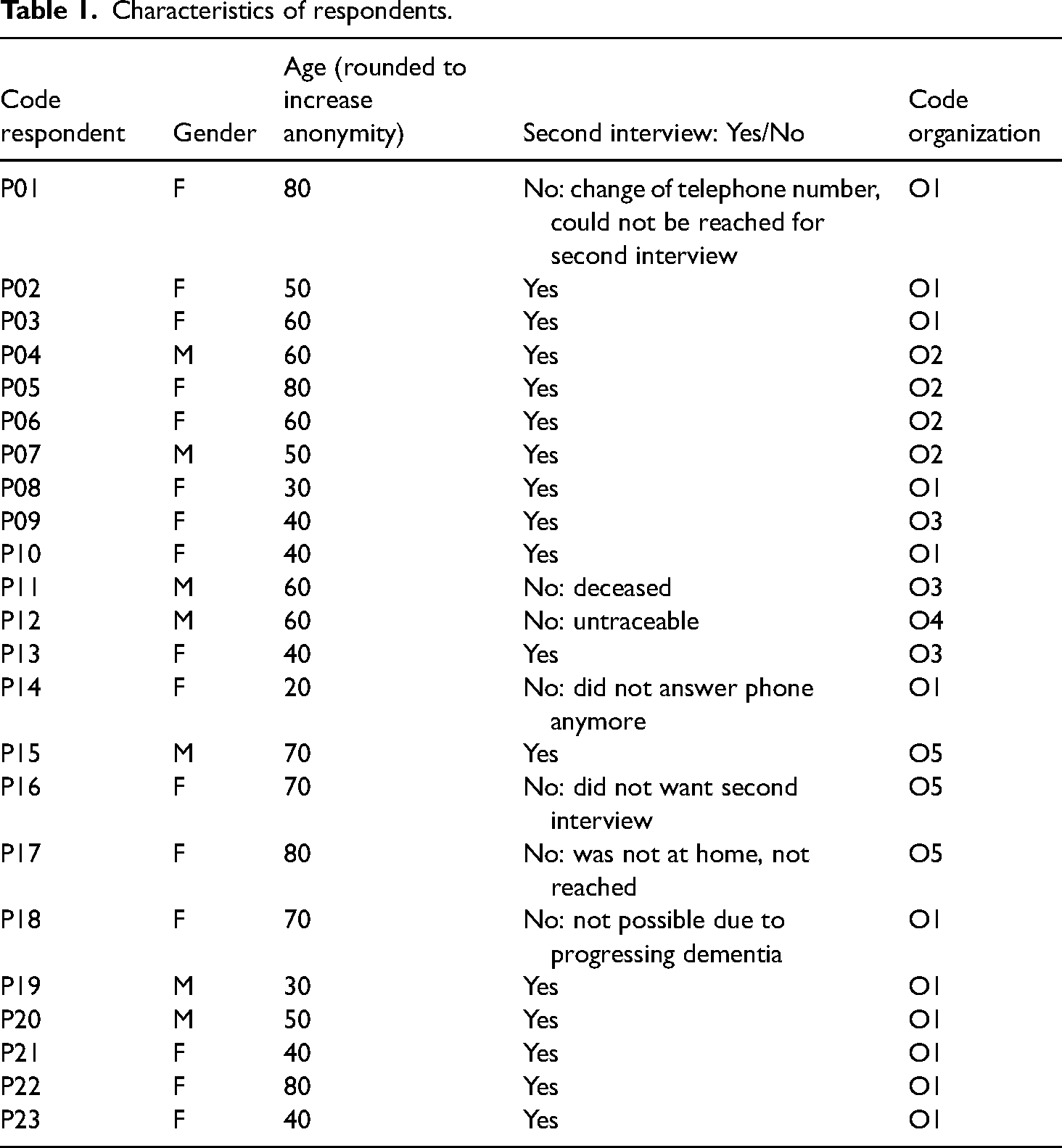
Through these five Dutch welfare organizations, we approached participants who had recently started a mentoring trajectory. After written consent, participants were interviewed at the start of the mentoring trajectory and 9–12 months later, when they had completed it. All participants received two 10-euro gift vouchers (1 for each interview). Interviews were held at respondents’ private homes, according to the respondents’ preference, and took between 45 minutes and 2 hours. We ended the recruitment of respondents when no new themes were identified in the data and when theoretical saturation was achieved, which was after we had included 23 participants. For the interviews, we used a semi-structured topic list, including questions about the size of the social network before the mentoring started, experiences with mentoring, perceived effect on well-being and health and perceptions about the way mentoring had contributed to their social network.
Fifteen of the participants were female and eight were male, and their age ranged from 20 to 80 years (see Table 1 for characteristics of the respondents). About half of the participants lived in a large city, while the other half lived in a small town. Most of the participants did not have paid work, but some of them were engaged in voluntary work. At the end of their mentoring period, seven of the 23 participants unexpectedly dropped out and were not interviewed for the second time. Reasons for dropping out included the following: one participant died, one participant suffered from progressing dementia, one participant was not traceable, neither by the researchers nor by the mentor or the welfare organization, one participant did not want to be interviewed anymore, and three participants did no longer answered their telephones.
Characteristics of respondents.
Data analysis
The interviews of both phase 1 and phase 2 were audio-recorded, transcribed, and analyzed, using a framework approach, involving a content and thematic analysis strategy (Pope et al., 2000; Ritchie & Spencer, 1993). This approach involved a systematic process of sifting, charting, and sorting material according to key issues and themes. First the interviews were read and reviewed carefully. This familiarization stage yielded an overview of the richness and diversity of the data, and started with the process of abstraction and conceptualization. While the data was being reviewed, short notes were made about the range of responses to our questions, as well as about recurrent themes and issues that seemed to be important to respondents. Once the material had thus been reviewed, the first author identified key issues and themes in these notes, which were used to examine the data. This resulted in a thematic framework by which the material was sifted and sorted. This framework was extended with a priori defined issues such as the three CMOs. In the next stage, the framework was systematically applied to the material, and all interviews were reread and annotated accordingly. Charts were devised with headings and subheadings for each key subject area, and entries were made for several respondents on each chart. The coding was done manually by the first author. Finally, these charts enabled patterns and connections to be described using an iterative and comparative process of searching, reviewing, and comparing the data. To increase its rigor and to identify possible discrepancies, this analysis was discussed with the two other authors and was then further refined. To further increase the rigor, we used the method of member-checking and discussed the results in a group interview with four participants who had completed the mentoring and two coordinators. The participants (two men, one woman) and coordinators (two women) were from the same welfare organization as the participants and coordinators who had been interviewed in phase 1. The participants were selected and approached by the coordinators, the selection being based on their ability to reflect on mentoring, according to the coordinators. The interview was audio-taped, transcribed, and analyzed, and the results confirmed the program theory.
Phase 3: Refining the initial program theory
The three CMO configurations from phase 2 were compared with the initial program theory of phase 1, which was modified using the findings from phase 2.
Results
The analysis of the data confirmed but also refined the mechanisms included in the initial program theory and added insights regarding the groups for whom mentoring was most effective. Below, we first discuss the final program theory with the three mechanisms that were substantiated and refined and then discuss for whom the three mechanisms were working. See Figure 1 for the final program theory. The quotes that are used to illustrate the mechanisms were selected because they represented examples of how a mechanism works best.
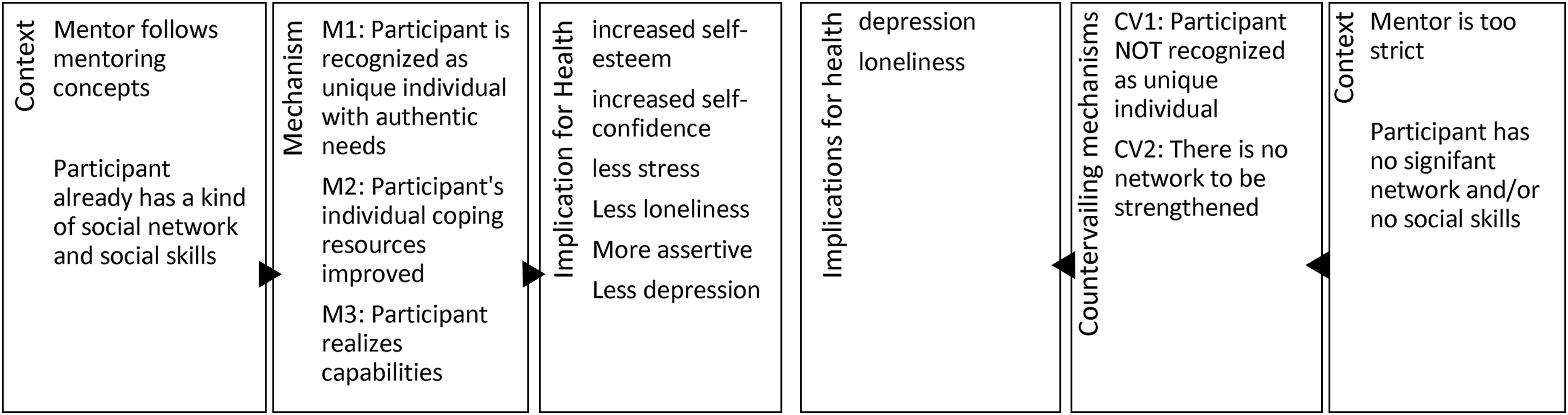
Final program theory.
CMO 1: The fact that mentoring recognizes participants as unique individuals with authentic needs enhances health (increased self-esteem, less stress, less loneliness)
Many participants described that mentoring started with being acknowledged, recognized, and respected as an individual with authentic needs and desires. As one participant explained: I just had a very good mentor. For me he was just right [laughs]. [Interviewer: And what made him right for you?] He just really listened to me. He did not offer tips or advice. He doesn’t know what is best for me because he is another person. [P09]
According to most participants, mentors explicitly confirmed their worth as a person or supported them to see their own worth, for example: What most helped me, I think, was that the mentor helped me to understand that I need to think about myself, arrange things for myself, enjoy it. [P21]
In the eyes of many participants, this confirmation of their worth increased their self-esteem. For example, when asked what the mentor had meant for her after the mentoring had come to an end, a participant observed: Just a little self-esteem. The mentor said: “You are a nice woman”. Well, yes, then I’m a nice woman. Whereas before mentoring, I used to think: “I’m tired, who is going to help me?”. [P13]
This acknowledging contact with the mentor also offered opportunities for companionship, thereby decreasing loneliness. For example, the next participant reflected that the mentor was there for her during a long period of illness: [Interviewer: How was [mentoring] good for your health? How did it support your health?]
It's always better than feeling totally isolated. Because that's when you start to feel lonely. Especially when you’re ill. […] For instance, when I had to go to the hospital for a check-up, I would receive a text message [from the mentor] while I was on my way to the hospital or when I came home. […] He was very considerate, yes, he didn't forget that. [P06]
CMO 2: The fact that mentoring improves participants’ individual coping resources enhances health (increased self-confidence, decreased stress)
Participants generally described the next step in mentoring as a step to improve their individual coping resources; the mentor helped them to identify why they had difficulties developing a social network and offered them coping strategies to deal with this. One important coping strategy that mentors offered was positive reappraisal: several participants described their improved coping with problems related to developing a social network, because the mentor helped them to take a different look at these problems. By doing so, participants felt more confident about future contacts with other people. For example, one participant who described herself as very insecure in contacts with other people felt reassured when the mentor pointed out that this is a common problem for many people: He gave me certain insights and he disclosed how he saw me. […] He used to tell me that my insecurity … is something an awful lot of other people have. [P03]
Another coping strategy mentioned by several participants was that the mentor helped them redefine stressful situations. This advice was generally given with the idea that less stress in a participant's life results in more opportunities for finding a social network. For example, mentors advised participants to think more positively or try not to be annoyed when something stressful happens, such as stressful situations at work or daily nuisances such as computer problems. Participants continued to use this strategy also after mentoring was over. For example, one participant was always stressed by daily nuisances such as the traffic when he drove his car: Now, when something happens, I always think: “what would the mentor say?!” [P20]
A final coping strategy mentioned by several participants was that by discussing difficulties regarding friendships or family, mentors taught them to deal with their social network by “setting boundaries” or learning to be more assertive in contacts with others. For example, one participant described how the mentor had helped him address these problems: I often feel I’m a burden to other people, and I forget to think of myself, which I shouldn’t do. [Interviewer: And these are things you discussed with your mentor?] Yes, she always stressed that I should not forget to think of myself. [Interviewer: And did that help?] Yes quite a lot. That I need to say more “I”. [P19]
Having these new coping strategies in their life gave many participants more self-confidence and motivation to pursue new activities. For example, when asked what mentoring had done for his health, the same participant answered: Yes, mentally quite good. [Interviewer: And what do you mean by that?] Respondent: Well, more self-confidence, more assertive. [P19]
Other participants experienced less stress because of the new coping strategies. For example, a respondent said that the mentor had helped her to be more assertive and that this helped her take better care of her own needs, which decreased her feelings of stress: I went to the doctor with complaints about pain in my shoulder, with pain radiating towards my heart and towards my back, and then I said, yes, I think I have heart problems or something. […] And then the doctor said it's just stress and that causes you to have complaints. And if you don't do something now, you'll have even more complaints later. […] And that's why I take it [the advice of the mentor to set clear boundaries toward other people] really seriously, so I think yes… I have to take better care of myself, start thinking about myself too. [P21]
CMO 3: The fact that mentoring enables participants to realize their own capabilities to strengthen their social network enhances health (increased self-confidence, less loneliness, less depression)
When participants felt they had acquired sufficient coping skills to deal with possible barriers in developing a social network, they described the final step as one where the mentor had helped them explore and realize those capabilities that they thought were necessary to develop and be included in a social network. In the next quote, a participant with physical disabilities who felt very lonely in the small town she had moved to 18 months before, described the most important change after mentoring, in terms of renewed awareness about self-directing possibilities: A while ago I said to myself: I’m going to do my best to build something sustainable here [in the new town]. And by that I mean to explore my possibilities for work, but also simply to explore how I can solve things, get a social network and really make this town my home. […] And before [mentoring], I simply didn’t see it that way. [P23]
This participant, like several others, felt activated by the mentor to initiate activities to strengthen a new social network. Participants felt it was very important that the mentor helped them explore their capabilities and initiate actions that fitted their needs, rather than simply suggesting possible ways of finding a social network: She [mentor] doesn’t ask, okay, what are your hobbies and what do you want to do? She also looks at the bigger picture: what is your personal situation, what kind of person are you. For example, a while ago I used to do volunteer work, and it drove me crazy, it just took over my life, I had to do more and more work. I simply collapsed. And my mentor said: “saying no” is not your strongest point. (…) So it's not about: ”Oh you like painting? Well let's do that.” She helps me explore what things make me happy in the long term. [P23]
By listening to what the participants themselves thought was important, the mentor not only gave them practical advice, but more importantly, instilled in them a sense of being someone who matters and who deserves being listened to, as is hypothesized in the theory of the capability approach. As a result of the way the mentors listened to them, many participants experienced self-confidence, self-esteem and happiness, for example: It is so nice that someone listens to you and gives you advice, such as “You should simply dare to ask people.” It gave me a boost of self-confidence. I am now the one who is listened to and it feels strange but also wonderful. So now I’m at a point where I invite people to my home. [P21]
Several participants mentioned that the activities they had engaged in—supported by their mentors—resulted in less loneliness and depressive feelings: I believe that if you’re sad, that mentoring makes you feel less depressed, that it does something to your mind. [..] Also because of the things you do and experience. And that you’re not alone, it's being in the company of other people, you experience similar things so to speak and then you share something and I think that has a good influence on everything. [P21]
In retrospect, for many participants, it was not only having a strengthened network that turned out to be important, but also the realization through mentoring that they had become self-confident and self-directing in developing a social network, as well as participating socially in their network: Yes it [the social network] is more or less the same, but I think that I can now show more positive sides of myself. [P03]
She [the mentor] actually said: you don't need me at all. She said: I am a mentor for other people too, and if it's their birthday then one or two people come to visit. And she said: You have 45 persons on your birthday. She actually says you don't need me at all, she says. She says I understand that you want something to do during the day, but in principle, your network is so large, she says, even though they are located throughout the Netherlands, but you can call someone and they are there for you. So in that respect I’m also very rich. I can’t complain. [P10]
What works for whom and why?
After their period of mentoring had come to an end, many participants felt they now had a stronger social network, mostly because they had strengthened social ties with old friends or strengthened existing ties with neighbors, parents from their children's school, or with fellow volunteers (e.g., from a community vegetable garden). However, there were four interviews where we did not find these mechanisms, but found two countervailing mechanisms. One countervailing mechanism opposes mechanism 1 (recognition of being a unique individual with authentic needs), and the other opposes mechanism 3 (realization of capabilities to strengthen the social network). We did not find a countervailing mechanism for mechanism 2 (improving individual coping resources).
Countervailing mechanism 1—The mentor fails to explore authentic needs
Four participants were not satisfied with the mentoring. Two of them reported that in their view, the mentor had not recognized their authentic needs (as predicted by CMO1): I always felt that the mentor was above me and I was down below. (…) I didn’t think it was equal. Not at all. I thought: ‘The moment I don’t agree with her, I’ve got a problem’. [P01]
These participants felt that the mentor was following the rules of the organization about mentoring too strictly, rather than listening to their individual needs. One participant described this as follows: We came to a point in mentoring where you have to renew contacts with old friends. And well, I have been a drug addict for years, so that was just not a good idea. And then we reached an impasse (..) My mentor was very strict. I think this was what he had been taught. He had learned one tune and that's what he whistled all the time. [P07]
In these cases, there was no positive effect on health; two of the dissatisfied participants even reported a negative effect. They still felt lonely and depressed after mentoring had come to an end: My mental health is worse now [more depressed] [..]. I had a difficult time because my mentoring stopped, but my befriending scheme also stopped and my supervisor stopped. And suddenly I had nothing. Yes my husband of course and my household. [P01]
Countervailing mechanism 2—Participants with a weak/small network
All four dissatisfied participants described that before mentoring, they hardly had a social network that met their social needs, and they therefore lacked the capabilities to strengthen their social network (as predicted by CMO3). They described, for example, that they hardly had a social network because they lacked the social skills to build and maintain a network or hardly had a network left because they had only recently stopped taking drugs. They generally described a social network that consisted of only a few persons, for example, a spouse (who also had no network) or an elderly parent. When participants had a very small and non-supportive social network, in their view mentoring did not help them enlarge this network. For example, when asked how his network had changed compared to the situation at the start of mentoring, one participant answered: Much smaller [Interviewer: Much smaller? How did that happen?] Well I never go anywhere. [P07]
These four participants expected the mentors to solve their problems for them, rather than adopting an active role themselves toward finding a new network. For example, another participant was disappointed because the mentor had not suggested activities for her to expand her existing network. She also dismissed the mentor's attempts to break the ice or to build rapport and to elicit authentic needs as chit-chat and did not see them as useful for mentoring: The mentor was actually a very nice woman, but it also struck me that talking with her degenerated sort of into a social chat about nothing. I thought: Is this mentoring, just a bit of social chat? [Interviewer: And what do you mean by social chat?] Well, for example about the cat or about her children. I think that's not what we’re here for. She was here for quite a long time, from ten to twelve or something, and she said, well, now I have to go pick up my son from school. I thought yes, but you didn’t suggest any concrete activities. [P01]
Participants not only have to have some kind of social network to start with, it also seems that they need to have a certain level of social skills to be self-directing and to take part in the mentoring. Given their difficulty of directing their own social network, these participants generally felt that befriending schemes, where they are not responsible for building their own network but develop a friendship with a volunteer to undertake activities together, would have suited them better: I don’t really have to think about it, actually I think befriending is much better than mentoring. [P01]
Discussion
Summary of the findings
Our realist evaluation of mentoring found three mechanisms that worked. Mentoring worked when a personal contact between mentor and participant was established, based on acknowledgment, recognition, and acceptance, which enhanced participants’ self-esteem and decreased their loneliness (CMO1). Secondly, mentoring worked when the mentor helped the participant develop individual coping resources to deal with social situations, resulting in a more positive perspective on life and favorably influencing self-esteem and self-confidence. This also helped to reduce stress (CMO2). Finally, mentoring worked when the mentors helped the participants realize their own capabilities to strengthen their social networks, resulting in increased feelings of self-esteem and self-confidence and decreased feelings of depression and loneliness (CMO3). Mentoring did not work when mentors did not recognize and explore the authentic needs of participants (countervailing mechanism 1). Mentoring also did not work for participants who had no (or hardly any) social network and the skills to be self-directive and self-confident in developing a stronger social network (countervailing mechanism 2).
Mentoring generally worked as predicted by the program theory. According to this theory, “recognition, coaching coping skills and stimulating self-direction” is what is needed, and this was indeed achieved, depending on the participants’ social network and the mentors’ skills.
Interpretation
Our results, which indicate that an intervention that helps to enlarge participants’ social network improves their mental health, are in line with a growing volume of literature demonstrating the positive effects of social capital on health outcomes. We also found that this was established via different pathways (Berkman et al., 2014). Most importantly, mentoring improved participants’ health, not only by offering social support that allowed them to believe that they were being cared for, esteemed and valued, as is often hypothesized in studies about social networks, but also by offering them coping strategies to address maladaptive beliefs. This is in line with studies that found that interventions addressing maladaptive social cognition reduced participants’ sense of loneliness (Masi et al., 2011). Furthermore, mentoring increased health by realizing the participants’ capabilities, which is in line with studies that found that engagement in socially valued roles is important for the recovery from mental health problems (Salehi et al., 2019) as it may provide a sense of social cohesion (Manuel et al., 2012). The mentor functions as “bridging capital,” which other studies also found to relieve the mental distress of vulnerable persons (Mitchell & LaGory, 2002) by allowing them to feel included in the community (Salehi et al., 2019). It seems that the participants for whom mentoring was successful already had a social network with both strong and weak ties (e.g., a network consisting of family relations but also of acquaintances, colleagues, neighbors, etc.). When the mentor was not able to function as bridging capital, as was the case with the four participants who hardly had any social network, mentoring did not improve their health. In these cases, the participants only had a few strong ties (e.g., a husband or a father). Granovetter (1973) predicted that persons with only strong ties may be socially disadvantaged and may also need weak ties (e.g., through bridging capital) to gain access to other perspectives, social activities, and opportunities.
Our results indicated that the skills of the mentor are pivotal, which is in line with studies that stressed the importance of acceptance, acknowledgment, and encouragement by volunteers to support participants who want to enlarge their network, and enable them to find solutions themselves (Mitchell & Pistrang, 2011). When our mentors engaged in interactions that were perceived as demonstrations of superiority, or when very general rules of the organization were followed rather than those of the intervention, this belittled or undermined self-perceived identity, and the mentors seemed to be destroying rather than cultivating participants’ capabilities to experience inclusion in their community and new social networks. This is also in line with other studies, which found that positive bridging capital (having positive and reciprocal social interactions with outsiders) gave people with mental disabilities and their family members access to a wide range of resources, whereas non-reciprocal negative relationships could result in social exclusion and reduced trust (Henderson et al., 2011).
Our study also showed, however, that participants should have the skills and the network to make this possible. Individuals with no, or hardly any, social network did not benefit from the mentoring, and it did not help them enlarge their network and form friendships with other people. This may mean that a mentor in a befriending scheme may be more useful in forming weak ties. Also these participants could have more instrumental help with forming friendships, that is, strong ties (Granovetter, 1973) than is generally supplied by mentoring, with its focus on participants’ self-reliance. Furthermore, as we found with one participant, when individuals are trying to free themselves of drug or alcohol dependency, they frequently also need to leave their existing social network, as this consists of other substance users. Such networks of negative social capital (Putnam, 2000), in which the group norms do not help an individual to stop their substance use, are of course less susceptible to mentoring, as the group norms will not easily be changed, and individuals are better off quitting their entire old network (Hansen, 2009). We thus found that an intervention that aims at network enlargement without taking the existing social network into account is not an adequate strategy. Also, mentoring that does not take account of the participants’ social skills may not be sufficient. Participants who lack the social skills to build or enlarge their social network may be served better when mentoring is combined with additional social skills training (Howarth et al., 2016; Kruithof et al., 2018). Furthermore, these participants could be served better by mentors who themselves become a strong tie rather than remaining a weak tie, thus becoming more of a buddy within a befriending scheme, as some participants argued.
Implications
A number of practical factors should be considered when designing future mentoring schemes. Firstly, we suggest that the targeted population should be clearly defined, and that those participants who are most likely to benefit from the mentoring should be identified. This means that potential participants with no or hardly any social network or the skills to build one may benefit more from other interventions, such as befriending, or community activities such as eating together (Kruithof et al., 2018). They may also be supported by having their social skills trained as a part of the mentoring intervention. This may, for example, involve learning how to initiate and exit conversations, showing nonverbal interest in conversational partners (e.g., head nodding, maintaining eye contact) and asking questions (Rose et al., 2021).
In addition, this also means that mentoring should not be imposed, as is sometimes done by forcing people to join as part of other programs (Philip & Spratt, 2007). Even though the intervention that we studied, explicitly emphasized that mentoring should always be voluntary and based on a participant's genuine need to enlarge their social network, this was not always the way the intervention was carried out. Secondly, we recommend to always train voluntary workers and offer them peer feedback and coaching. Building and sustaining mentoring relationships can be difficult for voluntary workers, demanding skills in building mutual, respectful, empathic and nonjudgmental relationships (Philip & Spratt, 2007). Thirdly, we therefore believe that good matching is crucial to the success of a mentoring scheme, to ensure that the combination of mentor and participant works. How mentor and participants can best be matched should be the focus of further research. Fourthly, our results suggest that organizations that promote standardized forms of mentoring will not improve the mental health of participants, nor strengthen their social networks. Therefore, organizations should allow mentors to have a certain freedom to engage in an authentic and mutual relationship with a participant.
Limitations of the study
The most important strength of our study is that we were able to recruit several participants from vulnerable groups with hardly any network at all, whose perspectives gave us further insights not only into the mechanisms that work, but particularly into the countervailing mechanisms. One limitation is related to the fact that several participants described their initial experience of mentoring as starting a new life, in which they decided not only to find support to strengthen their social network, but also looked for other ways to improve their life, such as finding a new job or starting physical exercise. One important limitation was therefore that it was not always possible for the participants to clearly state whether their increased social network and increased self-confidence or self-esteem could be attributed solely to the mentoring intervention or to other experiences they had during the same period. These “fresh start” experiences (Mitchell & Pistrang, 2011) have elsewhere been hypothesized as positive events that introduce hope and as a potential mechanism of change in befriending (Harris et al., 1999), but apparently play a role in mentoring as well.
Conclusions
Our article has explored the theoretical and empirical links between a mentoring intervention and health. Three mechanisms were found that contributed to health: participant's authentic needs are recognized, their coping resources are improved, and they realize their capabilities to strengthen their social network. These mechanisms resulted in increased self-esteem and self-confidence. What seems crucial to mentoring is establishing a mutual, respectful, nonjudgmental relation in which the client's identity is “repaired” and in which capabilities are explored and realized. These aspects seem to be more important than the original aim of the mentoring intervention, which was to strengthen the social network. Another crucial aspect for mentoring to work is that participants already need to have some kind of social network.
Footnotes
Ethics
According to the Dutch Medical Research Involving Human Subjects Act, this study was deemed exempt from approval by a medical research ethics committee in the Netherlands, because respondents were only interviewed. We followed the Declaration of Helsinki adopted by the World Medical Association (World Medical Association, 2018) and guaranteed the anonymity of respondents by using codes. Each respondent gave written consent after being informed of the aims and methods of the study beforehand.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by ZonMw (The Netherlands Organisation for Health Research and Development), (grant number: 531005003).
Acknowledgements
We would like to express our grateful thanks to the respondents and the participating mentoring organizations for their time and for sharing their perspectives with us. We also would like to express our sincere appreciation and our deepest gratitude to Martin van de Lustgraaf, the developer of “Of course a network mentor!” (in Dutch: “Natuurlijk een netwerkcoach!”) for giving us the opportunity to evaluate the intervention.