
Abstract
Objective:
This study was undertaken to determine contemporary trends in the use of the Twin Block appliance among UK orthodontists, including the wear time currently prescribed. In addition, the study explored if there had been any change in wear time prescribed, considering recent research evidence proposing part-time wear.
Design:
Cross-sectional, online survey.
Participants:
Members of the British Orthodontic Society (BOS).
Methods:
The questionnaire was emailed to all BOS members in November 2021 and hosted on the QualtricsXM platform. The questionnaire was piloted for content validity and tested for reliability.
Results:
A response rate of 19% was attained. Nearly all (n = 244, 99%) participants used the Twin Block, and 90% (n = 218) prescribed full-time wear including/excluding eating. Although the majority (n = 168, 69%) had not made changes to their wear time prescriptions, nearly one-third (n = 75, 31%) had. Those who reported a change in their prescriptions currently prescribe less wear time than before, and commonly quoted ‘research evidence’ as the reason. A wide range in success rates (41%–100%) was reported, with patient compliance as the main reason for treatment discontinuation.
Conclusion:
The Twin Block is a popular functional appliance among orthodontists in the UK, originally designed by Clark to be worn full time to maximise functional forces applied to the dentition. However, this wear regime may place considerable strain on patient compliance. Most participants prescribed full-time Twin Block wear excluding eating. Approximately one-third of orthodontists made changes to their wear time prescriptions during their practising career, and currently instruct less wear time than before.
Keywords
Introduction
Functional appliances are a group of orthodontic appliances aimed at growth modification and work by changing the oral functional environment. They have been shown to affect significant dental and skeletal changes in the growing patient, although the theories underlying their mechanism of action remain a matter of considerable controversy and debate. Of the wide variety of functional appliances available, the Twin Block was found to be the most popular in the UK (Chadwick et al., 1998). The Twin Block was originally designed to be worn for almost 24 hours a day to maximise all functional forces applied to the dentition, including masticatory forces. However, patient compliance can be problematic, with functional difficulties such as eating and speaking (O’Brien et al., 2003), alongside perceived negative effects on social interactions (El-Huni et al., 2019).
Recent studies investigating Twin Block wear protocols would appear to suggest favourable results with part-time wear, which were comparable to that achieved with full-time wear (Parekh et al., 2019; Sarul et al., 2022). Moreover, Parekh et al. (2019) reported poorer patient compliance when full-time wear (22 h) was prescribed and improved patient compliance when part-time wear (12 h) was prescribed. In light of these findings, it was felt that a cross-sectional survey would provide important information regarding contemporary trends in Twin Block wear protocols among UK orthodontists.
Participants and methods
Data were collected using an anonymous, cross-sectional, online survey hosted on QualtricsXM. The software required participants to answer questions in a chronological manner, hence reducing the risk of incomplete responses. In addition, this platform reduced the risk of multiple submissions by the same individual, by using cookies on web browsers.
Population and sampling
The sampling population was determined using the British Orthodontic Society (BOS) membership list (n = 1489) to maximise data collection from the UK orthodontic profession. The BOS Clinical Governance Committee granted support for dissemination of the online survey to all BOS members via the BOS membership e-mailing list. A target response rate of 15%–20% was set as this was felt to be a realistic goal for an online survey within the allocated timeframe. Reference is made to a previous survey study that targeted a similar sampling population using an online survey method (Sandler et al., 2019).
Ethical approval
Ethical approval was granted by the Proportionate University Research Ethics Committee (UREC) at the University of Manchester.
Pilot questionnaire
A pilot questionnaire was designed with input from a small focus group (one orthodontic consultant and two orthodontic registrars), as inspired by previous surveys and information obtained from a literature review.
Validity testing
The validity of the questionnaire was tested by disseminating the pilot questionnaire and participant information sheet (PIS) via email to panel of clinicians (three consultants, three registrars, five specialists) with varying levels of clinical experience and based in a variety of work settings (primary, secondary and tertiary care) across the UK. Feedback was requested regarding the relevance of questions included, language used, length of questionnaire and time taken to complete the questionnaire. The mean time taken to complete the questionnaire was 10 min.
Reliability and readability testing
The reliability of the questionnaire was tested by comparing the responses of orthodontists at two time points (1 month apart). An invitation to participate in the reliability testing process was initially sent to 25 orthodontists who were selected by convenience before the survey launch. However, only 20 orthodontists completed the questionnaire on both occasions and therefore only their responses were analysed. Reliability testing was run alongside data collection when the survey was launched. The orthodontists involved in reliability testing were assigned a unique identifier and were emailed a unique weblink at the two time points. This enabled identity concealment of the test panel while allowing comparison of individual responses between the time points. The Kappa statistic was used to measure test–retest reliability, as the questionnaire collected mainly categorical data. The readability of the questionnaire was assessed with the Flesch–Kincaid test and a score of 64.4 was attained, indicating its suitability for the target audience.
Content of the finalised questionnaire
The final questionnaire (Appendix 1) contained 23 questions (17 single answer questions, five multiple answer questions, one open-ended question) and participants were required to enter free text information if ‘other’ options were selected. The questionnaire was structured into seven sections.
Section 1: Introduction and consent
Section 2: Demographics (five questions)
Section 3: Experience with functional appliances and Twin Block appliance (six questions)
Section 4: Twin Block wear prescription (four questions)
Section 5: Reported Twin Block issues (four questions)
Section 6: Successes and failures with Twin Block (four questions)
Section 7: Researchers’ contact details
Disseminating the questionnaire
The first email invitation was disseminated to all 1489 members on 1 November 2021, which gathered an initial response rate of 14% (n = 208). A reminder email invitation was sent on 1 December 2021, which increased the response rate to 19% (n = 284). The email included a cover email (Appendix 2), PIS (Appendix 3) and an anonymous link to the online survey. The survey remained active between 1 November 2021 and 31 December 2021, and data were exported into an SPSS format from the QualtricsXM platform for analysis. The responses from both complete (n = 232) and incomplete (n = 65) questionnaires were evaluated.
Results
Reliability testing
The Kappa values calculated varied widely (range = −0.235 to 1.0) with a mean of 0.60, suggesting moderate agreement overall (Landis and Koch, 1977). Questions that required single answers tended to have substantial agreement (mean = 0.66), whereas questions that allowed multiple answers had moderate agreement (mean = 0.43).
Demographics
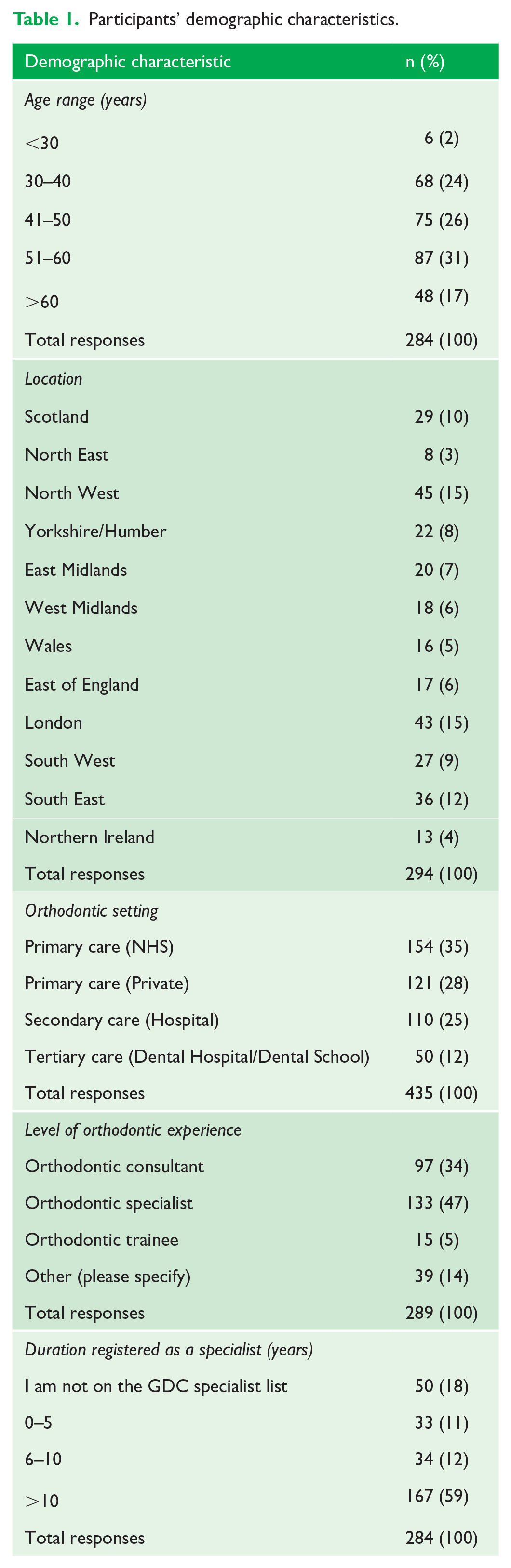
Most participants were aged 30–60 years, with 87 (31%) within the 51–60-year age bracket (Table 1). The majority of responses were from orthodontists who worked in the North West (n = 45, 15%), London (n = 43, 15%) and South East (n = 36, 12%). Most (n = 275, 63%) worked in NHS/private primary care, while 110 (25%) worked in secondary care and the remaining 50 (12%) participants were based in tertiary care. The highest number of participants identified themselves as orthodontic specialists (n = 133, 47%) and consultants (n = 97, 34%). In addition, 39 (14%) participants classified themselves as ‘other’ and were primarily dentists with a special interest in orthodontics (DWSI) (n = 36), clinical assistants (n = 2) and an orthodontic specialist undergoing further training (n = 1). Most participants had been registered on the GDC specialist list for over 10 years (n = 167, 59%).
Participants’ demographic characteristics.
Experience with functional appliances and Twin Blocks
Nearly all (n = 279, 99%) participants reported the use of functional appliances for the correction of Class II malocclusions in growing patients, and the majority (n = 175, 65%) solely used removable functional appliances. A further 72 (26%) participants used a combination of removable and fixed functional appliances. Furthermore, nearly all participants (n = 244, 99%) reported using the Twin Block.
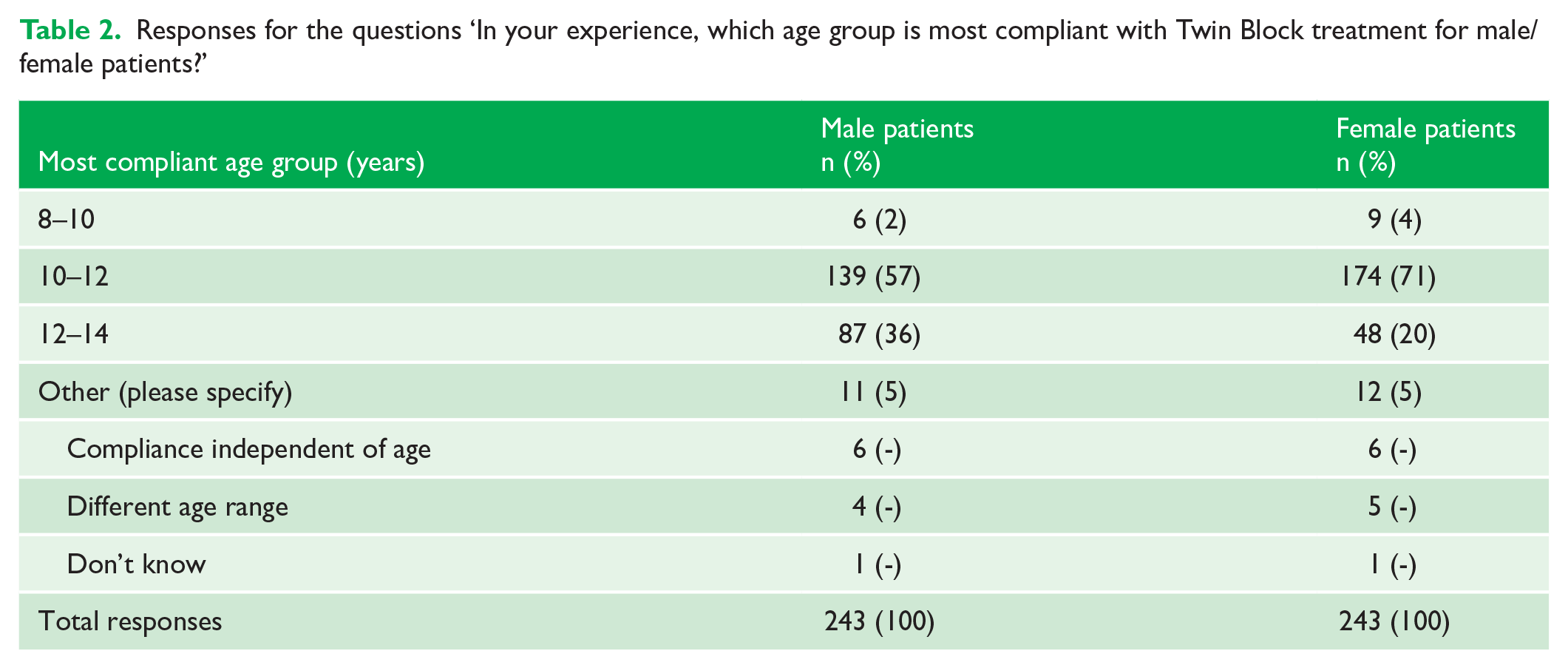
When questioned regarding the influence of age on Twin Block compliance, the majority reported that patients were most compliant at the age of 10–12 years for both sexes (Table 2). Participants who selected ‘other’ provided free-text answers, from which common themes were deduced.
Responses for the questions ‘In your experience, which age group is most compliant with Twin Block treatment for male/female patients?’
Twin Block wear prescription
In terms of Twin Block wear time prescribed, 153 (63%) participants routinely instructed full-time wear, excluding eating, and a further 65 (27%) participants prescribed full-time wear, including eating (Figure 1). Only 10 (4%) participants excluded school hours and eating, and another 10 (4%) prescribed evening and bedtime wear only (12–18 h). None of the participants instructed bedtime wear only. The 5 (2%) participants who selected ‘other’ indicated that their approach was flexible and patient-dependent, as summarised from the free-text responses (Appendix 4).
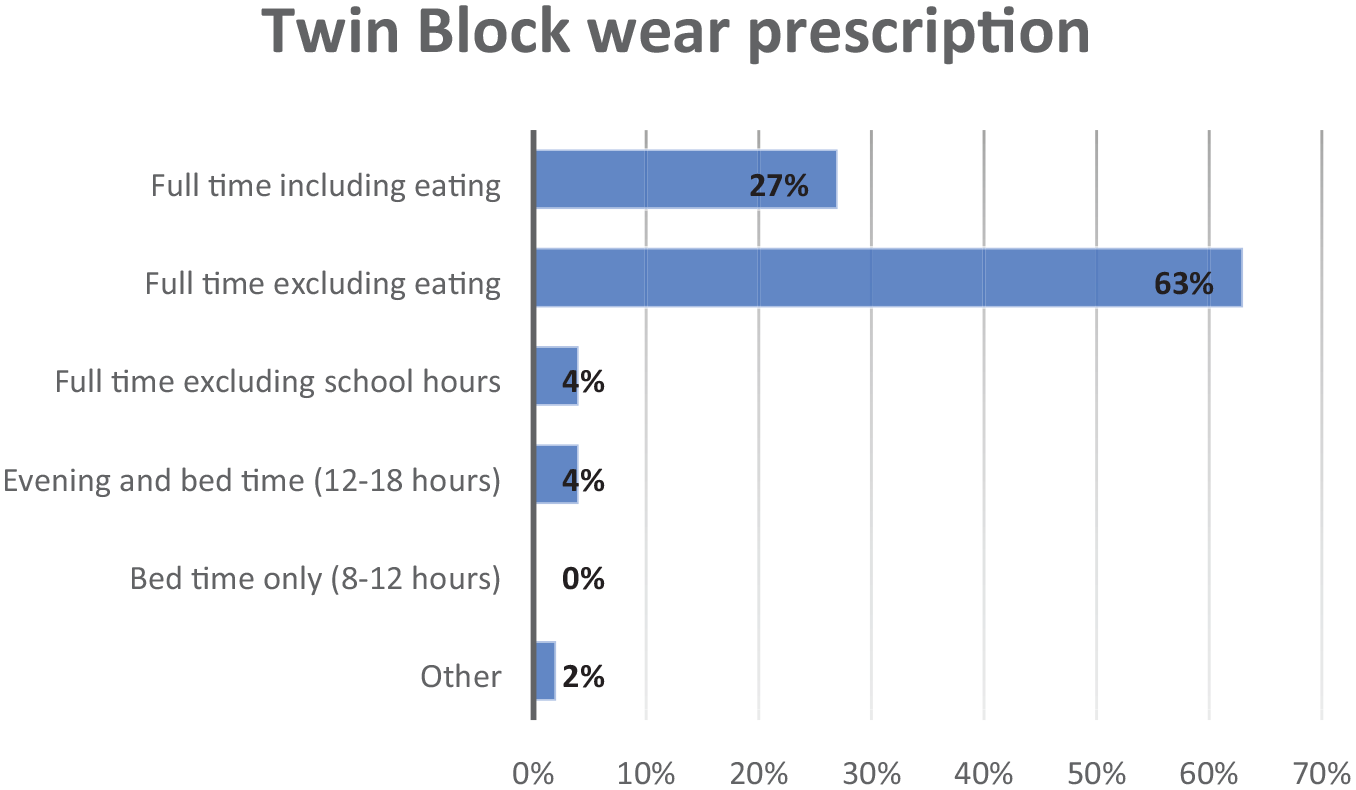
Responses for the question, ‘How long do you routinely instruct your patients to wear the Twin Block during active treatment?’
Participants were asked if the Twin Block wear time they prescribed had changed throughout their practising career. Most participants (n = 168, 69%) did not change their prescriptions, while the remaining 75 (31%) did. Among those who changed their prescriptions, 55 (77%) reported that they prescribe less wear time than previously prescribed. The remaining 16 (22%) participants prescribe more wear time than before (Figure 2).
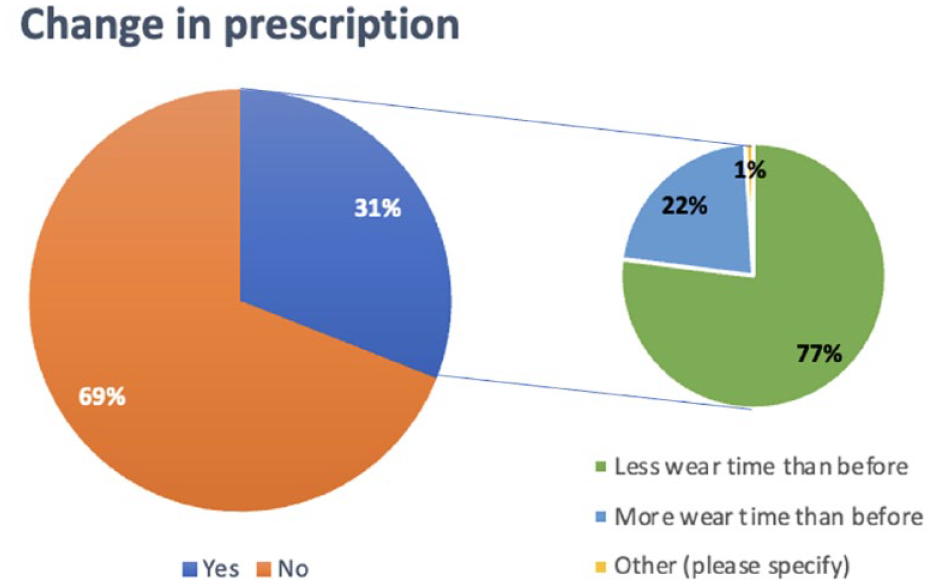
Participants’ reported change in wear time prescription.
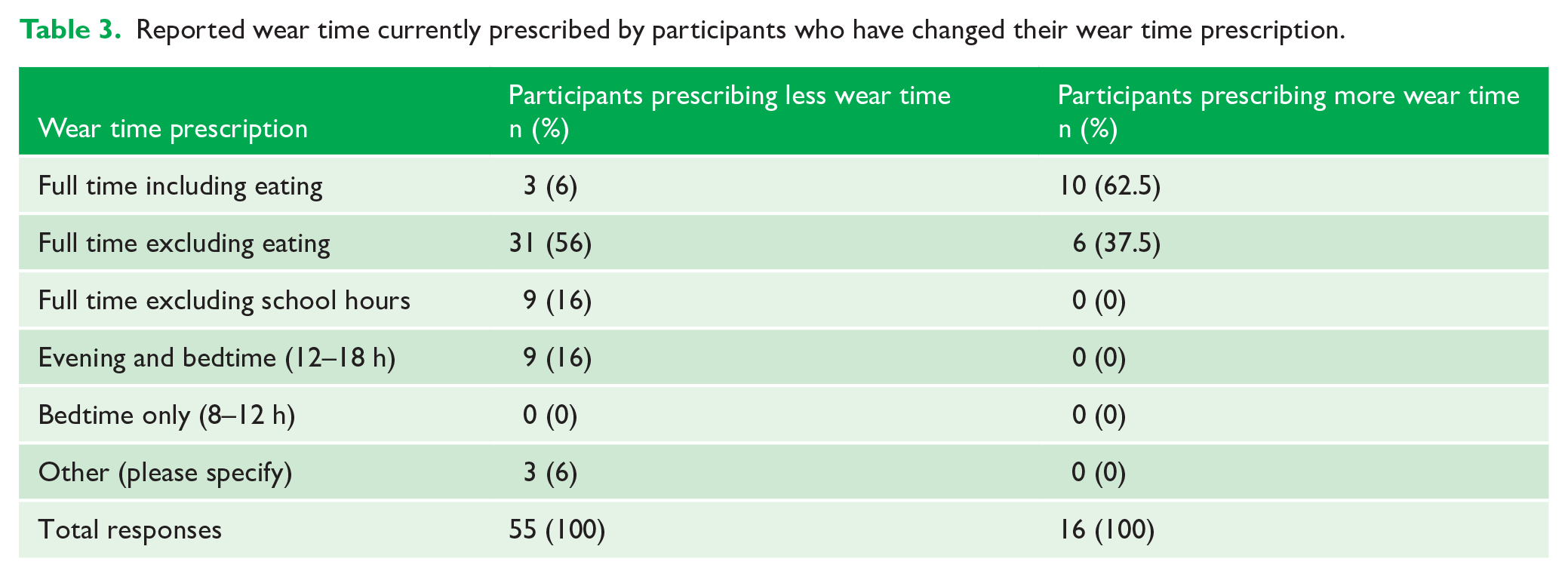
For the subgroup who currently prescribe less wear time (n = 55), the majority (n = 131, 57%) prescribe full-time wear excluding eating, suggesting that full-time wear including eating was previously instructed (Table 3). As for the subgroup who currently prescribe more wear time, 10 (62.5%) participants instruct full-time wear including eating, and the remaining 6 (37.5%) instruct full-time wear excluding eating (Table 3).
Reported wear time currently prescribed by participants who have changed their wear time prescription.
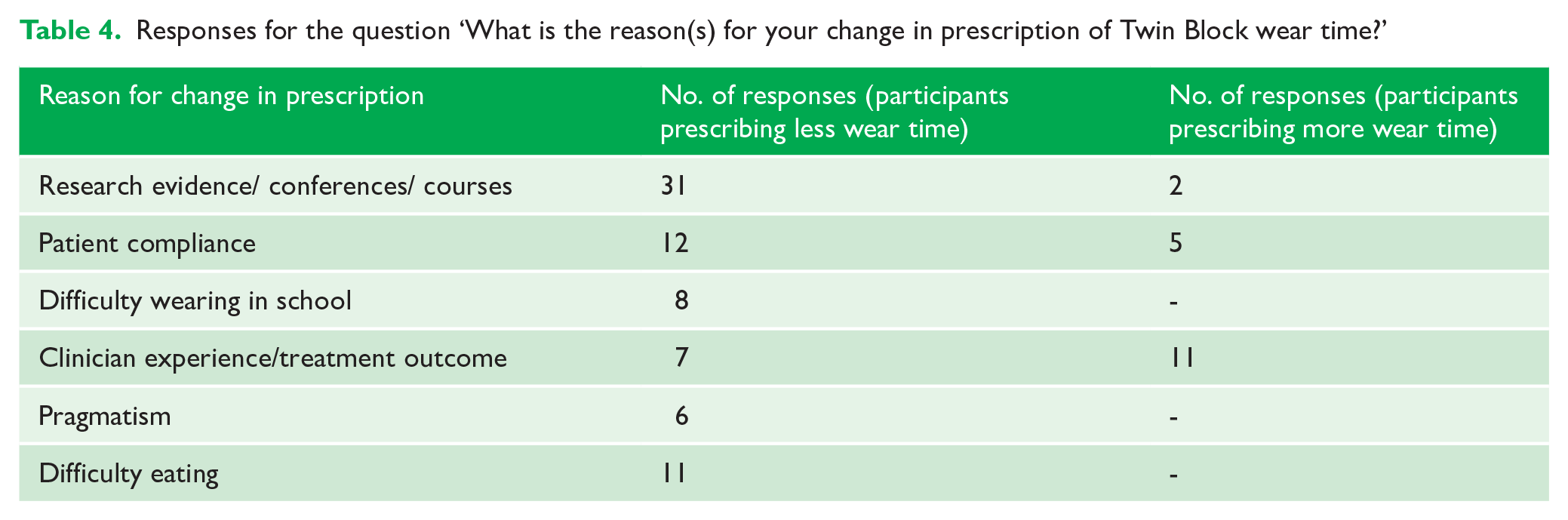
Free-text responses to the open-ended question about reason(s) for a change in wear time prescriptions revealed common themes (Appendix 5). ‘Research evidence’ and ‘conference’ was most quoted by those who currently prescribe less wear time. On the other hand, the responses given by participants who currently prescribe more wear time were most frequently categorised as ‘clinician experience/treatment outcome’ (Table 4).
Responses for the question ‘What is the reason(s) for your change in prescription of Twin Block wear time?’
Reported Twin Block issues
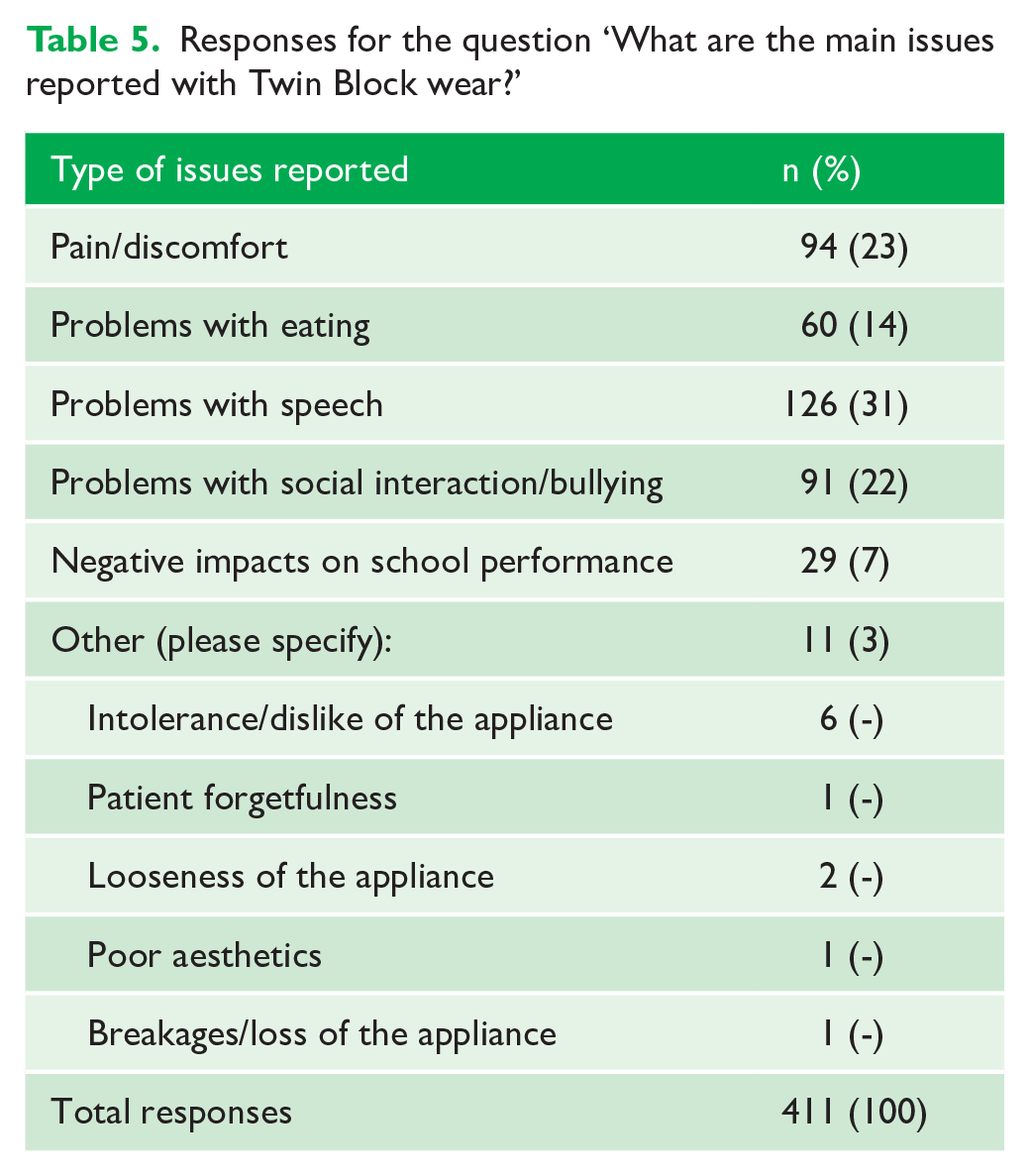
Most participants (n = 154, 64%) identified that patients or parents have reported issues with Twin Block wear. The main issues reported were concerning speech (n = 126, 31%), pain or discomfort (n = 94, 23%) and issues with social interaction or bullying (n = 91, 22%) (Table 5). A further 60 (14%) participants reported problems with eating, and 29 (7%) reported negative impacts on school performance. ‘Other’ issues were reported by 11 (3%) participants, as summarised in Table 5. Furthermore, 196 (82%) participants identified that patients or parents reported issues with Twin Block wear in school.
Responses for the question ‘What are the main issues reported with Twin Block wear?’
Reported success and failures with Twin Blocks
The success rate of Twin Block treatment (in terms of overjet correction) was quoted as 61%–80% for the majority of participants (n = 132, 57%). A further 70 (30%) participants quoted even higher success rates of 81%–100% and the remaining 30 (13%) quoted lower success rates of 41%–60%.
Participants who made changes to their Twin Block wear time prescriptions were asked how these changes affected their success rates with Twin Block treatment. For those who prescribe less wear time than before (n = 53), 29 (55%) reported no change in success rates. However, 18 (34%) participants reported an increase in success rates, whereas 1 (2%) reported reduced success rates. Five participants (9%) who selected ‘other’ expressed that the changes were recently implemented and therefore their impact was yet to be determined.
Among participants who prescribe more wear time than before (n = 15), 11 (73%) reported an increase in success rates and the remaining 4 (27%) reported no change in success rates.
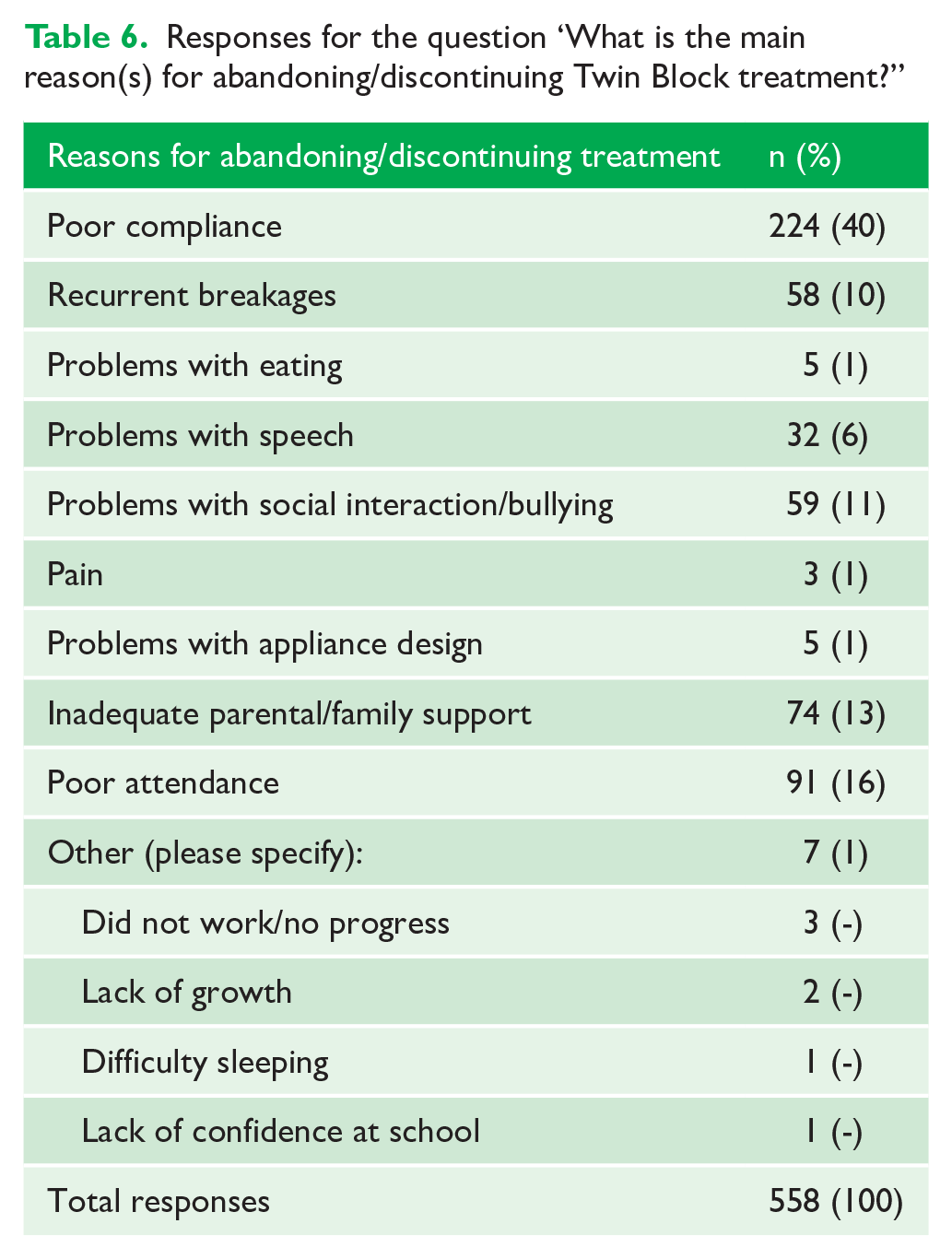
When participants were asked about their reasons for abandoning or discontinuing the Twin Block treatment, the main reasons were poor compliance (n = 224, 41%), poor attendance (n = 91, 16%) and inadequate parental or family support (n = 74, 13%) (Table 6). ‘Other’ reasons reported by 7 (1%) participants are described in Table 6.
Responses for the question ‘What is the main reason(s) for abandoning/discontinuing Twin Block treatment?”
Discussion
The demographic similarities between participants in our survey when compared to other UK surveys (Chadwick et al., 1998; Perry et al., 2021; Sandler et al., 2019; Yassir et al., 2019) may allow the assumption that the data collected in this survey represents current UK orthodontic opinion.
In this survey, 99% of participants use functional appliances for the correction of Class II malocclusions. A previous survey by Chadwick et al. (1998) reported that 99% of UK orthodontists used functional appliances to treat Class II division 1 malocclusions. In addition, nearly all participants in Chadwick’s survey used removable functional appliances, with only 1% using the Herbst appliance. While the majority (n = 175, 65%) of participants in our survey solely use removable functional appliances, 96 (35%) currently use fixed functional appliances, indicating a rise in their popularity over recent years. This may be attributed to greater patient compliance with fixed functionals, which has been shown to increase the chances of treatment completion (O’Brien et al., 2003).
The Twin Block is reportedly the most popular appliance in the UK, being used by 75% of UK orthodontists in 1998 (Chadwick et al., 1998), and 99% in recent times as this survey has found. This appliance is also widely used in other countries, being the most common Class II corrector in Australia (Miles, 2013) and frequently used by 90% of Malaysian orthodontists (Bahar et al., 2021). This contrasts with the US experience in which the Forsus appliance was most favoured, being used by 56% of US orthodontists, in comparison to the Twin Block, which was reportedly used by 12% of participants (Keim et al., 2020). The differences observed could reflect similarities or differences in the training background of orthodontists in various regions.
In terms of age for optimum compliance with Twin Block treatment, most participants selected the 10–12-year age group, with the 12–14-year age group also being a popular option for male patients. Our findings coincide with that of Banks et al. (2004), who reported significantly better compliance in patients aged 12.3 years or less. McDougall et al. (2017) suggested that pre-adolescents are thought to be more amenable to treatment as they have a greater tendency to seek the approval of adult role models. Compliance in the adolescent cohort is unpredictable as the patient enters a period of change compounded by social and psychological pressures, and a shift from parental to peer-influenced behaviours is observed. Research involving adolescents has revealed that female patients often score higher than male patients on measures of self-consciousness, being most intense in early to middle adolescence (Rankin et al., 2004). These findings, when taken together with the reported negative impacts of Twin Block treatment on social wellbeing (El-Huni et al., 2019; Kettle et al., 2020; O’Brien et al., 2003), would suggest a narrow opportunity for optimum compliance especially in female patients.
This survey also sought to ascertain participants’ Twin Block wear prescriptions and found that the most common regime among participants was full-time wear excluding eating (n = 153, 63%). Historically, 65% of UK orthodontists instructed full-time wear including eating, and 40% prescribed full-time wear excluding eating (Chadwick et al., 1998). This suggests that UK orthodontists are prescribing less wear time than in the past. As evident in our survey, most (n = 55, 77%) participants who made changes to their wear prescriptions are currently instructing less wear time. The most frequently reported reason for a reduction in wear time was research evidence/conferences (n = 31), with references made to the randomised controlled trial (RCT) by Parekh et al. (2019) and the British Orthodontic Conference (BOC).
The BOC 2021 featured the Chapman Prize 2020 presentation on research investigating full-time (22 h) versus part-time (12 h) wear of Twin Blocks (El-Huni et al., 2019; Parekh et al., 2019), which concluded that both wear protocols were just as effective. It is therefore interesting that our survey results have not demonstrated a greater proportion of orthodontists prescribing part-time wear, considering the quoted reasons for wear time reduction. In fact, 218 (90%) participants in our survey were still instructing full-time wear including/excluding eating, which is similar to the full–time protocol (22 h) in the aforementioned research by Parekh et al. (2019). This observation provides an example of how differences in individual interpretations of research can dictate the manner in which the evidence is applied (Kay and Blinkhorn, 1996; Nordenram and Norberg, 1998). Moreover, the threshold for daily wear time was determined as 8 h in a recent prospective study (Sarul et al., 2022), providing some evidence that a bedtime-only routine (8–12 h) would be effective. Our survey shows that no participants currently prescribe this regime. Nonetheless, the trends observed would suggest a step closer towards the recommendations proposed by contemporary research, considering that the Twin Block was originally recommended for full-time wear including eating (Clark, 1982, 2019).
Participants who prescribe less wear time also observed improved compliance, particularly when patients were not expected to eat with the appliance or wear them at school. This finding is mirrored in previous studies that reported that patients overperformed when shorter wear durations were prescribed and underperformed when longer wear durations were expected (Parekh et al., 2019; Tsomos et al., 2014). Moreover, good outcomes were also reported with reduced wear time, suggesting the possibility of a win–win situation: a less restrictive wear regime without compromising treatment outcomes.
On the contrary, participants who prescribe more wear time reported faster and/or better results. Some participants also increased wear time to address compliance issues, and expressed that patients tend to fall short of the duration prescribed. This phenomenon is well reported in the literature (Al-Moghrabi et al., 2017; Arponen et al., 2020), with the average discrepancy between actual and prescribed daily wear time being 6 h (Al-Moghrabi et al., 2017).
Nearly two-thirds (n = 168) of participants maintained the same Twin Block wear prescriptions throughout their practising career. The reasons for this were not explored in this survey and can only be postulated. Could it be that we, as human beings, are creatures of habit? Research suggests that individuals who have formed habits become less receptive to new information which challenges present behaviour and they are therefore less likely to act upon it (Verplanken and Wood, 2006).
Moreover, conflicting research on wear times may confuse readers. A systematic review concluded that patients’ actual daily wear time of removable appliances was estimated to be 5 h less than prescribed (Al-Moghrabi et al., 2017). These findings were echoed by an RCT that found that patients wore their Twin Blocks 43% less than the prescribed daily wear time of 12 h (Arponen et al., 2020). Therefore, studies reporting a general lack in patient compliance may imply benefits of increasing wear time (Al-Moghrabi et al., 2017; Arponen et al., 2020), which contradict recent evidence on the effectiveness of part-time wear (Parekh et al., 2019; Sarul et al., 2022). The individual interpretation of research findings may therefore influence whether and how an orthodontist decides to change their practice.
Although the Twin Block maintains its popularity in the UK, the problems reported with wear are identical to those previously described (El-Huni et al., 2019; Kettle et al., 2020; Lena et al., 2017; O’Brien et al., 2003). ‘Problems with speech’ (n = 126, 31%) and ‘problems with social interaction/bullying’ (n = 91, 22%) were frequently reported, which was unsurprising considering the importance of speech in socialising. Although pain/discomfort was commonly reported (n = 94, 23%), this was rarely (n = 3, 1%) a reason for treatment discontinuation. This suggests that issues with speech and social interaction are more persistent and less likely overcome, whereas pain/discomfort tends to be a transient. Moreover, most patients/parents (n = 196, 82%) reported issues with wearing the appliance in school. These findings would therefore appear to strengthen the case for a part-time regime outside of social hours if patients are more likely to be successful in wearing the appliance.
Implications for clinical practice
This survey highlights a lack in change of practice in Twin Block wear prescriptions among participants. However, it is appreciated that evidence-based dentistry is not simply the application of evidence as presented in the literature, but involves the integration of clinical expertise and considers patient values (Sackett and Rosenberg, 1996). Therefore, the absence of change does not necessarily reflect individuals who object to change but may highlight the multifactorial and complex nature of the clinical decision-making process (Barry et al., 2000; Kay and Blinkhorn, 1996; Newton, 2000). Clinicians are urged to critically appraise the evidence base as it applies to their unique patient cohorts. Lastly, emphasis is made on the importance of assessing patient outcomes following the implementation of change to ensure high standards of care.
Implications for further research
Further research is required to produce a greater body of high-quality evidence providing more consistent guidance for Twin Block wear prescriptions. Future surveys may also explore how trends in wear prescriptions continue to develop over time. Moreover, this survey did not explore the reasons for a lack of change in practice among participants, and further studies may identify important factors for this.
Strengths and limitations
The validation and reliability testing processes contribute to the strength of this survey and its internal validity. However, the questionnaire could be improved by using clearer language to avoid ambiguity and misinterpretation. For example, Question 7 asks ‘Of all your Class II cases treated with functional appliances, what proportion of these (in %) are treated with fixed and removable functional appliances? It may be assumed that fixed appliances were being referred to, as opposed to fixed functional appliances.
Our response rate is similar to that of previous online surveys that have sampled BOS members (Perry et al., 2021; Sandler et al., 2019). Nonetheless, the overall low response rate predisposes the survey to non-response bias and selection bias, limiting its external validity. Drop-out attrition was also observed, as the number of participants progressively reduced with each question. This is a common risk in online surveys due to respondent fatigue (Hochheimer et al., 2016), and the questionnaire was kept short (Edwards et al., 2009) to reduce this risk. Moreover, the responses obtained are prone to recall bias, with limited information being obtained as a self-administered survey.
Conclusion
The Twin Block remains popular among UK orthodontists. A shift from full-time wear including eating to full-time wear excluding eating was seen, which may reflect orthodontists’ efforts to optimise patient compliance. Although most orthodontists maintain the same Twin Block wear prescriptions, nearly one-third had made changes during their practising career and prescribe less wear time than before. However, despite ‘research evidence’ frequently quoted for this change, orthodontists had not necessarily implemented part-time wear prescriptions as proposed by recent evidence.
Supplemental Material
sj-docx-1-joo-10.1177_14653125231176569 – Supplemental material for Contemporary Twin Block appliance wear protocols: A survey of UK orthodontists
Supplemental material, sj-docx-1-joo-10.1177_14653125231176569 for Contemporary Twin Block appliance wear protocols: A survey of UK orthodontists by Queenie Ong, Hamza Anwar and Ahmed EL-Angbawi in Journal of Orthodontics
Supplemental Material
sj-docx-2-joo-10.1177_14653125231176569 – Supplemental material for Contemporary Twin Block appliance wear protocols: A survey of UK orthodontists
Supplemental material, sj-docx-2-joo-10.1177_14653125231176569 for Contemporary Twin Block appliance wear protocols: A survey of UK orthodontists by Queenie Ong, Hamza Anwar and Ahmed EL-Angbawi in Journal of Orthodontics
Supplemental Material
sj-docx-3-joo-10.1177_14653125231176569 – Supplemental material for Contemporary Twin Block appliance wear protocols: A survey of UK orthodontists
Supplemental material, sj-docx-3-joo-10.1177_14653125231176569 for Contemporary Twin Block appliance wear protocols: A survey of UK orthodontists by Queenie Ong, Hamza Anwar and Ahmed EL-Angbawi in Journal of Orthodontics
Supplemental Material
sj-docx-4-joo-10.1177_14653125231176569 – Supplemental material for Contemporary Twin Block appliance wear protocols: A survey of UK orthodontists
Supplemental material, sj-docx-4-joo-10.1177_14653125231176569 for Contemporary Twin Block appliance wear protocols: A survey of UK orthodontists by Queenie Ong, Hamza Anwar and Ahmed EL-Angbawi in Journal of Orthodontics
Supplemental Material
sj-docx-5-joo-10.1177_14653125231176569 – Supplemental material for Contemporary Twin Block appliance wear protocols: A survey of UK orthodontists
Supplemental material, sj-docx-5-joo-10.1177_14653125231176569 for Contemporary Twin Block appliance wear protocols: A survey of UK orthodontists by Queenie Ong, Hamza Anwar and Ahmed EL-Angbawi in Journal of Orthodontics
Footnotes
Acknowledgements
The authors would like to acknowledge the help of Ann Wright during the distribution of this survey, and the panel of orthodontists involved in the validity and reliability testing of this survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.