
Abstract
Human-interest narratives are journalistic tools to captivate and engage the audience, influence public opinion and bring revenue to media organizations. This paper analyses how human-interest narratives are used in contemporary health journalism across media systems and health systems. Based on a comparative content analysis of Norwegian, Spanish, U.K. and U.S. newspapers (2016–2017), it studies how human-interest stories are contextualized, health problems explained and responsibility attributed. The article reveals a complex picture of the role of human-interest stories in health coverage. In line with expectations, the study finds that human-interest stories do tend to emphasize individual biomedical treatment of illness and to privilege idealized victims who fit the routines of dominant media dramaturgy. In contrast to theories that consider personalization of news as an individualization of responsibility and dumbing down of public debate, however, the study finds that human-interest narratives are also used to explain health as a structural phenomenon and a collective responsibility, appealing to political intervention and accountability of health authorities. Such claims are more prominent in European human-interest health stories and less frequent in the more strongly commercialized U.S. health and media system.
A focus on the experience of ordinary people in the form of human-interest stories that bring ‘a human face or an emotional angle to the presentation of an event, issue, or problem’ (Semetko and Valkenburg, 2000: 95), has gradually become more prominent in the current media landscape (Beckett and Deuze, 2016; Wahl-Jorgensen, 2016). Human-interest narratives are tools that can captivate and engage the audience, influence public opinion and bring revenue for media organizations (Zillmann, 2002). Health journalism has traditionally been strongly dominated by elite sources such as medical experts and health authorities (Briggs and Hallin, 2016), but also within this journalistic beat, studies suggest an increased focus on the personal experiences of ordinary people, both within traditional news media (Hinnant et al., 2013; Stroobant et al., 2016) and in social media networks (Conrad et al., 2016). Case studies have explored how health journalists reflect on their use of lay person exemplars (Hinnant et al., 2013; Figenschou, 2017); how health interest groups pitch such exemplars to the media as part of their strategic media work (Thorbjørnsrud and Ytreberg, 2020), and how lay people represented in health news disproportionately represent younger persons (Stroobant et al., 2016) and idealized victims (Seale, 2002).
There is, however, a lack of studies that explore the function of human-interest stories in health reporting more broadly and systematically. In spite of its wide appeal across social backgrounds and media platforms (Hamilton, 2004; Lalazaryan and Zare-Farashbandi, 2014), in-depth studies of health journalism in general have been few both within journalism studies and in sociology of health and medicine (but see Briggs and Hallin, 2016; Seale, 2002; Stroobant et al., 2016). Particularly, comparative and systematic analysis beyond single case studies has been lacking (but see Hallin, Figenschou and Thorbjørnsrud, 2020). Addressing this gap, the present study conducts a comparative content analysis of newspaper health coverage in four Western democracies (Norway, U.K., Spain and the U.S.). Focussing on how human-interest stories are related to dominant understandings of health and the attribution of responsibility to avoid and fight illness, it asks: How are human-interest stories contextualized, health problems explained and responsibility attributed in contemporary health journalism across media systems and health systems?
The article builds on a theoretical framework that contextualizes human-interest stories as part of broader processes of popularization and commercialization of the media, and outlines two opposing theoretical approaches to the impact of human-interest stories in news reporting. The first, and traditionally dominant line of argument, emphasizes that personal stories, by ignoring structural and social conditions and focussing on episodic, singular events, tend to attribute agency and responsibility to the individual (Eide, 2017; Iyengar, 1994). The other emerging approach to human-interest stories takes the opposite view, and argues that the use of personal accounts spurs calls for collective action and appeals to public authorities to take responsibility (Boukes et al., 2015; Hopmann et al., 2017; Ostfeld and Mutz, 2014; Zillmann, 2002). In the following, we elaborate on these two main positions; how they relate to the development of health journalism and political advocacy, and how a (perceived) impact of such personal narratives may privilege some stories and some victims of disease over others.
Analytical framework
Popularization and personalization of health coverage
Health coverage includes a wide variety of topics, reflecting increasingly wide definitions of what health and illness encompass and the increased use of advanced medical interventions. The health sector is characterized by rapid progress and the expansion of medical science (Briggs and Hallin, 2016) and medical science is increasingly specialized and technical. Hence, health reporters often remain dependent on medical expertise (Tanner et al., 2015) and perceive themselves as translators and interpreters of medical information (Hinnant et al., 2016). Consequently studies identify dominant sources and actors in health coverage to be scientists, medical experts and government officials (Amend and Secko, 2012). Nevertheless, broader processes of popularization of the news media (e.g. Hughes, 2014; Otto et al., 2017), have arguably made their impact on health coverage, as a less deferential tone towards medical elites has been paired with a stronger focus on the personal experinences of lay people (Schudson, 2015).
Stories focussing on personal experience have in particular long been deemed imperative in commercial television and popular magazines (Figenschou, 2017; Stroobant et al., 2018) and have been found to be most prominent in market-oriented media systems (Umbricht and Esser, 2016). Compelling personal narratives are deemed to increase audience engagement (Wahl-Jorgensen, 2016), reflecting and competing with the explosion of personal stories in networked social media (Beckett and Deuze, 2016). Typical health stories in weekend magazines or commercial television news include celebrities sharing their weight struggles, accounts of medical miracles or tear-jerking stories of medical scandals. Such ‘tabloidization’ is often criticized for dumbing down news and political reporting. In line with this broader criticism, personal narratives have often been seen as simplistic and emotional, low quality reporting (Pannti, 2010), although more recent work questions the premise that quality journalism and emotional, personal narratives are mutually exclusive (Wahl-Jorgensen, 2016). Similar criticism is present in discussions about the use of personal narratives in health journalism, where critics are concerned about emotionalizing and simplifying health issues at the cost of scientific reason (Hinnant et al., 2013). Based on this literature on human-interest reporting as a result of commercialization and popularization, we would expect health coverage in countries with the most commercialized media systems to have the highest proportion of human-interest stories, we therefore hypothesize that:
Hypothesis 1: Human-interest framing in health journalism will be most prominent in the most commercialized media systems compared to less commercialized media systems.
The impact of human-interest framing
A broad literature finds that the use of personal exemplars has the potential to attract and engage the audience. This impact is explained by factors such as vividness, proximity, identification and the activation of emotions. Regarding how human-interest stories influence audience attitudes, conclusions have been more mixed (Ostfeld and Mutz, 2014). The response to a story is dependent on several factors, and audience involvement and attributions of blame and responsibility are highly related to different emotional cues.
One tradition has focussed on how the use of human-interest frames tends to individualize and privatize social life, at the expense of explaining social phenomena as structural and political (Eide, 2017). A particularly influential contribution here, Iyengar’s (1994) study, finds that episodic news based on individual cases leads to the attribution of individual responsibility and blame rather than stressing solidarity, collective solutions or holding politicians accountable. Hence, personalized news is argued to encourage people to take an egocentric view on political issues (Bennett, 1996). For health news in particular, the attribution of responsibility to the individual for their health and well-being may be related to the expansion of service and life-style journalism, inducing the individual to make informed choices and lifestyle changes to minimize their risk of falling ill (Briggs and Hallin, 2016; Eide and Knight, 1999). Typical popularized formats are inspirational features of people who have improved their health and lifestyle; confessional shows where ordinary people are being helped on air, or online help groups where lay experts help each other (Fürsich, 2012). It is an underlying premise here, connected with the shift towards neo-liberal ‘governmentality’ that patient-consumers are expected to make rational choices to maximize their well-being, promoting certain products, cures or lifestyle regimes (Briggs and Hallin, 2016). From this strand of literature we hypothesize that:
Hypothesis 2a: Health journalism with a human-interest frame is associated with attribution of responsibility at the individual level, including appeals to self-governance and individual responsibility to avoid illness and choose healthy lifestyles.
On the other hand, more recent studies within exemplar theory have demonstrated that human-interest stories actually might increase attribution of responsibility to government and support for political intervention (Boukes et al., 2015; Ostfeld and Mutz, 2014), particularly when the individuals featured are similar to the audience (Andersen et al., 2017); are portrayed as deserving and innocent (Hopmann et al., 2017) and when the story resonates with deep-seated values and prior beliefs (Chong and Druckman, 2007). As revealed by experiments, who is chosen to represent or illustrate an issue impacts how it is understood and where blame is directed. Journalists’ choice of deserving or undeserving exemplars thus influences the impact of a story (Skovsgaard and Hopmann, 2020).
Buttressing the arguments from experimental exemplar theory, content and text analysis of human-interest framing in the coverage of foreign affairs, migration and international crisis, find that human-interest stories tend to privilege unambiguously innocent victims and ‘worthy’ heroes as a means to gain attention and engagement (Figenschou and Thorbjørnsrud, 2015; Moeller, 2002). With regard to health news, Seale (2002) similarly argues that patients and their relatives are routinely given the role of suffering victims and fighting heroes, whereas politicians or health bureaucrats are often portrayed as ‘villains’ rejecting to provide the necessary treatment or care. Seale (2002) further finds that children and those who care for them are portrayed as undeserving of their fate, brave and positive in spite of their situation.
In health journalism in particular, these are stories that rather than communicating how the individual can avoid risk, typical for classic service journalism, communicate their grievance and indicate that someone else is to blame and should take action (Eide and Knight, 1999; Seale, 2002). This strand of literature thus questions the correlation between human-interest frames and individualized responsibility (discussed above) and on this basis we formulate an alternative hypothesis:
Hypothesis 2b: Health journalism including a human-interest frame will involve calls for political intervention and collective responsibility on behalf of the inflicted individual, and will therefore address readers not only as patient/consumers but as citizens.
Personal stories as tool for political mobilization in different national contexts
Studies of the media strategies of organized health interest groups and patient movements indicate that media’s appetite for compelling personal stories interacts with the need of these groups to engage the audience, raise awareness and impact political decisions (i.e. Figenschou and Thorbjørnsrud, 2020). Reflecting the impact of media bias, studies find that health advocacy groups adapt to the preferences of the media and forward representatives that are more in line with the media’s preferences for youth, pretty faces and charismatic personalities rather than representative of the standard patient suffering from the affliction in focus (Thorbjørnsrud and Ytreberg, 2020). Providing compelling exemplars to the media gives the groups much-wanted visibility and attention, enabling interest groups to raise awareness, mobilize supporters, mount political pressure and impact political decisions and priorities (Fredheim, 2021; Thorbjørnsrud and Ytreberg, 2020). In line with this approach to personal stories as tools for political mobilization, we expect that there will be more human-interest stories that attribute responsibility to health authorities and governments in countries in which health is clearly established as a public and political responsibility, based on universal public health care. We hypothesize that this tendency is further enhanced in countries where public responsibilities go beyond biomedical interventions and treatment. This involves the institutionalization of the rationale of social medicine in public health policy (Hobæk and Lie, 2019), a public health policy that emphasizes preventive measures linked to socioeconomic conditions. Further, we expect that appeals to public health authorities and collective responsibility will be less frequent in systems with commercial and market-based health systems. In market-based systems the responsibilities of public health authorities are more disputed and medical actors and health practitioners have stronger economic incentives to appeal to individuals as rational (high) consumers of lifestyle regimes and medical interventions. Based on this argument, we hypothesize that:
Hypothesis 3: Human-interest frames that appeal to collective responsibility and socio-economic explanations for health will be more frequent in countries with public health systems than in countries with a market-based and commercial health system.
We test these hypotheses based on a comparative quantitative content analysis supplemented by a close reading of the news stories that employ human-interest frames. The method and design is outlined in the next section.
Method and design
The study is based on samples of health news in newspapers from four countries, chosen to represent different models of both health care system and media system: Norway, Spain, the U.K. and the U.S. Two broad models of healthcare systems are represented (Beckfield et al., 2013). The U.S. is the classic case of a highly commercialized, private insurance system: health care providers are mostly private institutions, with over half of U.S. health expenditures sponsored by private sources. The U.K., Norway and Spain all represent variants of the Beveridge model, characterized by tax-based funding and comprehensive coverage, publicly-owned and operated hospitals and universal access based on residency. While all three health care systems have seen the growth of private service providers and supplementary private health insurance, large majorities still rely on the universal and state-run public system (Giovanella and Stegmüller, 2014).
The four countries also vary in their media systems, with the US representing the classic case of the Liberal model in Hallin and Mancini’s (2004) typology, Norway a classic case of the Democratic Corporatist model, Spain a variant of the Polarized Pluralist model and Britain a mixed case between the Liberal and Democratic Corporatist models, or an example of what Brüggemann et al. (2014) refer to as the Central model. The primary media system variable in this analysis is commercialization, and as the analysis deals with newspapers, the US and Britain, with their highly competitive tabloid market, could be considered the most commercialized, and Norway, with its subsidized newspapers, the least. In each country, three newspapers were chosen which would cover major categories of the print press within that system. In Norway they were Aftenposten, the best-known national ‘quality’ broadsheet (centre-right in political orientation), VG, the principal tabloid and Bergens Tidende, a regional newspaper. For Spain they included two Madrid newspapers with national circulation, El País (centre-left in political orientation) and El Mundo (centre-right), and the most important Barcelona-based newspaper, La Vanguardia. For the UK they included two broadsheets, The Guardian (centre-left in political orientation) and The Telegraph (centre-right) and one tabloid, the Daily Mail. For the US they included The New York Times, the principal newspaper of record, the Houston Chronicle, a regional newspaper and USA Today, a national newspaper and flagship of a chain with many local newspapers. The keywords medicine, medical, doctor, health, illness, pharmaceutical and nutrition (and equivalents in Norwegian and Spanish) were used to identify stories, which were screened by the coders to confirm that they were indeed centrally focussed on health issues and to eliminate sponsored content. From this broader sample five stories from each paper that had health as the main topic were sampled from each month through 2016 and 2017, a total of 120 stories for each newspaper. Consequently, our sample covers health stories over a 2-year-period, avoiding the possibility that a few major stories should impact the data. Aiming to analyse these newspapers full coverage of health to reflect that health is an issue with particular broad appeal (Hamilton, 2004) and to fully capture the complexity of human-interest framing, we included health stories across genres (including news articles, feature stories, op-eds and editorials), comprising a total sample of 1440 articles.
Newspapers remain central to the construction of issues in the public sphere, particularly in discussion among elites and active publics, and are therefore a good focus for initial analysis. Clearly, however, a full account of health news across the four countries in the current media landscape would require looking at multiple media outlets (Stroobant et al., 2016). Selecting newspapers for comparative analysis represents a conservative test regarding the presence of human-interest in health coverage. Other, more popularized formats such as commercial television and popular magazines traditionally rely more heavily on a personalized and emotional type of journalism. Newspapers tend to play different roles in different countries. In our sample, Spanish newspapers are more elite-oriented, with television traditionally reaching the wider audience. In Norway and U.K., on the other hand, newspapers to a higher degree also appeal to a mass market, involving combinations of hard and soft news that combine tabloid, commercial styles of reporting with the critical watchdog role of the press (Eide, 2017). Hence, by comparing the role of human-interest stories in newspapers across these countries, we are also able to gauge possible differences in the role of human-interest stories in countries where tabloid and broadsheet newspapers have different roles and different reach.
Measures
The primary measure in this study is the human-interest frame, building on Semetko and Valkenburg’s (2000) authoritative operationalization: the use of human examples, adjectives or personal vignettes that generate empathy, consideration of how individuals are affected, personal or private information and visual information that generates empathy. Expanding this approach, we have measured to what extent the human-interest frame is present in an article, coding the human-interest frame as ‘not present’, ‘present but not dominant’ and ‘dominant frame’.
To analyse how human-interest frames are contextualized we include measures of the audience orientation of health stories, and of framing of health issues and attributions of responsibility which follow from different frames.
In terms of audience orientation, we followed Hallin et al. (2013) in mapping four target audiences of health news based on textual characteristics of the stories. The target audience variables measure whether human-interest stories approach the audience as individuals and potential patients, political citizens, biomedical professionals or potential investors in the biomedical industry. Stories targeting the audience as patient/consumers are written to inform individuals about how to cope with health problems, what treatments are available, how and where to get help and, more broadly, the pursuit of ‘wellness’. Stories coded as characteristic of this audience orientation are identified by such indicators as providing advice and practical information to readers, use of the second person ‘you’, providing basic explanations of scientific knowledge or procedures of health institutions and recounting the experience and perspective of patients or families. Stories coded as targeting the audience as citizens address health issues in terms of public policy or, more broadly, social choice (as for example in reports about genetic engineering that may be framed in terms of ethics). Beyond the focus on public policy, stories coded as characteristic of this audience orientation are identified by such indicators as the inclusion of politicians as sources and the use of conventions of political balance. Stories coded as targeting the audience as investors provide business-related information, and are identified by such indicators as references to particular health businesses (e.g. stock prices, market share and fundraising), and the use of business analysts as sources. Stories coded as targeting the audience as professionals are those that address readers directly involved in health professions as well as those interested in biomedical science for its own sake, and are identified by such indicators as use of technical language, providing details about research methodology and clinical practice, and making reference to developments that affect the privileges and working conditions of biomedical professionals. These target audience or audience orientation variables were coded according to a ‘fuzzy set’ logic, with stories coded as ‘not characteristic’, slightly characteristic’, ‘substantially characteristic’ and ‘strongly characteristic’ of each model.
A second set of variables measured the framing of underlying causes and solutions for health problems in terms of a common distinction in public health and sociology of health, among three perspectives. The biomedical frame explains health and illness as biological phenomenon that can be cured by pharmaceutical and other biomedical interventions and technology (Breilh, 2008). The lifestyle frame explains health as a result of individual choices and actions (Clarke and Everest, 2006), while the social frame emphasizes factors outside of the control of the individual, such as socioeconomic factors and disease prevention on a societal level, factors such as poverty, pollution or breakdowns in the regulation of food safety. These frames were not considered mutually exclusive, and were coded as not present, present but not dominant and as the dominant frame for each story. With regard to the issues posed here about attribution of responsibility and human-interest framing, it is particularly the contrast between the social frame and the two other frames that is of interest: the biomedical and lifestyle frames involve approaches to health that focus on the individual body and individual choices, whereas the social frame represents an approach to health as defined by collective and structural measures.
The multilingual, international team (authors and assistants) organized several workshops to develop, test and adjust the code book, before three assistants (who are all fluent speakers in the languages they coded) conducted the analysis. Intercoder reliability for these variables, calculated using Krippendorf’s
In addition to the quantitative content analysis the authors conducted a close reading of the human-interest stories, to provide insights into how this frame is used beyond the quantitative approach. In this qualitative analysis, the authors studied the lay actors featured in human-interest stories more closely, to assess who they are: from what position they speak (patients, relative or other lay actors), their gender (men or women), their age (children/adolescents, working adults or elderly individuals) and further what health issues these protagonists represent. Throughout the analysis insights from this close reading will be added to inform and explain the quantitative findings.
Analysis
Human-interest framing in health journalism: Scale and scope
One third of the articles in our sample employed a human-interest frame. In 18 percent, the human-interest frame was dominant, meaning that the personal account and experience of ordinary people is the key narrative of the story. An additional 14 percent incorporated human-interest elements to introduce or briefly exemplify the health issue covered, though the human-interest frame was not dominant. Figure 1 shows the frequency of human-interest elements in the four countries. Norway has the highest proportion of human-interest frames (it is more often used and more often the dominant narrative), followed by Spain, and then the U.S. and U.K. These results are surprising if commercialism, either of the media system or the health system, is considered to be the primary determinant of human-interest content (as proposed in H1). In the U.S. coverage we also find that human-interest framing, when present, is less prominent in the stories. H1 is not confirmed, and this result suggests that something more is probably going on with the human-interest content than pure commercialism in the classic sense.
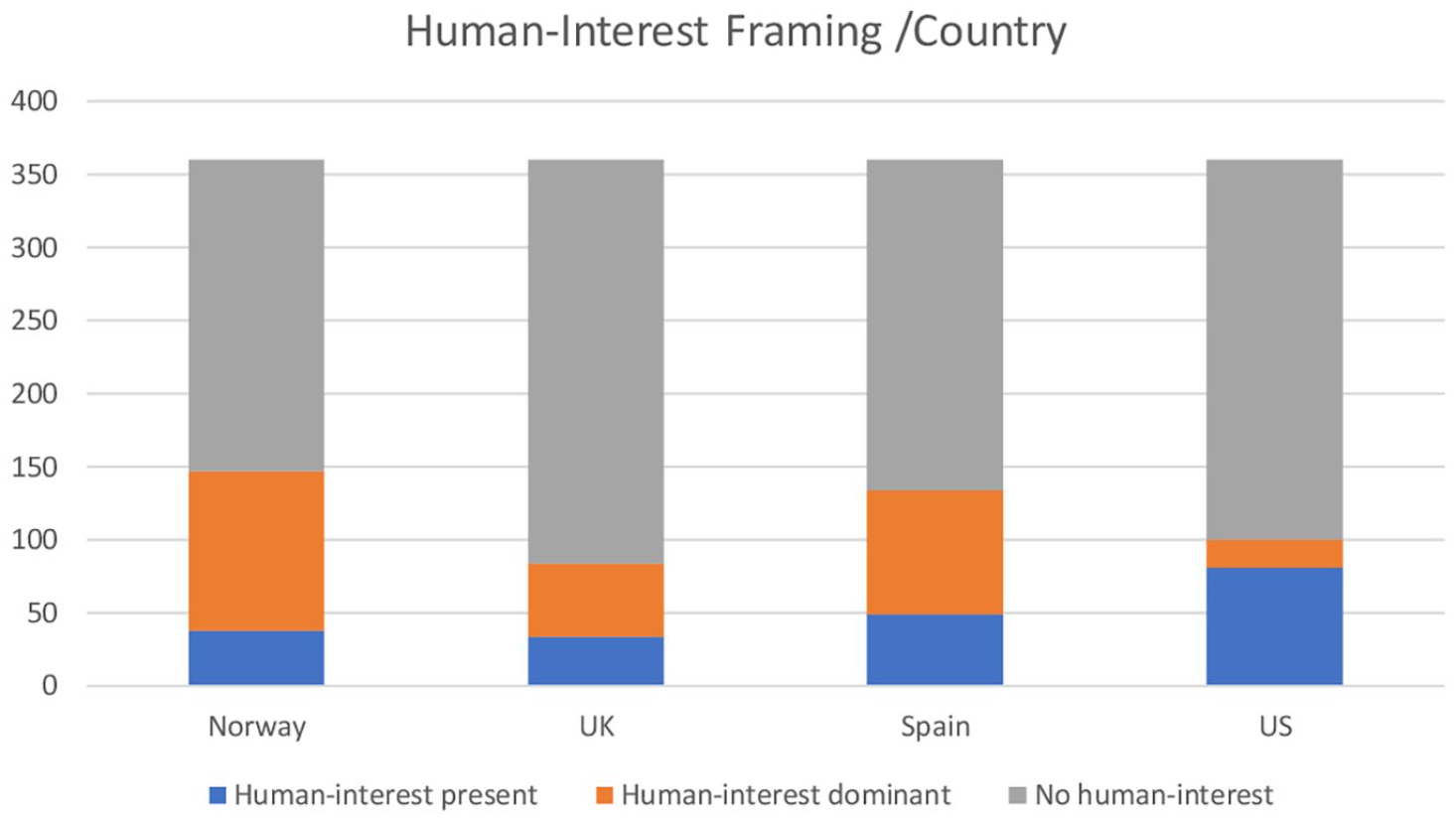
Human-interest framing in health coverage in Norway, U.K, Spain and U.S. (N = 1440).
Regarding whose stories are featured in human-interest narratives in health journalism, our analysis confirms previous studies finding that lay person exemplars have become important in health journalism today (see Hinnant et al., 2013; Stroobant et al., 2016). Stories focussed primarily on patients (60%), family members of patients (13%) and biomedical professionals (18%), with 8 percent of the exemplars in the ‘other actors’ category. The two countries with the highest number of human-interest stories, Norway and Spain, stand out in different ways. One factor in the high level of human-interest content in Norway is the relatively high number of patients and their family members sharing their stories with health reporters. In addition to the many news stories with human-interest framing, the Norwegian papers published many op-eds (26 op-ed articles) written by patients and their next of kin. The Spanish newspapers, on the other hand, had the highest number of human-interest stories about biomedical professionals. They were featured in about one-third of the articles with human-interest framing. In part, this reflects a common practice in the Spanish press of publishing in-depth interviews and feature stories with doctors and biomedical researchers, focussing on their careers, use of new medical technology and personal experiences from clinical practice. Human-interest stories featuring health professionals were also a bit more prevalent in the US than in Britain or Norway.
Zooming in on these human-interest stories featuring ordinary people as the main actor, we find more females than males (female patients or females in the roles as care-takers – mothers, daughters or spouses of patients). Women are the main actors in the human-interest narratives in almost six of 10 articles, a finding that concurs with broader studies on ‘ordinary people’ in the media, as the role of unaffiliated, lay actors is one of very few positions in the news media where there are more women than men (Wheatley, 2020). Further, although most of the patients featured are adults, there are notably more children and adolescents than elderly patients. This indicates that the use of human-interest frames does not reflect the ageing of the population and its related health consequence. This age distribution corresponds with previous studies which find that the aging wave is not reflected in health news (see Stroobant et al., 2016) nor in medical status hierarchies (Album and Westin, 2008). Particularly small children are foregrounded as victims of grave conditions (such as cancer), and typical articles emphasize the children’s suffering from malpractice and insufficient health care services.
Engaging private individuals or citizens? Target audiences in human-interest framing
In terms of audience orientation, articles with human-interest framing show a significant tendency to address the readers as individual patient-consumers, as Table 1 shows. This audience orientation is strongly or substantially characteristic of 64 percent of articles in which the human-interest frame is dominant. This is expected, as recounting the experience and perspective of patients or families is one of the defining characteristics of this audience approach. This approach is typical in classic human-interest narratives where the story of the individual person is laid out, focussing on the particular disease and personal story of the main actor, without explicit reference to general interest or collective action. This result can be seen as consistent with Hypothesis 2a, which associates human-interest framing with commercialized and individualistic approaches to health.
Patient-consumer target audience by human-interest framing.
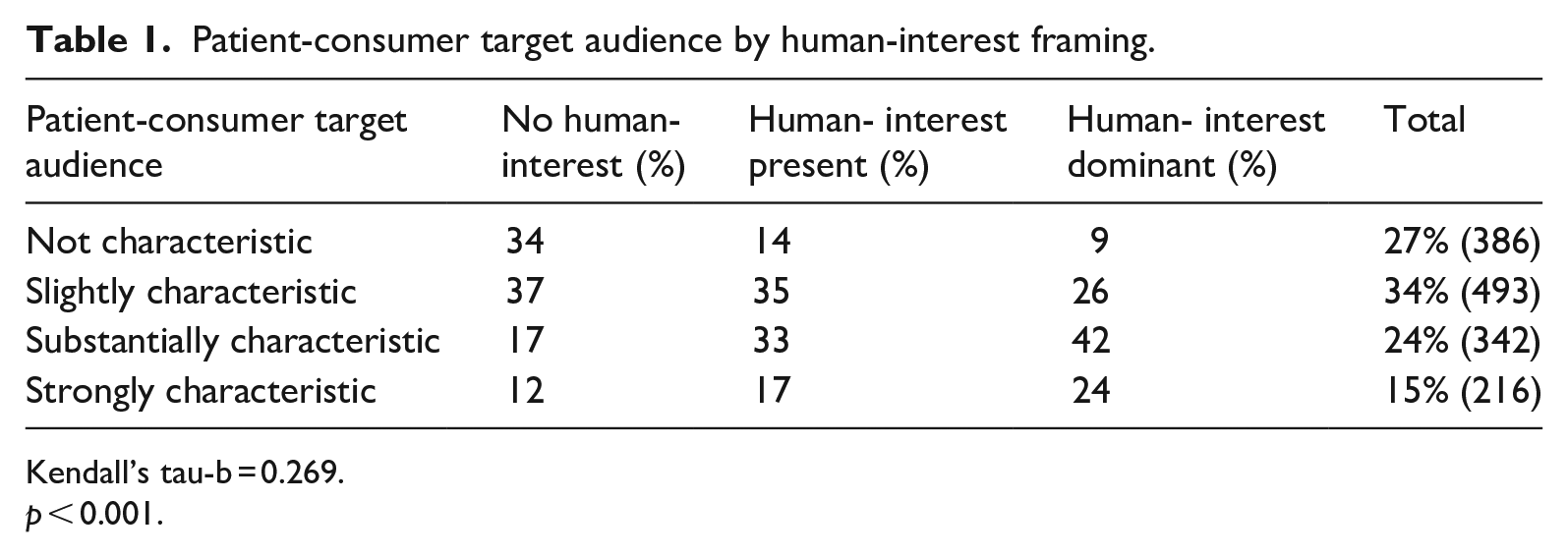
Kendall’s tau-b = 0.269.
p < 0.001.
More interesting is the question whether human-interest framing tends to exclude the other three ways of addressing audience measured in our study, targeting the audience as political citizens, especially, or as professionals or investors. There was, in fact, a significant negative correlation between human-interest framing and targeting the audience as citizens or investors. In the case of writing for a citizen target audience (Table 2), the negative association was strongest for the U.S., probably reflecting the fact that in the U.S. there were many stories on health policy which had a political game frame, and these rarely had human-interest elements. This may seem on the surface to support hypothesis 2a against the opposing hypothesis 2b. This is probably too simplistic a reading of the results, however. As we can see in Table 2, even if there is an overall negative association between human-interest framing and the citizen target audience, many human-interest articles do in fact address readers as citizens; just over 25 percent of stories with predominant human-interest framing were coded as substantially or strongly characteristic of the citizen target audience. A qualitative reading of these articles shows that they often illustrate negative consequences for individuals of public health policy, changes in the health care system, and medical developments. Other articles which strongly fit the citizen target audience model address accounts of medical errors and poor care, with individuals voicing claims for justice, compensation and political action.
Citizen target audience by human-interest framing.
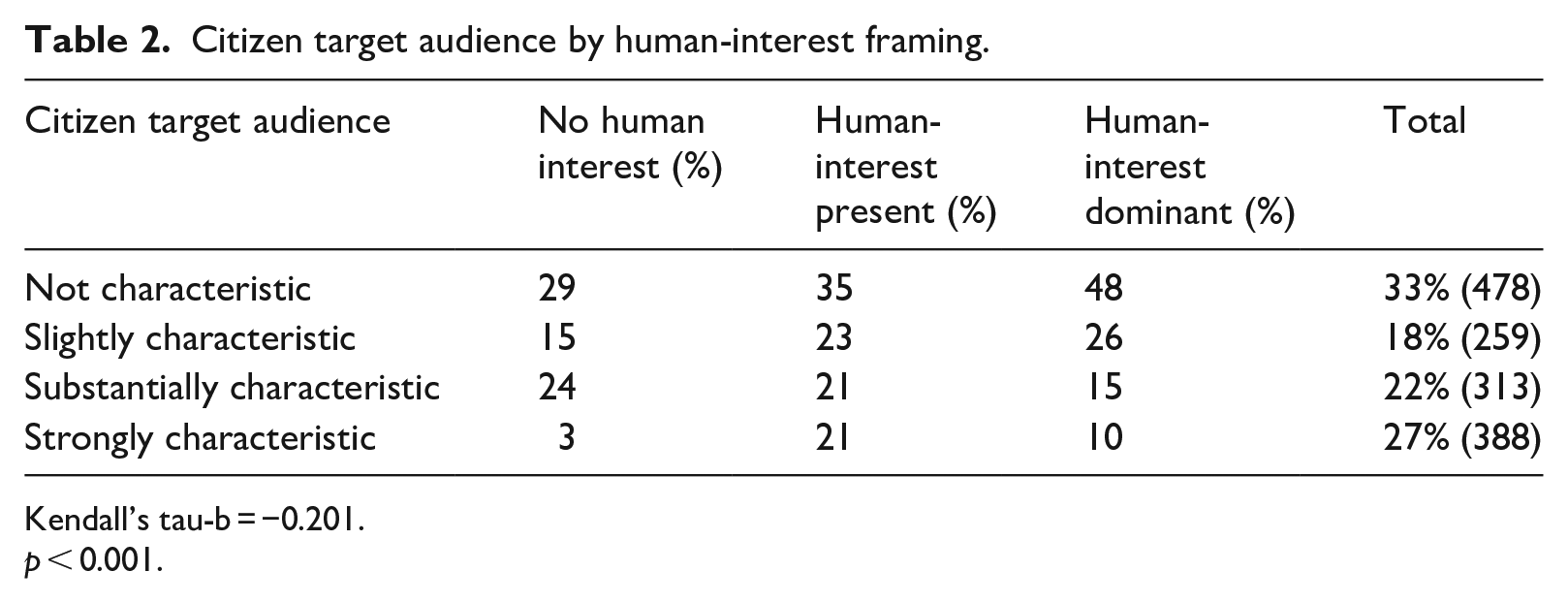
Kendall’s tau-b = −0.201.
p < 0.001.
There was no significant correlation, positive or negative, between human-interest framing and addressing the audience as biomedical professionals. As this audience approach provides technical medical information, information about research methodology and the medical professions, we would not expect a high number of human-interest stories with the professional audience orientation. Nevertheless, one third of the human-interest articles address readers as professionals or experts, which indicates that the use of human-interest framing is not solely a marker of simplification of (health) journalism, but is used as one of many journalistic tools across genres. Medical anthropologists have noted the rise of the ‘expert patient’, a lay person with a chronic disease who follows research carefully (Dumit, 2012). Reporting on new biomedical research is often directed simultaneously to specialized readers working in biomedicine, and to these expert patient readers, with the exemplars serving both to bridge these audiences, and, as Hinnant et al. (2013) note, to draw a wider range of readers into otherwise technical stories.
Moreover, the analysis show that different target audience approaches are often combined. Although almost all the human-interest articles address readers as patient/consumers, both the citizen model (addressing the audience as political citizens) and the professional model coexist with the patient-consumer model in about half the stories. Particularly in the European context, criticism of medical errors or substandard care tends to be followed by calls for political intervention, particularly in the U.K. and Norway; in these cases it is clear that human-interest frames can be politicized, consistent with hypothesis 2b. This further nuances the traditional approach to human-interest framing as a simplified, one-dimensional style of journalism.
Framing of health and attributions of responsibility in human-interest stories
Tables 3–5 show the association between human-interest framing, and our three variables which measure the framing of health issues in terms of pharmaceutical and other biomedical interventions and technology (biomedical framing), as a result of individual lifestyle choices and actions (lifestyle framing), or as caused by socioeconomic factors which call for disease prevention on a societal level (social framing).
Human-interest framing in health journalism is positively associated with the biomedical frame (Table 3), which conveys an understanding of health in line with a dominant medical model. This frame is dominant in one third of the articles in which human-interest frames are also dominant, and present in two thirds, and is particularly prominent in the Spanish coverage (reflecting the high number of biomedical professional actors in the Spanish human-interest stories). These health stories lay out personal experience of going through medical treatments, living with various health conditions, and the benefits of new treatments and technological breakthroughs. Stories on new developments in medical technology were very common in our sample and often included human-interest element; often patient-exemplars are provided for such stories by public relations officers for pharmaceutical companies. The predominance of the biomedical frame across contrasting health and media systems reflects the broad hegemony of the ‘biomedical techno-service complex’ (Clarke et al., 2003: 167). And its correlation with human-interest framing is again consistent with Hypothesis 2a and the idea that human-interest framing tends to individualize issues.
Biomedical framing of health by human-interest framing.
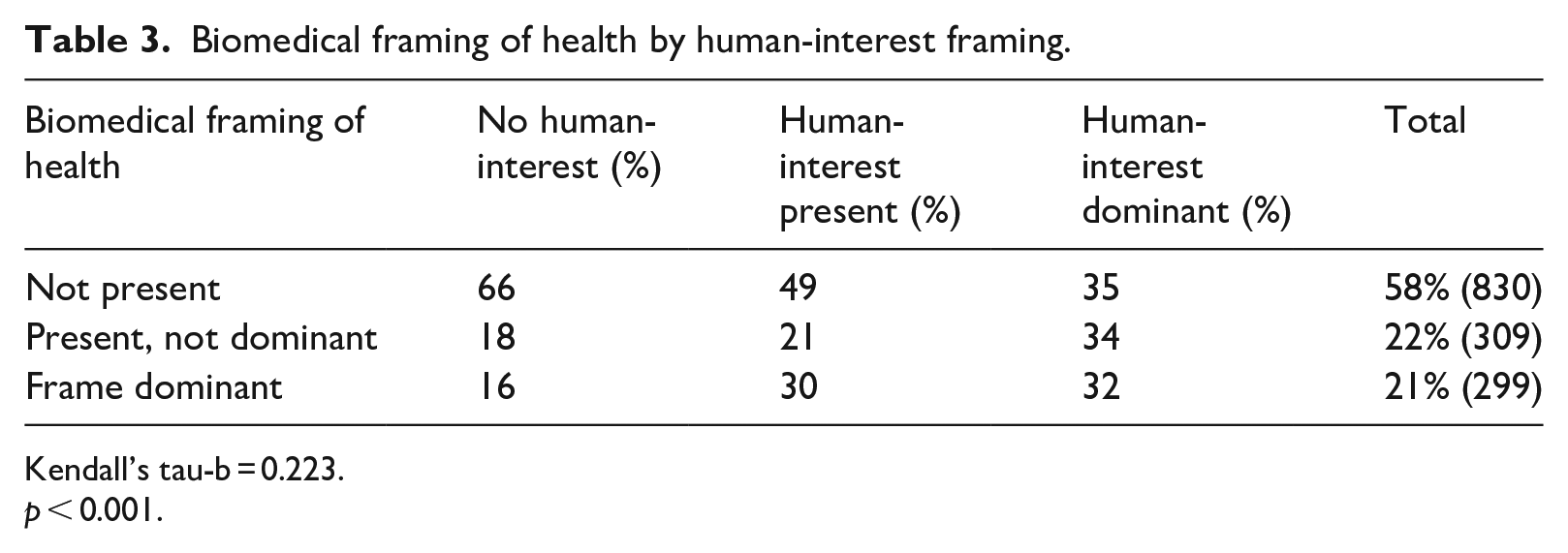
Kendall’s tau-b = 0.223.
p < 0.001.
On the other hand, the lifestyle frame, which explains health as a result of individual choice, was uncorrelated with human-interest framing (Table 4), and here the results fail to support hypothesis 2a. The lifestyle frame was less prevalent in the sample overall than the other two health frames, and we thus find little support for the hypothesis that human-interest narratives and the role of lay persons in health is reductive to the attribution of individual responsibility in the sense of the ‘governmentality perspective’. In three-fourths of the human-interest cases, there is no lifestyle frame present at all. Here, however, there was one notable country difference: For the U.S., there was a significant positive correlation (tau-b = 0.182, p = 0.001) with human-interest framing. A lifestyle frame is present in 36 percent of the US human-interest stories, 23 percent in Spain, 19 percent in the UK and 14 percent in Norway. This may reflect more commercial or individualistic, neo-liberal context of the U.S. health system or more specifically the prevalence of styles of service journalism focussed on ‘wellness’, though it should be noted that lifestyle frames were not more prevalent in the wider sample of U.S. health journalism, beyond stories using a human-interest frame.
Lifestyle framing of health by human-interest framing.
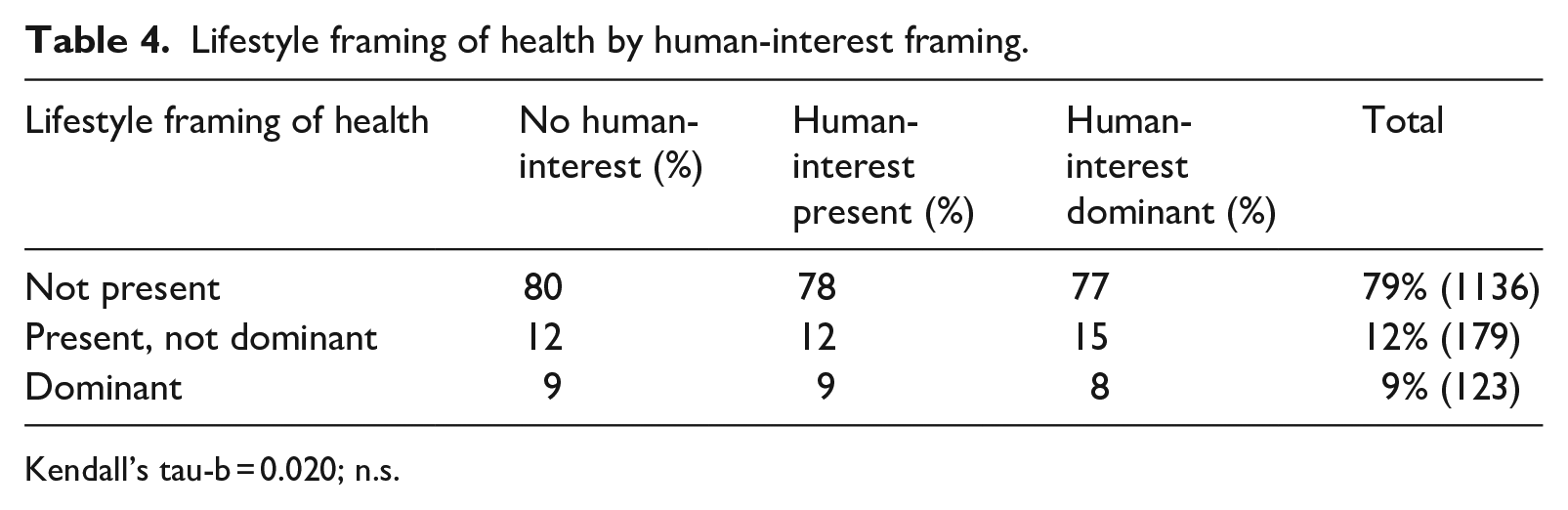
Kendall’s tau-b = 0.020; n.s.
When we turn, finally, to the social frame there was again no significant relationship with human-interest framing, and as we saw with our audience orientation variables, even if human-interest framing may commonly be associated with more individual-level understandings of health – here mostly focussed on biomedical intervention – it certainly can be deployed in journalism focussed on social and political perspectives (Table 5). The social frame was present in 48 percent of stories with human-interest framing dominant, and 38 percent of stories where it was present but not dominant. The social frame is present in human-interest stories in roughly the same percentage as in the overall sample, including articles that convey the individual health consequences of such factors as social disparities, environmental hazards poverty, and work-related stress, and thematize these as collective issues. Here again we do find significant support for Hypothesis 2b, and our results challenge the perception that personalization of health journalism automatically involves the attribution of individual responsibility at the expense of socio-economic and political approach to health.
Social framing of health by human-interest framing.
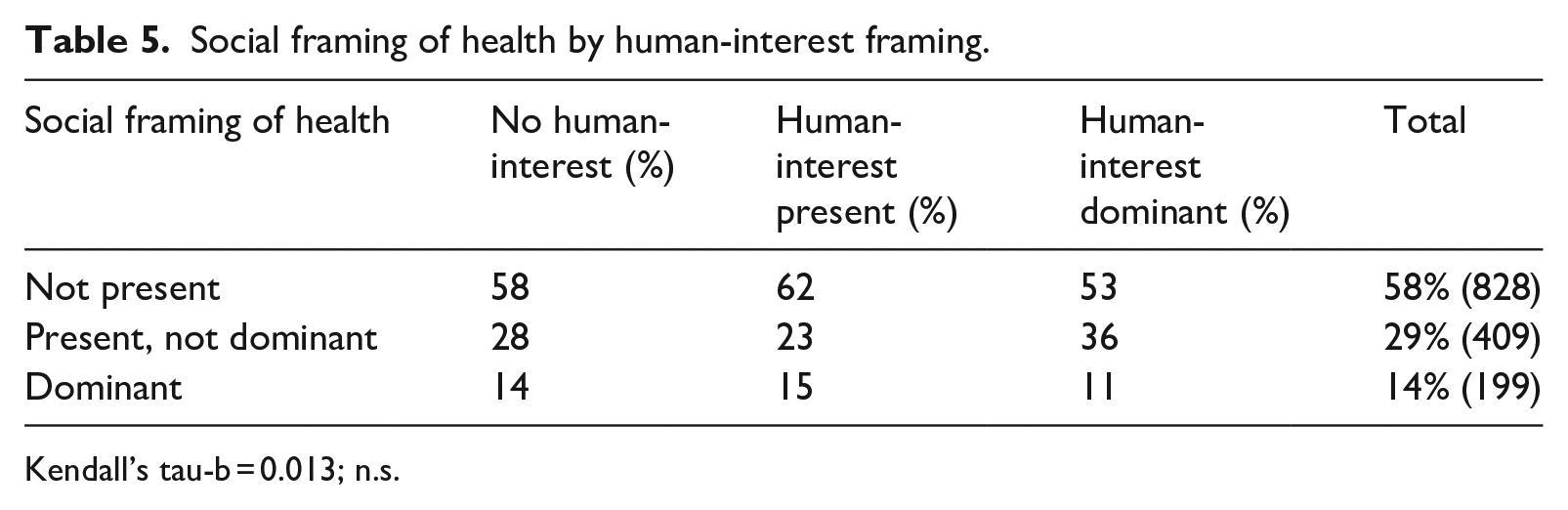
Kendall’s tau-b = 0.013; n.s.
As with the target audience variable, health frames also appear in combination in our data, the biomedical frame, in particular, being combined with the social frame and the lifestyle frame (whereas the lifestyle frame and the social frame are rarely combined). Particularly in-depth stories of individual experiences with health and illness will often involve multiple aspects and reflections, which combine and cut across these different approaches to health.
In comparative terms, social frames were, in general, more prominent in the European countries in our sample than in the United States (Hallin et al., 2020), and this is also the pattern when human-interest frames are employed. A social frame is present in 57 percent of the Norwegian human-interest stories, 46 percent in the UK, 41 percent in Spain and 24 percent in the US. Hypothesis 3 is thus supported. We find that more human-interest frames appealing to collective responsibility and socio-economic explanations for health in the European countries with extensive public health care system compared to the privatized commercial US health care system. Norway (representing the Nordic welfare state) and the US represent opposite ends of the spectrum regarding the presence of social frames. The strong presence of social frames in Norway probably reflects the institutionalization of social medicine (emphasizing social inequality and socioeconomic factors) within public health authorities and health care institutions (Hallin et al., 2020).
Concluding discussion
In this study we analyse how human-interest narratives are used in contemporary health journalism across media and health systems, focussing on the question raised in previous studies of whether human-interest framing tends to privilege the understanding of issues at the individual level, displacing understandings that focus on accountability of public institutions for health problems. The picture we found was complex.
We found human-interest framing to be very common in health journalism across the four countries, present in about one third of all stories. Contrary to expectations, however, we did not find it most common in more commercialized media systems – or in the US with its more commercialized health system. It was most common in Norway, which would generally be considered to have the least commercialized media system of the four. As Eide (2017) argues, Norwegian newspapers combine popularization and critical news journalism, with human-interest frames prevalent across many news genres, including politically-oriented reporting; it is not narrowly associated with service journalism or infotainment.
Looking at the audience orientation we found that stories employing a human-interest frame did tend to address individual patient-consumers, and were less likely to address readers as political citizens, biomedical professionals or potential investors. This was not surprising, as human-interest stories clearly focus the experience of particular individuals, usually patients and their families; to a significant extent the criteria for coding our patient-consumer target audiences and human-interest framing variables overlapped. Human-interest framing was negatively correlated with the citizen target audience. The association was not strong, however, and many stories with human-interest frames did, in fact, address readers as citizens. Often, multiple audience orientations were combined in human-interest stories. Indeed, as argued by Eide and Knight (1999), to address the audience as individuals in need of health-related information useful for personal health or as citizens, mobilized to ask for political intervention and government involvement, can be overlapping in practice (Briggs and Hallin, 2016; Eide, 2017; Schudson, 2015). This finding challenges the traditional citizen-consumer dichotomy (Eide and Knight, 1999).
If we turn to the framing of health issues in terms of the biomedical, lifestyle and social perspectives, biomedical understandings of health were present in two thirds in health stories employing human-interest frames, and dominant in a third: most of the time when individual narratives are included in the health coverage, they serve to exemplify illnesses and health issues understood as conditions that can be treated, cured or solved by biomedical intervention (Briggs and Hallin, 2016). In that sense they are indeed associated with the more individualized understanding connected with the dominant biomedical model of health. On the other hand, we did not find that personalization was correlated with a framing of health as the product of individual lifestyle choices. The relatively low presence of lifestyle frames in our study is corroborated by other quantitative studies of European health news (i.e. Stroobant et al., 2016, Thorbjørnsrud and Ytreberg, 2020). The US coverage is a partial exception here, consistent with the idea that human-interest and lifestyle frame framing can be connected in certain genres of news driven by commercial interests, advertisers or sponsors (Fürsich, 2012; Schwitzer, 2013). The fact that we have studied newspapers, and not other more commercially oriented outlets might have an impact here. Other studies find that framing health as a result of individual lifestyle is indeed prevalent on front pages (Hågvar and Alnæs, 2020) and in popular magazines and online entertainment sites (Stroobant et al., 2016). Finally, and contrary to previous studies (Clarke et al., 2003; Iyengar, 1994), we did not find that human- interest framing was negatively related to social framing. In fact, human-interest stories are regularly employed to illustrate socio-economic understandings of health and illness. This is the more often the case in the European coverage, most prominently in the Norwegian data.
The finding that human-interest stories do not consistently attribute responsibility to the individual, but in many cases appeal to collective action and intervention of health professionals, suggests that it matters which actors are selected as exemplars. From the 1960s onwards, patient rights have been formalized and politicized, and particularly influential patient organizations mobilize on behalf of their members (Schudson, 2015). For these pressure groups it is essential to use a personal narrative to gain media attention, and adapting to the media’s formats, style and news values has become crucial. Studies of media content (Seale, 2002; Stroobant et al., 2018) and also of professional health advocacy groups (Figenschou and Thorbjørnsrud, 2020; Fredheim, 2021; Thorbjørnsrud and Ytreberg, 2020), suggest that lay people figuring as victims of disease tend to conform to commercial and media dramaturgical criteria for what makes a good story. Moreover, interests that conform with the dominant medical hierarchies (Album and Westin, 2008), representing well-funded patient interest groups will dominate over critique representing marginalized groups or critique of the knowledge regimes or treatment paradigms of a biomedical field (Briggs and Hallin, 2016).
In our qualitative analysis of what roles ordinary people play in human-interest stories, we find that lay people are primarily invited into health news as patients, family members or supporters of patients. Inviting patients to share their experiences, in contrast to silence or expert jargon, can empower people in vulnerable positions (i.e. Frank, 2013). When patients and their loved ones are granted such experiential legitimacy in the media, their rights and claims are often justified in a way found to increase the attribution of responsibility to the authorities (Boukes et al., 2015). We find that female and young patients are foregrounded in the human-interest articles, illustrating how particularly ‘innocent’, media-friendly patients are privileged over others. Moreover, the qualitative reading identifies patterns of age stratification of individual health stories. Focussing on younger, more engaging and appealing patient exemplars belies the statistical fact that the chance of falling ill increases with age, and that a majority of people afflicted by diseases are elderly. Zooming in on the human-interest stories in this study, we find that media-friendly cases are privileged, supporting the existence of a ‘human-interest economy’ in international health journalism (Thorbjørnsrud and Ytreberg, 2020). Previous studies find that claims made by such vulnerable, worthy victims, whom the audience can identify with, often gain public support for their cause increasing the pressure for political or medical intervention (Hopmann et al., 2017; Ostfeld and Mutz, 2014).
The findings in this paper broaden our understanding of the role of human-interest stories in contemporary journalism. Like all studies this paper has its limitations; we particularly call for more studies of human-interest framing addressing other news topics and societal sectors, studies that systematically investigate the interplay between personal narratives in social media and human-interest narratives in established news, and further, systematic analysis of the political impact of human-interest stories and which interests these stories serve.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Research Council of Norway [grant number 258993].