
Abstract
Summary
Children of social service users are at risk for developing mental health problems as well as social and behavioral problems. Social service counselors should therefore be aware of service users’ children and provide support for them. In fact, they are obligated by law to consider children's views and their best interests in cases affecting them. Despite this, little is known about social service counselors’ child focus in their practice. In this study, self-reported survey data from 93 counselors working for the Norwegian Labor and Welfare Administration (NAV) were analyzed to explore their child focus.
Findings
Findings suggest that a particular focus on children is no part of common practice among NAV counselors; nor is use or knowledge of The United Nations Convention on the Rights of the Child (CRC). Knowledge and use of the CRC may be a predictor of child-focused practice. The results showed a significant difference of medium effect size between NAV counselors who ask about children and NAV counselors who do not when it comes to knowledge and use of the CRC.
Applications
Policy makers and practitioners should utilize NAV's potential as a preventive arena. For NAV counselors to be aware of and support children of social service users they need a stronger focus on children and hence know and use the laws concerning children's rights. Incorporating children's rights into social workers’ education and internal training may strengthen the focus on children in NAV counselors’ practice.
Introduction
The Norwegian Labor and Welfare Administration (NAV) administers the social welfare system in Norway. NAV manages and provides schemes such as unemployment benefits, work assessment allowance, sickness benefits, pensions, child benefits and cash-for-care benefits (Arbeids og velferdsetaten, 2019). In addition, NAV offers financial assistance and counseling, guidance, temporary accommodation, qualification programs, and more. Work assessment allowance and disability benefits are provided to social service users who cannot work, or are temporarily without work, due to health issues. Economic benefits support social service users who are not able to provide for themselves through employment, own funds or other economic benefits. Counselors in the local NAV offices have various educational backgrounds. Commonly, counselors have a bachelor or a master's degree in social work, child welfare, social science, pedagogic, economics, or law (NAV, 2019c). The counselors are employed as social workers, primarily in contact with adult social service users. Counselors administer the schemes and guide users who have difficulties regarding labor, need financial assistance, or public housing (Arbeids og velferdsetaten, 2019).
When receiving economic benefits, social service users should be able to provide for themselves. However, four out of ten clients struggle to make ends meet (Statistics Norway, 2018a). In 2017, ∼26% of economic benefit receivers had children under 18 years to provide for. Around 70,000 children depend on economic benefits their parents receive (Skjøstad, 2019). Half of the receivers were single providers. Twenty-eight percent of these families were tenants in public housing, which is a temporary housing measure for disadvantaged people. In addition, 2,000 parents who received economic benefits were homeless (Skjøstad, 2019). Moreover, according to data from Statistics Norway (2018b), almost 54% of economic benefit-receiving parents were unemployed and did not attend education, courses, or other job-related initiatives. In Norway, around 10% of children live in families that are persistently poor, and the numbers are increasing (Brattbakk & Andersen, 2017). Due to the coronavirus crisis, unemployment rates for the Norwegian workforce increased from 2.3% to 10.4% over a few weeks in March 2020 (Bratsberg et al., 2020), and the report by Bratsberg and colleagues shows that people with low income, low educational level, and fewer economic resources were more likely to lose their jobs during the crisis. In addition, families with children were more often laid off compared to families without children. This means that the number of children depending on the economic benefits their parents receive is likely to be much higher today than the numbers from earlier years might otherwise indicate. The report does not give exact numbers but shows that approximately 100,000 children live in families where parents seek unemployment benefits (Bratsberg et al., 2020). In other words, the crisis has had a particularly severe impact on and added additional burdens to families with low socioeconomic status.
In Norway, as in other countries, socioeconomic status affects health and mortality outcomes (Mackenbach et al., 1997; Zahl et al., 2003). Growing up in families with low socioeconomic status is a risk factor for developing cognitive, behavioral, social, and emotional problems among children (Cohen et al., 2010; Duncan et al., 1994; McLoyd, 1998). Norwegian adolescents in families with lower income and lower educational level had poorer health and lower rates of high school completion (Sznitman et al., 2017). The study by Sznitman et al. (2017) found that household income affects high school completion rates for Norwegian adolescent through its effects on adolescent health. A life-course study of children born in New Zealand found that children who grew up in families with low socioeconomic status had poorer physical and dental health as adults (Poulton et al., 2002). In addition, dependence on alcohol and tobacco as adults was weakly linked to low childhood socioeconomic status. An upward move in socioeconomic status did not reverse or reduce the effects on adult health (Poulton et al., 2002). A review study by Bremberg (2002) for the Swedish institution for public health found large differences between children of parents with low socioeconomic status and children of parents with high socioeconomic status. For children of parents with low socioeconomic status physical health problems were 60% more common, mental health problems 70% more common, and risk factors for health problems 80% more common (Bremberg, 2002).
Being out of work is associated with negative mental health outcomes (McKee-Ryan et al., 2005). Researchers have found a medium to strong effect of unemployment on mental health in meta-analyses (McKee-Ryan et al., 2005; Paul & Moser, 2009). These studies also found that the longer the unemployment lasted, the stronger the negative effect on mental health was. Paul and Moser (2009) found that unemployed individuals are more than twice as likely to have psychological problems compared to employed individuals. The causal link between unemployment and mental health problems is complex. Psychological and financial consequences of unemployment affect health negatively through factors like mental stress due to joblessness and financial insecurity, financial challenges, and social exclusion (Wilkinson & Marmot, 2003). The negative effect unemployment has on the mental health of an individual can also affect their children.
Children of parents with a mental illness have up to a 50% chance of developing a mental illness themselves (Leijdesdorff et al., 2017), and they are at risk for developing both the same diagnosis as their parent and any other mental diagnosis (van Santvoort et al., 2015). One-third of offspring of parents with a severe mental illness develop a severe mental illness themselves by early adulthood, and one out of two of these children develop a mental disorder (Rasic et al., 2014). Offspring of parents with depression have a three times higher risk of suffering from major depression, and a twice as high risk of suffering from other mood disorders and anxiety (Weissman et al., 2016). Children of mentally ill parents can lack developmental support and are at risk for child abuse, neglect, identity problems, academic failure, substance use, medical problems, mortality, behavioral problems, dysfunction, and other emotional problems (Brennan et al., 2000; Clark et al., 2004; Sundfær, 2012; Weissman et al., 2016).
According to NAV, 36% of all disability benefits receivers had a mental disorder as their main diagnosis in 2016. Around 20% of the receivers had minor children. Notably, the prevalence of mental disorders among receivers of disability benefits was higher in age groups where individuals are more likely to have minor children (18–39 years = 61.5%, 40–49 years = 46.3%) (NAV, 2019b). In the years 2015–2020, 42% of work assessment allowance receivers had a mental disorder as their main diagnosis (NAV, 2019a). From another point of view, 52% of patients with a mental disorder who were parents and 53% of patients with a substance use disorder who were parents reported receiving unemployment benefits from NAV. If including parents receiving sickness benefits the percentages were respectively 69% and 65% (Ruud et al., 2015, p. 47).
It is evident that NAV provides services for many users with mental health issues who are parents. The children of users with mental health issues are at risk for poor outcomes later in life. Additionally, NAV counselors meet parents of children growing up in poverty. NAV counselors are therefore in a unique position to become aware of and support children who are at risk. Especially for children of parents who are immigrants, NAV has a unique opportunity to detect and support children at risk. Immigrants have less contact with health care institutions, despite the fact that the prevalence of mental illness is higher for immigrants from countries where the average income is low to medium (Reneflot et al., 2018). However, immigrants are highly represented among social service users of NAV (Dokken, 2015).
Safeguarding children's interest—Mandatory by law
The United Nations Convention on the Rights of the Child (CRC) was incorporated into Norwegian law in 2003, and has precedence over ordinary legislation (The United Nations Association of Norway—UNA Norway, 2019). Children have the right to express their views in matters affecting them, and their views should be given due weight, as stated in article 12. According to article 3, children's best interests must be the primary concern when making decisions that may affect them (United Nations, 1989). Therefore, as obligated by law, NAV counselors must take the views of children of social service users into consideration in all cases where children are affected. Social service counselors need to have a family focus and offer support for families with children. In order to have such a child focus, awareness of the CRC is essential.
Children do not only have the right to be involved; they also want to be involved and provided support. In a study presenting young people's perspectives of the support they want, 94% of the children of a parent with a mental illness answered that they did want some kind of support (Grove et al., 2016).
Implementation of the CRC
Implementation of laws and interventions in human services requires thoughtful and effective implementation strategies at multiple levels (Fixsen et al., 2005). In a study by Lauritzen and Reedtz (2013), health care workers’ awareness of and support for patients’ children were assessed. Results indicated that in order to change practice, there must be development on several levels in the organization and in the workforce. Health care workers who supported children of patients had higher levels of knowledge about children's rights, and this might be a factor facilitating a child focus (Lauritzen et al., 2015).
In an empirical analysis of how the CRC is put into action among people working with child poverty, Heimer and Palme (2016) address the issue of children being only indirect receivers of income or services through the family as a unit. According to a report from the Swedish Ministry of Health and Social Affairs (Nyman & Lönnerheden, 2004), social workers usually only focus on the needs of the adult service users and rarely reflect on the child's situation. In a qualitative study conducted in Norway, six NAV counselors were interviewed (Krane et al., 2018). None of the counselors spoke with the children directly, despite the children's right to have a saying in cases affecting them. Krane et al. (2018) point out that the family's economy significantly impacts the conditions for children's upbringing, and talking to the children could help ensure that their needs are secured, both short term and long term.
The Ombudsman for Children in Norway (2017) is concerned that decisions affecting children are too often made without review and assessment of the best interest of the child. A report from The Norwegian Board of Health Supervision (2013) revealed serious shortcomings in the majority of the inspected municipalities, in particular with respect to lack of information and assessment of children's situations and needs when providing financial support benefits. According to the Ombudsman, the results were disturbing, and 49 of 70 municipalities committed offenses. The CRC is not sufficiently implemented in practices at NAV, and there is a need for training and guidance of counselors at NAV on the CRC (The Ombudsman for Children in Norway, 2017). Professionals working with children need knowledge about the CRC, in addition to knowledge about and guidelines for how to apply the convention in practice. The Ombudsman for Children in Norway (2017) recommends systematic training for professionals and information on CRC in all relevant educational institutions. To prevent child poverty in Norway, it is important to train social workers to discover children who are stigmatized and marginalized (Tjelflaat, 2014). Social workers are in a position to help these children by securing a good childhood and prevent further problems, and they must therefore also cooperate with other institutions in the process of helping (Tjelflaat, 2014).
Aims
There are few studies on child-focused practice in social services for adults. The fact that children are not the primary clients at NAV has not only influenced practice among NAV counselors, but also the research field. The research field also mainly concentrates on child-focus practice in services that are in direct contact with children. Yet, insofar as children's rights and children's welfare is a matter of concern, it is important to know how and to what extent NAV counselors take children of social service users and their interests into consideration. The overall purpose of this study was to explore the child focus in current social work practice of counselors at NAV. Additional aims were to:
assess NAV counselors’ levels of knowledge about the CRC and to what extent NAV counselors applied this knowledge in their social work practice. investigate how knowledge and use of the CRC, usefulness of collaboration and perceived quality of the office's system, routines and guidelines were associated with a child-focused practice in NAV, and subsequently investigate which of these factors predict a child-focused practice. investigate differences in terms of knowledge and use of the CRC, usefulness of collaboration and perceived quality of the office's system, routines, and guidelines for NAV counselors asking about children, compared to NAV counselors not asking.
Method
Procedures and participants
This was a cross-sectional study. The two participating NAV agencies in this survey had received grants from the Directorate of Labor and Welfare through the Childhood Poverty Project. To ensure variation in the sample, the agencies were of different sizes and located in different municipalities and regions. The contact person at the NAV agencies distributed the survey to the staff.
In smaller agencies, all employees are responsible for a diversity of services provided by NAV, while in bigger agencies employees are more specialized. All counselors in participating agencies with user contact were invited to take part in the survey, regardless of their area of responsibility, because a child focus should be a fundamental premise for all the organization's activities. Participants were provided with a link to the survey in the data collection program SurveyXact via email. Reminders were sent three times over a three-week period. In 2015/2016, 93 social workers completed the survey. The overall response rate was 67%, representing 11 workers from the smaller agency and 82 from the larger agency. Demographic information about the participants was not collected to ensure the participants’ anonymity.
The largest participating agency in this study serves around 75,000 people, and the other agency serves around 4,000 people. In these two municipalities, around 450 receivers of social help benefits had children under 18 years, representing more than 820 children living in families that received social help benefits. Nationwide, a total of 66,902 children live in families that receive social help benefits (Statistics Norway, 2018b). In the municipalities included, 22% of social benefits receivers had minor children in 2016. Nationwide, the 2016 number was 25%. NAV also provides other benefits and services and is therefore in contact with social service users with and without children. However, these numbers indicate what percentages of NAV clients are also parents, and how many children are affected.
Measures
The county governor in Troms, the project coordinator, and two NAV counselors developed the survey. Only one demographic item was included in the survey, identifying at which of the offices the participants worked. Other demographical items were not included to avoid the possibility of indirectly identifying participants. To ensure the agencies’ anonymity, the variable identifying workplace was removed. The survey included the following topics: child-focused practice, knowledge and use of the CRC, collaboration, and the office's systems, routines, and guidelines.
Child-focused practice
To measure the NAV counselors’ practice considering a focus on the clients’ children, four items were included:
“In your work as a counselor: When you meet a new user, do you ask whether the user has dependent children or caring responsibilities?” “Do you assess the case differently if the user has children?” “In meetings with users who have children, do you assess the children's needs?” “Do you ask users what their children need?”
All four items measuring child-focused practice were scored from “never” (1) to “always” (5). These four items were included in the scale “Child-focused practice.” The reliability analysis of the scale had a Cronbach's α coefficient of 0.78, indicating an acceptable internal consistency of the scale.
NAV counselors who did not answer “always” to item 1 were given an open-ended follow-up question: “What is the reason that you do not always ask if the user has children?” The answers were recoded into five different categorical values: “I do not think of it or remember to,” “I already know,” “It is not relevant,” “I do not prioritize it,” and “I consider it unlikely because of the user's age or situation.”
A new variable “Askers” was created by recoding the variable “Reasons for not asking about children” into two groups: (1) “NAV counselors who do not ask about children” and (2) “NAV counselors who ask about children.” Those who always ask and those who already know were assigned to the group “NAV counselors who ask about children,” and those who do not think of or remember to, find it not relevant, do not prioritize it or consider it unlikely because of the social service users’ age or situation were assigned to the other category.
Knowledge and use of the CRC
To measure NAV counselors’ knowledge and use of the CRC, three items were included and scored using a 5-point Likert scale:
“How relevant do you consider the CRC to be for your work at NAV?,” scored from “totally irrelevant” (1) to “highly relevant” (5). “How well do you know/what is your level of knowledge about children's rights, as determined by the CRC?,” scored from “no knowledge” (1) to “high degree of knowledge” (5). “Is the CRC something you use in the assessment when you supervise clients, or when you process or conclude in cases involving clients who have children?,” scored from “never” (1) to “always” (5). The alternative “not relevant” (6) was recoded to “never” (1).
These three items were included in the scale “Knowledge” and tested for reliability. The Cronbach's α coefficient was 0.73, indicating that the scale had acceptable internal consistency.
Collaboration
One item measured how NAV counselors perceived the usefulness of collaborating with other institutions in cases involving children by asking “How do you perceive how useful it is for the office to collaborate with local institutions in cases concerning children?” The response scale went from “extremely useless” (1) to “extremely useful” (5). A “don't know/not relevant” alternative was also included in the survey.
The office's systems, routines, and guidelines
One item measured NAV counselors’ perception of the office's systems, routines, and guidelines for promoting a child-focused practice by asking “Do you think the office has systems, routines and guidelines etc. that promote a child-focused practice?” Response options were given on a five-point scale from “no systems” (1) to “very good systems” (5).
Statistical analysis
Data from the survey were exported from Excel files into SPSS. Statistical analyses were done using SPSS (Version 25), except for the confirmatory factor analysis (CFA), which was performed in Mplus (Version 8).
We created a model with the two latent variables “Knowledge” and “Child-focused practice” from seven items based on the thematic content of the questions. To test the fit of the created scales, a CFA was conducted. We compared the general model where all seven items loaded on the same general latent variable to our model with the two latent variables. The reliability of the scales was also tested.
Descriptive analyses were performed to describe the level of knowledge and child-focused practice among NAV counselors.
The relationships between child-focused practice and knowledge and use of the CRC, perceived quality of the offices’ systems, routines, and guidelines, and usefulness of collaboration were explored using Kendall's tau correlation coefficient, two-tailed.
To detect how well the factors of knowledge and use of CRC and perceived quality of the office's systems, routines, and guidelines were predicting a child-focused practice, a multiple regression analysis was conducted. The dependent variable was the child-focused practice scale variable. “Collaboration” was not included in the analysis as a predictor due to missing values. Including the variable would result in a sample size too small for generalizability.
An independent sample t-test was performed to compare mean scores of knowledge and use of the CRC for NAV counselors who do ask about children and for those who do not, using the variable “Askers” (n = 84). We tested for difference in knowledge and use of the CRC using the scale variable “Knowledge.” We calculated the effect size in the t-test using Cohen's d. Criteria used to evaluate the Cohen's d were in accordance with Cohen's (1988) effect criteria, where d = 0.2 is considered a small effect, d = 0.5 is considered a medium effect and d = 0.8 is considered a large effect. Additionally, we conducted an ordinal regression analysis to test for differences between the two groups for the ordinal variables “Collaboration” (n = 59) and “System/Routines/Guidelines” (n = 84).
The data had few missing values overall. The variable “Collaboration” had some answering in a response category labeled “not relevant/I don't know.” This category was labeled “missing” before the independent sample t-test and the ordinal regression analyses were conducted.
Results
Confirmatory factor analysis
The two tested models from the CFA are illustrated in Figure 1. The general model, model 1, where all items load on the same general latent variable, had a value of 40.728 on the χ2 test of model fit, and was significant (p = .0002). The root mean square error of approximation (RMSEA) estimate was 0.143, the comparative fit index (CFI) was 0.96 and the Tucker Lewis index (TLI ) was 0.95. In the hypothesized model, model 2, four items load on the scale “Child-focused practice” and three items load on the scale “Knowledge.” In model 2, the χ2 test value had decreased to 20.274, and was not significant (p = .08), indicating a nonsignificant misfit. The RMSEA estimate had also decreased to 0.078, and CFI and TLI values had improved (CFI 0.99 and TLI 0.98). A good model should have RMSEA values under 0.05, and CFI and TLI scores larger than 0.95 or 0.97 (Schermelleh-Engel et al., 2003). These results indicate that model 2 is a better fit for the data and is more appropriate for representing what is measured than model 1.
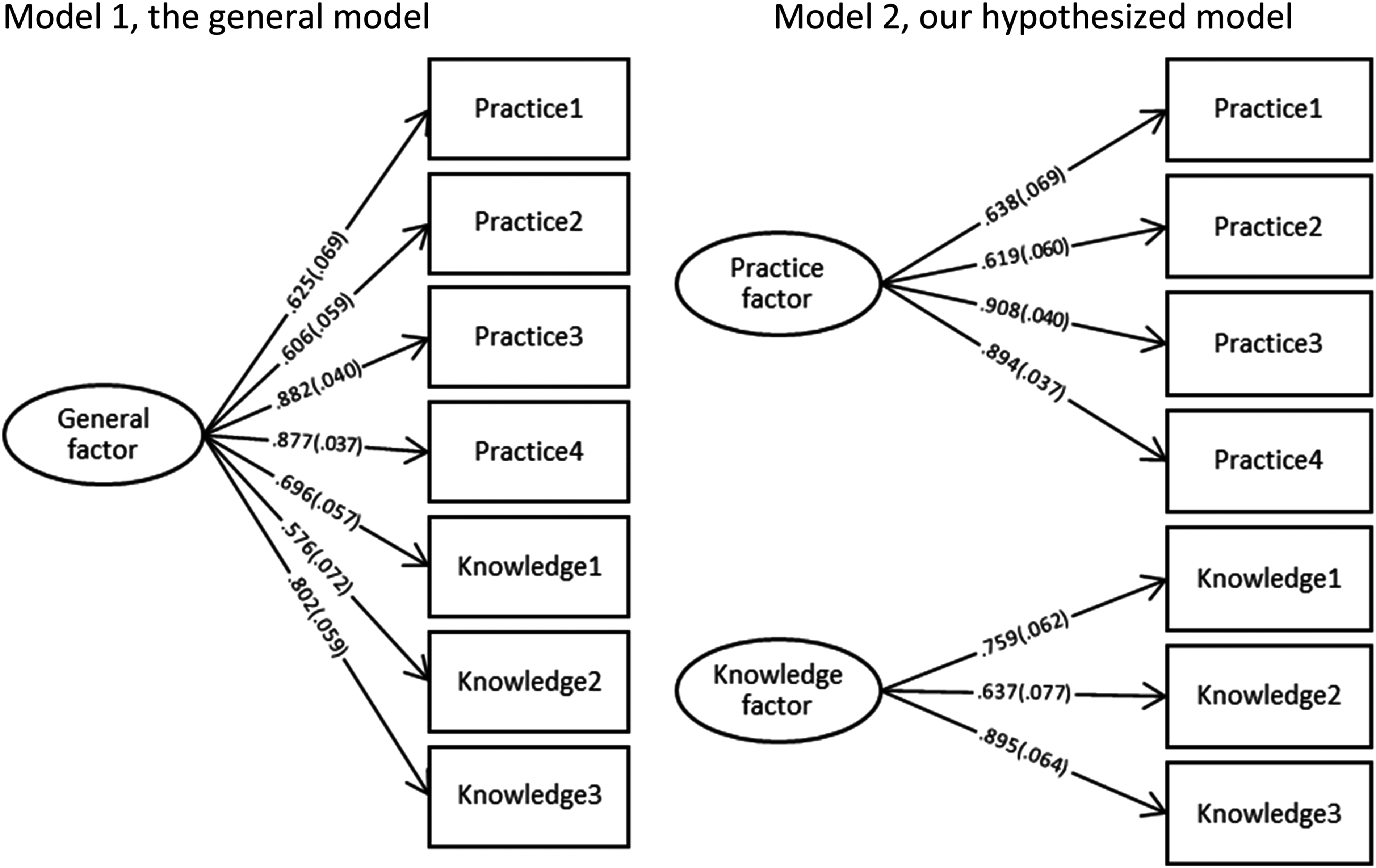
Illustration of the general model and the hypothesized model.
Ideally, the sample size for conducting a CFA should be over 100. Despite our sample being small, we did have a simple and small model with only three to four indicators for each of the two latent variables. We did not have any estimation errors, which also implies that the amount of data is acceptable for testing the models.
Level of child-focused practice and knowledge and use of CRC
As many as 74.2% of NAV counselors answered that they “never” (43%) or “rarely” (31.2%) used the CRC when assessing cases involving social service users with children (n = 93) (Figure 2).
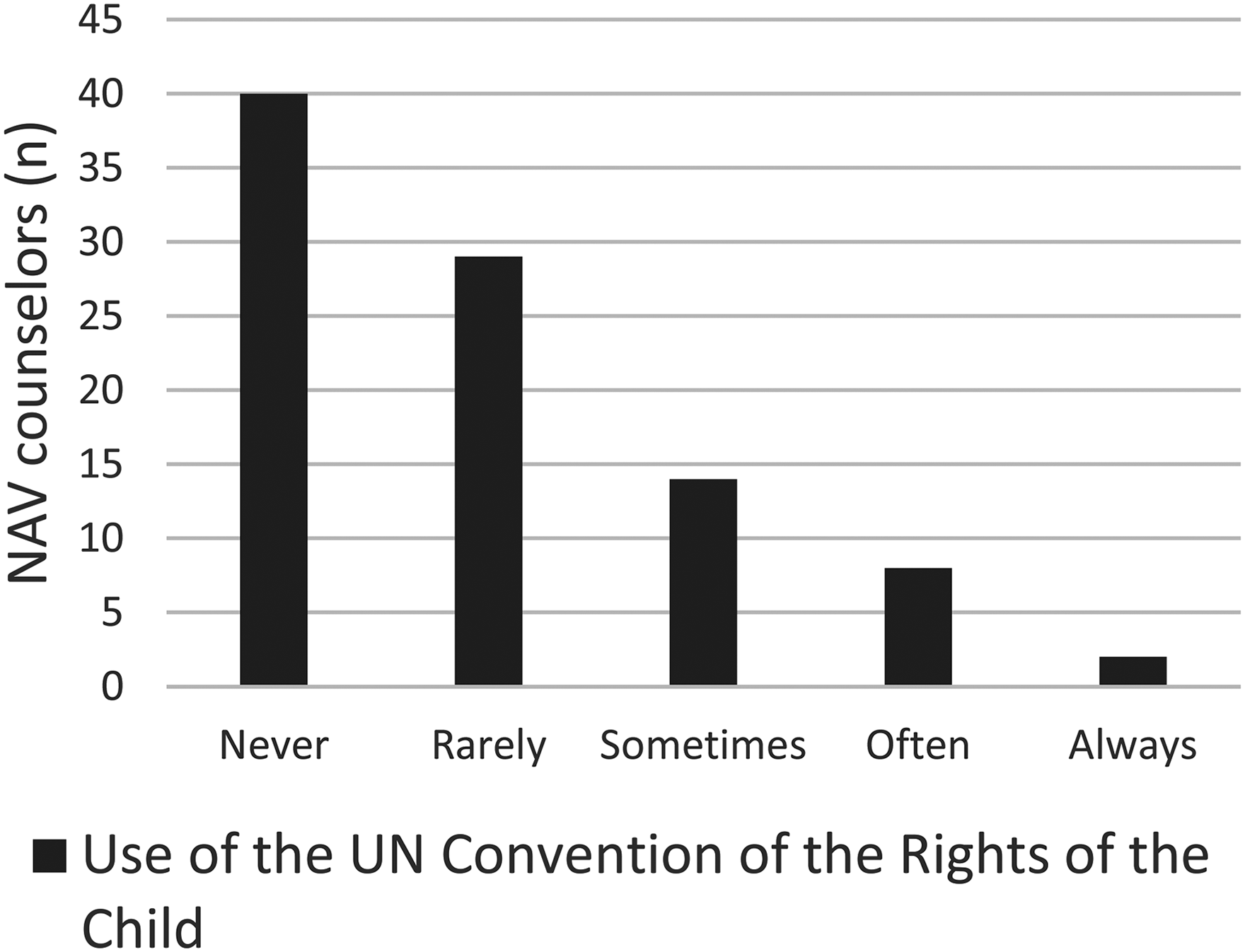
Distribution of NAV counselors’ frequency of use of the CRC.
The computed scale variable “Child-focused practice,” measuring individual degree of assessment of children's needs and how cases are influenced by information about children, had a mean score of 3.36 (SD = 0.86, n = 90).
As shown in Figure 3, 43% of NAV counselors do not ask whether the social service user has children because they do not remember to do so, consider it unlikely because of the social service user's age, life situation etc., consider it irrelevant, or do not prioritize asking.
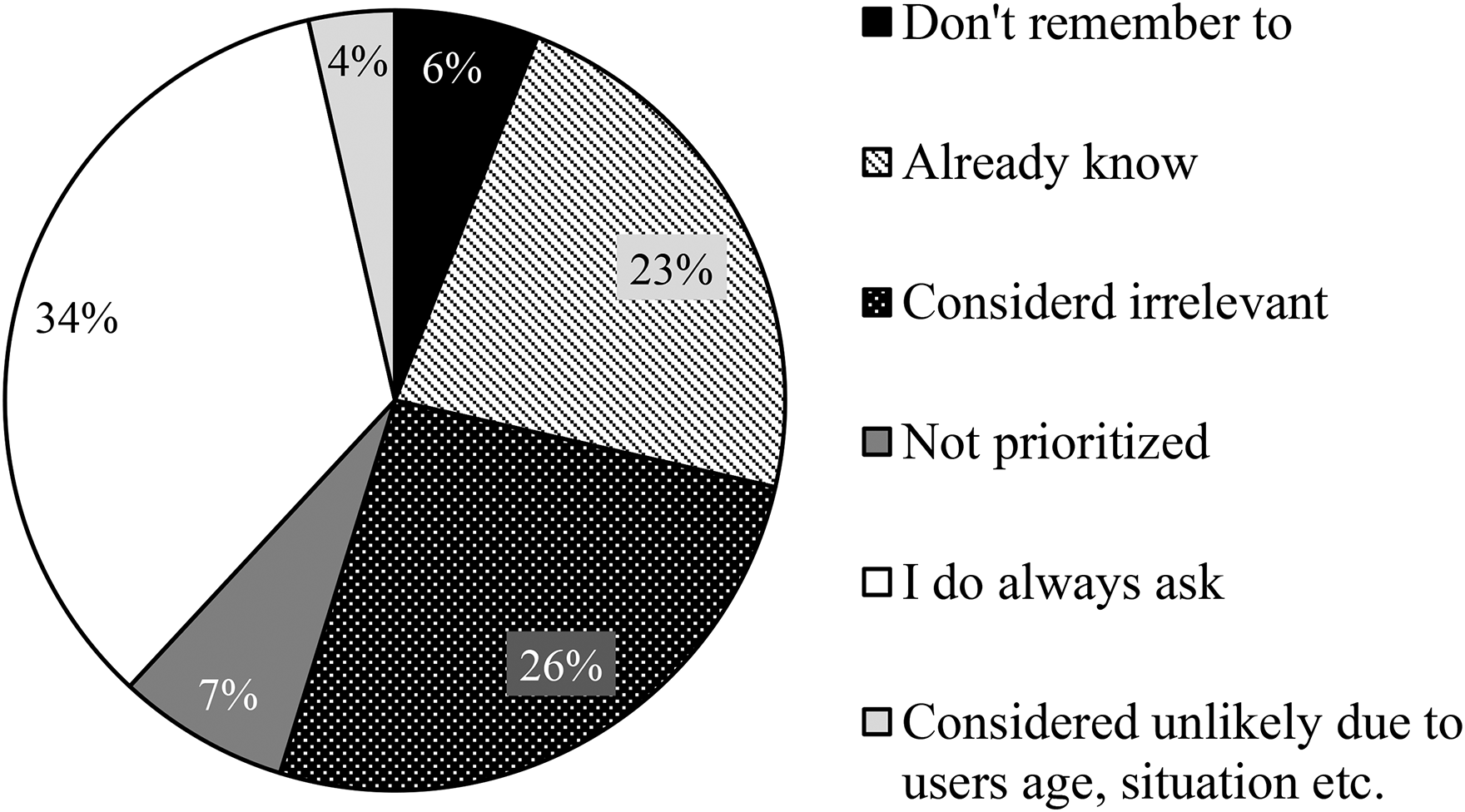
Reasons Norwegian Labor and Welfare Administration (NAV) counselors do not always ask if users have children.
The mean score of the computed scale variable “Knowledge,” measuring knowledge and use of the CRC, was 2.73 (SD = 0.77, n = 93).
Relation between child-focused practice, knowledge, collaboration, and systems/routines/guidelines
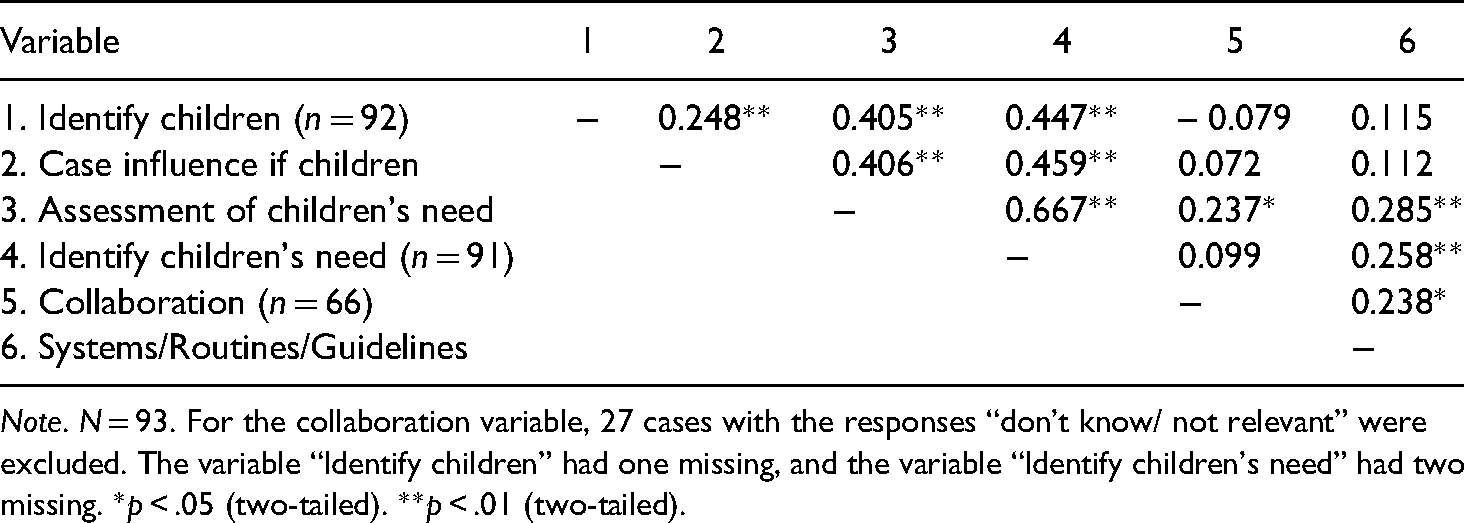
Correlations between child-focused practice and knowledge are shown in Table 1. Identifying children was weakly positively correlated with perceived relevance of the CRC (r = .148, n = 92), and was not significant at the 0.05 level. Identifying children's needs was weakly positively correlated with perceived relevance of the CRC (r = .219, n = 91), and was significant at the 0.05 level. The variable measuring if cases were influenced by the social service user having children and the variable measuring if the counselor used the CRC had a weak positive correlation, significant at the 0.01 level. All remaining correlations between variables measuring child-focused practice and knowledge and use of the CRC had a medium, positive correlation (between 0.310 and 0.472), and was significant at the 0.01 level. High levels of knowledge and use of the CRC are associated with more child-focused practice.
Kendall's Tau correlations between measures of child-focused practice and knowledge.
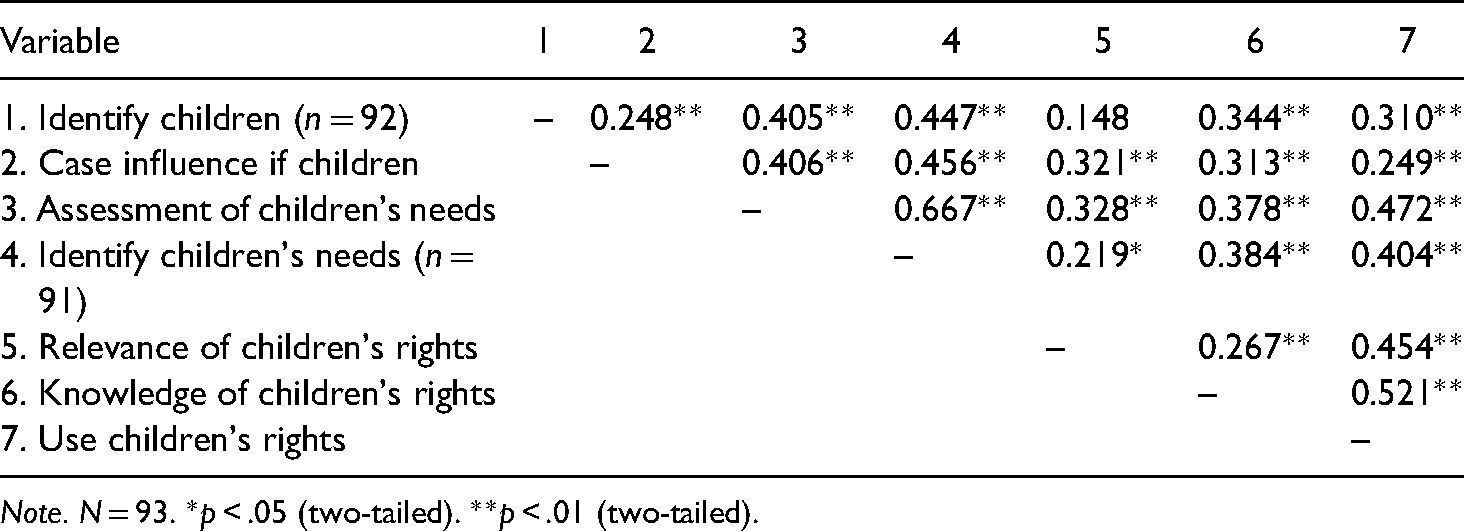
Note. N = 93. *p < .05 (two-tailed). **p < .01 (two-tailed).
Associations between child-focused practice, “Collaboration” and “Systems/routines/guidelines” are shown in Table 2. Higher levels of perceived benefits of collaboration with other local institutions in cases concerning children are weakly positively associated with NAV counselors more often assessing children's need (r = .237, n = 66, p < .05). Perceived quality of the offices’ systems, routines, and guidelines to ensure a child-focused practice was weakly positively associated with assessment of children's need (r = .285, n = 93, p < .01) and identifying children's needs (r = .258, n = 91, p < .01).
Kendall's Tau correlations between measures of child-focused practice and collaboration and systems/routines/guidelines.
Note. N = 93. For the collaboration variable, 27 cases with the responses “don't know/ not relevant” were excluded. The variable “Identify children” had one missing, and the variable “Identify children's need” had two missing. *p < .05 (two-tailed). **p < .01 (two-tailed).
Univariate general linear model
The results from the linear regression for child-focused practice (Table 3) show that the total variance explained by this model was 41%. Knowledge and use of the CRC makes the strongest significant unique contribution to explaining child-focused practice.
Linear regression for child-focused practice.
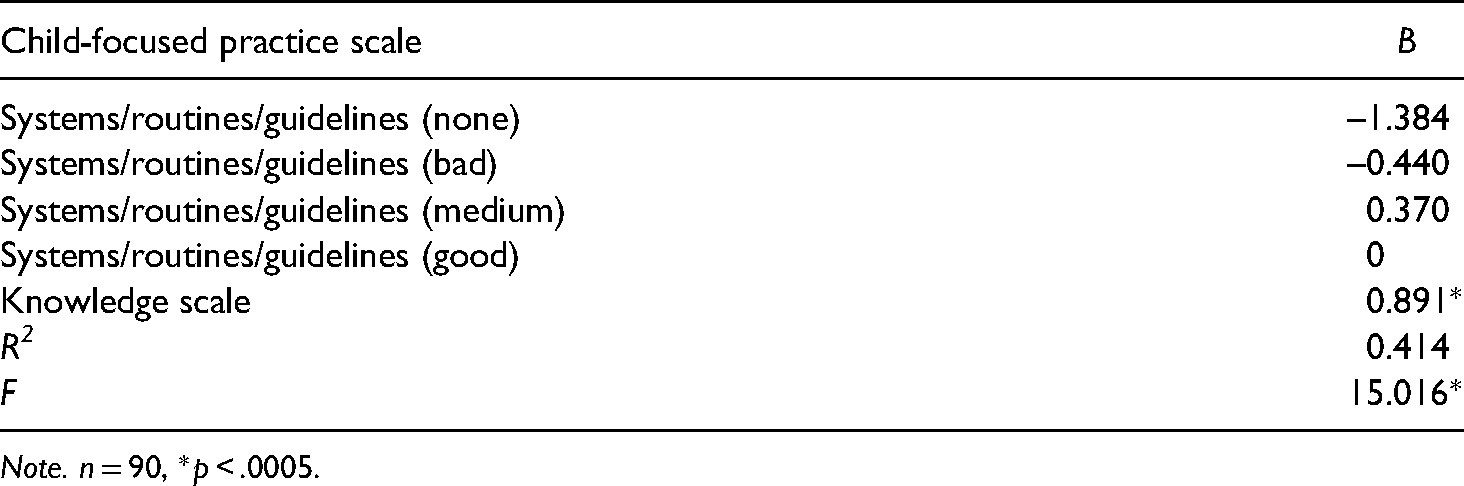
Note. n = 90, *p < .0005.
T-test and ordinal regression analysis—comparing NAV counselors who ask to NAV counselors who don't ask
As shown in Table 4, there was a significant difference in the mean score of knowledge and use of the CRC for NAV counselors who do ask about children (M = 8.77, SD = 2.43) and NAV counselors who do not ask about children (M = 7.44, SD = 2.13; t (82) = –2.61, p = .011 two-tailed). The magnitude of the differences in the means (mean difference = –1.33, 95% CI: –2.34 to –0.31) was of a medium effect size (Cohen's d = 0.58), according to Cohen’s (1988) effect criteria.
Independent sample T-test of differences between Norwegian Labor and Welfare Administration (NAV) counselors who ask about children and NAV counselors who do not ask about children in terms of the knowledge scale.
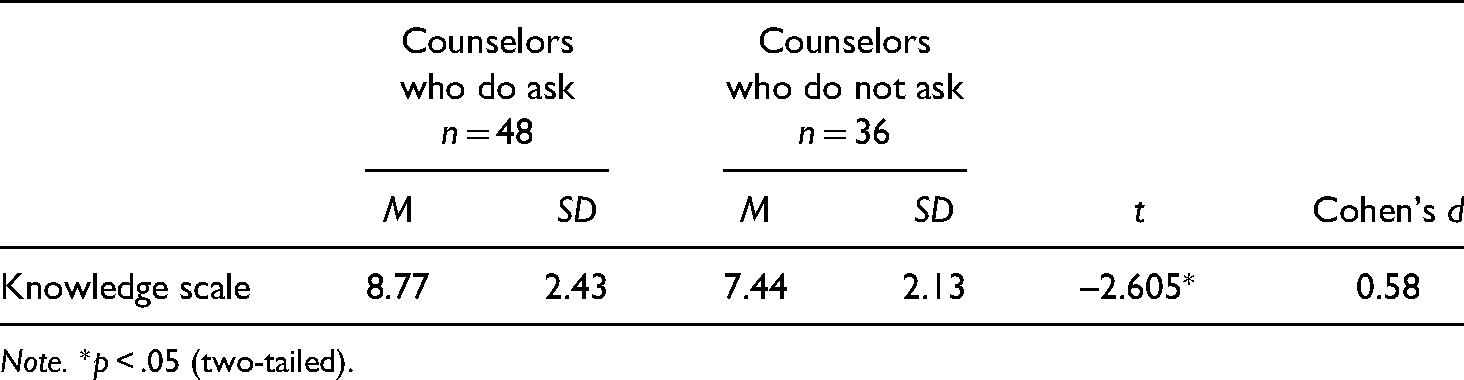
Note. *p < .05 (two-tailed).
There were no significant differences between askers and non-askers for “Collaboration” (Wald = 3.141; p > .05) or for “Systems/routines/guidelines” (Wald = 2.772; p > .05).
Discussion
This study explored the practice of NAV counselors in terms of having a child focus in their social work practice. We also aimed to determine NAV counselors’ level of knowledge about the CRC and the degree to which this knowledge was used in their social work practice. According to the CRC, counselors should give children a chance to express their views. When counselors are making decisions the needs and the situation of user's children should be a primary concern. The level of child focus among NAV counselors was not in compliance with the legislation.
Child-focused practice
NAV counselors rated their level of child-focused practice at 3.36 on a 5-point scale, indicating that a child-focus informed their practice, on average, between “sometimes” and “often.” For various reasons, 43% of NAV counselors reported that they did not always ask if a social service user had children, meaning that almost half of the NAV counselors had not established a routine for always asking whether the social service users were parenting minor children. In addition, approximately one out of four considered asking about the issue to be irrelevant. By law, NAV counselors are obligated to consider the children in all cases affecting them. This means that it is reasonable to claim that the number of NAV counselors who consider the needs of the children of social service users is lower than it should be. When most social workers do not even ask whether social service users have children, it is obvious that common practice is not in line with the requirements of the law. A study on health professionals’ awareness and support of patients’ children found results suggesting that to have a focus on children it is not enough to include this obligation in the law (Lauritzen & Reedtz, 2013). Factors inhibiting a child focus were found on several levels. Some of the challenges were related to organization and management, for example, lack of routines, time, training, or interventions. Other challenges were lack of interest, lack of time, reduced capacity within the staff, and reluctance from the users themselves for involving the children (Lauritzen & Reedtz, 2013). This suggests that legislation alone is not sufficient to ensure that there is a child focus in social services.
In this study, higher levels of knowledge and use of the CRC were associated with a child-focused practice. It is not surprising that there was a correlation between the measurements “use of the CRC” and “a more child-focused practice,” because use of the CRC more directly implies asking about children and their needs. However, knowledge of the convention and perceived relevance among NAV counselors were also associated with a child-focused practice. Knowledge and use of the CRC (Knowledge scale) made the strongest significant unique contribution in our model to explaining a child-focused practice, and it can therefore be a predictor of child-focused practice. This implies that it is important to make knowledge about the requirements of the law part of the training program for new counselors at NAV. We were not able to test for confounding factors due to limitations in the data of background variables and other possible variables influencing both knowledge and child focus. In further studies, we recommend controlling for counselors’ area of responsibility, education, and attitudes toward a child focus.
Perceived higher quality of systems, routines, and guidelines was weakly associated with assessment and identification of children's needs. Because most of the participants in the study were from the same office, most of them used the same systems, routines, and guidelines. It might be that counselors who perceive the quality of systems, routines, and guidelines as higher also entertained more positive attitudes toward a child-focus practice. Furthermore, higher perceived benefits of collaboration were weakly associated with higher levels of assessment of children's needs. It is uncertain whether counselors who think collaboration is useful have a stronger focus on children for example because of a successful collaboration, or if a stronger focus on children makes collaboration with other institutions in cases that concern children more useful for the counselors. In addition, factors such as education and positive attitudes toward a focus on children can explain both the usefulness of collaboration and having a more child-focused practice. Further studies should explore these factors to provide more knowledge about factors predicting a child-focused practice. In order to be able to make recommendations for the practice field based on these associations, more research is needed about underlying factors.
Legal basis—levels of knowledge and use of the CRC
NAV counselors’ levels of knowledge and use of the CRC were on average rated a little below a medium level. Given that the CRC is a part of the legal basis for NAV counselors, their level of knowledge and use of the convention should be higher. We were surprised to find that the majority of NAV counselors (74%) reported that they never or rarely used the CRC when assessing cases involving social service users with children. However, it is possible that NAV counselors did have knowledge about the importance of considering the children in making decisions affecting them without knowing that this is a right given by law, and without linking it to the CRC. Therefore, this measurement does not provide the total picture of NAV counselors’ level of knowledge about the actual content of the convention. However, earlier studies and reports support the finding that social care workers lack knowledge about children's rights (Krane et al., 2018; Nyman & Lönnerheden, 2004; The Ombudsman for Children in Norway, 2017).
Counselors asking about children
When comparing counselors who asked about children to those who did not, there were no significant differences between the groups with regard to collaboration and office routines, guidelines, and systems. There was, however, a significant difference of a medium effect size (Cohen's d = 0.58) for level of knowledge and use of the CRC. “Knowledge” was found to make the strongest significant unique contribution to explaining a child-focused practice. Similar results were found in a study conducted by Lauritzen et al. (2015), where health personnel who identified children of social service users were significantly different from those who did not in terms of knowledge about children and the legislation. The results may indicate that more knowledge about children's rights might explain a child-focused practice. However, it has been well documented that knowledge alone is not enough to change practice (Fixsen et al., 2005). A continued focus on implementation drivers and prerequisites is therefore necessary to increase the focus on children of social service users within social services. Some prerequisites for successful implementation are financial and personnel resources, well-described tools, staff training, and policy support (Fixsen et al., 2005).
Limitations of the study
A limitation of the study is that we were not able to test for confounding factors. For example, associations between a child-focused practice and level of perceived benefits of collaboration might be explained by education or attitudes toward child protection services. NAV counselors’ education might both explain their level of child focus and their level of knowledge and use of the CRC. For instance, counselors with education in child welfare might have a stronger focus on children than counselors with education in economics. Our data material does not encompass the complexity of the NAV system, and more in-depth understanding of the various aspects of the system might help us understand the lack of child focus among counselors. We recommend further studies that include more participants from several randomly picked offices, as well as inclusion of background variables and variables measuring NAV counselors’ attitudes toward cooperating organizations involved in safeguarding children. Such studies may contribute to a better understanding of what factors promote a stronger focus on the children of social workers’ clients.
The three items included in the measure “Knowledge” on the 5-point Likert scales are labeled differently. Computing items with different scale labels can lead to bias in the scale variable and thus affect the results. However, after discretionary considerations we found that the scales are corresponding to a sufficient degree despite different wording in labels. Another limitation of the study is our sample size (n = 93), which is below the recommended limit (n = 100) for conducting a CFA. We therefore decided not to use the latent variables from the CFA in the following analyses. We simply used the CFA to be able to tell whether the created scales “Knowledge” and “Child-focused practice” was a meaningful way to group the variables included in the scales. We chose to use Kendall's tau coefficient to test correlations between variables because of the small data set and because Kendall's tau is a better estimate for correlation in small samples.
There is a weakness of the measurements of collaboration and systems, routines, and guidelines. Measuring only how NAV counselors perceive the quality of collaboration and systems, routines, and guidelines at the office gives us limited information about the objective quality of these elements and how they influence child-focused practice. An inclusion of validated measurements for collaboration and systems, routines, and guidelines would be beneficial to determining whether these factors are predictors for child-focused practice. This limitation also applies to the other measurements in the study. However, the CFA analysis strengthened the measurements for child-focused practice and knowledge and use of the CRC.
Most of the participants in our sample were from the same NAV agency. Having a diverse sample from different offices would likely have made our sample more representative for NAV counselors at NAV agencies as a general group. The participating agencies had received grants from the poverty project, which may have influenced the agencies by increasing awareness of children and by making more resources available to support a child focus in their work. Other agencies might therefore have an even lower child-focus practice.
The study was based on self-reported data. The actual level of child-focused practice might therefore deviate from our reported findings.
Conclusion and implications
The overall purpose of this study was to explore the current social work practice among NAV counselors when it comes to having a child focus. We found that NAV counselors had some degree of focus on the children of social service users. However, a focus on children was not routinely incorporated into daily practice. Knowledge about the CRC was associated with a focus on children.
To our knowledge, this is the only study investigating the degree to which practices among NAV counselors are child focused, and the only one to study counselors’ knowledge and use of the CRC. The study suggests that a stronger focus on children of social service users is needed in the social work field, as well as in the political field and in research. NAV is a public agency, and both their goals and funding are partly decided by the sitting politicians. The politicians can influence NAV's focus areas and its financial resources.
NAV provides services for individuals with mental health issues and low socioeconomic status, and social service users are hence often parents of children at risk. The potential for prevention of transgenerational mental illness is considerable in the adult social service sector, and this is something that should be utilized. Counselors at NAV can potentially detect children at risk that are difficult to identify elsewhere. Future studies need to investigate other factors predicting a child-focused practice. Such factors might be background variables for counselors like education, gender and age, their attitudes towards a child focus, and amount of workload. The organization of the NAV office and the counselor's area of responsibility should also be studied as predictors. Prevention effects when awareness and support of children is provided must also be examined. These effects can be studied comparing long-term outcomes for children of service users in offices with a child focus to children of service users in offices practicing as usual.
Research ethics
During data collection, the project was categorized as a quality assurance project. Participation was informed and voluntary. Participants were anonymous during the data collection and throughout the study. Personal data were not processed and data protection services were therefore not notified of the project. After approval from all participating offices and the Directorate of Labor and Welfare, UiT—The Arctic University of Norway, RKBU North received the anonymous data from the directorate and the project manager. As required, participating agencies will not be identified in this publication.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: UiT—The Arctic University of Norway and The Norwegian Directorate of Health financed the study.
Acknowledgements
We would like to thank the project coordinator Janne Wilhelmsen and the county governor in Troms and project manager, Eivind Pedersen for developing the survey and the study procedure as well as for collecting the data. We thank the NAV counselors who participated in the study and The Directorate of Labor and Welfare for making the data available to us. Moreover, we thank Bjørn Helge Handegård, statistician at RKBU North at UiT—The Arctic University of Norway, for support with the CFA analysis in Mplus as well as for providing help with the presentation of the results.