
Abstract
Objective:
To assess the influence of varying degrees of gingival display on perception of smile aesthetics judged by orthodontists, dentists and lay people.
Design:
Cross-sectional study.
Setting:
Barts and the London, School of Medicine and Dentistry, Queen Mary University of London, UK.
Participants:
Three groups of raters comprising 25 orthodontists, 25 dentists and 25 lay people.
Methods:
Videos in increments of 1.5 mm of the final lip position ranging from 3 mm incisal coverage to 7.5 mm of gingival display were produced. Three rater groups assessed the attractiveness of smile videos using a visual analogue scale (VAS). Multiple regression analysis was undertaken, and images were compared using the Tukey HSD method.
Results:
The intraclass correlation coefficient (ICC) was 0.65% (95% confidence interval 0.59–0.71), indicating moderate intra-rater reliability. The highest ranking for female videos was with 1.5 mm of incisal coverage, with no significant difference between 3 mm of incisal coverage and 3 mm of gingival exposure. For the male videos, the highest ranking was 0 mm of gingival show, with no significant difference between 1.5 mm of incisal coverage and 1.5 mm of gingival exposure. There was a significant drop in the scores with further increase in gingival exposure, with more than 6 mm being rated very low aesthetically. Video rating was not influenced by rater group (female: P = 0.60; male: P = 0.06), rater gender (female: P = 0.17, male: P = 0.74) or rater age (female: P = 0.16, male: P = 0.25).
Conclusion:
There is a significant difference in the perception of smile aesthetics with varying amounts of gingival show. There is a clear threshold of acceptance up to 3 mm of gingival display for the female videos and 1.5 mm in for the male videos, after which the aesthetics of the smile decline with increments of increasing gingival display. No significant differences were observed in the perception of smile aesthetics with varying amounts of gingival show between orthodontists, dentists and lay people.
Plain language summary
Introduction
Traditionally, the main premise of dental treatment has largely been focused around restoration of health and masticatory function. Increasingly, however, patients often seek treatment for aesthetic reasons, coinciding with an increased importance placed upon facial aesthetics and, in particular, smile aesthetics in our culture (Sharma and Sharma, 2012; van der Geld and van Waas, 2003). Smile aesthetics are strongly correlated with overall facial attractiveness. Although the eyes typically draw the most visual attention, the presence of malocclusion redirects focus towards the mouth (Almotairy et al., 2025). Therefore, careful assessment of features that contribute to smile aesthetics play an integral role in orthodontic treatment planning to produce beautiful and attractive smiles. In this regard, it is recognised that interplay between visible maxillary gingiva and the framework of the lips during facial expression contribute to smile aesthetics and remain an important consideration (Sharma and Sharma, 2012).
The gingival smile line is where the gingiva superior to the maxillary anterior teeth is exposed during smiling (Peck et al., 1992b). Excessive gingival display is commonly known as a ‘gummy smile’ and is described as overexposure of maxillary gingival band during voluntary or involuntary smiling (Allen, 1988). An excessive gingival display can result from a combination of factors of vertical maxillary excess, short upper lip, increased overjet, increased overbite and a short incisor crown length (Allen, 1988). It can have a significant negative impact on the overall aesthetics of both the smile and face as a whole (Ioi et al., 2010). A low smile line is considered to be a trait of aging and is not typically a desired outcome among patients (Peck et al., 1992a).
Previous research in this area has largely been conducted via the use of static photographs, which does not consider the dynamic aspects of the development of a smile and therefore the effect of this on the overall impact on facial attractiveness. Given the development of a smile is a dynamic and progressive process of facial expression, assessment in static expression has limitations. Although a still photograph might be sufficient to capture the height of the smile, a fixed representation of a facial expression fails to provide enough information for the interpretation of that expression (Ekman et al., 1987). Using techniques to record the entire dynamic range of the smile at rest to smiling captures all features of the facial expression as a whole, thus, significantly improving the diagnostic value compared to only focusing on the static position of a maximum smile.
Although numerous studies have evaluated the effect of excessive gingival exposure on smile aesthetics based on static photographs, research is limited on the influence of gingival display during active facial expression on the perception of smile aesthetics (Walder et al., 2013). This study aims to assess the impact of varying maxillary gingival exposure using dynamic smile videos.
Methods
Participants and methods
Approval to conduct this cross-sectional study was granted by Queen Mary ethics for research committee, Queen Mary University London (reference no. QMREC1646a).
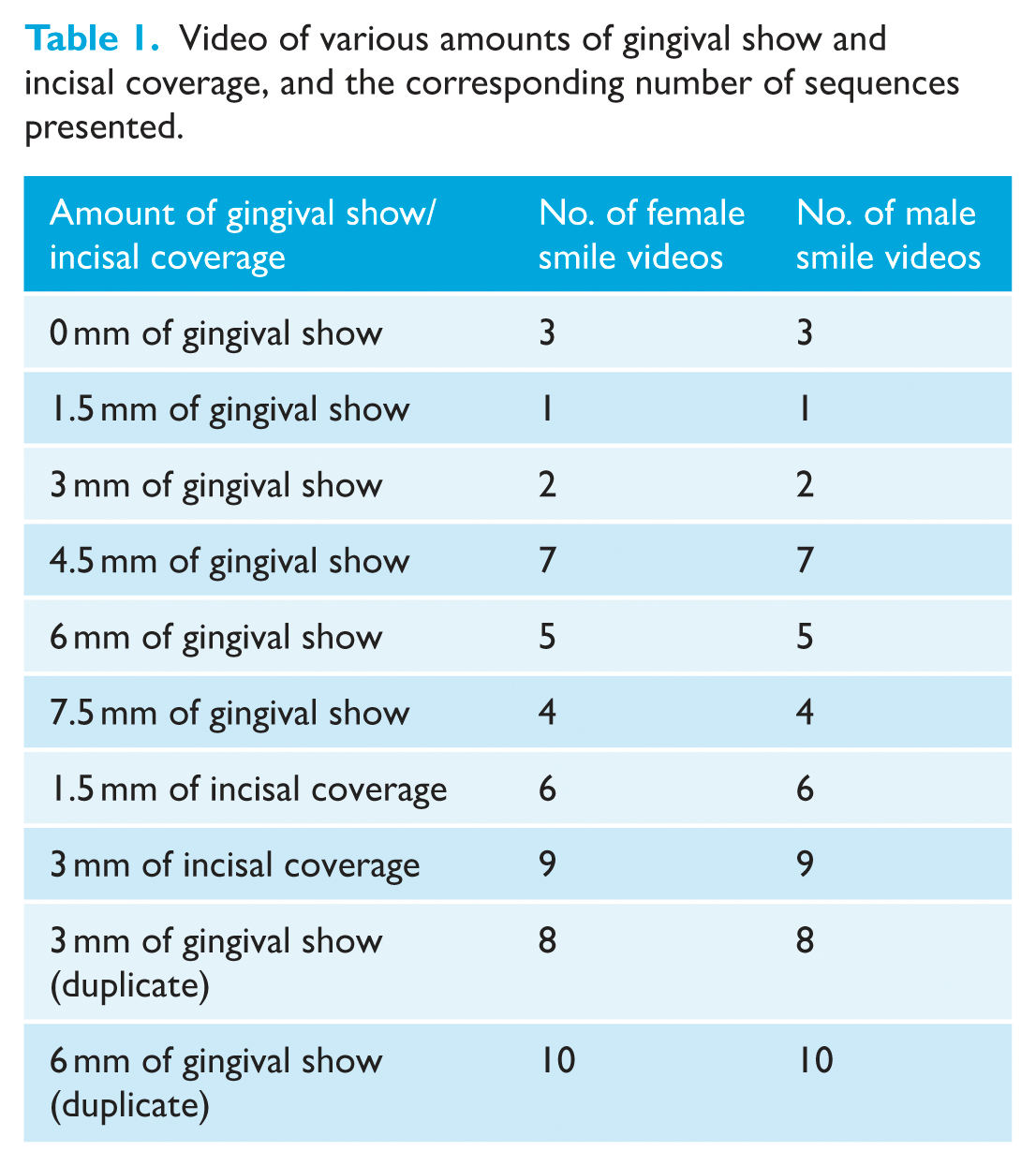
High-definition videos of smiles were purchased from a stock photography website, www.shutterstock.com, which is a source for royalty-free images and videos. These videos were manipulated to display the proposed deviations to maxillary gingival display. The following incremental changes used were as follows: 3 mm incisal coverage; 1.5 mm incisal coverage; 0 mm gingival show; 1.5 mm gingival show; 3 mm gingival show; 4.5 mm gingival show; 6 mm gingival show; and 7.5 mm gingival show (Table 1). The use of increments less than 1.5 mm would have resulted in too many images and risk raters being unable to discriminate between the videos, whereas using increments greater than 2 mm would risk too great a change between images reducing the sensitivity of the study.
Video of various amounts of gingival show and incisal coverage, and the corresponding number of sequences presented.
Adobe Photoshop (Adobe Systems, 2016) and Adobe After Effects (Adobe Systems, 2016) were used for the digital manipulation. The videos were cropped to avoid other facial elements influencing the assessment of the smile and any eye-catching features, such as spots, blemishes and moles, were removed. Manipulation of the image was undertaken with the use of a Mesh Warp (Adobe Photoshop, Version CC 2016, Adobe Systems Inc.), which allowed the video image to be divided into a grid, with each intersection representing a prominent point on the face that could be moved in isolation. This technique allowed for production of a series of images with variations of incisal and gingival show (Figure 1). The gingival smile was manipulated for each of the seven variations by separating the necessary areas inside the mouth into sections so they could be moved and cut out to produce a new digitally painted mouth allowing for up to 7.5 mm of gingival reveal.

Master photographs indicating final lip positions and level of gingival exposure or incisal coverage: (a) female and (b) male.
The master video was prepared at 25 frames per second (fps). Therefore, the manipulation to the still image was done to a constantly changing face that was ultimately made up of approximately 150 still images (i.e. 6 s of video at 25 fps). The video was split into an upper and lower mouth, so that any manipulation to the upper lip did not have an undesired effect on the lower lip line. Finally, the various videos were rendered out to consolidate all the layers and effects into a watchable video. Each video consisted of a 6-s animation, starting from relaxed lips and developing into a full smile as demonstrated in Figures 2. This process produced a total of 16 videos in total (Figure 3).

Stills demonstrating the development of male smile during the animated video (first to final frame of animation) – example of 0 mm of gingival exposure at full smile.
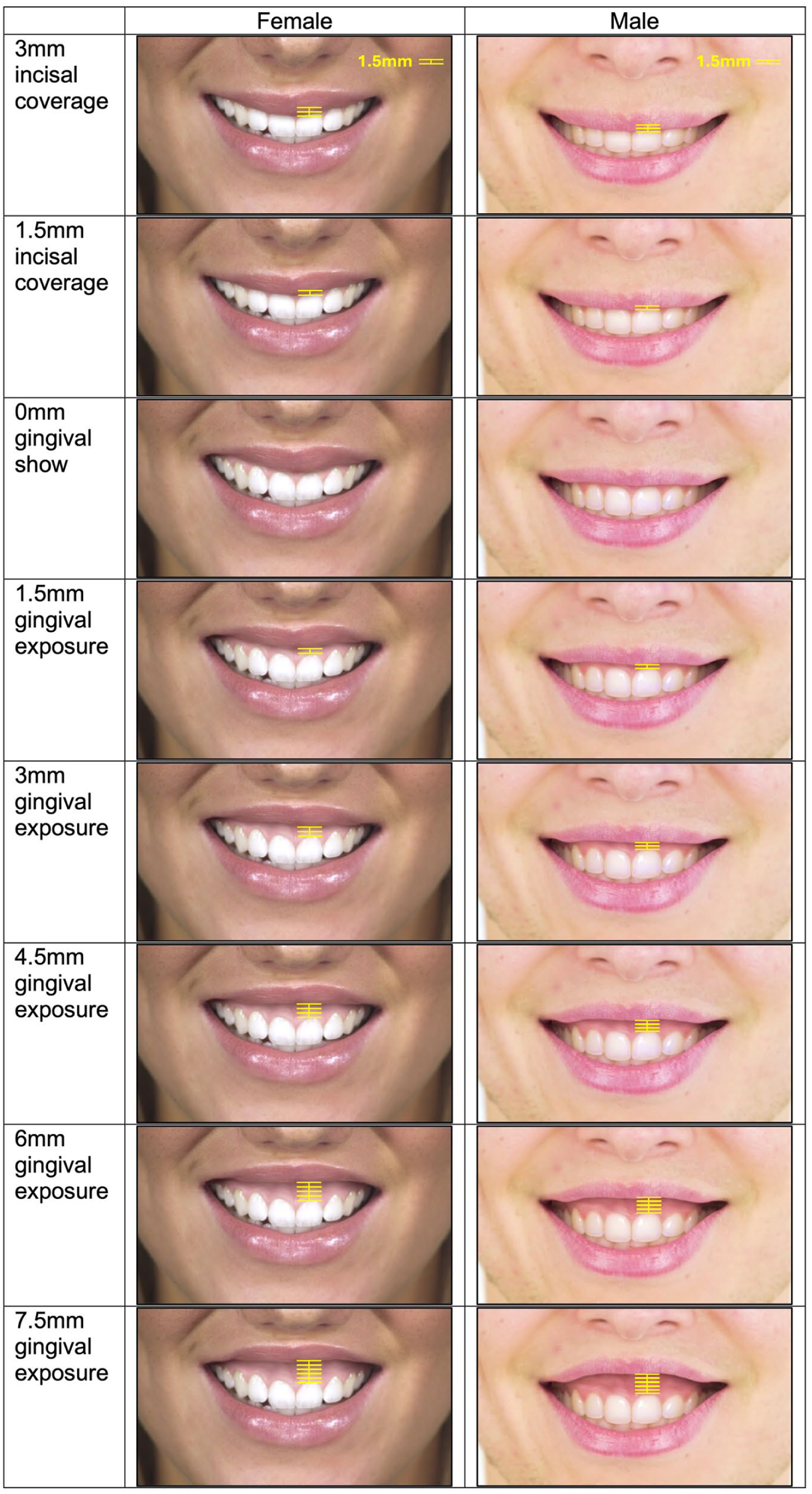
Stills of the maximal gingival display for each female and male video.
Rater groups, presentation of video and assessment method
The rater group consisted of a convenience sample of 75 individuals, divided into three groups of equal sizes: 25 orthodontists, 25 general dental practitioners (GDPs) and 25 lay people. The orthodontists were recruited at the British Orthodontic Conference to ensure a wide mix of backgrounds and level of experience. The GDPs were recruited at a local meeting consisting of practitioners from across East Anglia, ranging greatly in age and level of experience. The lay people were recruited from a combination of parents attending with children at an orthodontic practice in Ipswich and a dental institute in London.
Potential participants read the information sheet attached to the data collection booklet. Once they agreed to participate, they signed a consent form. Instructions were then provided on how to proceed with the study, which were repeated at the start of the video presentation. To facilitate identification of trends or association that may be associated with altered perception of smile aesthetics, the following demographic details were recorded for each participant: age, sex, ethnicity, professional capacity/job title/grade and years qualified (if dentist or orthodontist).
The videos were exported into a Microsoft PowerPoint (Microsoft, 2017) presentation. The videos were presented in a set sequence of female and male smiles as a series of individual 6-s videos, with two videos duplicated to check the intra-examiner validity of the results, thus 20 videos were shown in total (Table 1). Each PowerPoint slide had a different smile video that played automatically once the new slide was selected. Participants were given access to the PowerPoint presentation to view the videos by moving through each slide of the presentation with the 10 female smiles first followed by the 10 male smiles. After viewing each video, the participants completed the corresponding visual analogue scales (VAS) for each video. The participants were instructed to assess and score each video based on gingival display, with 0 being least aesthetic and 10 being most aesthetic.
Pilot study
A pilot study was completed using 12 volunteers. A combination of both clinical and non-clinical staff were chosen to ensure the instructions and study were clear to all participants. The pilot study was completed exactly as outlined above, and feedback was gained for the study. In terms of the clarity of the instructions, video quality and length and the duration of the study, no negative comments were made. No changes were made to the methodology following the pilot study.
Data analysis
Data were analysed using descriptive and analytical statistics using software R 3.4.1. (R Core Team, 2017). Reliability was estimated by an intraclass coefficient (ICC) with a mixed model approach and a Bland–Altman plot for each of the four repeated videos. A multiple regression mixed-models approach was undertaken to take into account the repeated measures structure of the sample. Video ratings were compared using the Tukey honestly significant difference (HSD) method. The level of significance was set at P <0.05.
Results
Reliability was examined for each of the two repeated videos separately. Agreement was estimated visually using Bland–Altman plots with very few observations falling outside the 95% agreement range. The following number of observations fell outside the 95% agreement range: female 3 mm = 3 (4%); female 6 mm = 6 (8%); male 3 mm = 5 (7%); and male 6 mm = 2 (3%) — no clear pattern indicated differences between rater professions (Figure 4). For both pairs of repeated videos, the first seemed to have a wider agreement range, especially for the female smiles (Figure 4). ICC was estimated for all repeated videos together using a linear mixed model, with random effects for each reader and video combination of 0.65% (95% CI 0.59–0.71) indicating moderate reliability.
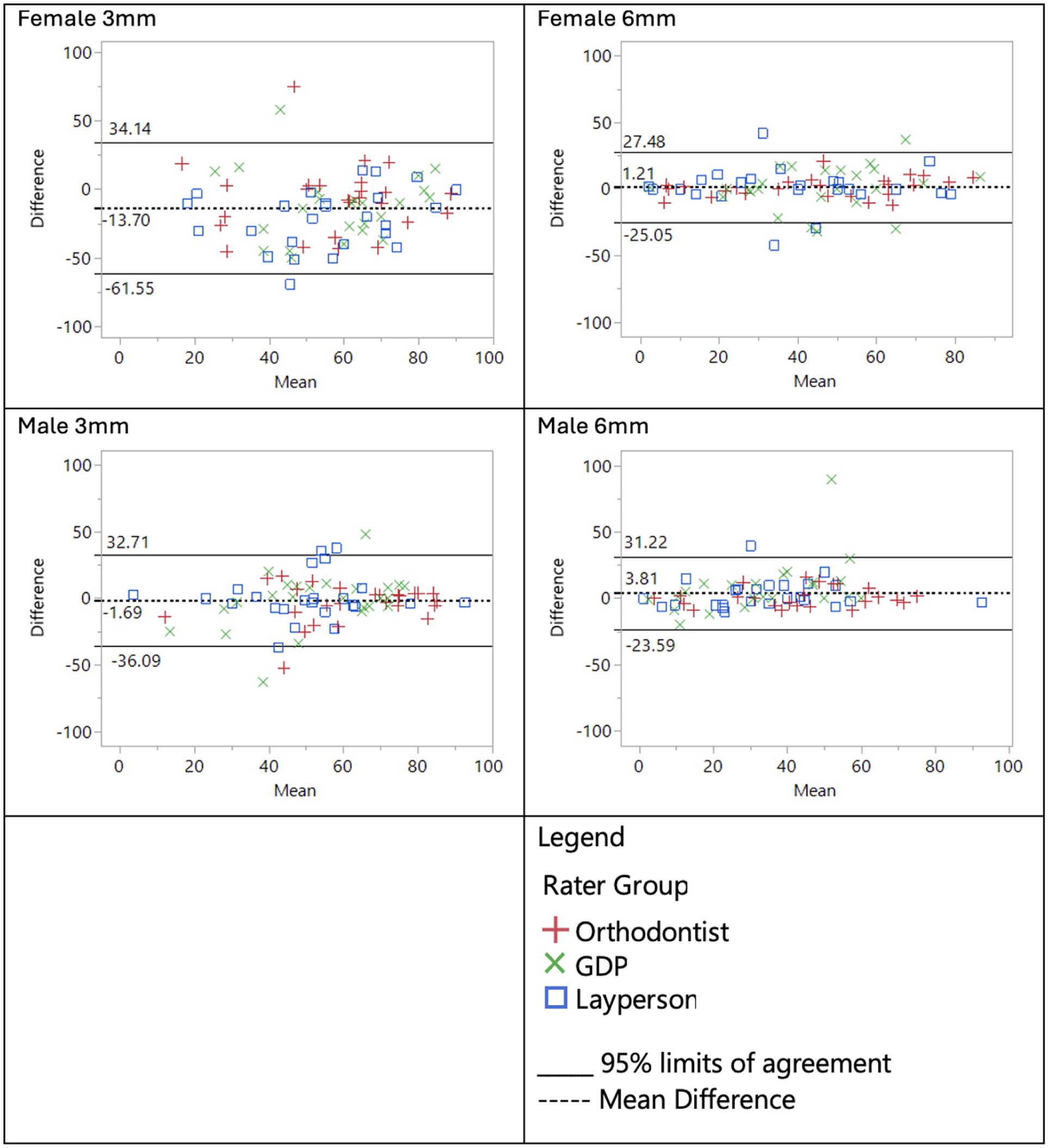
Bland–Altman plots for four repeated videos.
The participants consisted of 75 raters, 25 in each rater group. The mean age of the participants was 46.75 ± 11.62 years. In terms of ethnicity, there were 62 (83%) white/white British raters, 8 (11%) Asian/Asian British, 2 (3%) other raters and one Arab, Chinese and Mixed/Multiple Ethnicity person (Table 2).
Age, sex and ethnicity distribution among all rater groups.
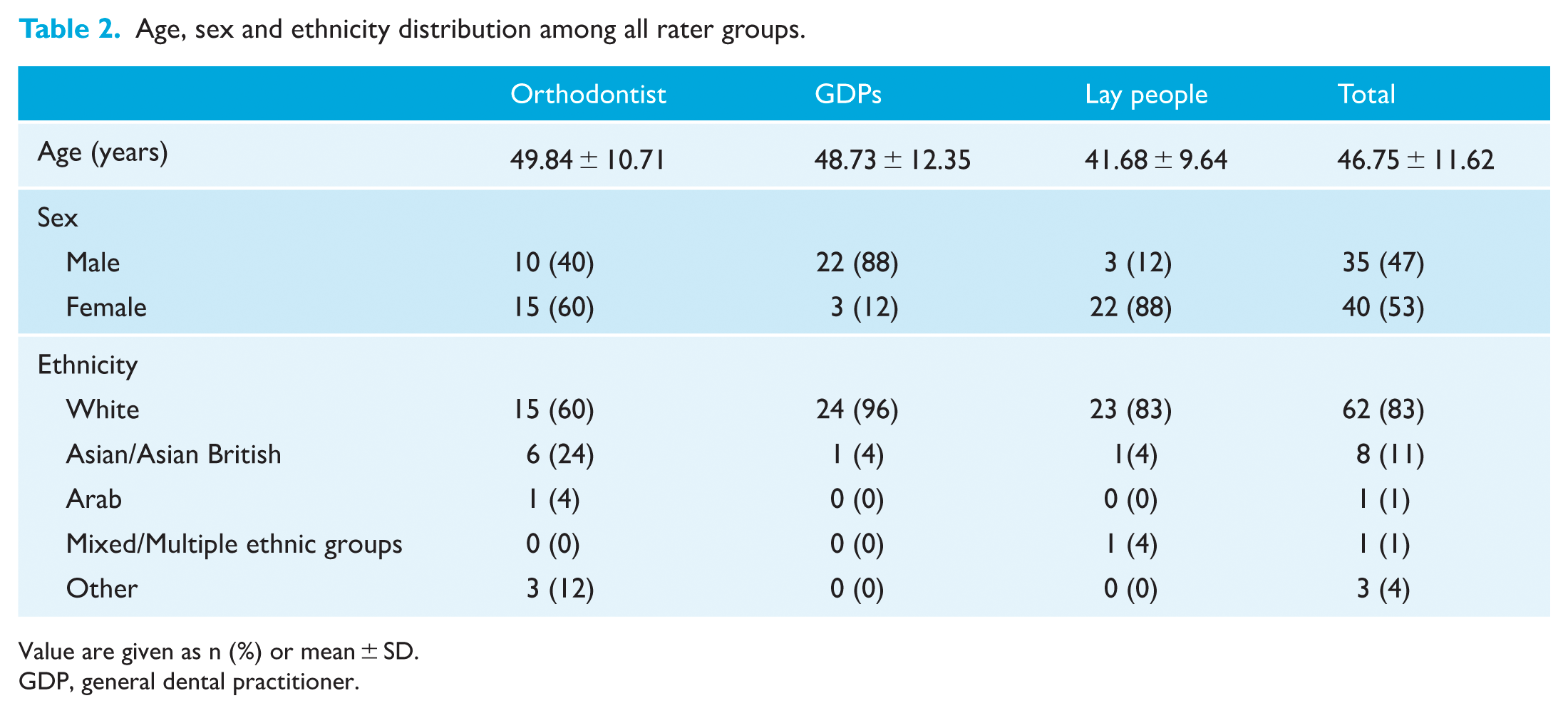
Value are given as n (%) or mean ± SD.
GDP, general dental practitioner.
Mean attractiveness scores are presented separately for male and female videos (Figures 5 and 6). A Tukey HSD compared each pair of videos with one another for significant differences (Tables 3 and 4).
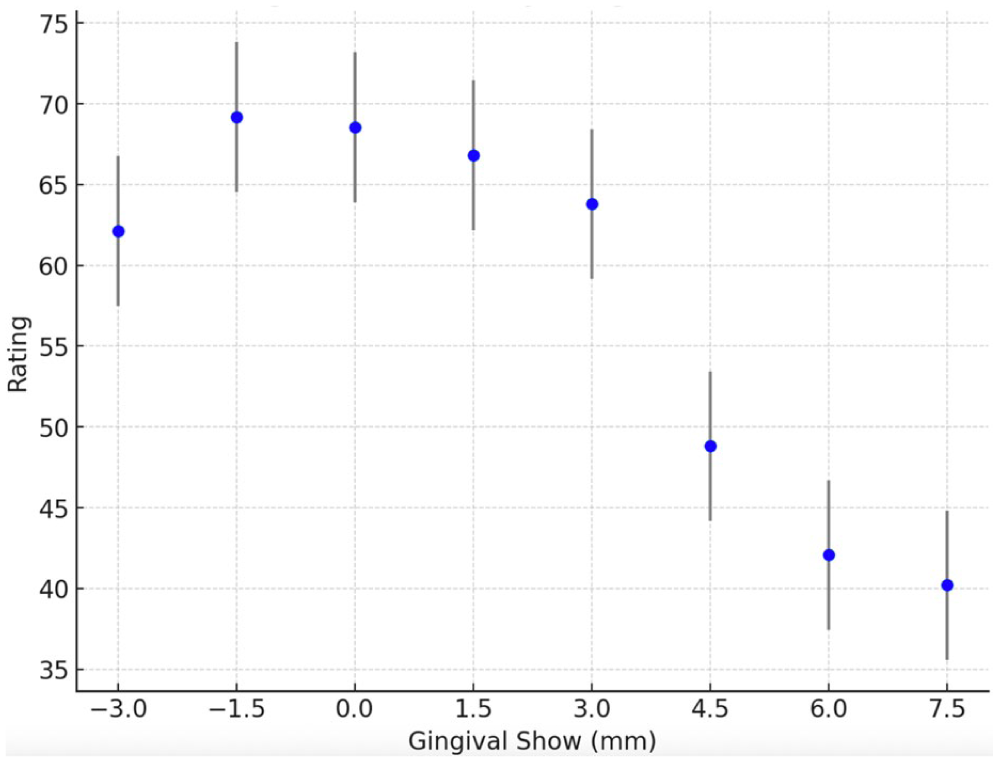
Video ratings – mean and 95% confidence interval for each female video.
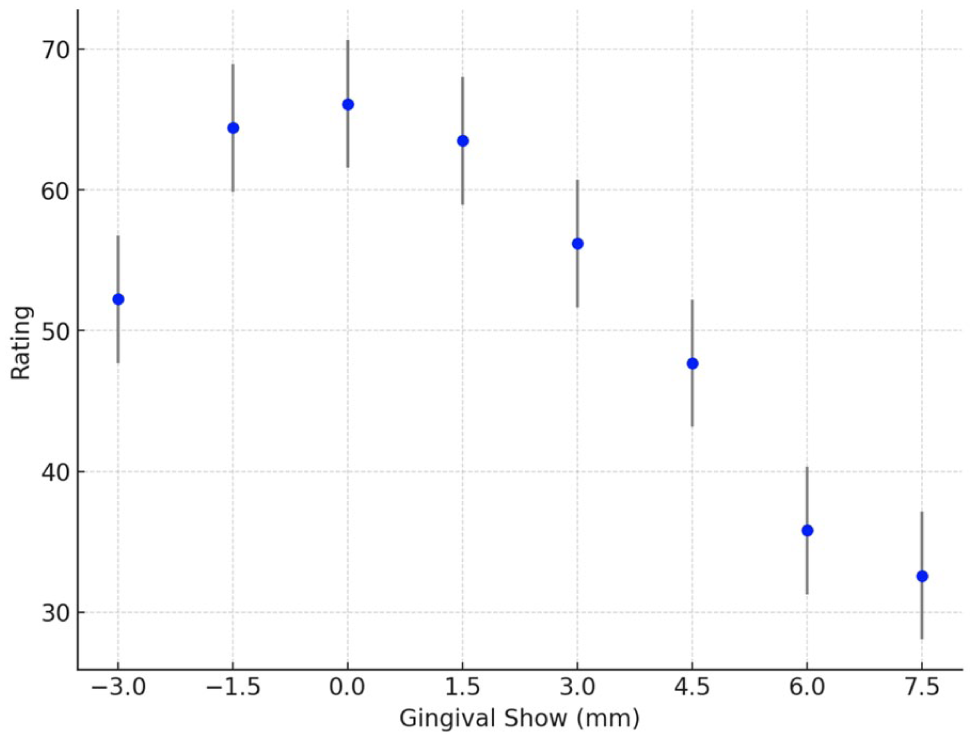
Video ratings – mean and 95% confidence interval for each male video.
Tukey HSD multiple comparisons for female videos.
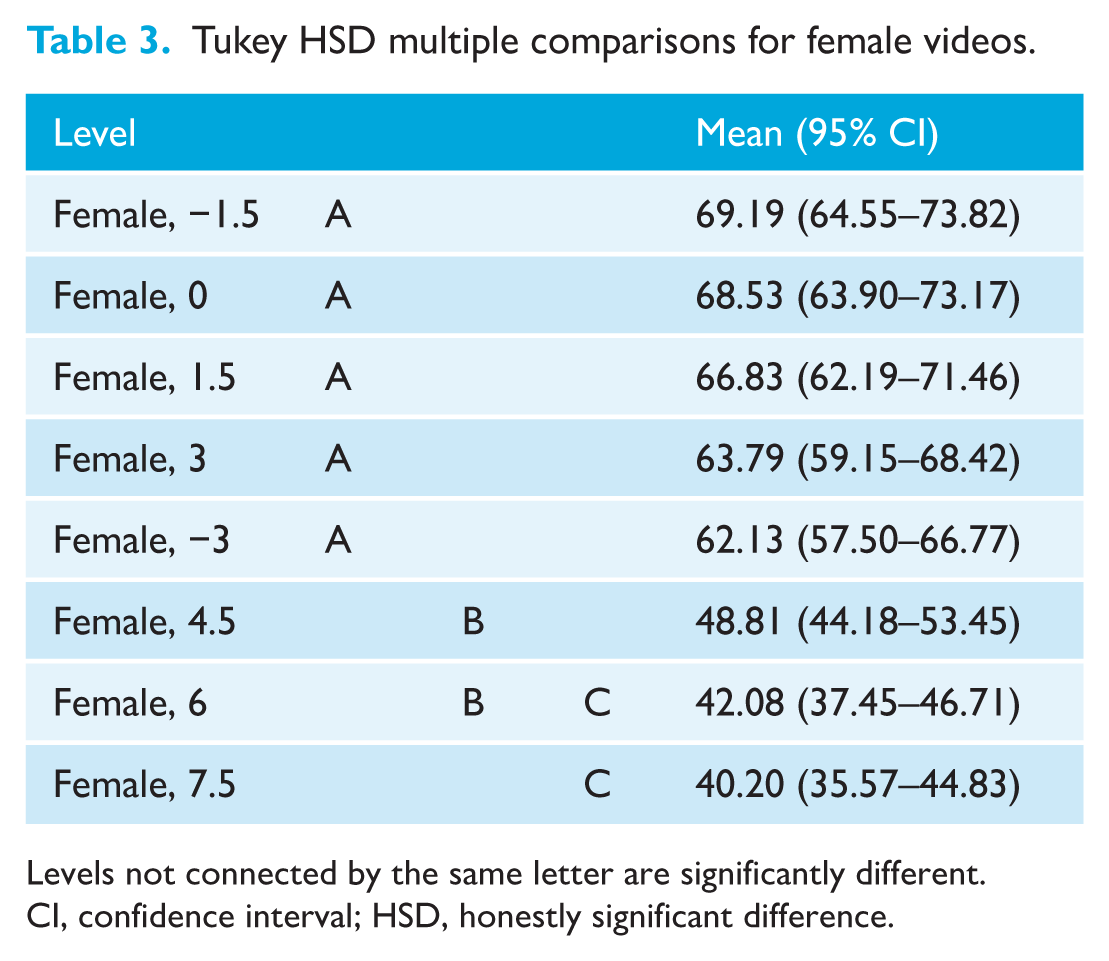
Levels not connected by the same letter are significantly different.
CI, confidence interval; HSD, honestly significant difference.
Tukey HSD multiple comparisons for male videos.
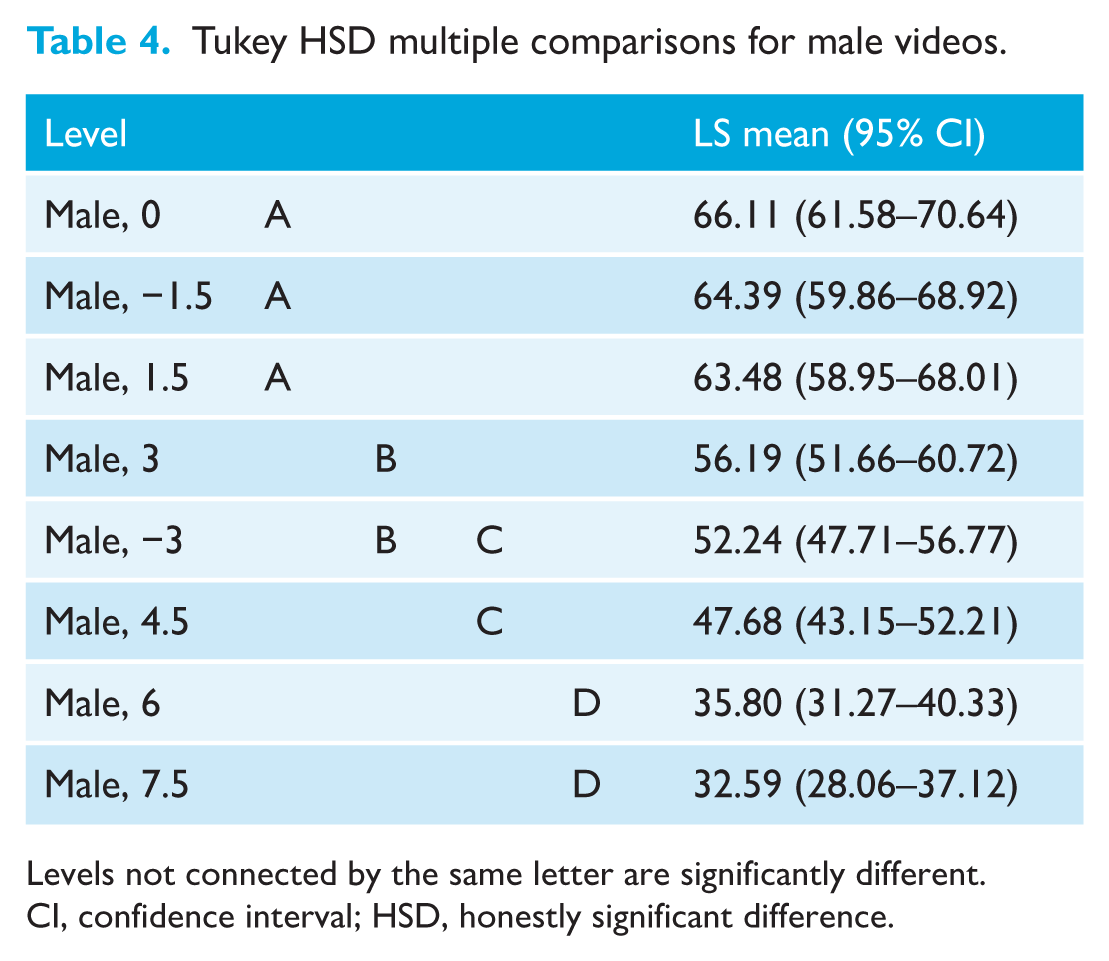
Levels not connected by the same letter are significantly different.
CI, confidence interval; HSD, honestly significant difference.
For the female set of the videos, the highest ranking video was with 1.5 mm of incisal coverage followed by 0 mm, 1.5 mm, 3 mm, −3 mm, 4.5 mm, 6 mm and finally 7.5 mm of gingival exposure. This set displayed a noticeable gap in mean ratings between the −3 mm and 4.5 mm (Figure 5). The Tukey HSD of the five videos with up to 3 mm of incisal coverage to 3 mm gingival exposure was found to be not significantly different. The latter three videos had a significantly lower ranking than the top five and the 7.5 mm was significantly lower than 4.5 mm. Among the three, 6 mm was not significantly different from both 4.5 mm or 7.5 mm (Table 3).
For the male set of videos, the highest ranking was the 0 mm, followed by −1.5 mm, 1.5 mm, 3 mm, −3 mm, 4.5 mm, 6 mm and 7.5 mm of gingival exposure (Figure 6). The Tukey HSD analysis of the videos showed that 1.5 mm of incisal coverage to 1.5 mm of gingival exposure were rated the highest. In the mid-rankings, there was no significant difference between 3 mm of gingival exposure and 3 mm of incisal coverage, while both scored significantly higher than 4.5 mm of gingival exposure. The 6 mm and 7.5 mm gingival exposures were rated significantly lower than the others (Table 4).
Since raters varied in the range and magnitude of the scores they gave across the video set, a mixed effects approach was chosen. In further regression analysis, a separate model was estimated for each set of videos (male and female) to assess the influence of gingival reveal on video rating. The control variables were added one at a time to assess their net contribution to the ratings. Table 5 provides the fixed effects summary for each model by video set and with the additional control variables.
Effect summary table for regression models.
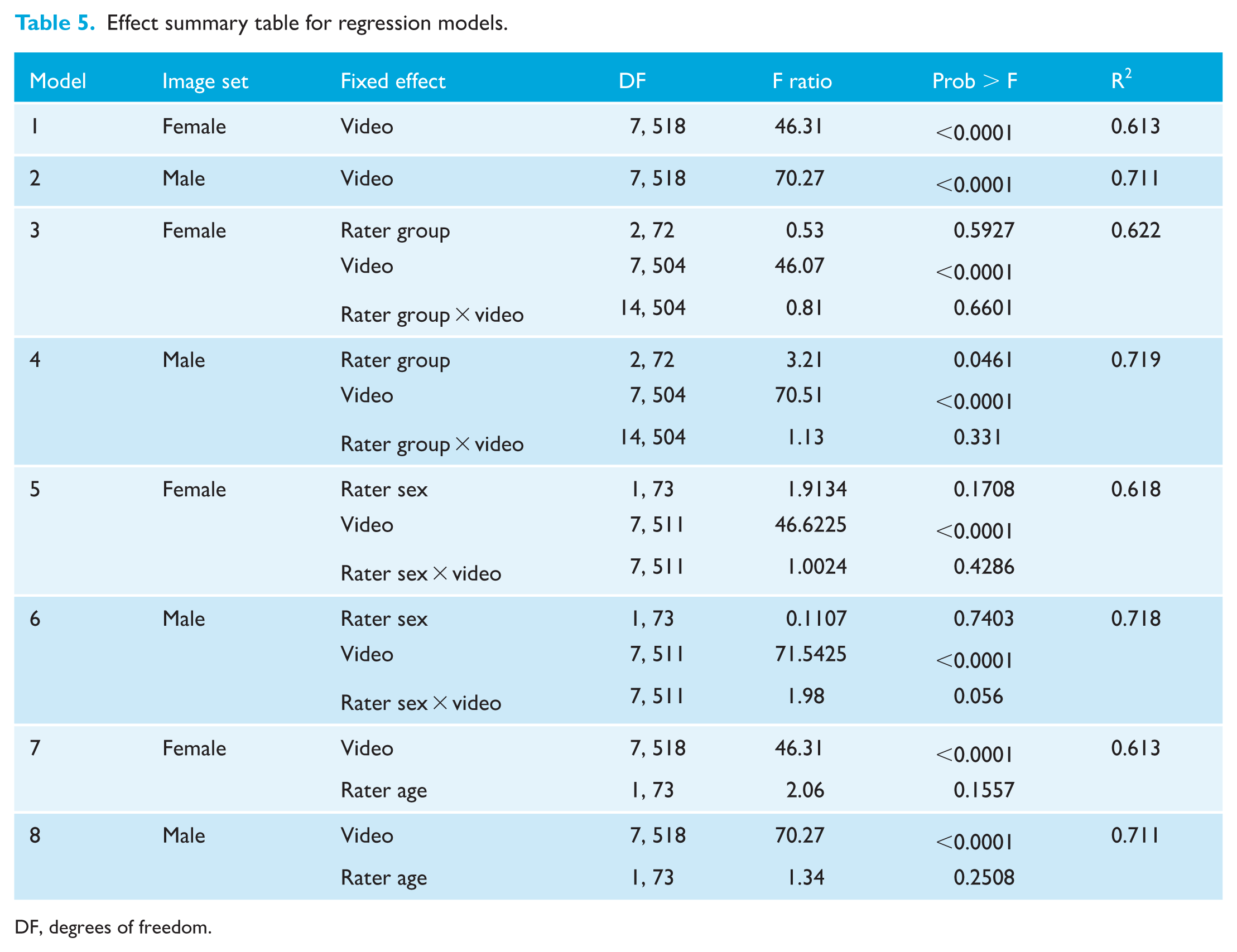
DF, degrees of freedom.
Overall, none of the control variables were found to be significant or add much to the share of variance explained. Video rating was not influenced by rater group (female: P = 0.60; male: P = 0.06), rater sex (female: P = 0.17, male: P = 0.74) or rater age (female: P = 0.16, male: P = 0.25). The effect of different videos was statistically significant in all models also confirming the robustness of the estimation.
Discussion
Summary
The primary aim of this study was to assess the effect of increasing amounts of gingival show on the perception of smile aesthetics. In this study, the ideal range of gingival show for female smiles was 3 mm of incisal coverage to 3 mm of gingival show, with 1.5 mm of incisal coverage being rated as the most aesthetic. Male videos, however, demonstrated a slightly narrower range of 1.5 mm of incisal coverage to 1.5 mm of gingival coverage as the most aesthetic, with the 0 mm of gingival show being most preferred by raters. Significant declines in attractiveness are seen with more than 3 mm of gingival exposure in female smiles and 1.5 mm in male smiles, with smiles being rated as progressively less aesthetic with increasing gingival show. Furthermore, no significant differences between orthodontists, GDPs, and lay people were identified when assessing dynamic smile attractiveness with a small difference of 1.5 mm increments of incisal coverage or gingival exposure.
Comparison with other studies
Geron and Atalia (2005) graded the aesthetic range of gingival exposure up to 1 mm for upper incisors. Hunt et al. (2002) reported that the most aesthetic smile was with 0 mm of gingival exposure, while very little difference was detected when comparing the smile with either 2 mm of incisal coverage or 2 mm of gingival exposure. The finding of more tolerance of gingival show in female smiles in this study may reflect the fact that women tend to have more gingival show compared to men (van der Geld and van Waas, 2003). The ‘form concept’ suggests that the more we are exposed to a certain characteristic, the more we perceive this presentation as correct (Peck and Peck, 1970). It was reported that the relaxed external upper lip length in female smiles was 3.1 mm shorter than in male smiles, resulting in greater incisor display at rest and 2.5 times more prevalence of high smile line in women (Miron et al., 2012), while Drummond and Capelli (2016) found that the further decrease in maxillary incisor display with ageing was more significant for men. There was also a possible tendency of perceiving gingival overexposure among men as feminisation of male physiognomy (Pausch and Katsoulis, 2017), which may explain the finding of low acceptance of increased gingival exposure in men in this study.
Interestingly, although more tolerance of gingival show in women was identified, the reduction of the aesthetic score in men with the increase of gingival display was of a more gradual change with less clear cutoff point compared to women. Previous studies have found a large range of acceptable aesthetics. One of the limitations of these studies is the limited range and increments used. To address this, we covered eight increments from 3 mm of incisal coverage to 7.5 mm of gingival show to reflect the true range of patients attending orthodontic clinics. In the current study, a further significant drop of aesthetic score was identified when gingival exposure was more than 6 mm in both men and women, indicating very poor facial aesthetic outcome with excessive gummy smile. The cross-cultural exchanges as the result of globalisation significantly influence individual perception of facial attractiveness (Broer et al., 2014), which can result in adopting and merging beauty standards and perceptions of facial attractiveness of different ethnic background (Pavlovič et al., 2021). This is particularly relevant given the nature of world globalisation and migration, which has contributed to the increased diversity of patient population in our clinical settings, knowing that maxillary excess is more prevalent in certain ethnicities.
Many studies have compared the perceptions of smile aesthetics between dental professionals and lay people. Kokich et al. (1999) found that orthodontists were less tolerant of gingival exposure at smile and considered more than 2 mm to be unesthetic, while GDPs and lay people rated gingival exposure up to 4 mm as acceptable. Similarly, Sarver and Jacobson (2007) found that orthodontists and maxillofacial surgeons tended to be less tolerant of an increase in gingival show whereas lay people only found it to have a negative impact on smile aesthetics in the more extreme cases. In the current study, no significant difference between orthodontists, GDPs and lay people were identified when assessing dynamic smile attractiveness, indicating that lay people were as good as trained professionals in picking up small differences that impact facial aesthetics. The engagement with highly visual social media online has been linked to the development of life aesthetic literacy (LAL), defined as capacity of interpreting and evaluating aesthetic signs (Pan and Lee, 2024). It has been identified that the increasing use of social media and the role of ‘selfie culture’, with its emphasis on visual imagery, fosters a hyper-awareness of minor aesthetic flaws that can be amplified by the front-facing smartphone cameras (Rahman et al., 2024). This may have a profound impact in shaping the general populations understanding and interpretation of factors that influence facial aesthetics and in so doing, provide an explanation for the similarity between professionals and lay people’s assessment of facial attractiveness.
Sarver and Ackerman (2003) have identified the importance of assessing dynamic smile; however, their interpretation of a dynamic smile involved analysing a smile in frontal, oblique and sagittal static dimensions and considering the influence of time. Although a still photograph might be sufficient to capture the height of the smile, a fixed representation of a facial expression failed to provide enough information for the interpretation of that expression (Ekman et al., 1987). It was reported that when a panel consisting of lay people, oral surgeon, orthodontist and prosthodontist subjectively assessed the smiles of 22 individuals simultaneously photographed and videotaped on two separate occasions, they preferred to see the entire range of the smile with videotapes because it gave them significantly more information than the still images (Walder et al., 2013). Using generated videos, this study was able to recreate the complete dynamic process of the smile, providing a realistic perception of smile aesthetics as a whole, thus overcoming some of the deficiencies in previously published research. This enabled the detection of more subtle differences, making it more reflective of real-life scenarios.
A cropped video showing only the mouth, was chosen to avoid any influence from other facial features. Although some studies found no statistical difference between frontal facial pictures and cropped smile pictures (Caramello et al., 2015; Suzuki et al., 2011), Flores-Mir et al. (2004) found that lay people’s awareness of dental aesthetics increased when presented with close-up dental views of the smile compared with a full smiling face. We aimed to reduce potential confounding factors to a minimum by cropping out facial features, such as the eyes, which have been shown to contribute significantly to facial aesthetics. Furthermore, the introduction of the dynamic element could produce further confounding factors due to the dynamic movements of features, such as the eyes, which move quite dramatically throughout the smile (Messinger et al., 2012). With numerous confounding factors, it would have been difficult to assess accurately the influence of changes in gingival display alone.
Limitations and implication for research
A limitation of the current study was the use of a white woman and man to construct the videos; as such, the results may not be applicable to other racial backgrounds. Further areas of study could evaluate these parameters among differing populations in terms of race.
Furthermore, change of upper lip morphology is inevitable during the manipulation process to simulate a natural smile, which results in slight difference in the lip morphology at different lip heights mainly due to the change of the lip curvature (Weeden et al., 2001). Although the use of real male and female videos reproduce a more realistic smile, this approach may unintentionally introduce a potential confounding difference in male and female video assessments based on lip morphology. To help mitigate for this, raters were instructed to rate the attractiveness of the smile videos presented on gingival display.
Implications for clinical practice
This study shows that an increase in the amount of gingival exposure played an important part in dynamic smile aesthetics, with clear thresholds influencing perception of both clinicians and patients. This affects us as clinicians in setting treatment objectives and treatment planning. When a patient presents with more than 1.5 mm in gingival show on smiling in men and 3 mm in women, and certainly more than 6 mm of show, we should be thinking of our options to optimise final smile aesthetics depending on the aetiology and severity of the gummy smile, which may include gingivectomy, plastic or orthognathic surgery. Furthermore, natural age-related changes associated with the smile should be taken into consideration when evaluating a patient's gingival display in producing an appropriate amount of gingival/teeth display based on age or, conversely, achieving a more youthful appearance as many patients seek to achieve. A pattern of decreasing change from rest to smile has been recognised, especially evident after the ages of 30–39 years (Desai et al., 2009). This reduction can be more significant in the male population (Drummond and Capelli, 2016; Singh et al., 2013). The emergence of using lip Botox injections to address gummy smiles, with an average reduction in gingival show of approximately 2.5 mm, can be achieved in the short term (Rojo-Sanchis et al., 2023); however, the change to the dynamic characteristics of the smile remains unclear, highlighting the importance of assessing this parameter of smile aesthetics as a dynamic action.
Conclusions
There was a significant difference in the perception of smile aesthetics with varying amounts of gingival show. Although subtle differences did exist between 1.5 mm of incisal coverage and 1.5 mm of gingival exposure, there was a clear threshold of acceptance up to 3 mm of gingival display in women and 1.5 mm of gingival display in men, after which the aesthetics of the smile declined with increasing increments of the gingival display beyond 6 mm rated as very unaesthetic. No significant differences were observed in the perception of smile aesthetics with varying amounts of gingival show between orthodontists, GDPs and lay people.
Footnotes
Acknowledgements
We would like to thank Mr. Ron Horne for providing statistical support.
Author contributions
PS conceived and designed the study; PS and JG wrote the protocol. PS, JG and AJ obtained funding and ethical approval. JG and PS collected the data. XZ and JG analysed the data. XZ, JG and PS interpreted the data. XZ and PS wrote the manuscript draft. All authors edited the manuscript and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was obtained from Queen Mary, Univserity of London (QMUL).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.