
Abstract
Objectives:
To evaluate the treatment outcomes between Twin Block and AdvanSync2® appliances by comparing the skeletal, dentoalveolar, and soft tissue changes.
Materials and Methods:
Radiographic data of 20 patients were retrospectively analyzed. Data were selected from patients in their skeletal growth spurt as evaluated by the cervical vertebral maturation method (CVMI 2, 3, and 4), with class II malocclusion characterized with retrognathic mandible (ANB > 4°, SNB < 77°, FMA = 25 ± 5°, overjet > 5 mm). There were 10 patients in each group that underwent orthodontic correction for class II malocclusion: either using Twin Block or AdvanSync2®. Independent t test and Paired t test and chi-square tests were used for the data analysis. The level of statistical significance was set at P value ≤.05.
Results:
The chronological and skeletal age were similar in both the groups. Records were taken for the functional treatment with mean treatment span of 8 ± 1 month. Changes in SNB (group I = 1.59°, group II = 3.11°) (P < .01), Co-Gn (group I = 2.89 mm, group II = 5.34 mm), and U1-L1° (group I = −1.51°, group II = 2.97°) showed statistically different outcome between the groups, when the pre-post data were studied. Rest of the variables—cranial base, maxillary skeletal, mandibular skeletal, intermaxillary, vertical skeletal, maxillary dentoalveolar, mandibular dentoalveolar, and soft tissue—showed similar outcome (P > .05).
Conclusion:
Both appliances lead to desirable outcomes in the correction of class II malocclusion. AdvanSync2® resulted in inducing more of changes in SNB and effective mandibular length as compared to Twin Block. Overjet and molar relation improved significantly with both the appliances. Both the appliances resulted in similar skeletal, dentoalveolar, and soft tissue changes.
Introduction
Managing a patient with class II malocclusion is a challenge because of the variable skeletal positioning of the jaws—mandibular retrognathism or maxillary prognathism. 1 Class II malocclusions with mandibular retrusions are believed to be more common than maxillary prognathism. The most favorable treatment options for growing patients include using functional appliances which enhance mandibular growth (mandibular advancement) and headgears, that provide extra oral force to restrict further maxillary growth. 2
Removable functional appliances are generally used in patients who are yet to reach their pubertal growth spurt. Among the different removable appliances (Activator, Twin Block, Bionator, Frankel’s appliance), Twin Block, developed by Clark, may be the most common functional device used, because of its high compliance. It acts by promoting mandibular growth, restricting further forward growth of the maxilla and improving skeletal relationships in individuals with mandibular retrusion. 3 In short term, removable functional appliances are effective in improving class II malocclusion. 4
In contrast to removable appliances, which have an “intermittent” mode of action, the fixed ones work “continuously.” Class II correction with a fixed functional appliance is a combination of skeletal and dentoalveolar changes, which include restraining maxillary growth, dubbed as the “headgear effect,” retroclination of maxillary and proclination of mandibular incisors, distalization of upper and mesial movement of lower molars, along with clockwise rotation of the occlusal plane. 5 Herbst (fixed functional) appliance was introduced by Emil Herbst. 6 The disadvantage of Herbst appliance is that the axles and the screws which attach the rod to the lower part stick out into the cheek in the area of lower first bicuspids. Due to the big telescopic design, it becomes difficult to have patient cooperation and maintenance of oral hygiene simultaneously and appliance tends to break off in the lower premolar region. 7
AdvanSync2® appliance is the modification of Herbst appliance, which was developed by Terry and Bill Dischinger in 2008. It consists of crowns cemented to the maxillary and mandibular permanent first molars, which are connected by telescoping rods; hence also known as molar-to-molar appliance. Being significantly smaller, it fits more in the posterior of the mouth. The device allows simultaneous use of conventional edgewise appliances. The telescoping mechanism helps the mandible to take a forward posture upon closure, thereby enhancing mandibular growth. 8 AdvanSync2® has been shown to produce its effects through maxillary skeletal growth restriction and mandibular dentoalveolar changes.
To date, few studies in the literature have evaluated the effects of the AdvanSync2® appliance.9–11 Most studies have compared AdvanSync2® to other fixed appliances. Hence, this study aimed to evaluate and compare the cephalometric skeletal, dentoalveolar, and soft tissue effects of a removable appliance (Twin Block) and a fixed functional appliance (AdvanSync2®) since compliance is a major factor which can be supposed to alter and differentiate the treatment outcomes. The null hypothesis taken for the study was that there would be no significant difference in the skeletal, dentoalveolar, and soft tissue changes with the AdvanSync2® appliance and Twin Block appliance in the treatment of class II malocclusion.
Materials and Methods
The retrospective study was conducted at the Department of Orthodontics, ITS-CDSR Dental College and Hospital, Ghaziabad, Uttar Pradesh, India, with the records belonging to the period of February 2014 to October 2019 for Twin Block and October 2016 to October 2019 for AdvanSync2®. A written approval was obtained from the Institutional Ethical Committee (Approval number: ITSCDSR/IIEC/2018-21/ORTHO/002).
Inclusion criteria for this study included patients treated in the late mixed dentition or early permanent dentition (aged 10-15), patients with class II malocclusion characterized by orthognathic maxilla with retrognathic mandible (ANB > 4°, SNB < 77°, FMA = 25 ± 5°) with overjet of more than 5 mm, and Angle’s class II (half cusp to full cusp) molar relation, during the growth spurt as indicated by the cervical vertebral maturation (CVM) method 12 (CVMI stage 2, 3, and 4), no missing teeth (excluding third molars), minimal crowding, nonextraction treatment protocol cases, pre- and postfunctional patient records available, and identifiable landmarks on all the radiographs. Exclusion criteria included patients who have undergone previous active orthodontic treatment and syndromic or craniofacial anomaly.
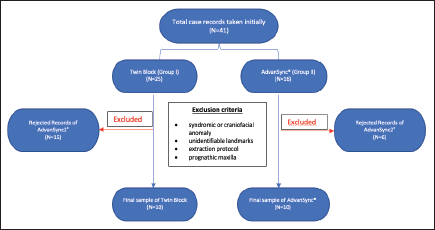
Sample size was calculated by power analysis using G*Power 3.1.9.7 software, with a type 1 error frequency of 0.05 and actual power of the statistical test set at 0.95 for a clinically significant difference for effect size of 1.3, resulting in sample size of 10 for each parameter in each group. After the manual search of the records in the department was done for the time records belonging to the period of February 2014 to October 2019 for Twin Block and October 2016 to October 2019 for AdvanSync2®, 41 radiographic records of the patients (Twin Block = 25 and AdvanSync2® = 16) were initially analyzed, and only records of 10 patients per group, that had undergone class II malocclusion treatment with either a Twin Block or an AdvanSync2® appliance, were selected for the study. Rejections of the records were due to the factors such as unidentifiable landmarks, extraction protocol, and prognathic maxilla in some records along with records which could not be properly digitized. Hence, the study sample consisted of 20 patients grouped into the following: group I: 10 patients of class II malocclusion treated with the Twin Block appliance and group II: 10 patients of class II malocclusion treated with AdvanSync2® appliance (Figure 1).
Flowchart of Data Extraction and Sample Size.
Cephalometric Analysis
The lateral cephalograms represent the treatment groups taken at baseline (T1) and completion of functional therapy (T2) as indicated by the changes in the molar relation (class I or super class I ) and overjet correction. All radiographs for each patient were taken using Carestream Kodak 8000C Digital X-ray system with exposure parameters set at 72 kV, 15 mA, an exposure time of 1.2 s with the magnification error of 8%. For standardization purposes, the magnification was corrected to 0% for all cephalograms.
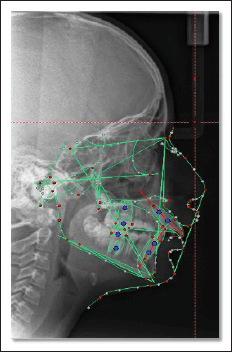
All cephalograms were then imported into commercial software (Dolphin Digital Imaging system version 11.0), where they were digitally traced by 1 investigator using a customized digitization (Figure 2). Thirty-four variables were produced per X-ray and were chosen from different cephalometric analyses to evaluate the skeletal, dentoalveolar, and soft tissue changes with the functional appliance treatment. The cephalometric variables measured for evaluation are given in Table 1.
Dolphin Imaging Software Tracing.
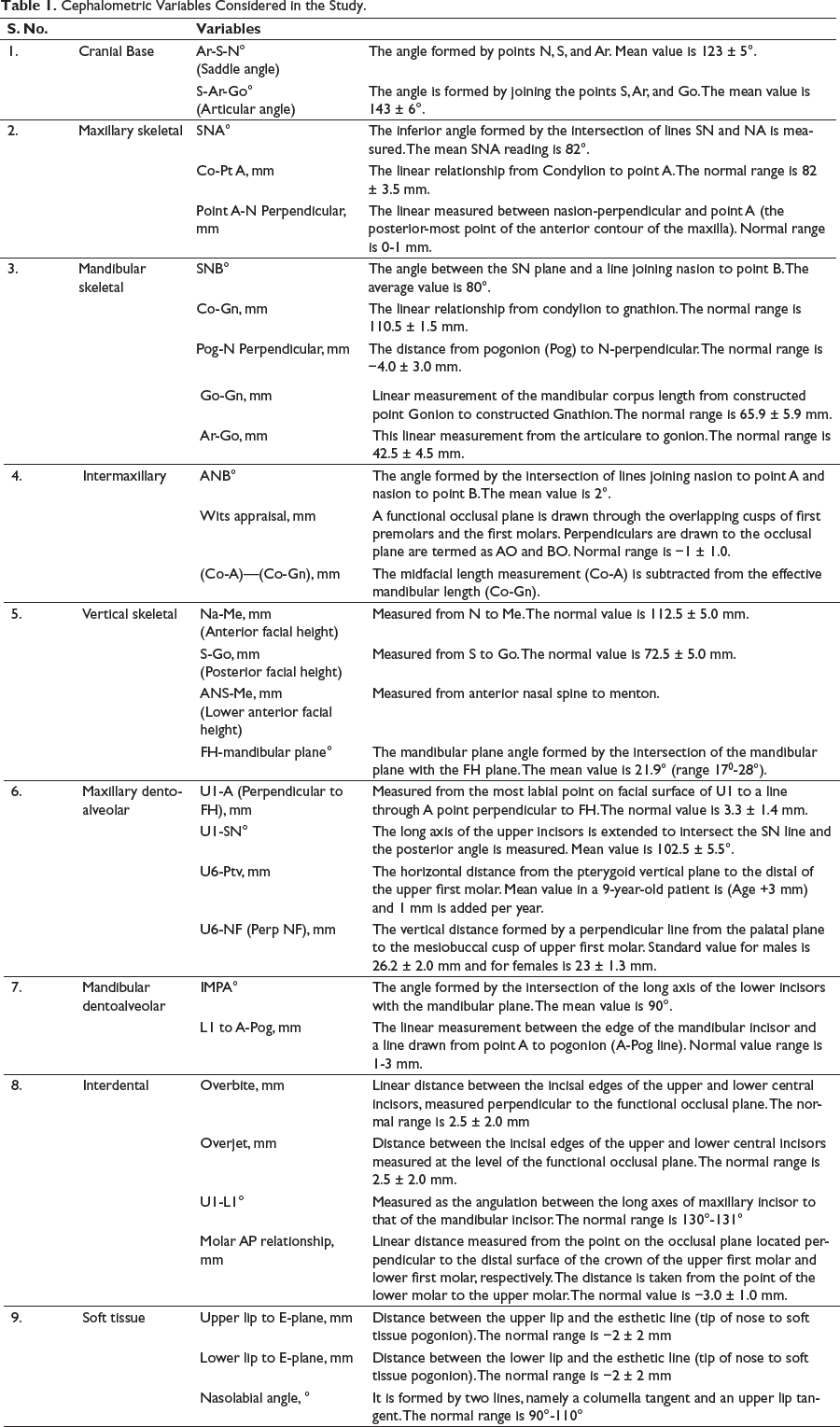
Cephalometric Variables Considered in the Study.
Method Error
To determine accuracy of the method, 10 cephalograms were randomly selected after 21 days and were retraced and their values were remeasured by the same investigator. Intraclass correlation coefficient was done to check reliability. All the measurements showed high reliability (between 0.91 and 0.98) and were all within 0.6 mm/0.6° of the original using Dahlberg’s formula.
Statistical Analysis
Data was analyzed using Statistical Package for Social Sciences (SPSS) version 21, IBM Inc. Descriptive data was reported for each variable. Descriptive statistics such as mean and standard deviation for continuous variables was calculated. Shapiro Wilk test was used to check the normality of the data. As the data was found to be normally distributed, bivariate analyses was performed using Independent t test and Paired t test and chi-square tests. Level of statistical significance was set at P value less than .05.
Results
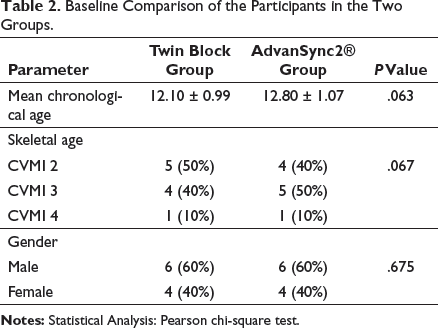
All the records spanned a mean functional treatment span of 8 ± 1 month. The groups were comparable in terms of age, gender, CMVI, and the cephalometric variables (except Ar-Go, Na-Me, and S-Go) on using Pearson chi-square test as shown in Tables 2 and 3, comparing the baseline data.
Baseline Comparison of the Participants in the Two Groups.
Intergroup Comparison for the Pretreatment (Baseline) Cephalometric Variables.
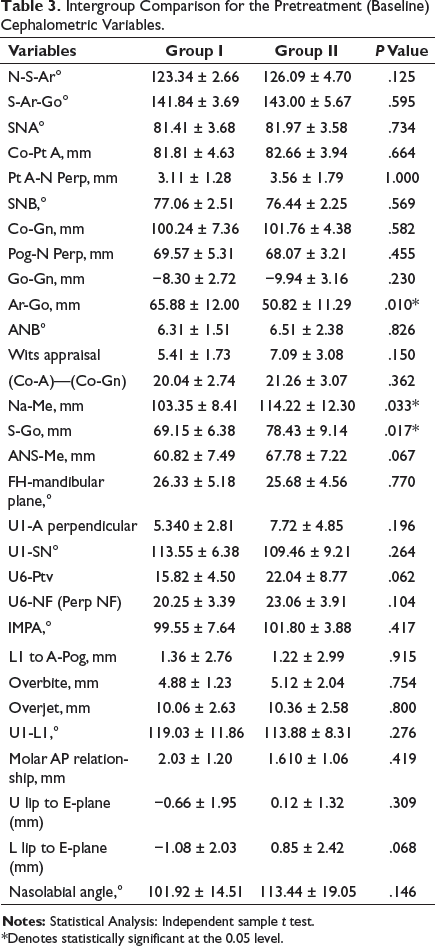
*Denotes statistically significant at the 0.05 level.
Pre-Post Treatment Comparison of the Study Parameters in Group I (Twin Block).
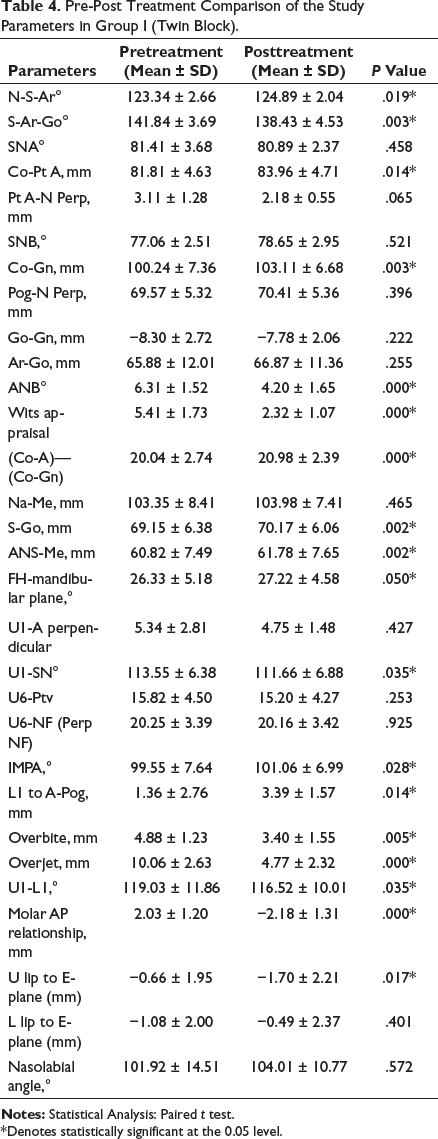
*Denotes statistically significant at the 0.05 level.
Pre-Post Treatment Comparison of the Study Parameters in Group II (AdvanSync2®).
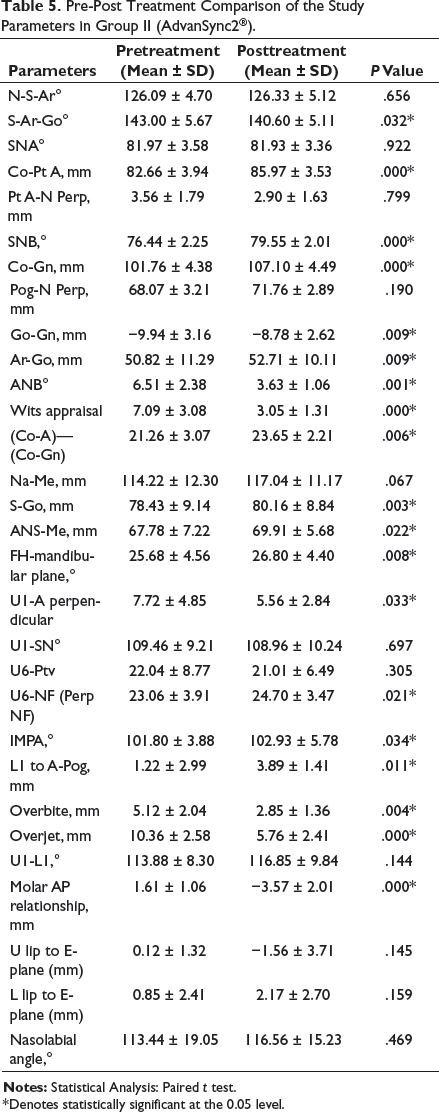
*Denotes statistically significant at the 0.05 level.
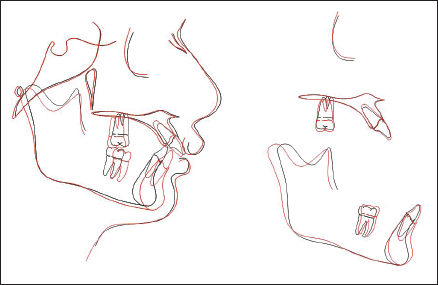
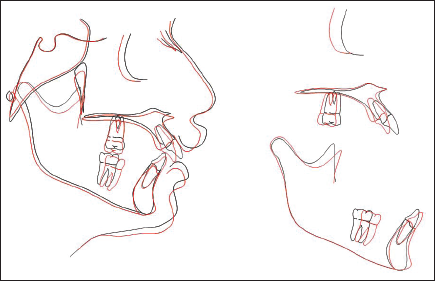
On the intergroup comparison (Table 6) using Independent t test, few variables showed significant difference between the outcomes for Twin Block and AdvanSync2® appliance—U1-L1°, Co-Gn, and SNB0, whereas rest of the variables show comparable changes (Figures 3A, B and 4A and B). Figures 5 and 6 show the typical overall superimposition of a Twin Block (group I) patient and an AdvanSync2® (group II) patient, respectively.
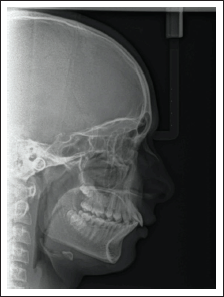
Pretreatment Lateral Cephalogram—Group I (Twin Block).

Posttreatment Lateral Cephalogram—Group I (Twin Block).
Pretreatment Lateral Cephalogram—Group II (AdvanSync2®).

Posttreatment Lateral Cephalogram—Group II (AdvanSync2®).

Superimposition of Twin Block Patient: Black (T1) and Red (T2).
Superimposition of AdvanSync2® Patient: Black (T1) and Red (T2).
Intergroup Comparison of the Mean Difference for the Study Variables.
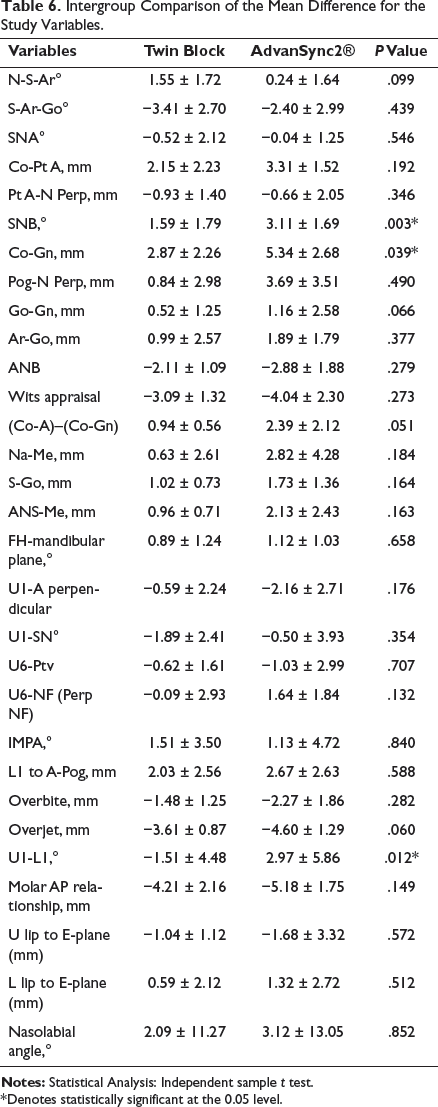
*Denotes statistically significant at the 0.05 level.
Discussion
This retrospective study was designed to compare the skeletal, dentoalveolar, and soft tissue changes with the AdvanSync2® appliance and Twin Block appliance in the treatment of class II malocclusion. Control group could not be selected for this study due to the ethical reasons which precluded the use of concurrent control group whereas historical control couldn’t be accessed for this study. The selected patients (aged 10-15, CVMI stage 2-4) had been treated in the late mixed dentition or early permanent dentition. The mean pretreatment age in group I was 12.10 ± 0.99 years and for group II was 12.8 ± 1.07 years. In group I, 50% of the patients were of CVMI stage 2 and 40% were of CVMI stage 3, and 10% were of CVMI stage 4 whereas in group II, 40% of the patients were of CVMI stage 2, 50% were from CVMI stage 3, and 10% were from CVMI stage 4. Baccetti et al 13 suggest that favorable skeletal manipulations could be expected with use of functional appliances, if the treatment is started just before peak, rather than after the onset of the pubertal growth spurt. Some researchers are of the opinion that, such devices when used in patients during their pubertal growth, show more long-term skeletal effects, compared to prepubertal phase. 14
Cranial Base Variables
Twin Block brought about a significant increase in the saddle angle (+1.55°) and decrease in articular angle (−3.41°). In the AdvanSync2® group too, the articular angle decreased (−2.40°) significantly, suggesting the forward positioning of the mandible with respect to cranial base. Thus, the changes in the cranial base cephalometric variables were found to be similar in both the groups.
Maxillary Skeletal Variables
The Twin Block group showed a significant increase in Co-Pt A (+2.15 mm) whereas SNA (−0.52°) and Pt A-N perpendicular (−0.93 mm) decreased nonsignificantly. The decrease in SNA (−0.52°) could be explained by the distal reciprocal force exerted on the maxilla (headgear effect) by the appliance. The increase in Co-Pt A could be due to the normal growth changes during this period of treatment or may also be due to growth of mandibular condyle in an upward and backward direction that can be stimulated by the functional orthopedic treatment.10, 11, 15 The findings are similar in the AdvanSync2® group also. Schaefer et al 16 also compared the Twin Block and the Herbst appliance and did not find any significant differences between the outcomes.
Studies by Al Jewair et al 10 and Jayachandran et al 9 reported a significant restriction of maxillary growth with the AdvanSync2® appliance. These authors advocate the use of the AdvanSync appliance particularly in class II patients requiring restriction of maxillary growth. In contrast in this study, the restrictive maxillary effect obtained with AdvanSync2® was found to be minimal.
Mandibular Skeletal Variables
In the Twin Block group, a significant increase (2.87 mm) was observed in Co-Gn and SNB (1.59°), whereas changes in other variables (Pog-Nperp [0.84 mm], Go-Gn [0.52 mm], and Ar-Go [0.99 mm]) were found to be nonsignificant. Several other studies evaluating changes with the Twin Block appliance have also reported an increase in effective mandibular length (Co-Gn) 13 . Siara-Olds et al 17 compared the effects between Bionator, Herbst, Twin Block, and MARA. They reported a significant increase in the mandibular length for all the appliances by an average of 3.08 mm, whereas SNB increased significantly in the Twin Block (0.9° per year).
In the AdvanSync2® group, a significant increase was observed in SNB (3.11°), Co-Gn (5.34 mm), Pog-Nperp (3.69 mm), and Ar-Go (1.89 mm) (P < .01). The significant increase of 5.34 mm in effective mandibular length (Co-Gn) is in accordance with the studies by Al Jewair et al, 10 Jayachandran et al, 9 and El Mofty et al. 11 However, in contrast to the present study, they reported minimal or nonsignificant changes in SNB, Pog-Nperp, and Ar-Go.
On intergroup comparison, the changes in SNB (group I = 1.59°; group II = 3.11°) and Co-Gn (group I = 2.87 mm; group II = 5.34) were significantly more with AdvanSync2® as compared to Twin Block, whereas Pog-Nperp, Go-Gn, and Ar-Go showed comparable changes. Hence, in this study, AdvanSync2® resulted in inducing more of changes in SNB and effective mandibular length as compared to Twin Block. Both the appliances resulted in an increase in the mandibular length and changes in SNB which may be due to the mandibular anterior positioning in both appliances. 16 This effective result with AdvanSync2® fixed functional appliance may be attributed due to the effective full-time wear obtained whereas patient compliance may have been compromised with the Twin Block appliance.
Intermaxillary Variables
A significant decrease was observed in ANB (group I = −2.11°, group II = −2.88°) and Wits measurement (group I = −3.09 mm, group II = −4.04 mm), whereas maxillary/mandibular differential (group I = 0.94 mm, group II = 2.39 mm) increased significantly with the Twin Block as well as AdvanSync2® appliances. The decrease in ANB and Wits measurement can be attributed to minimal decrease in SNA and slight increase in SNB. The significant increase in the maxillomandibular differential can be attributed to the greater increase in the effective mandibular length (Co-Gn, 2.87 mm) (due to mandibular growth as well as due to the forward positioning of mandible due to appliance) as compared to the lesser increase in the effective maxillary length (Co-Pt A, 2.15 mm). On the other hand, the effective increase in the mandibular length was brought about by effective telescopic mechanism of AdvanSync2® in placing the mandible forward.
Similar findings were reported by Chibber et al 5 who also found a significant decrease in ANB (−2.7 ± 1.29°) and increase in Co-Gn—Co-A(5.26 ± 2.3 mm). They postulated that the effect could be because of the synergism between pubertal growth and forward positioning of mandible that occurred with the appliance. Al Jewair et al 10 and Jayachandran et al 9 found similar changes with AdvanSync2®. In this study, changes in the intermaxillary cephalometric variables and maxillary/mandibular differential were found to be comparable between Twin Block and AdvanSync2®.
Vertical skeletal Variables
In both the Twin Block and AdvanSync2® group, a significant increase was observed in posterior facial height (S-Go, group I = 1.02 mm, group II = 1.73 mm), lower anterior facial height (ANS-Me, group I = 0.96 mm, group II = 2.13 mm), FH-mandibular plane angle (group I = 0.89°, group II = 1.12°), and anterior facial height (Na-Me, group I = 0.63 mm, group II = 2.82 mm). Hence, the changes brought about in vertical variables were equivalent.
The changes obtained with Twin Block appliance, especially in the posterior facial height and lower anterior facial height, can be attributed to the posterior bite plane effect of the appliance, whereas increase in the mandibular plane angle can be due to the downward and forward growth of the mandible leading to the clockwise rotation of the mandible. 18 Al Jewair et al 10 also found increased values of the vertical skeletal variables (Na-Me = 5.2 ± 4.2 mm, S-Go = 4.7 ± 2.3 mm, ANS-Me = 0.6 ± 1.1 mm, and FH-mandibular plane = 1.0 ± 2.7°) with AdvanSync2® appliance. Contrarily, Jayachandran et al 9 reported decrease in the mandibular plane angle (−0.39 ± 2.56°) with AdvanSync2®.
Maxillary Dentoalveolar Variables
In the Twin Block group, a significant decrease was observed with respect to U1-SN (−1.89°) whereas a nonsignificant decrease was observed with respect to U1-Aperp (−0.59 mm), U6-NF (−0.09 mm), and U6-Ptv (−0.62 mm). Supportive evidence can be found in the study by Burhan et al. 18 This could be due to a posterior reaction resulting from the anterior advancing of the mandible causing retrusion of upper incisors. The bite block effect and selective eruption mechanism associated with Twin Block impedes eruption of upper posterior teeth and allows free eruption of the lower premolar and second molars.19, 20
In the AdvanSync2® group, a significant decrease was seen in U1-Aperp (−2.16 mm) (retrusion of upper incisors) and U6-NF (1.64 mm) (extrusion of upper molars). Al Jewair et al 13 found minimal eruption (U6-NF = 0.1 mm) and distalization (U6-Ptv = −0.5 mm) of maxillary molars and retrusion of maxillary incisors (U1-Aperp, −1.8 mm). Jayachandran et al 9 reported minimal maxillary dentoalveolar effects such as decrease in U1-SN (−1.17°) and increase in U1-Aperp (0.20 mm), U6-NF (1.7 mm), and U6-Ptv (1.8 mm). However, El Mofty et al 11 reported a disparity because they found a significant retroclination of maxillary incisors (U1-SN, −5.3°) but no significant changes in maxillary molar position. The maxillary molar extrusion can be either to the distal tipping of the maxillary molar or the extrusion can be attributed to the natural tendency of the teeth to erupt occlusally and the alveolar remodeling occurring during growth. 5 The distalization of the maxillary molars (U6-Ptv, −1.03 mm) was not found with the AdvanSync2® in this study. This may have been due to the longer arm of the telescopic mechanism of the Herbst which delivers a posteriorly directed force on the maxillary molar whereas the rods of the AdvanSync2® appliance are directed more vertically hence, not resulting in a significant distal force on the maxillary molar.
On intergroup comparison, the changes in the maxillary dentoalveolar cephalometric variables were found to be similar (P > .05).
Mandibular Dentoalveolar Variables
In both the groups, a significant increase was observed with respect to IMPA (group I = 1.51°, group II = 1.13°) and with L1-Apog (group I = 2.03 mm, group II = 2.67 mm). Chibber et al 5 also reported significant increase in IMPA (4.40°) in their study on Twin Blocks. Elfeky et al 21 inferred that the mandibular incisor proclination and labial displacement occurs because of the teeth being part of the anchorage of the Twin Block appliance. Whereas Al Jewair et al 10 reported significant increase in IMPA (5.3°) and L1-Apog (2.6 mm), which they explained was due to the clockwise rotation of the functional occlusal plane with AdvanSync2®. Likewise, outcomes were shown by Jayachandran et al 9 with AdvanSync2®.
On intergroup comparison, the changes in the mandibular dentoalveolar cephalometric variables were found to be similar (P > .05).
Interdental Variables
In the Twin Block group, a significant decrease was observed with respect to U1-L1 (−2.51°), overjet (−5.29 mm), and overbite (−1.48 mm). Molar relation was corrected by 4.21 mm. In accordance with the results of this study, Baccetti et al 13 reported an overjet correction of 4.6 mm mainly by the proclination of mandibular incisors and molar AP correction of 4.7 mm, both by the distal movement of maxillary molar and mesial movement of mandibular molar.
In the AdvanSync2® group, a significant decrease was observed with respect to overbite (−2.27 mm), overjet (−4.60 mm), and molar AP relationship (−5.18 mm) whereas a nonsignificant increase was observed with respect to U1-L1 (2.97°). Al Jewair et al 10 and El Mofty et al 11 also reported significant decrease in overjet and overbite along with molar correction and U1-L1 with AdvanSync2®. In addition, Jayachandran et al 11 reported a decrease in the interincisal angle (−7.44°) with AdvanSync2®.
On intergroup comparison, U1-L1 showed significant difference between Twin Block and AdvanSync2® whereas overjet, overbite, and molar AP relationship were similar (P > .05).
Soft Tissue Variables
Twin Block group showed a significant decrease in upper lip to E-plane (−1.04 mm), and nonsignificant increase in lower lip to E-plane (+0.59 mm) and nasolabial angle (2.09°). A study by Quintao et al 22 reported a significant change in the upper lip inclination and position due to the upper incisor retroclination observed with Twin Block appliance but no significant change in the lower lip variables.
AdvanSync2® group showed a nonsignificant decrease in upper lip to E-plane (−1.68 mm) and increase in lower lip to E-plane (+1.32 mm) and nasolabial angle (3.12°). Jayachandran et al 9 evaluated the soft tissue changes with AdvanSync2® appliance and found nonsignificant changes in the variables upper lip to E-plane and lower lip to E-plane. A study by El Mofty et al 11 reported significant changes in the protrusion of lower lip with the AdvanSync2® appliance, contradictory to the above study. In this study, the results of the soft tissue that change with AdvanSync2® were nonsignificant. On intergroup comparison, changes in the soft tissue cephalometric variables were found to be comparable (P > .05).
Hence, this study concluded that both these appliances lead to similar desirable outcomes in the correction of class II malocclusion. AdvanSync2® showed minimal restrictive effect on the maxilla, an effective increase in mandibular length, minimal distalization, and slight extrusion of the maxillary molars. Overjet and molar relation improved significantly with both the appliances. Soft-tissue changes were found to be alike in both the appliances.
Hence, this study partially accepts the null hypothesis. In consideration with the limitations of the study, the authors recognize that the sample size was limited. Also, a prospective study with large sample size and an equal gender distribution with homogenous growth stages of the participants would have made the study more robust. Future prospective studies with a larger sample size, follow-up till the end of treatment with fixed appliances, and 3D radiographic evaluation are recommended.
Conclusions
Both AdvanSync2® and Twin Block affect the skeletal and dentoalveolar craniofacial complex and are effective in normalizing class II division 1 malocclusion.
Among the skeletal changes, AdvanSync2® showed minimal restrictive effect on the maxilla and a significant elongation of mandible compared to Twin Block.
Both the appliances resulted in similar skeletal, dentoalveolar, and soft tissue changes.
Both appliances giving similar results, clinicians can opt for any of the 2 functional appliances in treatment planning considering other patient factors (eg, compliance) and other treatment factors into consideration.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.