
Abstract
Summary
Unpaid carers were profoundly impacted by the coronavirus disease 2019 pandemic and public health responses. In the UK, in March 2020, people identified as clinically extremely vulnerable and their household members were advised to “shield” for an initial 12-week period, which meant minimizing all contacts from outside the household and not leaving the house at all, unless in an emergency. In a modified form, shielding guidance remained in place until August 2020 and was reinstituted from December 2020 until April 1, 2021. This article, reporting on qualitative interviews with 47 unpaid carers in Wales, thematically analyzed using a coding framework, explores the experiences of unpaid carers affected by this shielding guidance and their wider implications for social work with unpaid carers in the future.
Findings
Participants in our study described ways in which their caring role expanded, due to the need to provide additional practical and emotional support for loved ones who were shielding, and who lost access to other avenues of support. Some also described their caring role as becoming more involved and complex due to the declining health or self-care capacity of the person cared-for as a direct consequence of shielding restrictions. Alongside the increase in their caring responsibilities, carers reported losing access to important avenues of support for their own well-being.
Applications
We draw on ecological systems theory to highlight the importance during care planning and management of exploring the carer's mesosystem to identify and optimize sustaining forces, and of attending to the microsystem involving the carer and person cared-for.
Unpaid carers (individuals who provide care to another person who would not be able to cope without their support) are the backbone of the health and social care systems of all nations of the UK, 1 providing a contribution thought to be valued at £193 billion per year—a figure higher than the annual expenditure of the National Health Service (NHS; Carers UK, 2020). The tasks fulfilled by unpaid carers commonly include practical support (e.g., shopping and housework), personal care (e.g., toileting, washing, and help with medication), and/or emotional support. Unpaid carers fulfill their roles within the context of a wider ecological social system involving other individuals and services who support the person cared-for; other social networks through which they may receive support in their caring role; and the wider milieu of connections, responsibilities, and priorities that impact on their lives (Bronfenbrenner, 1979). Becoming an unpaid carer can have a significant impact on the way an individual has access to support from their social networks, which are central to the sustainability of the caring role (Ahmed et al., 2018).
Caring for another person can be fulfilling for the carer and can enable rewarding relationships to flourish between the carer and the person cared-for (Carbonneau et al., 2010; Pysklywec et al., 2020). However, it can also result in significant hardships. International evidence indicates that those who provide unpaid care to loved ones score significantly lower than the general population in a range of health and social measures, including mental health, physical health, social isolation, and broader quality of life factors (Robison et al., 2020; Vasileiou et al., 2017; Verbakel et al., 2014). Unpaid carers are also disadvantaged in terms of their ability to participate in and thrive in paid employment, with women, who represent 58% of all unpaid carers in the UK, being disproportionately impacted (Carers UK, 2021; Lorenz-Dant & Comas-Herrera, 2021). Women tend to become unpaid carers at a younger age than men, with 69% of claimants for Carers Allowance (a UK welfare benefit, currently at £76.75 per week, for carers who do not otherwise earn over £139/week after tax) being female (Foley et al., 2023) and 20% of women aged between 45 and 54 providing unpaid care to another person (Carers UK, 2021). Furthermore, caring appears to negatively impact women more than men; Verbakel et al. (2014), for instance, identified that the risk of depressive symptoms associated with caring was two times stronger for women.
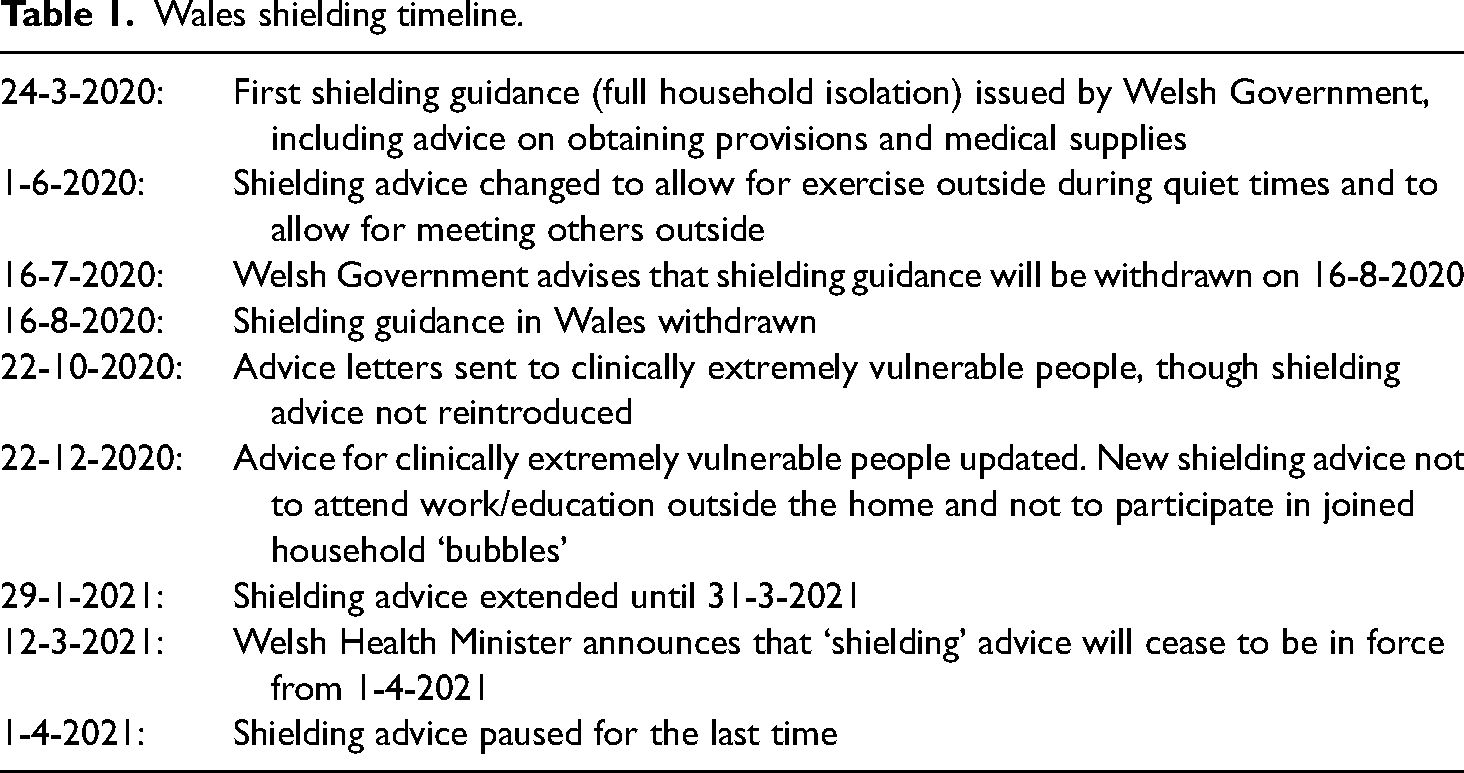
This paper reports on a qualitative study exploring the experiences of unpaid carers in Wales during the coronavirus disease 2019 (COVID-19) pandemic. The pandemic had a significant impact on unpaid carers because of the specific risks posed by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus for older people and those with a pre-existing health condition, who were most likely to be receiving care from a loved one. Among the many implications of the subsequent national lockdowns imposed across the UK, in which nonessential businesses were shut and all individuals were required to stay at home unless performing essential duties or activities, were that an additional 4.5 million people became unpaid carers. Furthermore, those who already provided care had to take on increased responsibilities because of other sources of care ending or being highly restricted (Carers UK, 2020). At the same time, the UK Governments also issued advice to people identified as clinically extremely vulnerable to “shield” for an initial period of 12 weeks. Shielding meant not leaving the home at all (even for exercise) unless seeking emergency care, and minimizing direct contact with any household member who was not able to follow the same guidance (Welsh Government, 2022). This was an unprecedented and deeply unsettling time, during which those identified on the shielding list were offered support with obtaining provisions and medical supplies through the armed services (see Table 1).
Wales shielding timeline.
Caring and shielding in the time of COVID-19
During the initial period of heightened societal response to COVID-19 in 2020–2021, lockdown and shielding policies directly increased the complexity of providing care because of their incidental impact on the people in need of care. People with learning disabilities, for example, needed additional support to understand the nature and necessity of shielding and social distancing, and to cope with the distress brought on by increased isolation (Courtenay & Perera, 2020). The disruption to routines resulted in increased presentations of challenging or concerning behavior (Villani et al., 2020), yet there were fewer services available to provide any direct support to meet these additional challenges (Doody & Keenan, 2021). In countries where schools shut, parents of children with learning difficulties were particularly susceptible to increased stress due to the lack of direct services and informal support (Bailey et al., 2021; Marsack-Topolewski, 2021; Willner et al., 2020). A population group affected particularly severely by the disruption to social life caused by shielding were people living with dementia. The loss of activities outside the home and increase in time spent on sedentary and repetitive activities resulted in the irreversible progression of many people's conditions at a rate faster than might otherwise have been expected (Lightfoot et al., 2021; Muldrew et al., 2022; Rising et al., 2022), and produced a negative impact to their mental health and associated behavior (Tsapanou et al., 2021).
Application of Pearlin et al.'s (1981) stress process model, conceptually adapted by Turner (2009), suggested that the increase in caring responsibilities led directly to an increase in unpaid carers’ stress (Altieri & Santangelo, 2021; Cohen et al., 2020; Savla et al., 2020) and, correspondingly, a higher prevalence of mental health issues has been noted among unpaid carers during the pandemic (Gallagher & Wetherell, 2020; Park, 2021). The strain placed on unpaid carers by the increased complexity of their caring roles was exacerbated by the fact that they often had to deal with such issues alone due to the reduction in services available for support (Rokstad et al., 2021). Unpaid carers’ isolation increased due to the loss of both formal and informal avenues of support (Muldrew et al., 2022). Understandable fears about the risk of transmission of the virus in residential care, and the collective trauma of times during which people were not allowed to see their loved ones in person even in their last moments, appear to have discouraged the use of residential care to enable carers to take a break and it may take some time to rebuild carers’ confidence to use these facilities (Samsi et al., 2022).
On top of the increase in stress brought about by expanded caring roles, continuing fear of passing on the virus to a vulnerable person has been a source of considerable worry to unpaid carers (Onwumere et al., 2021; West et al., 2021) and has curtailed access to the wider community for both the carer and person cared-for. A further worry for many carers has been the threat of becoming ill themselves, and what would happen to the person cared-for if they were to be incapacitated by the virus (Lorenz-Dant & Comas-Herrera, 2021; Muldrew et al., 2022; Rotarou et al., 2021). Consequently, personal shielding appears to have been broadly embraced and enacted by carers as a protective mechanism, despite the extreme isolation and associated risk factors this entailed outside of fears regarding the virus.
An important consideration to bear in mind in this discussion is the difference (within the UK context) between legally enforced lockdown rules and shielding guidance. Lockdown measures were portrayed by the UK government as an act of social responsibility towards others, encapsulated in the motto, “Stay at home. Save lives. Protect the NHS.” By contrast, shielding guidance was issued privately through letters from health services to those identified as clinically extremely vulnerable. “Shielding” is therefore much more concerned with personal risk and self-preservation and involves the development of self-imposed rules and choices, which once adopted may be difficult to discontinue due to the prevailing risk posed by the coronavirus.
Some unpaid carers did find that there were some unexpected advantages to life during the pandemic, since interventions like the UK Government's furlough scheme, in which people who usually worked in jobs deemed nonessential (e.g., hospitality) received government funding to cover a period where their workplace was shutdown, eased time pressures for those also in paid employment. Some appreciated a period of slower-paced life in which it was possible to spend more time with the cared-for person at leisure (Burrows et al., 2021; Lafferty et al., 2022; Lightfoot et al., 2021). Overwhelmingly, however, the pandemic caused increased distress and difficulty for unpaid carers and has had a negative impact on their well-being that must be of grave concern to policy makers and social care service providers.
Many carers chose to shield themselves to protect the person they cared for despite their own lack of vulnerability, while others found themselves with increased caring responsibilities due to the cared-for person following shielding guidance. Studies to date on carers and the COVID-19 pandemic have primarily focused on the impact of lockdown more broadly, however here we consider how the specific consequences of shielding guidance changed unpaid carers’ lives.
Our study
In early 2021 we conducted a qualitative exploratory study with the aim of capturing unpaid carers' experiences of caring for family members or friends, covering the time before, during, and after the initial lockdowns of 2020. Our three research questions were:
What were unpaid carers’ lives like before the pandemic began? How has COVID-19 impacted the lived experiences of unpaid carers and the roles they undertake? What has the impact of COVID-19 been on unpaid carers’ well-being?
Design
The research focused on generating carers’ qualitative narratives of their experiences to capture the practical, relational, and emotional impacts of caring over this period. We, therefore, elected to carry out semistructured interviews, which enabled participants to guide us to matters that they felt were of personal importance to them, while ensuring that we were able to capture data pertinent to the overall aims of the research (Clark et al., 2021).
Participants and recruitment
To represent the diverse experiences and viewpoints of carers, we sought a sample encompassing all age categories from 16 upwards, and from all regions across Wales. The legal constraints on social interactions at the time of data collection (January–April 2021) meant that it was necessary to carry out all recruitment activities online. We advertized the project via social media and through circulating details to relevant organizations to disseminate to users of their services. Those who were interested in taking part were directed to a weblink which included information about the study and a consent form. We found this approach successful in achieving a diverse sample and resulted in a total of 47 participants. A disadvantage of carrying out the study during this period, however, was that it was difficult for us to carry out targeted recruitment of groups who were under-represented in our sample, such as those aged over 75 and people from minoritized ethnic communities.
We consulted unpaid carer's organizations on the overall design and aims of the study, and produced the interview guide in consultation with carer groups, whose feedback on initial proposals was incorporated in producing the final guide.
Data collection
The final interview schedule was structured around four main topics:
Relationships with the person they cared-for: How the participant became a carer and how they feel about their identity as a carer. Support and sustainability of caring: The practicalities of caring and the services received and required to make it sustainable. The personal impact of caring on the participant: Finance and employment; education; mental health; physical health. The impact of COVID-19 and the future of carer support in Wales.
The research team was composed of four interviewers all with substantial or partial experience of researching social care in Wales. One interviewer was able to interview in Welsh. Interviews were conducted either by online video calling or telephone, depending on participant preference. We encouraged privacy during the interview to protect confidentiality, though some young adult carers, who were recruited through carer support groups and knew each other well, chose to be interviewed together in pairs. A total of four interviews were conducted in this way, with all the rest being carried out individually. The average length of interviews was 1 hour, with a range from 30 to 90 min. The interviews were audio-recorded, transcribed, and anonymized by the interviewer, who assigned each participant a pseudonym. Four interviews were carried out and transcribed in Welsh and then translated into English for analysis.
Data analysis
To analyze the findings, we developed a coding framework based on the study's research questions, supplemented by reflexively produced codes arising from participants’ narratives (Ritchie et al., 2013). Three out of four members of the interviewing team were involved in coding transcripts independently before collective sharing and discussion, which often led to further coding as our framework was revised and extended. All interviewers also wrote a short qualitative summary of each interview and their impression of the participant's priorities. The final coding framework consisted of 18 themes ranging across relationships with people and organizations, emotional and physical well-being, identities, feelings about the future, social support, and financial circumstances.
Ethics
Ethical approval of the study was provided by the Cardiff School of Social Sciences Research Ethics Committee (ref. SREC/4042) in December 2020. The interviews were often emotive and required the interviewers to show skill and sensitivity in response to participants’ narratives. We used discretion to omit questions that might cause undue stress in certain circumstances (e.g., asking a parent-carer about their future as a carer when their child had a terminal condition). At the end of each interview, researchers offered a nonrecorded de-brief to check how participants were feeling about the interview and to discuss their emotional responses freely. This also enabled us to signpost some participants to relevant services. As a research team, we worked closely to support each other and de-briefed informally where any interviews had been particularly emotive. This was particularly important while working from home and in relative isolation since the difficulties and frustrations described by some participants were liable to produce moral distress to interviewers who were powerless to assist beyond signposting to sources of potential help (Morley et al., 2017). As compensation for their time and expertise, we offered a small gift voucher to those who had taken part in the study.
Findings
We identified two overarching themes regarding the implications for carers of shielding guidance, with three subthemes emerging in each (see Figure 1).
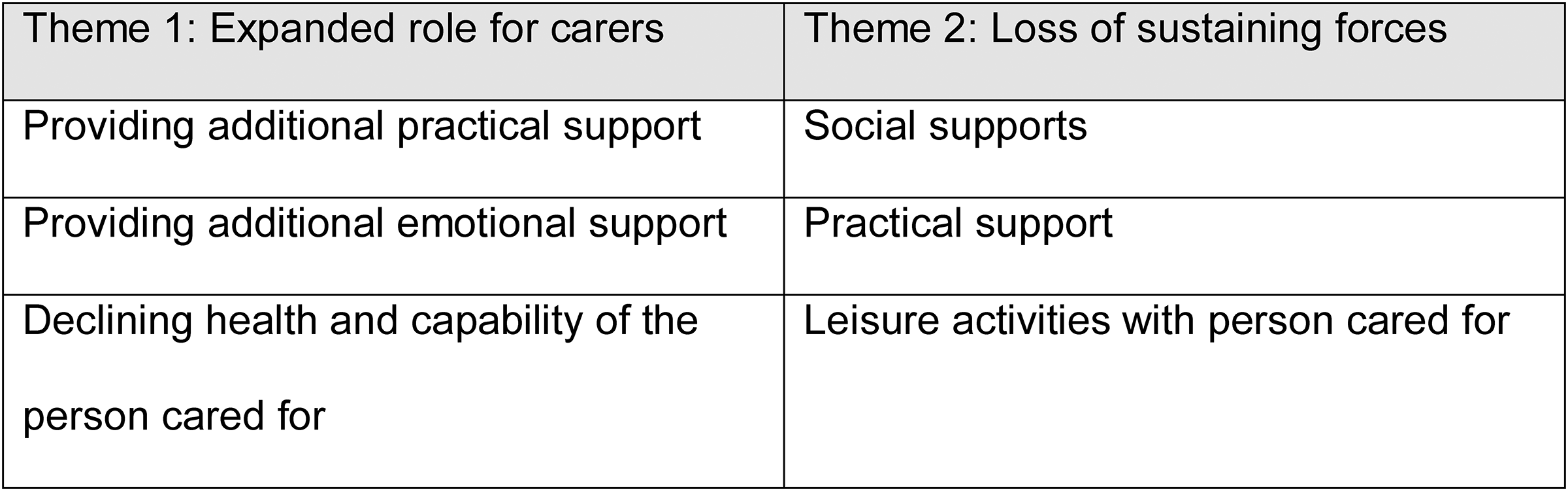
Themes and subthemes.
Theme 1: An expanded role for carers
Providing additional practical support
An unsurprising effect of the ‘shielding’ policy on unpaid carers was that many found that there were additional tasks they needed to complete for the person cared-for, either because that person was unable to leave the house, or because it was considered unsafe for others (e.g., friends or paid care services) to enter the homes of people shielding: Lately of course [the amount of responsibility I have] has been much bigger because she has been shielding completely for eight months now, so basically anything that happens outside of the house, things like collecting prescriptions, those sorts of things. (Natalie)
As Natalie, a young adult carer also engaged in full-time education, found, the roles fulfilled by individual carers expanded particularly in situations where they became the sole person having direct in-person contact with the person who was shielding. Taking care of “anything outside the house” placed additional stress on some carers due to the need to cope with unfamiliar tasks. This was particularly evident for younger carers who, despite having fulfilled caring duties for several years, did not necessarily know how to run a household: … Mum's now shielded, so it just means that I’ve got to [sighs] go shopping by myself … I have got to be an adult and I don’t want to be an adult. (Louise)
Louise's poignant comment about becoming an adult is a reminder that the expansion of a carer's role is not simply a matter of the additional tasks taken on, and the requisite skill, stamina, or time to complete them. Just as the initiation of caring changes the relationship dynamic between the carer and the person cared-for (Keating & Eales, 2017; Kitwood, 1997; Plank et al., 2012), alteration or expansion of an existing caring role also impacts on that relationship and on the identities of all parties within it. The significance of the additional roles taken on during the pandemic to the carer's biography should not be overlooked, since they may represent permanent transitions in the carer's role and identity. Indeed, while the official advice to shield in the strictest sense was lifted in August 2020, many people chose to carry on following the same restrictions throughout 2020 and through subsequent waves of the pandemic (Samsi et al., 2022). The lives of carers, therefore, did not return to their pre-COVID-19 norms simply because government guidance changed.
Additional emotional support
Not only did the shielding requirements place additional obligations on carers in terms of supporting the practicalities of that person's life, for some, they also led to new levels of responsibility for their emotional well-being. As Natalie commented, her visits to her mother to bring her provisions and other essentials took on additional significance because, “Going down and helping is very important in terms of her mental health because I'm the only person she sees”. It may have been possible for Natalie's mother to arrange for most things that happen ‘outside the house’ to be taken care of—supermarkets and pharmacies, for example, often provide delivery services and quickly developed policies to prioritize those who were identified as vulnerable. Doing so would likely have left her more isolated, however, whereas Natalie's visits for practical purposes also facilitated the direct human contact that she felt was necessary for her emotional and psychological well-being. The care needs of Natalie's mother are related to a lung condition that causes physical disability, yet Natalie's comment about her mother's mental health demonstrates how carers often adopt a holistic approach to the needs of the person cared-for. Where shielding created new needs in a person's emotional well-being, this holistic approach meant that it often fell to unpaid carers to meet these needs.
The relationship dynamics and role expectations within families mean that it is possible that many carers will continue to fulfill the roles they take on during the shielding period long after the heightened infection risk from the pandemic has passed. Judy, for example, who supports her mother and aunt, both of whom are in their 90s, felt that their dependency would not be reversed in the future due to the importance of her support to their emotional well-being. Well, they have become more dependent because they can’t leave the house. Auntie Lorna's got a little car, she shouldn’t drive it, she's totally unsafe. But before March she was popping out for her own shopping once a week … I know that I’m always going have to do her shopping … I’m sure that I could get online and maybe get deliveries to her. That might be something I could do, but, you know, then she wouldn’t see anybody. So I feel a bit trapped … (Judy)
As with Natalie above, Judy's comment demonstrates how practical acts of caring have significance beyond the immediate fulfillment of the task being completed. Caring between family members is a complex relational process, not a simple transaction of voluntary labor, and therefore it should not be assumed that responsibilities carers take on in an emergency will readily be lifted when the immediate crisis passes. What made Judy feel trapped was not only the permanence of the practical necessity of bringing Auntie Lorna her groceries now that she has lost the habit of driving but the fact that Auntie Lorna would lose out on human contact if Judy arranged delivery instead of bringing the groceries herself. The additional responsibility managed by working carers like Judy, who was furloughed from her paid job during the pandemic, is likely to have created difficulties as societies reduced and removed restrictions (e.g., the recommendation to work at home where possible). The return to “normality” may have made it challenging to balance additional caring responsibilities with post-pandemic expectations of employers.
Declining health and capability of the person cared-for
In addition to the need to undertake practical tasks that individuals would not be able to accomplish for themselves due to shielding, and the additional emotional support required due to the social isolation of shielding, some carers found that their caring responsibilities increased as a result in the decline in the condition of the person cared-for, which came about as an unwanted side effect of shielding. Alison, whose mother has dementia, noticed a decline in her mother's mobility as a direct result of being unable to take her to places where she would usually walk around: She just got quite happy sitting in her chair and not trying to do her exercises or anything … she was still mobile, she still was going out of the house but, obviously, when we got locked down and she was on shield—and I was on shield as well—we didn’t have that option to go out. So, the most we did was maybe take her out in the car and drive her round. But even that became impossible because she just would refuse to leave the house. (Alison)
The issue of shielding guidance occurred at a time when the risk of contracting the virus in the fresh air, or from surfaces, was less well known (see WHO, 2020). As a result, public spaces in which people could exercise were made much less accessible to those with reduced mobility: public conveniences were closed, benches were taped over, and there was considerable social censure for anyone who was seen to be idling (Wu et al., 2022). For people with dementia, mental stimulation is particularly important in order to slow down the progression of the condition and to maintain quality of life (Hughes et al., 2013), yet this need was not taken into account in the advice that was issued. As a result, it fell on unpaid carers to manage the negative side effects of the shielding and lockdown policies with little support or guidance.
Theme 2: Loss of sustaining forces
At a time in which carers’ responsibilities increased, one of the impacts of the shielding guidance (and wider “lockdown” policies) was that carers lost out on usual forms of support and sources of pleasure that help to make their role sustainable. This manifested in two distinct ways: Carers lost out on contact with social supports that were important to them in coping with the stresses of their roles and carers lost out on practical help with specific caring tasks. Additionally, both the carer and the person cared-for lost out on opportunities to enjoy leisure time together, which exacerbated stress and had a direct impact on their personal relationships.
Loss of social supports
For many, the fear of the impact of the virus on the person cared-for meant that the advice to shield was taken to apply equally to the carer. Because my son was shielding, and in those first weeks—first few months, I couldn't see dad at all. (Angharad)
[My friends] sometimes go into these cafes, but I don’t want to go into them just in case I bring something home. Just things like that, public things that are open, I don't feel too comfortable going in. (Sion)
Even in the most auspicious circumstances, caring can bring with it stresses and tensions, and these are often relieved by having social contact with family members, friends, and colleagues outside the household (Gupta & Pillai, 2000; Marsack-Topolewski, 2021; Washington, 2009). Losing such resources of emotional support at a time of heightened pressure may have increased the impact of their expanding responsibilities on carers. As the data extracts above demonstrate, public health measures for controlling the pandemic were uniquely challenging for carers’ mental health since they turned usual sources of emotional support into sources of danger and anxiety.
Loss of practical support
The loss of physical contact with friends and family members due to shielding was problematic for many carers because it reduced opportunities for carers to receive support in the provision of care. This could be particularly acute for parent carers, like Lindsey. I mean we really haven’t—because she's been shielding—we’ve not seen friends or family … normally, outside this pandemic, my mum would have Mia maybe one night every other week just to give a bit of respite, friends and family would come over and even just having people over for an hour at a time playing with Mia just give you a little bit of downtime yourself to be able to relax but, of course, we’ve not been able to have that and she's not been able to see her friends and have her downtime as well, which I think is equally as important as just the adult downtime. (Lindsey)
While the use of technology to keep in touch with loved ones was highly valued by many participants throughout the pandemic as a means of maintaining some level of emotional support, the loss of physical presence meant that carers lost both organized and irregular resources of respite. This reduced the amount of time carers had to focus on their own well-being, whether through leisure activities (e.g., socializing or exercising), or attending to their own health needs. It is, therefore, be anticipated that many carers’ mental and physical health will have declined through the course of the pandemic (Landi et al., 2022; Willner et al., 2020).
Loss of leisure activities together
For many carers, the potential impact of the virus on the person cared-for was a continuous threat, resulting in reduced opportunities for both the person cared-for and the carer to enjoy activities outside the home. … If he gets a cold, he gets sepsis, it's straight to resuscitation. He's in a condition where his life is on the line. So it's been, it's been really hard … it's severely restricted everyone's quality of life. (Angharad)
Angharad's words highlight how the loss of shared pleasures impacts the quality of life of both the carer and the person cared-for. A significant aspect of the shielding regulations in this regard was that exercise outside the home should be avoided, unlike those under general lockdown who were permitted to leave the home for up to one hour per day. This had a significant impact on the mental health of carers who were shielding, as well as the people they cared for: There's so many beautiful places in this area, some—not all wheelchair accessible, but the ones that are, we were slowly working our way around. And it was exciting, and I did my homework, and I had a big board of all the places I wanted to go. She was new to the area as well, so we were exploring together. That obviously all stopped. We weren't allowed to go out … it was a mental and emotional … Just to go sometimes to the beach and just to scream … You know, get it over and just cry and shout and yell and swear. (Louisa)
Louisa refers to the potentially cathartic experience of enjoying the outdoors, the loss of which is likely to impact the quality of the relationship between her and the person for whom she cares, potentially making the arrangement less sustainable in the longer term. The importance of accessing the natural world to mental health was considered secondary to the risk of COVID-19 transmission within the shielding policy, though later evidence on the risk of transmission in open-air environments suggests that this policy may have been misguided (Bulfone et al., 2021).
The loss of opportunities to be spontaneous for many carers resulted in a sense of ennui and repetitiveness. Sometimes I feel like every day's the same and it's sort like a, just a rollercoaster of sort of doing the same things, like cleaning, doing the washing for her, changing the bed, that type of thing. (Luke)
Caring can often involve mundane and difficult physical labor and it is therefore beneficial for carers to have sources of variety in their lives to avoid boredom and frustration (Yeandle, 2020). The lack of variety described by Luke, the sole source of support for his mother with challenging behaviors, was driven by the loss of opportunities for him and his mother to do things outside the house together. This was accompanied by a reduction in opportunities for him to have time to pursue his own interests away from his caring responsibilities. The necessity of shielding for many carers (and the restrictions of lockdowns) meant that opportunities for relieving the monotony in daily life were lost, which may have had damaging consequences for carers’ mental health.
Discussion
Unpaid carers’ accounts of shielding tell a striking story about the extent to which caring responsibility fell increasingly upon individuals in isolation. The minimization of direct contact between people meant that it became socially responsible for those who might usually provide occasional acts of assistance to stay away from people who were identified as highly vulnerable. This left all the responsibilities of care to just one individual, or members of just one household. Similarly, those in need of care were cut off from usual sources of support outside their own homes, whether through community-based formal services or their own informal networks. Considering this restructuring of caring duties, our participants reported a sense of being trapped and having no option but to continue with their old responsibilities and discharge the new responsibilities to the best of their abilities. The challenges that this brought about highlight the extent to which caring, in normal circumstances, depends on intricate social systems that both provide elements of direct interaction to meet the cared-for person's needs and offer support to make caring sustainable for individuals with the most caring responsibilities.
Situating shielding in the ecosystem of unpaid caring
Bronfenbrenner (1979) argued that individuals are connected to their social environment through a nested series of systems, which range from microsystems, in which direct contact between people takes place, through to the larger exosystems and macrosystems that influence individual and group decisions, behaviors and attitudes without direct contact or interaction. An individual may be part of a number of microsystems, such as immediate family, work, religious organization etc., all of which interact within the mesosystem, which might be thought of as a “system of microsystems” (Bronfenbrenner, 1979, p. 25). It is apparent from our findings that a key impact of shielding advice was the disruption of the mesosystems of both carers and people cared-for. The microsystem in which the carer and the person cared-for interact became isolated from other microsystems that would ordinarily provide crucial support for the caring role. Thus, for some carers, their work microsystem might usually have provided much-needed social contact and a sense of purpose crucial to their sense of self, or microsystems of friendship would offer emotional support vital for the carer's well-being. Similarly, microsystems that offered direct support to the person cared-for, for example, relatives who would visit and provide practical or emotional support, or paid domiciliary carers, were withdrawn. Shielding reduced the number of microsystems available, often resulting in an impoverished mesosystem (though sometimes also reducing carers’ stress due to a reduction of competing demands on their time).
The difficulties and opportunities caused by shielding highlighted in this study demonstrate how the mesosystem is a key level of the ecological system for determining the extent to which caring is sustainable and rewarding for the carer, or burdensome and detrimental. Successful caring involves not only the direct interactions in which an act of practical or emotional support takes place, but also the careful management of the mesosystem through which resources can be called upon to share out tasks and in which other microsystems can be accessed for emotional support (Ahmed et al., 2018). Of course, within the mesosystem there can also be component microsystems that make caring more difficult. For example, while some carers find work to be a welcome outlet, others find that the pressure on their time from the competing demands of work and caring are the cause of intolerable levels of stress (Hill et al., 2015; Phillips et al., 2002). The carer's mesosystem should be thought of as a network of microsystems that play a part in either supporting or undermining the caring role.
Unpaid carers’ experiences of shielding remind us how the mesosystem is vulnerable to disturbances brought about by both the microsystems nested within it, and by the exosystem and macrosystem in which it nests. An increase in the needs of the person cared-for, a change in the type of care to be provided, or a shift in the availability of other supporting parties within the microsystem of caring can significantly alter the carer's mesosystem, reducing or increasing their ability to access other microsystems upon which they rely. Similarly, our findings demonstrate how a disturbance within the macrosystem, as presented by both the arrival of the novel coronavirus and public health responses to it, caused a substantial shift in the operation of unpaid carers’ mesosystems.
Implications for social work practice
The importance and vulnerability of the carer's mesosystem highlighted within this study suggest that services to support carers should focus particularly on this level of the ecological system. Carers need a mesosystem in which there is support for the person cared-for, support for them in their caring role, and opportunities to engage in interests and pursuits that are unrelated to caring. Where isolation develops because of the caring role, carers need to re-establish connections with other important microsystems, and may also benefit from connecting with new microsystems, such as support groups with other carers. This is particularly the case for carers who are especially prone to isolation, such as spouse carers and carers of people living with dementia (Carers UK, 2019). It is essential to approach carers’ lives holistically, focusing on their concerns and desired outcomes beyond the fulfillment of their caring roles, so that caring can be a part of life as carers want to live it (Yeandle, 2020).
Within care planning and management, carer assessments offer an opportunity to explore with unpaid carers their ecosystems, allowing them to recognize supportive and detrimental microsystems and to identify how the systems in which they are involved can be adjusted to help meet their own needs. Washington (2009) found that drawing ecomaps with caregivers of children with disabilities enabled them to take stock of the people and organizations involved in their lives, raising their consciousness of avenues of support some were not even aware they had. Doing so can be a first step for unpaid carers in optimizing their mesosystem so that caring fits into their lives. Similarly, attention needs to be paid to the quality of the microsystem in which the carer and person cared-for are involved. Support for this microsystem should not be focussed only on providing relief or temporary replacement of the carer (though this may often be helpful and welcome), but also on how the relationship beyond the provision of care can be sustained.
Limitations of the study
The challenges of carrying out this work during a critical phase of the pandemic (January–April 2021) in the UK meant that we relied on video technology or telephones to conduct the interviews. This made it more difficult to establish rapport and to read body language, yet we felt that such disadvantages were often mitigated by our participants’ enthusiasm to tell their stories. The under-representation of male carers, older carers, and people from minoritized ethnic backgrounds limited the diversity of experiences captured in the study. It should also be noted that our study was conducted only with participants in Wales, and there are differences in health and social care policy context and pandemic response between Wales and the rest of the UK. However, given the ubiquity of unpaid caring and shielding as a health protection strategy across the UK and other countries internationally, our findings have relevance beyond the Welsh context.
Conclusion
The social and economic changes in the UK during and following the pandemic have altered the landscape of unpaid carers’ lifestyles dramatically. This research illustrates some of the challenging impacts this has had on the lives of unpaid carers who were affected by shielding guidance, whose caring duties often increased while access to support was reduced. Echoing the recommendations of other studies, we call for an additional focus from social care and health services on the well-being of carers post-pandemic. In relation to practice, we suggest incorporating a greater focus on holistic carer well-being in initial and ongoing assessments. This is particularly important for those carers who were shielded during the pandemic, as our study suggests they are at risk of additional negative impacts. Furthermore, in the event of future lockdown conditions relating to contagious disease, we would call for greater caution in delivering guidance to avoid socially distanced outdoor activity where early evidence suggests this has a low risk of disease transmission. A lack of access to the outdoors can have severe effects on those who are already socially isolated, such as carers and people cared-for. Finally, there is now a need for new evidence relating to unpaid carer support service design and delivery to understand how professionals and organizations have adapted to post-pandemic conditions. This should assess whether current resources and practice are sufficient to address the substantial impact of the pandemic on both shielding and non-shielding unpaid carers.
Footnotes
Ethics
Ethical approval was provided by the School of Social Sciences, Cardiff University ref. SREC/4042.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Public Health Wales, ref.520093 (grant number PHW-ITT-45594).
Declarations of Conflict of Interests
The Authors declare that there is no conflict of interest.
Authorship
DB contributed to the Project PI, data collection and analysis; and was article lead author. Lyttleton-Smith contributed to the Project Co-I, data collection and analysis; and was the article’s second author. LS contributed to the data collection and analysis. SJ contributed to the data collection. RK contributed to the conceptual development and article review.
Acknowledgments
The authors are grateful to Dr Jiao Song, Professor Alisha Davies, and Genevieve Riley for their support, and to our peer reviewers. We would like to thank our colleagues in Public Health Wales for their assistance and advice during this project. We are also grateful to our anonymous peer reviewers for their care and attention over this paper.