
Abstract
Background
The smile is one of the most fundamental facial expressions, used to convey friendship, agreement, and admiration. There are various smile analysis method available.
Objective
The aim of this scoping review to find most reliable smile analysis method. Which smile analysis method is most reliable and accurate while assessing the smile of patients undergoing orthodontic treatment?
Design
An electronic search was executed on PUBMED, Cochrane, SCOPUS, hand search was made on google scholar and references of the articles selected. Keyword used while searching the databases as “((smile analysis) AND methods) AND comparison.”
Results
A preliminary search of databases and grey literature yielded 525 articles. Following the application of the eligibility criteria, 16 articles were included.
Conclusion
With the use of latest technologies and knowledge in literature, a clinician can correctly identify the problem, assess the treatment need and give a satisfactory outcome to the patient.
Introduction
The smile is one of the most fundamental facial expressions, used to convey friendship, agreement, and admiration. When a smile is pleasing and appealing to observers, it benefits not only the person who smiles but also others who see it. An appealing or pleasurable smile obviously increases an individual’s acceptance in society by boosting the first impression in interpersonal connections. 1 The smile is a difficult trait to examine. Because it is not a fixed notion, aesthetic prediction of dynamic facial features after treatment completion can be much more difficult to appraise than any other physical process. However, professionals need reliable measurements and guidelines to fully evaluate the outcome of orthodontic therapy, which frequently begins with aesthetic concerns.
Janzen underlined that the ultimate treatment goal is a well-balanced smile. It must be acknowledged that there is no such thing as a universal “ideal” smile. The dentist must deal with two opposing forces. The first is soft tissue repose and animation, which is measured during the patient’s examination and includes how the lips animate on smile, gingival display, crown length, and other smiling features. The second is the impact of skeletal and soft tissue maturational and ageing characteristics on face change across a patient’s lifespan. Clinical success in smile design is decided by an understanding of the patient’s soft tissue, ‘reatment restrictions, and the extent to which orthodontics or interdisciplinary treatment may satisfy the patient’s and orthodontist’s aesthetic goals. 2 The clinician should prioritize these smiling characteristics in order of relevance in establishing a balanced smile. The final problem list will assist the orthodontist in determining the viability of various treatment options and selecting the best mechanotherapy for optimal smile design. 3 More patients are demanding extremely attractive treatment outcomes in modern dentistry. To increase smile attractiveness, physicians must perform a full facial and dental examination that analyses the smile and face objectively and standardized, addressing the patient’s sources of discontent and worry.
Facial, dentogingival, and dental aesthetics should be the primary criteria for aesthetic examination. Several computer software applications for digital smile design (DSD) have been introduced to clinical practise and research in recent years. They are multi-purpose conceptual tools that help improve diagnostic vision, communication, and treatment predictability by allowing careful study of the patient’s face and oral traits that clinical, photographic, or diagnostic cast-based evaluation techniques may have overlooked. 4 The aim of this scoping review to find most reliable smile analysis method. Research question: Which smile analysis method is most reliable and accurate while assessing the smile of patients undergoing orthodontic treatment?
Materials and Methods
This review was carried out in accordance with the Joana Briggs Institute’s scoping review criteria. 5 No ethical clearance is required for scoping review. The results are reported in accordance with the PRISMA statement extension for scoping reviews. 6
Inclusion Criteria
The articles in this review were chosen based on the participants, concept, and context (PCC) criteria. 5 This study attempts to help clinicians for choosing a smile analysis approach based on its reliability. Thus, the criteria were:
Participants
Individuals undergoing orthodontic treatment or approach orthodontist for the treatment.
Concept
Use of Smile analysis method for diagnosing, assessments and treatment purpose.
Context
Reliability of the smile analysis method.
Type of the Studies
Conference papers, experimental studies, quasi-experimental studies, exploratory research, randomized/non-randomized controlled trials, cross-sectional and qualitative studies would be included.
Search Strategy
An electronic search was executed on PUBMED, Cochrane, SCOPUS, hand search was made on google scholar and references of the articles selected. Keyword used while searching the databases as “((smile analysis) AND methods) AND comparison.” There were no time constraints attached to any database searches having last search till August 2022. Only English-language articles were included.
To discover potentially relevant papers, search results were evaluated based on their titles and abstracts, and duplicates were deleted by first and second reviewer. The papers were then assessed based on their abstracts, and those that were deemed to be relevant to the search topic were evaluated by all the authors using the inclusion criteria, only methods of assessment and comparative studies were included. A third reviewer and consensus-based discussion was used to settle disagreements. Based on the data gathered, responses to the targeted questions were developed, and suggestions were developed through consensus-based discussion.
Results
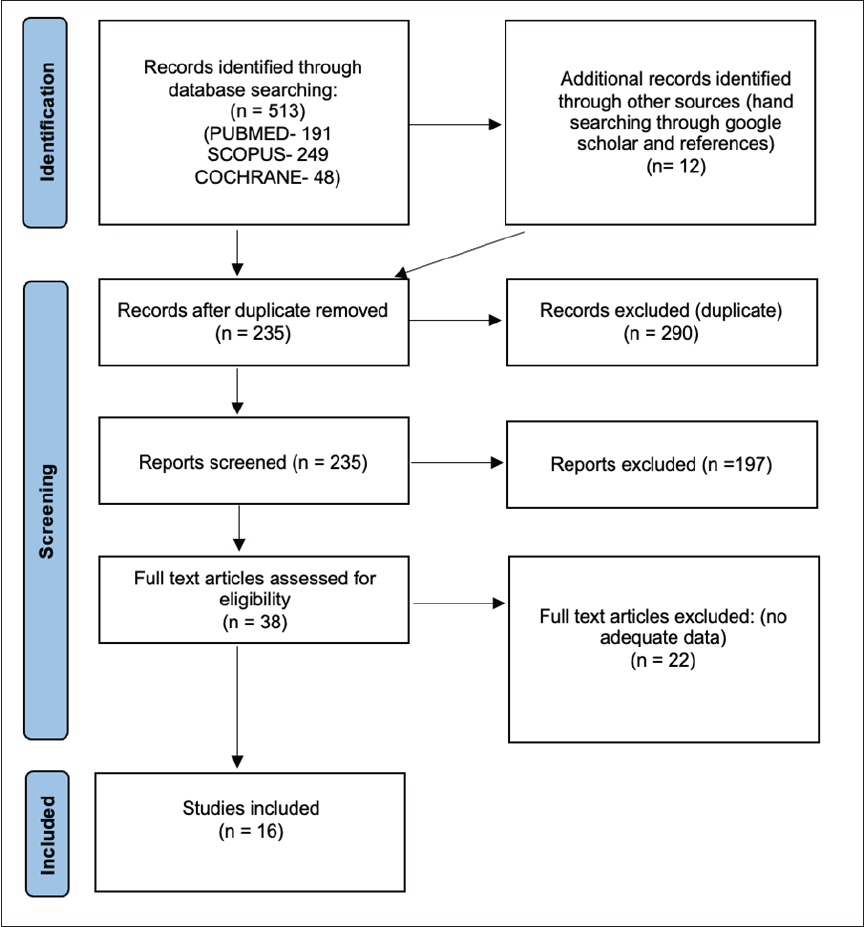
A preliminary search of databases and grey literature yielded 525 articles (513 through databases and 12 hand searched). In the Pubmed database, 191 articles were found using filters, a specific date range, and just English. The titles and abstracts of these were used to screen them. After screening and removing duplicates, 38 articles were read in their entirety. Figure 1 shows the PRISMA workflow diagram, which highlights each stage. Following the application of the eligibility criteria, 16 articles were included.
PRISMA flow diagram.
All studies were conducted at a single location using data from the local population. The most studies were using photographs to analyze smile. The majority of the research was conducted in India, describing every aspect of smile analysis. The characteristics of the studies are described in Table 1 including the level of evidence. 7
Characteristics of the Studies.
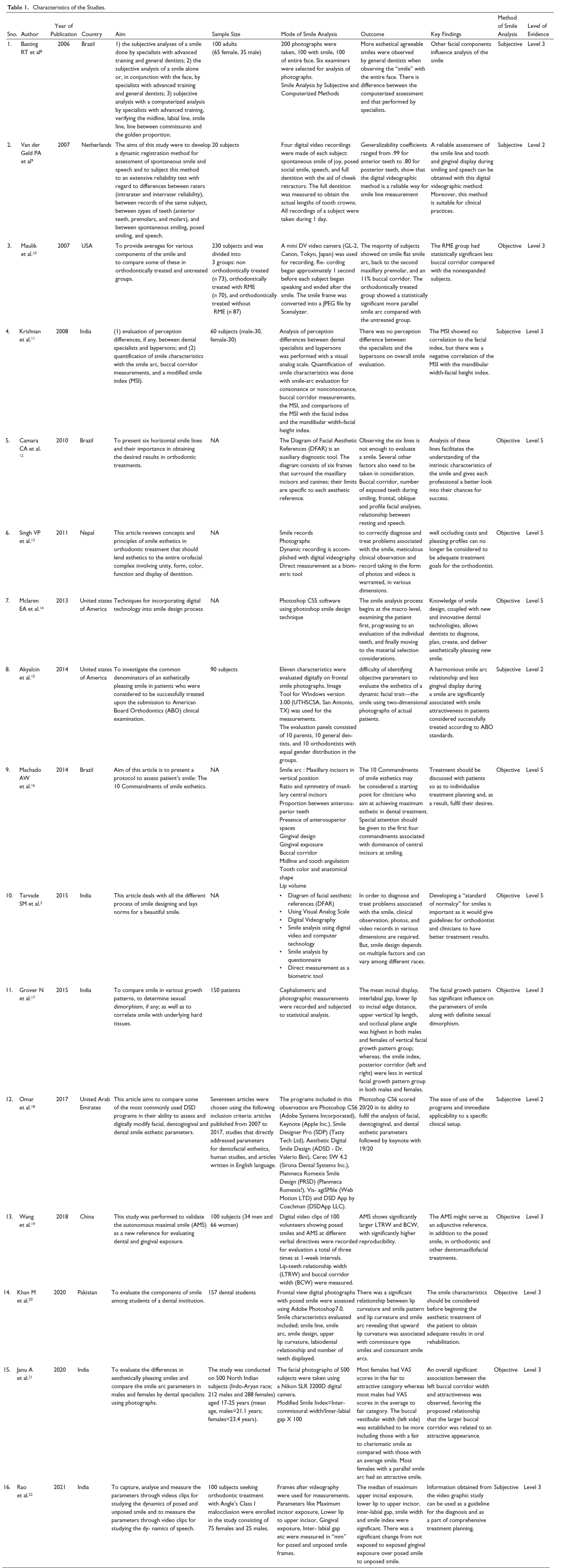
A total of 11 studies has focussed on static records like photograph are Basting et al. 8 , Krishnan et al. 11 , Singh et al. 13 , Mcleran et al. (photoshop CS6), 14 Akyalcin et al. (Image Tool for Windows version 3.00 (UTHSCSA, San Antonio, TX), 15 Machado et al., 16 Tarvade et al., 3 Grover et al., 17 Omar et al (DSD), 18 Janu et al., 21 Khan et al. (Adobe Photoshop7.0). 20 These studies used software to analyze the facial photograph as well as examined by selected specialists or dentist and results are compared showing a significant difference. 8
Six studies, Van der Geld et al., 9 Maulik et al., 10 Singh et al. 13 Tarvade et al., 3 Wang et al., 19 Rao et al. 22 have recorded videos of the patient as a dynamic records. They have recorded the patient while smiling, speaking, forceful smile, etc., each aspect of the facial feature to be analyzed later.
Three studies, Camara et al., 12 Singh et al., 13 Tarvade et al. 3 have done the direct measurement as a biometric tool of resting and dynamic tooth lip relationship, time related changes, philtrum and commissure height, interlabial gap, incisor show at rest and smile, crown height, gingival display, smile arc. But Grover et al. 17 measured cephalograms to understand the effect of hard tissue profile on soft tissue.
Discussion
Clinical success in smile design is decided by an understanding of the patient’s soft tissue, treatment restrictions, and the extent to which orthodontics or interdisciplinary treatment may satisfy the patient’s and orthodontist’s aesthetic aim. Basic knowledge of the aesthetic elements of natural dentition can help to reduce difficulties in the dentist-patient interaction regarding the patient’s smile, aesthetic appearance, and psychosocial integration in a simple yet effective way. Aesthetics, on the other hand, is very subjective. According to Tjan and others, beauty is mostly determined by ethnic and cultural characteristics, as well as individual choice.1, 23 Whereas Cvaillon argues that each dentist has his or her own canons for defining a patient’s aesthetic appearance. 23 There are numerous methods for analyzing smiles, making it difficult to determine which is more reliable. A consistent smile analysis method is required to meet the patient’s expectations.
Carlos Alexandre Câmara gave six frames surround the maxillary incisors and canines in the diagram. The goal of this method was to provide an accurate representation of the positioning and ratios of teeth in the frontal plane, as well as their interaction with the gums and lips. They concluded that observing the six lines is insufficient for evaluating a smile. A number of additional things must also be considered. Buccal corridor, number of exposed teeth while smiling, frontal, oblique, and profile facial assessments, link between resting and speech positions, and the smile are all aspects to consider when diagnosing mouth aesthetics. 12
Akyalcina et al. used a quantitative version of the visual analogue scale to score digital smile images of subjects taken in a standardized manner. Unattractive, average, and attractive smiles were divided into three categories. On the photograph, 11 smile features were digitally assessed. Smile arc (consonant, non-consonant) smile arc discrepancy/smile frame (%), gummy smile (present, not present), gingival display/visible dentition display (%), gingival display (right)/visible dentition display (%), gingival display (left)/visible dentition display (%), visible dentition width/inter-commissure width (%), dentition while smiling/distance from left to right cheilion during smiling visible dentition display/smile frame (%) right buccal space/visible dentition display (%). 15 This study indicates that in any group of participants, even those with the best occlusal relationships, there is individual variability—tooth shape, lip curl, and mouth expression—that influences whether a smile is viewed as aesthetically attractive or not. 24 . These findings also highlight the difficulties in developing objective measures to assess the aesthetics of a dynamic facial trait—the smile—using two-dimensional images of actual patients.
Khan et al. in their cross-sectional study took standardized photographs and analyze smile line or lip line, smile arc, smile design, upper lip curvature, labiodental relationship of the lower lip and maxillary anterior teeth, and number of teeth displayed. They concluded that the existence of an average smile line, consonant smile arcs, a cuspid-type grin, an upward lip curve, and a non-touching relationship between maxillary anterior teeth and lower lip, with teeth exhibited up to first premolars. Limitation of study was that findings can be used into smile analysis of only South Asian folks. 20
Machado et al. introduced 10 Commandments of smile esthetics which were Smile arc: Maxillary incisors in vertical position, ratio and symmetry of maxillary central incisors, proportion between anterosuperior teeth, presence of anterosuperior spaces, gingival design, gingival exposure, buccal corridor, midline and tooth angulation, tooth color and anatomical shape and lip volume. They concluded that the 10 Commandments of smile esthetics are a good place to start for practitioners who want to achieve maximal aesthetic in dental treatment. Special attention should be paid to the first four commands linked with central incisor dominance when smiling. 16
Van der Geld et al. proposed the following smile analysis approach. The dynamic smile was recorded, and the selected video frames were measured using the digora application. The measuring program was calibrated with the filmed reference standard for each record. They concluded that with this digital videographic approach, an accurate assessment of the smile line and tooth and gingival presentation while smiling and speech can be acquired. Furthermore, this approach is appropriate for clinical applications. 9
Rao et al. in their study included 100 patients seeking orthodontic treatment for Angle’s Class I malocclusion. The frames for speech were chosen by the primary investigator, while the suitable frames for posed and unposed smiles were chosen by a panel of five members. After-videography, frames were used for measurements. Maximum incisor exposure, lower lip to upper incisor, gingival exposure, inter-labial gap, and other parameters were measured in “mm” for posed and unposed smile frames. McNemar’s test was used to compare categorical data. p < 0.05 was considered significant. 22
Basting RT et al. selected six examiners chosen (three specialists with advanced training and three general dentists) and used AutoCAD software for computer analysis. Each specialist rated 100 images of smiles as aesthetically pleasing or unappealing. A week later, the same specialists rated photographs to see if they were aesthetically pleasing. This phase tested the impact of various facial features on smile aesthetics. Criteria adopted were midline, labial line, smile line, line between the commissures, golden proportion. Results found to be highly significant The McNemar test showed statistical differences in all factors assessed, with the exception of the midline (p = 0.1951), when the computerized analysis and subjective analysis of the specialists were compared. 8
Omar D et al., in their study analyzed eight digital smile design software and concluded that DSD systems include digital technology into the smile design process and can be utilized as diagnostic tools, treatment plan visualization tools, and communication tools with the patient and technician to improve treatment outcome prediction. However, not all DSD programs on the market today offer the same level of capability for full analysis of dentofacial aesthetic characteristics. Although Photoshop and Keynote were not designed specifically for digital smile design, they define, measure, and adjust the greatest number of dentofacial aesthetic criteria addressed. 18
The clinician can assess the dynamic anterior tooth display and smile analysis of the patient using computer and digital video technology. Esthetic smile design is influenced by a variety of factors and enables clinicians to treat patients using a personalized, interdisciplinary approach. 25 Based on the pioneering research of Kokich et al., 26 some authors turned to digital imaging technologies to find more scientific and consistent references. Since then, the following smile variables have been studied: Smile arc11, 22, 27, 10; buccal corridor10, 11, 19, 22, 28; amount of gingival exposure when smiling asymmetry 22, 28–30; presence of gingival and incisal 22, 22, 31-33 presence of anterosuperior diastema 29, 31 presence of midline shift and alterations in axial proclination26, 33 maxillary incisors ratio, size and symmetry.27, 34 Our scoping review also supports the use of digital video technology, DSD systems with use of 10 commandments of smile esthetics.8-10, 16, 18, 19, 22
With the use of latest technologies and knowledge in literature, a clinician can correctly identify the problem, assess the treatment need and give a satisfactory outcome to the patient. To have a better knowledge of the most reliable smile analysis method, a systematic review and meta-analysis should be performed.
Conclusion
To correctly identify and treat problems related to the smile, rigorous clinical observation and record taking in the form of images and videos in various dimensions is required. Treatment should be discussed with patients in order to personalize treatment plans and, as a result, fulfil their desires. Use of DSD system are more beneficial but not all DSD programs on the market today provide the same level of capabilities for comprehensive dentofacial aesthetic examination. Finally, interdisciplinary treatment, or cooperation, is essential for achieving optimal aesthetic results.
Footnotes
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not applicable
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Not applicable