
Abstract
Objective:
To explore university students’ experience of retention and identify potential barriers and facilitators to long-term adherence.
Design:
Cross-sectional qualitative study using virtual focus groups.
Setting:
University of Leeds.
Participants:
Dental and non-dental students from the University of Leeds, who had previously undergone orthodontic treatment and had received removable retainers.
Methods:
Students were invited to participate via email. Virtual focus groups were undertaken using Microsoft Teams. A topic guide was used to explore the experience of orthodontic retention including factors that influence long-term retainer wear. Focus groups were recorded and analysed using an inductive thematic approach.
Results:
In total, 23 students participated in four focus groups, including 13 dental students. The period since the end of orthodontic treatment varied from 9 months to 10 years. Of the 23 participants, 8 (35%) were no longer wearing their retainers. Four themes were identified: (1) experience of orthodontic treatment including knowledge of relapse; (2) experience of retainer wear, including motivators and barriers; (3) role of others; and (4) increasing adherence. Key factors influencing use of retainers were the importance placed on maintaining treatment outcomes, awareness of unwanted tooth movement and understanding of the role of the retainer, access to replacement retainers, and ongoing support to encourage retainer wear. Greater knowledge and dental awareness reported by dental students did not necessarily increase adherence.
Conclusion:
Adherence to removable retainer wear is an important aspect of orthodontic treatment but it is recognised that long-term retainer wear is highly variable. The understanding of relapse and retention is variable. Challenges in gaining access to replacement retainers are a common cause of cessation of retainer wear. Dental professionals are perceived to be important in encouraging and supporting retainer wear and individuals reported they would like more follow-up.
Introduction
It is widely recognised that corrected tooth position after orthodontic treatment is prone to relapse, but it can be difficult to predict the extent and rapidity of occlusal changes. Research suggests nearly all people who have had orthodontic treatment experience some degree of tooth movement, with up to 70% of patients having a need for retreatment 10 years after stopping wearing retainers (Little et al., 1981). As a result of this high level of unwanted tooth movement and its unpredictability, most people are now advised to wear retainers long term (Littlewood et al., 2017). However, adherence to orthodontic retention is known to be variable (Kacer et al., 2010; Kouguchi et al., 1990; Pratt et al., 2011; Schott et al., 2013) and has been seen to decrease over time (Banabilh and Almuqbil, 2019).
Two recent qualitative studies have used interviews to explore young people’s experiences of orthodontic retention in more depth (Al Moghrabi et al., 2019; Frawley et al., 2022). The first study found the perceived importance of maintaining tooth position resulted in good short-term adherence; however, longer-term adherence reduced as inconvenience and pragmatic issues associated with the retainers were experienced, such as retainer loss, breakage, issues with cleaning and forgetting retainers (Al Moghrabi et al., 2019). Facilitators to retainer wear included being shown examples of relapse, support from friends and family, follow-up with the orthodontist and getting into good habits of wearing and maintaining their retainers. The second study found retainers were generally perceived to be easier than active orthodontic appliances and most young people adapted to them easily (Frawley at al., 2022). Factors promoting retainer wear included fear of relapse, not wishing to waste resources through wasted effort if the teeth move and their relationship with the orthodontist.
Various strategies for promoting retainer adherence have been developed and tested. The aforementioned study by Al Moghrabi et al. (2019) was supported by another study that found showing illustrations of relapse was found to improve retainer wear (Lin et al., 2015). The study also found that retainer wear was further increased by involving parents to provide additional support. Monitoring participants by encouraging them to regularly submit photographs of their dentition to a text messaging group, rewarded with points, resulted in improved retainer wear, follow-up attendance and outcomes (Zotti et al., 2019). On the other hand, a trial testing the effectiveness of a mobile application to increase retainer adherence found no change (Zhang et al., 2021). The effectiveness of sensors to monitor retainer wear is conflicting, with one study showing increased retainer wear (Ackerman and Thornton, 2011) while another found no difference (Hyun et al., 2015). A multicentre audit investigating the effectiveness of the British Orthodontic Society ‘Hold That Smile’ campaign, which uses informative videos to educate and motivate patients about retention, found an increase in intention to wear orthodontic retainers (Bharmal et al., 2020). However, the audit did not measure whether an actual change in behaviour occurred.
The aim of the present study was to explore university students’ experience of orthodontic retention to help identify potential facilitators and barriers to retainer adherence in the medium to long term. Both dental and non-dental university students were included to investigate whether higher levels of dental knowledge, awareness and motivation influenced dental students’ behaviour. Examining whether greater knowledge and awareness leads to behaviour change is helpful when considering what type of intervention may be helpful for increasing long-term retainer wear.
Materials and methods
The Standards for Reporting Qualitative Research (O’Brien et al., 2014) and the Consolidated Criteria for Reporting Qualitative Studies (Tong et al., 2007) were followed in the reporting of this study. Ethical approval was granted by the University of Leeds Dental Research Ethics Committee (granted 3 November 2020).
Study design
This was a cross-sectional, qualitative study using focus groups. The underpinning theoretical basis for the research was critical realism, and methods were chosen to explore and interpret participant experience. Focus groups were chosen to encourage interaction and discussion between participants to identify shared and differing experiences (Gill and Baillie, 2018).
Population and setting
Participants were students at the University of Leeds who had received removable retainers after the completion of orthodontic treatment. Current retainer wear was not a requirement for participation to allow the experience of those who had ceased retainer wear to be captured. Participants needed to be sufficiently fluent in English to partake in the discussion as it was not feasible to provide translation services. Focus groups were undertaken virtually using Microsoft Teams.
Research team and reflexivity
The research team members’ characteristics, credentials and role in the research are summarised in Supplemental Table A. All members of the research team were dental professionals who may have pre-existing assumptions and beliefs about orthodontic treatment and retention. The potential scope for the moderators to influence the conversation was managed by use of a topic guide with non-leading questions and prompts. Bias in the interpretation of the data was managed by independent coding of the transcripts and group discussions about coding, interpretation and theme development.
Focus groups were conducted by two final-year dental students (SW and DI). The moderators had no prior experience of qualitative data collection so online training and bespoke training with a qualitative researcher was provided. A pilot focus group with five participants from dental and non-dental backgrounds was undertaken to test the virtual platform and the phrasing and order of questions in the topic guide. The video of the pilot focus group was reviewed with a member of the research team with experience of qualitative research (SB) to provide constructive feedback on the moderators’ technique. Data from the practice group were not included in the data analysis. In prior to the subsequent focus group was reviewed by SB to provide further feedback to the moderators.
It was anticipated that as peers of the participants, honesty and freedom of expression would be encouraged in the discussion through shared experiences and a reduction of the self-censorship, which can result when there is an age or power imbalance between moderator and participants (Djohari and Higham, 2020). The moderators were familiar with some of the participants in the dental student focus groups, but review of the data did not suggest that this had altered the structure or content of the focus group discussion. Peer-led focus groups may present other challenges, such as creating an ‘echo chamber effect’ and encouraging normative influences where individuals do not wish to raise certain views out of fear of group disapproval (Smithson, 2000). The second moderator’s role was to identify when dominating voices may be overly influencing the conversation and to allow other, potentially differing, opinions to be discussed. To minimise the risk that some comments were received more favourably than others, the moderators used neutral language when probing further into comments.
Sampling and recruitment
Recruitment was via online posts placed in University of Leeds student groups on Facebook. Facebook was chosen because it is the most extensively used social media platform and is still commonly used among students for information sharing. Recruitment posts explained the study purpose and requirements for participation. All those who expressed an interest were screened to check their eligibility and all eligible volunteers were included in the study. Participants were given a £5 Amazon voucher and a selection of Colgate products to acknowledge their time contribution.
Participants were allocated into focus groups of 4–8 people depending on their availability. Dental and non-dental students were allocated into different groups because it was expected dental students may have knowledge and use terminology that could exclude non-dental students from the discussion.
Data collection
Due to the COVID-19 pandemic, focus groups were undertaken using Microsoft Teams to ensure safe participation. Students routinely used this platform for studies so were familiar with how to use it.
The focus groups lasted a maximum of 60 min and were video recorded. One moderator (DI) asked the questions in the topic guide while the second moderator (SW) took field notes and identified any areas for additional discussion.
A topic guide was developed by the research team and tested in a pilot focus group (Table 1). Questions related to the following areas:
Treatment and retention history
Recall of information and education they received concerning retention
Factors that influenced their adherence, including internal and external motivators
Any suggestions for overcoming barriers and promoting long-term retainer wear
Topic guide.
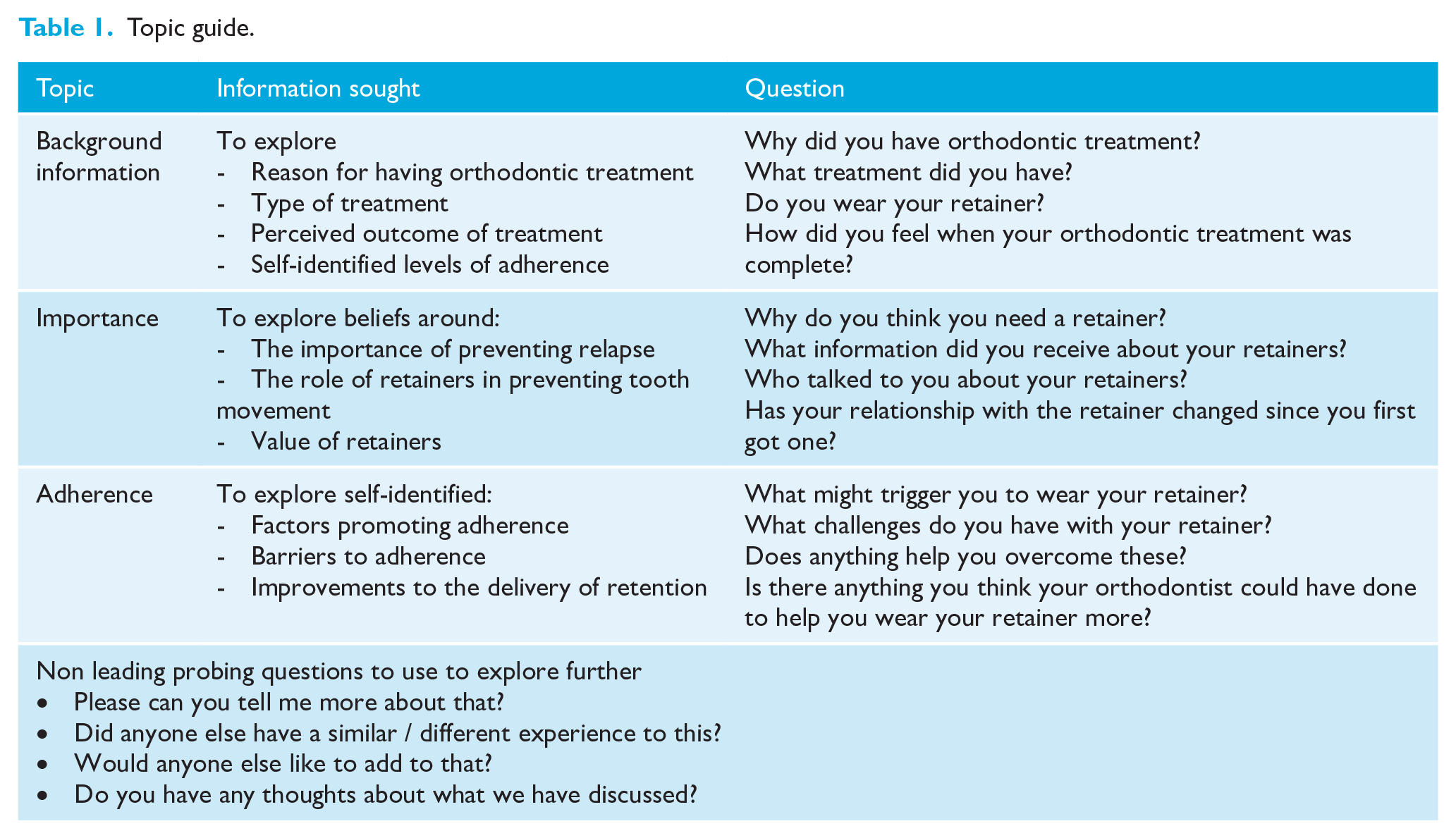
In addition, a set of non-leading probing questions were devised. Transcripts and recordings from each focus group were reviewed to allow iterative revision of the topic guide.
Data management
Video recordings of the focus groups were transcribed using the Microsoft Teams auto-transcription function, then reviewed and edited for accuracy by the moderators. Participants were assigned a unique identifier during the transcription process to allow anonymous data analysis. No participants withdrew from the study.
Data analysis
Qualitative data analysis used an inductive thematic approach to identify emerging themes (Braun and Clarke, 2013). Initial complete coding was performed by SW and DI independently and in duplicate after first familiarising themselves with the transcripts. Codes were assigned to describe the meaning of units of dialogue. Codes were discussed by the research team and revised accordingly to develop the thematic framework. Illustrative quotes were selected to support explanation of themes.
Results
Focus groups were undertaken in November and December 2020. A total of 23 students participated across four focus groups, two dental student groups (n=13) and two non-dental groups (n=10) (Table 2). Eight of the 13 dental students were in the fourth or fifth year so had received orthodontic teaching.
Participant characteristics.
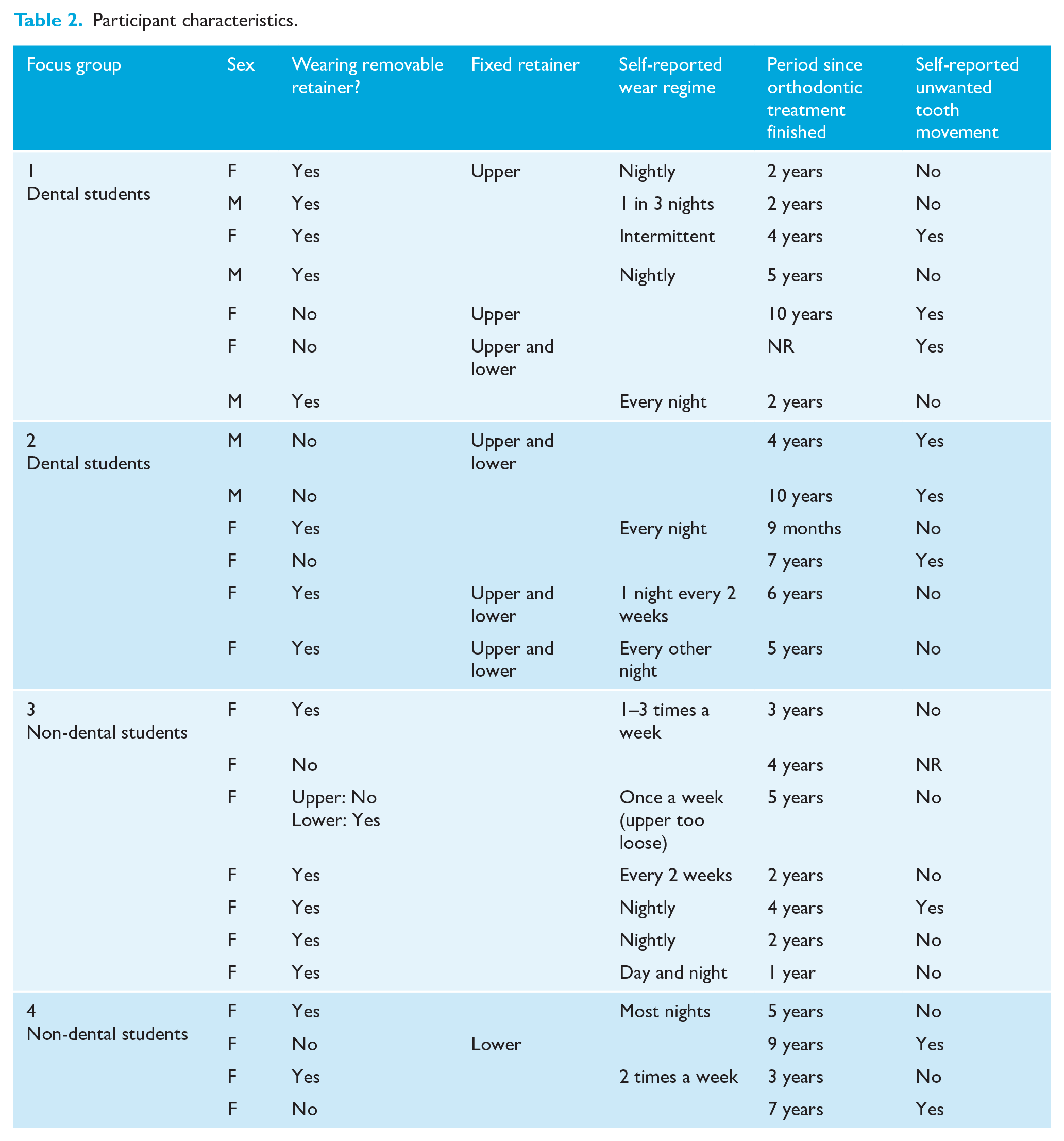
All participants had received vacuum-formed retainers and eight also had fixed retention. The duration since orthodontic treatment finished varied from 9 months to 10 years. In this sample, 8 (35%) participants were no longer wearing their orthodontic retainer. The reasons given for termination of retainer wear were that the retainers no longer fitted (n=3) or were lost (n=2), the participant reported the orthodontist had stopped retention (n=1) or the participant stopped wearing them (n=2).
Four themes were developed:
Experience of orthodontics: experience of orthodontic treatment, understanding of relapse and long-term unwanted tooth movement, attitude to further orthodontic treatment
Experience of retention: understanding and experience of retention, factors promoting retainer wear, barriers to retention
Role of others: role of parents and dental professionals, awareness of other people’s unwanted tooth movement
Increasing adherence: education, habit formation, support
Experience of orthodontic treatment
Participants discussed their experience of orthodontic treatment, their understanding of relapse and unwanted tooth movement, and their attitude towards further orthodontic treatment (Table 3).
Illustrative quotes to explain participants experience of orthodontics.
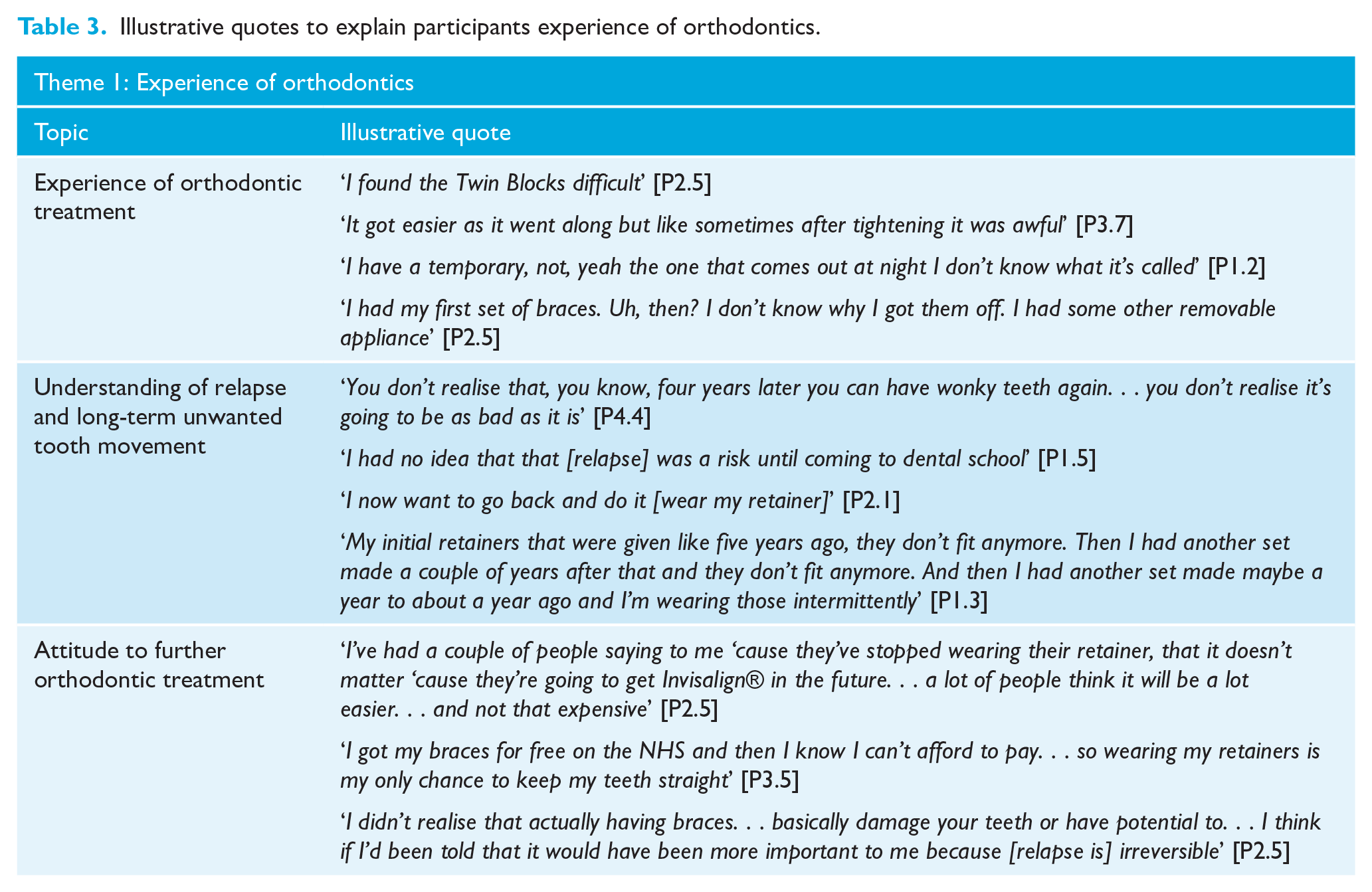
Aspects of orthodontic treatment were often perceived to be burdensome with considerable personal investment of time and labour, but with mostly positive outcomes. There was evidence of misunderstanding about the purpose and process of orthodontic treatment, and while seven of the dental students reported that their undergraduate dental teaching had increased their understanding of orthodontic treatment, there was still evidence of confusion about aspects of their own treatment.
Five participants who had experienced unwanted tooth movement after orthodontics reported that they did not fully understand that teeth could move or appreciate the importance of the retainer in preventing this. Multiple participants expressed regret about the tooth movement; however, some admitted that they did not increase retainer wear even after experiencing tooth movement.
Despite the reported burden of orthodontic treatment, a number of participants reported a willingness to undergo further orthodontic treatment to correct tooth position, though preferably with aligners. This was noted for both people who had and had not experienced tooth movement. In contrast, for other people avoiding retreatment was a motivator for retainer use. One dental student highlighted that they had not appreciated the risks and limitations of repeat treatment until they learnt more about orthodontics during their undergraduate training.
Experience of orthodontic retention
Participants discussed their experience of retention in terms of their understanding about retainers and factors that encouraged or reduced their retainer wear (Table 4).
Illustrative quotes to explain participants experience of retention and factors that promote and reduce wear.
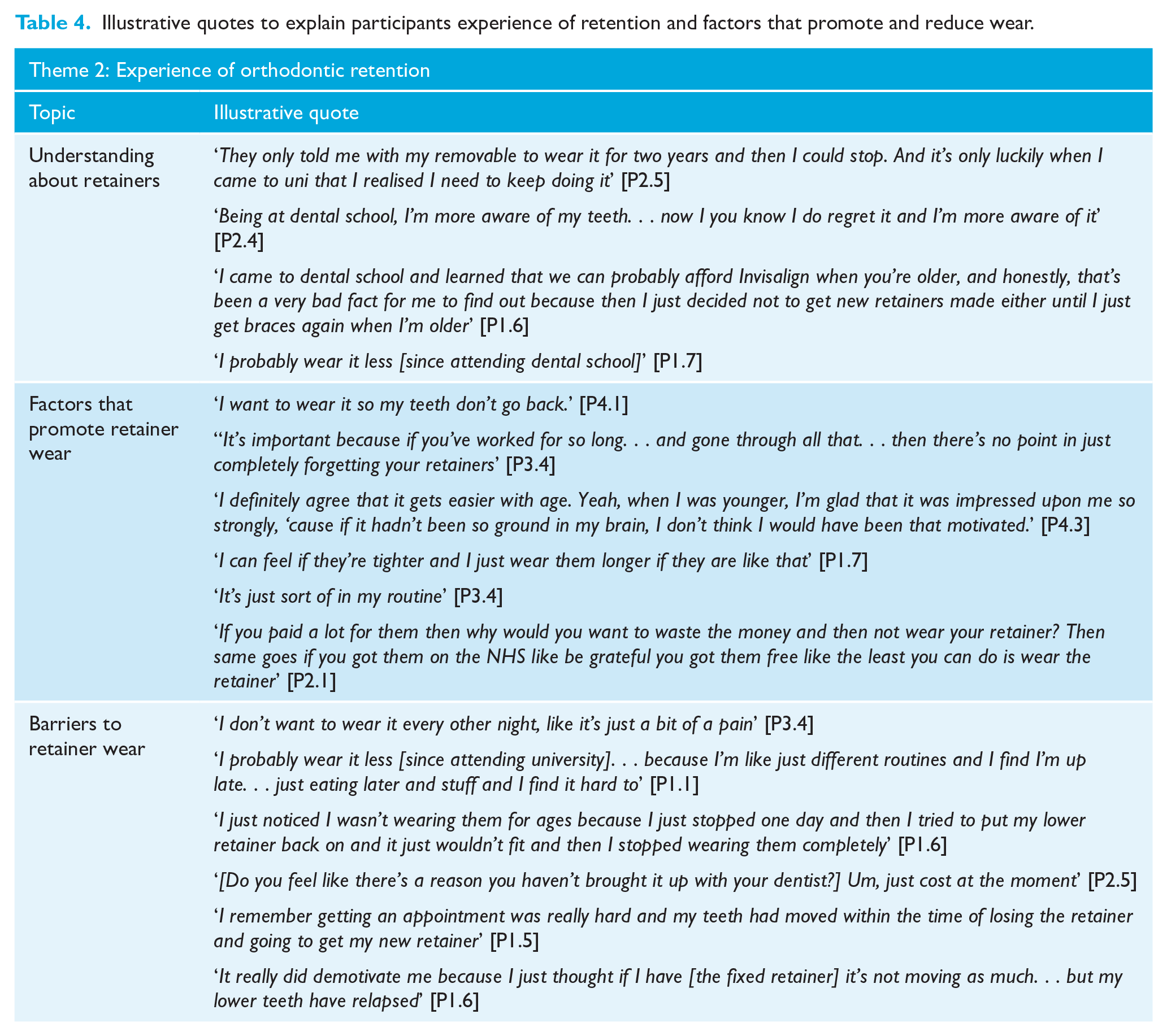
Six of the dental students described how undergraduate teaching had increased their knowledge and awareness of retention in terms of the purpose of retainers, wear regimes and the realities of retreatment. These students felt their knowledge increased the value they placed on the retainer, which often lead to greater retainer wear; however, this was not the case for three of the dental students who admitted that knowing more about retention and relapse had not altered their behaviour.
The main motivator for retainer wear was the high value placed on maintaining the orthodontic treatment outcome. In addition, for some people the perceived challenges during orthodontic treatment increased the importance of retainers. Other factors that were identified as potential motivators were increasing age and understanding of the importance of retention, early signs of tooth movement, such as retainer tightness, and retainer wear becoming a habit. Appreciation for free NHS treatment or significant financial investment may also be motivators.
A number of potential barriers to long-term retainer wear were identified. Retainer wear was considered a burden due to the retainer being uncomfortable, a poor fit or an inconvenience. Participants reported competing priorities such as education or sports, which they prioritised over retainer wear, and challenges from busy and variable routines. Others admitted that they ceased to wear the retainers but could not recall a specific reason.
The majority of participants reported that they had required at least one replacement retainer but there were common barriers to seeking a replacement, such as cost (reported by nine people) and access (reported by six people). One dental participant identified that having a mother who is a dentist provided easy access to get a replacement retainer.
It was commonly believed by participants that fixed retention obviates the individual’s responsibility for retention and fixed retainers were commonly referred to as ‘permanent’. This belief reduced the motivation for wearing removable retainers for some people, and a number of participants without fixed retainers expressed a desire to have them as a result. However, some people with fixed retainers did highlight the issues they experienced with retainer breakage, plaque retention and unwanted tooth movement.
Role of others
Participants described how their adherence to the recommended retention regime was influenced by their parents, peers and dental professionals (Table 5).
Illustrative quotes to explain how participants perceived the role of others.
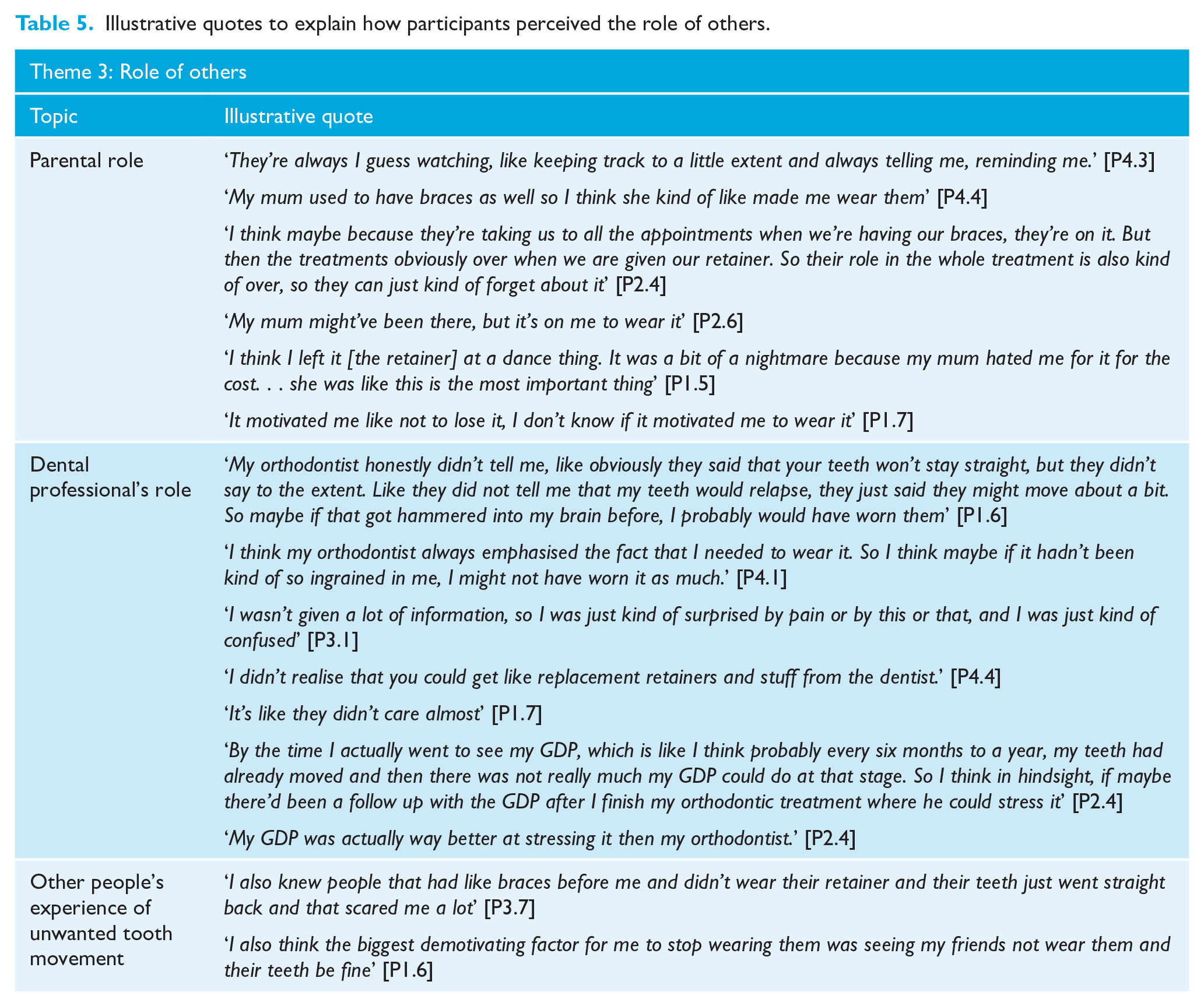
Parents had a role in promoting retainer wear by providing reminders and encouragement. Parental support was perceived as being greater if parents had prior experience of orthodontic treatment or unwanted tooth movement. Some participants described how their parents’ role decreased during the transition from active treatment to the retention phase. Others felt that the responsibility for retention was theirs rather than their parents. The need for replacement retainers often prompted an increase in parental involvement, largely due to the cost, which could lead to a subsequent increase in motivation; however, this sometimes centred around not losing the retainer rather than encouraging wear.
Participants described how their adherence was influenced by the attitude and advice of their orthodontist and general dental practitioner (GDP). The orthodontist’s attitude towards retention was highly influential in both increasing and decreasing wear. Of the 23 participants, 13 reported they felt the education and support they received from the orthodontist was inadequate and left them uninformed about the risk and signs of unwanted tooth movement, the role of retention and replacement retainers.
Frequent recall and reinforcement were seen to be ‘motivational’; however, a number of participants reported no or only one follow-up appointment with the orthodontist, which they felt conveyed a message that the retention phase was unimportant. Two participants felt if the unwanted tooth movement had been identified by a dental professional earlier and some support given, its progress may have been halted. Thirteen participants reported that they had received useful information and support from their GDP.
The role of peers was largely in raising awareness of other people’s experience of unwanted tooth movement. For some, seeing examples was a key motivator for wearing retainers; however, instances where people had not worn their retainers without tooth movement undermined the perceived importance of retainers. No participants described embarrassment or impact on socialising as being an influence on their current retainer use but all but one participant were only wearing retainers at night.
Increasing adherence
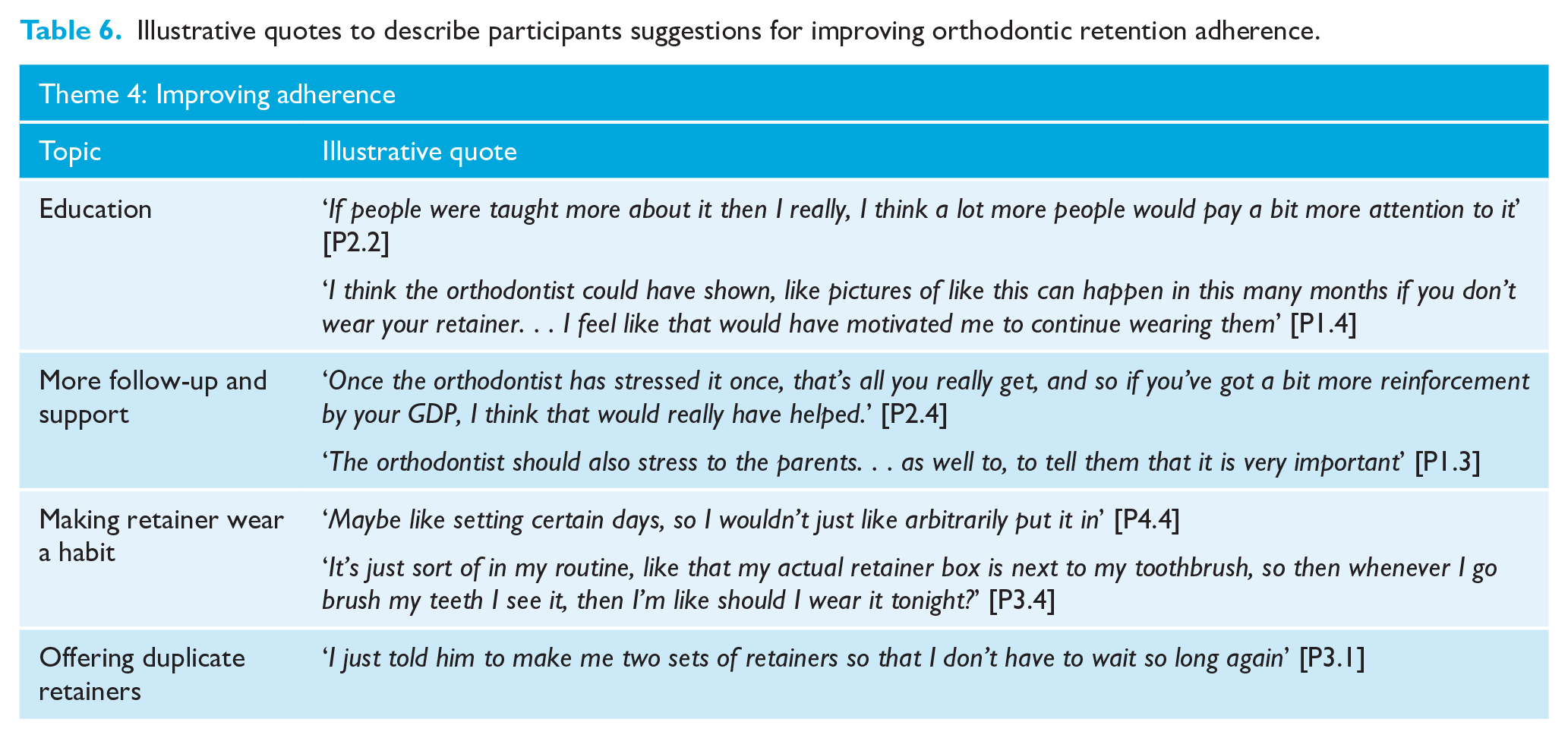
Participants offered suggestions that they felt would have benefited them and helped them wear their retainer more (Table 6). The first was greater education about unwanted tooth movement, the risk of relapse and the benefits of retention. Participants suggested showing photographs to demonstrate unwanted tooth movement and providing written materials to aid recall of verbal instructions. The second suggestion was greater support from the orthodontist and GDP through follow-up appointments aimed at both the individual and parents. Dental professionals were seen to have an important role in emphasising the importance of retainers, promoting behaviour change and identifying relapse early. A third suggestion was to advise and support people to make retainer wear a habit, for example, by keeping the retainer in a visible, accessible place and setting defined days during the week for retainer wear. The remaining suggestions related to overcoming some of the identified barriers in getting replacement retainers. Providing a duplicate set of retainers was valued and seen as a good solution to difficulties experienced in replacing lost or broken retainers.
Illustrative quotes to describe participants suggestions for improving orthodontic retention adherence.
Discussion
The present study explored the medium- to long-term experience of orthodontic retention with a group of young adults, including some dental students. The importance participants placed on maintaining treatment outcomes, along with a good understanding about relapse, longer-term unwanted tooth movement and the role the retainer plays in preventing this were the main motivators for long-term retainer wear. The influence of perceived retainer importance on adherence is supported by previous research (Al Moghrabi et al., 2019).
A number of different reasons were given to explain why participants had ceased to wear their retainers, including the perceived burden of the retainer, being busy and having variable routines with other priorities. A number of participants admitted they could not recall a specific reason and it is possible for these people the teeth were stable or they were willing to accept some tooth movement. The wide range in time since completion of orthodontic treatment (9 months to 10 years) may also be a factor in the variable adherence. Across both groups, those under 1–2 years after treatment were all still wearing their retainers compared to approximately half of those who were >3 years after treatment. The financial investment or gratitude for cost-free treatment may influence attitudes towards retainer wear; no previous research into this area could be identified.
The lack of understanding about orthodontic treatment, subsequent tooth movement and retention, even among dental students, highlights that there is still an important role for further patient education. However, it is also interesting to note that in this sample, some dental students admitted that their increased knowledge and awareness did not necessarily translate into behaviour change. It is recognised that increased awareness and knowledge alone may not translate into behaviour change, because behaviour is complex and multifactorial (Michie et al., 2015). The value of orthodontist-led patient education throughout treatment and visual aids to demonstrate the consequences of poor retainer wear and subsequent relapse has been demonstrated in previous research (Al Moghrabi et al., 2019; Lin et al., 2015; Littlewood et al., 2017). The realities and longevity of retention should be explained before treatment and reinforced throughout to ensure patients are prepared and adequately understand the significance of non-adherence. The expectation that retention will be life-long is an important aspect of the decision-making and informed consent process (Littlewood et al., 2017).
The low level of reported post-treatment follow-up is surprising in this sample; however, it is not possible to verify whether review appointments were offered. The value of follow-up has been reported (Al-Moghrabi et al., 2019; Wouters et al., 2019; Zotti et al., 2019); however, the most beneficial frequency and duration of follow-up has not yet been demonstrated (Wouters et al., 2019). Limited follow-up may be a reflection of the current NHS contract, which specifies supervision of retention for only one year (NHS England, 2019), and potential capacity challenges if specialist orthodontists were to offer longer-term review appointments. GDPs are ideally placed for long-term follow-up because they provide regular care and are recognised as a valuable source of support (Johnston and Littlewood, 2015; Kotecha et al., 2015; Narayanan et al., 2021; Wouters et al., 2019); however, good communication between orthodontists and GDPs is required to facilitate effective GDP-led follow-up.
Parental involvement in promoting retainer wear was shown in our sample and in other studies (Al-Moghrabi et al., 2019; Lin et al., 2015; Mirzakouchaki et al., 2016). Encouraging and educating parents in supporting their child’s adherence may improve wear, particularly for younger people, but it must also be recognised that placing the onus on parents may lead to parent–child conflict, and as young people mature and become independent, parental influence will naturally reduce.
There was variability in the retention regimes and although several participants reported receiving written instructions, not all could not recall if they did. Those who recalled written instructions felt they were a useful reminder. Unlike previous studies (Hichens et al., 2007; Lin et al., 2015; Saleh et al., 2017; Wong and Freer, 2005), in our sample, forgetfulness, difficulty eating and social embarrassment were not cited as reasons for poor adherence. This may be because all participants were wearing clear plastic aligners and for all but one, this was night wear only. This may also reflect that there is increasing normalisation of both orthodontic appliances and retainers. On the other hand, cost and access to replacement services were identified as the main barriers to replacement of retainers. To overcome this issue, provision of duplicate sets was suggested to reduce the urgency of replacing a lost or broken retainer. No studies specifically investigating the experience of replacing retainers were identified but there is clear value in examining how to improve access and disseminating information about avenues for retainer replacement to patients.
It was anticipated that dental students would have greater knowledge and awareness of orthodontic issues and that this may influence their adherence. In our sample, a higher level of dental education appeared to increase awareness and prioritisation of their oral health; however, this did not necessarily translate into better adherence. This challenges the assumption that improved health literacy will increase adherence, as has been demonstrated in other medical therapies (Miller, 2016; Sabatè, 2003). Variable attitudes and understanding shown by dental students towards retention may exist in the GDP population, and if so, this may impact on how GDPs are able to support retention. Evidence suggests GDPs may require further training in the delivery of retention advice (Kotecha et al., 2015; Littlewood, 2017) and repair and replacement of orthodontic retainers.
This research adds to the growing evidence-base about orthodontic retention adherence and challenges. This is clearly an important topic area because relapse or longer-term unwanted tooth movement reduces the net benefit of orthodontic treatment. Steps were taken to ensure data collection and analysis were as rigorous as possible, including training for undergraduate researchers in qualitative research methods and close supervisor support during data collection and analysis. This included focus group debriefs and independent duplicate coding and theme development. The use of Facebook for recruitment may have excluded potential participants who do not use this platform. As with all research, there may have been a self-selection bias in those who chose to volunteer. It was explicitly stated in the recruitment documents that current retainer wear was not required, and this allowed the experience of non-adherence to be captured. Due to COVID-19 social distancing measures, it was not possible to conduct in-person focus groups. Online meetings may have impeded group discussion and limited non-verbal communication, but it may also have improved accessibility and provided a more diverse sample. There is evidence that participants have fewer inhibitions and answer more honestly in virtual focus groups, allowing more accurate portrayals of their experience (Liamputtong, 2011). The retrospective nature of somewhat questions may have allowed for some recall bias, but this is unavoidable when exploring long-term experiences.
Conclusions
The importance placed on maintaining the orthodontic treatment outcome and understanding of retention influence long-term adherence.
Challenges in accessing replacement retainers are a common cause of cessation of retainer wear.
Dental professionals are perceived to be important in encouraging and supporting retainer wear and individuals reported they would like more follow-up.
Suggestions for improving adherence included more education, showing examples of unwanted tooth movement, greater support and providing duplicate retainers to avoid issues with getting replacements quickly.
Supplemental Material
sj-docx-1-joo-10.1177_14653125221134300 – Supplemental material for Orthodontic retention experience of university students: A qualitative study
Supplemental material, sj-docx-1-joo-10.1177_14653125221134300 for Orthodontic retention experience of university students: A qualitative study by Sophie Wilson, David Idicula, Simon J Littlewood and Sophy Barber in Journal of Orthodontics
Footnotes
Acknowledgements
The authors would like to thank all the students who took part in this study. We would also like to thank Colgate for providing gifts for the study participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.