
Abstract
For patients, hospital emergency departments (EDs) are unfamiliar, institutional contexts involving high-stakes communication in heightened emotional circumstances. This study examines laughter, as one expression of emotion, in an existing 649,631-word corpus of naturally occurring clinician-patient interactions recorded in five Australian hospitals. A mixed methods approach revealed (1) the spread, frequency and producers of laughter, and (2) the functions of laughter in unfolding interactional contexts. First, a corpus analysis showed that laughter in the ED was most frequently produced by nurses and patients, but relatively infrequently by doctors. Secondly, two case studies comprising all the interactions of two patients for the whole duration of their ED visits were analysed in detail to explore the individuals’ contrasting patterns of laughter. The analysis revealed how laughter can be a cue to the affective dynamics of patient-clinician interactions about serious matters, for example, signalling difficult topics and managing anxiety in the ED context. Laughter, and any related humour, can indicate the achievement of mutuality, which is considered a cornerstone of genuine shared decision-making and patient participation in their own care. Therefore, the findings suggest that a sensitive responsiveness to patient-initiated laughter, and any associated humour, may promote patient-centred relationships in clinical interactions.
Keywords
Introduction
Laughter is a universal interactional phenomenon that is ‘mediated strongly by social context’ (Scott et al., 2014: 618). Laughter can range from more spontaneous or responsive instances to more controlled or strategic ones (Scott et al., 2014: 618; Wild et al., 2003). Occasionally a contagious behaviour, laughter can be seen as a kind of ‘conversational resource’ drawn upon for multiple functions, including ‘identity work and indexing relational status through affiliation and disaffiliation’ (Boxer and Cortés-Conde, 1997; Liebscher and Dailey-O’Cain, 2013: 237). Thus, as an affective signal, instances of laughter can offer insights on the ‘dynamics of emoting in interaction’ (Mesquita, 2010: 91). It tends to occur in environments of ‘celebration’, where it enhances togetherness and intimacy; or ‘trouble’, where it can mitigate meanings, moderate actions or align interactants (Glenn and Holt, 2013). Jefferson’s influential work on ‘troubles-talk’ demonstrated that laughter can be deployed by an individual resisting a source of anxiety or tension and that, in turn, a recipient may orient to the teller’s problem, rather than joining in with the laughter (Jefferson, 1984). From a neurobiological perspective, the laughter of the troubles-teller might help to ‘“de-escalate” a negative emotional experience’ (Scott et al., 2014: 620).
Hospital emergency departments (EDs) are abundant in potential for ‘trouble’ environments: they involve encounters with strangers, medical and institutional registers and stressful circumstances. In EDs, a high state of emotional arousal occurs alongside high-stakes communication, which must be both efficient and effective given the time constraints. If we understand emotions as ‘contextualised acts’ which ‘emerge in dynamic interaction between individuals and their social contexts’ (Mesquita, 2010: 84), examining laughter, as both an expression of emotion and a ‘contextualisation cue’ (e.g. Gumperz, 2015), will provide a window on how ‘emoting’ (a ‘property of the relationship rather than the individual’) in spoken interaction might build relationships for patient-centred care. To this end, this study investigates the presence and role of laughter across participants – health professionals, patients and carers/relatives – within unfolding interactional contexts over the duration of patient visits to EDs.
Background
Communication in hospital emergency departments (EDs)
Patients typically present to EDs with no medical records or familiarity with the multiple clinicians who will treat them. Consequently, emergency care relies predominantly on spoken communication, which is subject to extreme time constraints and multiple interruptions (Fairbanks et al., 2007; Slade et al., 2008). Although both interpersonal and medical aspects of communication are critical to the implementation of patient-centred care, medical tasks are likely to be prioritised over the development of rapport and empathy with patients in increasingly challenging ED contexts (Eggins et al., 2016; Fairbanks et al., 2007). In the context of continuously increasing numbers of ED presentations, the negative impacts of overcrowding are particularly detrimental to outcomes for the most vulnerable patients (Dinh et al., 2020; Stephens et al., 2023).
In a major study of communication in EDs, Slade et al. (2015) observed that establishing ‘positive interpersonal relationships between clinicians and patients’ can lead to greater patient involvement in tasks such as treatment planning resulting in better clinical outcomes (Slade et al., 2015: 125). Using naturally occurring spoken interactions between clinicians and patients (compiled in the ‘EDCOM corpus’, introduced below), Slade et al. (2015) reported that instances of ‘shared laughter’ and ‘judicious use of humour’ appeared to ease patient anxiety and build rapport (pp. 142–143). This was one of a range of interpersonal strategies used by clinicians to nurture higher patient involvement and therefore to help ensure better clinical outcomes (Slade et al., 2015: 125). The current study furthers this observation by delving systematically into the phenomenon of laughter, as represented in the EDCOM corpus, through quantitative and qualitative explorations of the extent and role of laughter and the surrounding discourse.
Laughter in healthcare settings
Despite the large number of studies that describe ‘relational’ or ‘communication practices’ in healthcare (see, e.g. Emmamally et al., 2020; Sehlbach et al., 2020; Tubbert, 2016), relatively few have focused on the role of laughter and humour in these interactions. This is surprising, given the potential these intertwined interactional phenomena have to ease the tensions and face threats associated with sensitive topics, distressing emotions and physical examinations, and to create closer relationships between patients and healthcare professionals (Beach and Prickett, 2017; McCarthy et al., 2013; Sala et al., 2002; Phillips et al., 2018). Although laughter is also ‘the most common, overt indicator of the presence of humour’, the well-attested phenomenon of nervous laughter points to a more complex relationship (Glenn and Holt, 2013: 2; Partington, 2006). In this review, only studies that have explicitly used laughter as their unit of analysis are included. Where the identified laughter is linked to humour in a study, this is indicated.
In patient-physician interactions, patients tend to be more proactive in generating humour than their physicians (Beach and Prickett, 2017; Sala et al., 2002; Saunders, 1998). Given this finding, it is perhaps not surprising that a common subject of humour is the patient’s medical condition (Phillips et al., 2018: 274) – a troubles-telling context in which response laughter may not be the intended effect of the utterance (Jefferson, 1984). This expectation has been corroborated by a study of 60 medical consultations which found that in 70% of cases, patients’ laughter was not reciprocated (Haakana, 2002: 213). Similarly, Beach and Prickett (2017) observed that the doctors tended not to reciprocate patients’ laughter and humour about sensitive personal matters. The oncology patients in their study used laughter and humour to manage distressing and embarrassing moments, as well as to display resilience by minimising the threats associated with the disease and providing evidence for their own ‘wellness’ (Beach and Prickett, 2017: 792).
Sala et al. (2002) reported that patients were more satisfied after doctor visits that contained more laughter and humour, especially when these were generated by the doctors. High-satisfaction doctor visits contained equal amounts of laughter from patients and physicians (laughing separately and together), whereas low-satisfaction visits were more likely to contain physician laughter only. Similarly, Greene et al. (1994) found that shared laughter positively correlated with older patients’ satisfaction. Patient enablement – that is, patients’ ‘understanding, confidence and coping ability’ – was also positively associated with laughter in doctor-patient encounters (Pawlikowska et al., 2012: 70). Haakana (2002) points out that rapport-building applies particularly to shared laughter which exhibits ‘such positive interactional functions as intimacy, affiliation and alignment and to be sharing of a similar sense of humour, a similar attitude towards something’ as well as sharing equal status (p. 209).
Laughter that is not shared may have diverse effects on the unfolding interaction (Clift, 2016). In health consultations, responsive laughter can be used to pursue the institutional goals of the interaction, for example in ‘laughing off’ challenging questions and overcoming patients’ resistance (Zayts and Schnurr, 2011: 1). Such laughter, termed ‘coping laughter’, efficiently paves the way for the interaction to shift to a non-serious, more harmonious frame when the potential for conflict arises (Warner-Garcia, 2014: 177). Along with managing sensitive topics, laughter and associated humour can foster rapport between patients and healthcare professionals (Zayts and Schnurr, 2011: 1). Although laughter and overt humour are not co-extensive in interaction, humour that elicits laughter is associated with positive affect and reduced face-threat in healthcare interactions (Mallett and A’hern, 1996; Ragan, 1990). This association is at its strongest in laughter therapies (Foot and McCreaddie, 2006), but the spontaneous use of humour and laughter as conversational techniques with therapeutic effects has also been advocated in nursing contexts (Beck, 1997: 351).
Laughter occurs in complex communicative patterns in clinical communication. It is multifunctional, it varies in relation to topic and speaker, and it is associated with higher patient satisfaction. Various relational concepts have been linked to laughter, including rapport-building, down-grading potential conflicts, demonstrating resilience and therapeutic interaction. Beach and Prickett (2017) suggest that a greater awareness of the potential significance of laughter, and greater attention to instances of laughter in consultations, can help healthcare professionals to gain deeper insights into patients’ concerns, emotions and sensitivities (p. 800). Taken together, these findings suggest that laughter offers a useful window on emotional work as the basis for patient-centred relationships in clinical interactions.
Methodology
This study examines laughter in spoken interaction in a specific clinical context. It seeks to reveal general patterns of who produces laughter in EDs as well as what laughter can reveal about the emotive aspect of communication and relationships over the course of a visit to an ED. These aims are best met using a mixed-methods approach which enables investigations of group behaviours and analysis of interaction over time.
Data: The Emergency Department Communication Corpus (The EDCOM Corpus)
The EDCOM Corpus (Slade et al., 2015) represents one of the largest databases of authentic, naturally occurring clinician–patient interactions in EDs. It comprises transcribed audio recordings of English spoken interactions over 1093 hours of observations (649,631 tokens) in five large Australian hospital EDs. Participant consent was obtained first verbally and then in writing, including for secondary data analysis. Patients with immediate or imminent life-threatening conditions were not approached (only Triage Category 3 patients). The project received approval from the ACT Health and Community Care Human Research Ethics Committee (Approval number: ETH. 4.11.080). The analytic unit used by the original research team was the patient journey which comprises ‘all interactions that occurred between the patient and their attending clinicians, or other emergency department or hospital staff, from triage (assessed and categorised for emergency care) to the time of their disposition (when a decision was made either to admit them or send them home)’ (Slade et al., 2015). There are 72 patient journeys in the corpus. The EDCOM corpus is stored on the platform CQPWeb (Hardie, 2012). The process of rendering the transcriptions in this data suitable for corpus analysis is described in Collins and Hardie (2022).
Research questions
The first exploration of the data was quantitative, using corpus linguistic (frequency-based) methods, and responded to the following questions: To what extent does laughter occur? Who does the laughing?
Subsequently, we explored the circumstances and functions of the laughter, as well as the surrounding turns (or laughter episodes). This qualitative stage responded to the following questions: In what immediate interactional circumstances does laughter arise? What functions are served by the laughter and any co-occurring humour?
Stage 1: Frequency-based exploration of laughter
The EDCOM corpus contains rich metadata relating to patient and staff demographics (gender, age, language background), professional roles (nurse, doctor, radiographer, etc.) and the clinical case (presenting illness, triage category, diagnosis and duration of stay). CQPWeb enables searches using metadata queries, for example, enabling queries relating to speakers in particular roles (i.e. doctors, nurses, etc.), as well as comparisons between these. In operationalising the transcripts as a corpus, transcriber comments were recorded in XML tags (Collins and Hardie, 2022), which meant that we could direct our corpus query to locate these descriptive records of ‘laughter’ and differentiate them from, for instance, mentions of the word ‘laugh’ in the spoken content. These CQPWeb functions enabled us to explore the distribution of instances of laughter across the different participant groups.
Instances of laughter indicated by the original transcribers were identified using a wildcard search on the terms ‘laugh*’ and ‘chuckl*’ (which includes various word endings for these terms, e.g. laughs, chuckling). Alternative terminology (e.g. joking, giggling) was checked to ensure we captured all instances. We did not have access to the original recordings, but the transcripts had all been checked and revised by the researchers who collected the data between 2007 and 2010. A limitation of this study, typical of secondary data analysis, is that the laughter is only that which has been identified and deemed transcript-worthy by the transcribers and transcript checkers (see conventions in Appendix A). While this probably results in a conservative estimation of the prevalence of laughter, we can be sure that the focus of the analysis is clear instances of laughter. However, we are unable to draw any conclusions about important aspects such as the timing or quality of the laughter (pitch, duration, volume, shape), or about non-verbal, non-vocalised communication.
Stage 2: Examining laughter in context
Based on the investigation of the distribution of laughter across participant groups, we identified cases for closer examination. This sequential mixed-methods approach reveals a temporal and relational perspective on the distribution of laughter which expands, contextualises and offers some explanation on the Stage 1 findings about the distributions of laughter in the EDs (see Bryman, 2006). Because our interest in laughter arises from its potential role in patient-centred and relational care in the ED context, the qualitative analysis encompasses both the immediate interactional context and the broader institutional context. We draw on socially-oriented approaches to discourse analysis: Interactional Sociolinguistics (e.g. Gumperz, 1992; Roberts, 2014) and Systemic Functional Linguistics (e.g. Halliday and Matthiessen, 2014). In particular, instances of laughter are treated as ‘contextualisation cues’, which Gumperz (1982) defines as ‘any feature of linguistic form’ that ‘contribute to the signalling of contextual presuppositions’ (p. 131). Roberts explains that such signs can ‘nudge the inferential process in a certain direction and may have large interactional consequences if the conditions for shared interpretation are not present’ (Roberts, 2014: 199). The Stage 2 methods are based on the Stage 1 findings, and therefore these are provided in more detail following the frequency-based findings.
Stage 1: Frequency-based findings across participant groups
The queries we used to search for instances of laughter retrieved 794 matches across 69 of the 72 patient journeys. The distribution of instances across the different types of participants is shown in Table 1.
Occurrences of laughter according to participant role.
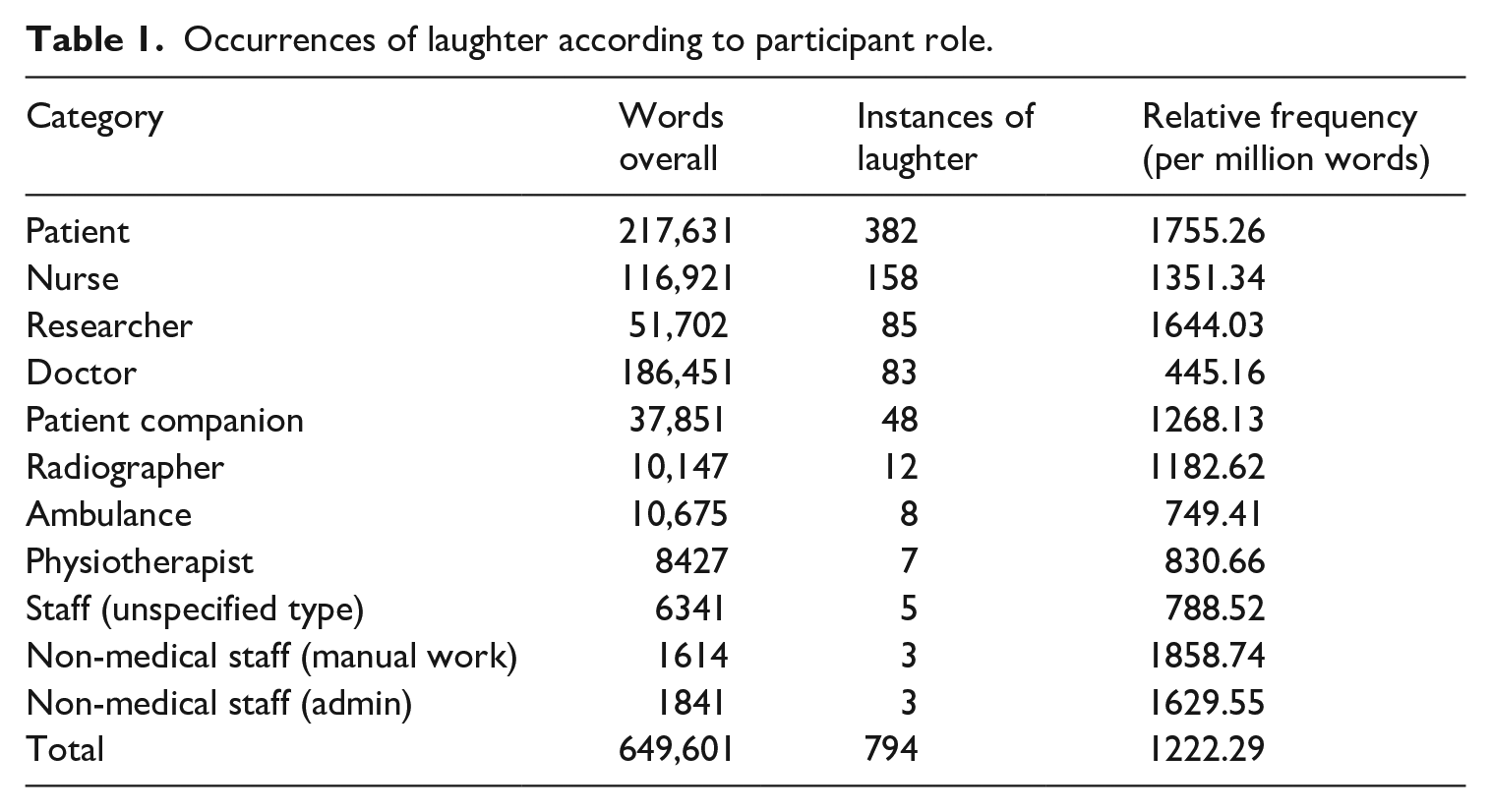
Table 1 shows that laughter was particularly prevalent in the contributions from nurses and patients, but was relatively infrequent in the speech of doctors. The relative frequencies are also high for participants from radiography, non-medical staff (manual work) and non-medical staff (admin). However, these are very few in terms of actual (raw) occurrences. Verbal contributions from the researchers – in which they explained their presence in the ED, sought consent from participants, and occasionally interacted with interlocutors in other ways – are excluded from our investigation, since these were deemed not to represent ‘typical ED talk’.
Identifying cases for qualitative analysis over time
As mentioned earlier, the EDCOM corpus comprises patient journeys which include all the interactions the patient had with staff, in addition to ethnographic notes about the activities and the goings-on around the patient (e.g. problems with the X-ray machine, chatting in the walkway). Two patient journeys were selected as case studies for a closer, temporal examination of the interactions surrounding instances of laughter. The selection of cases was based on the frequency analysis using (1) a minimum raw frequency of 20 laughter instances, and of those cases, (2) the two cases with the highest and lowest number of instances of patient laughter. These criteria ensure that we capture sufficient instances of laughter for analysis and that we analyse the interactions of patients who are more and less inclined to laugh in this context. Of the 72 patient journeys in the corpus, 48 included fewer than 20 instances of laughter; 8 of these contained laughter from staff but zero instances from patients. On average, over half (57%) of the instances of laugher were patient laughter specifically, but there was considerable variability in the extent to which individual patients laughed. Taking the 25 cases with at least 20 occurrences of laughter (see Table 2), we selected ‘Graydon’, who produced the lowest number of instances of laughter (2), and ‘Janet’, with the highest number of instances of laughter (38). Graydon (male) and Janet (female) are roughly comparable in terms of time spent in the ED (approximately 6 hours and 40 minutes), their linguistic and cultural backgrounds (English-speaking Anglo-Australian) and age (50s).
Occurrences of laughter per patient journey and individual patient.
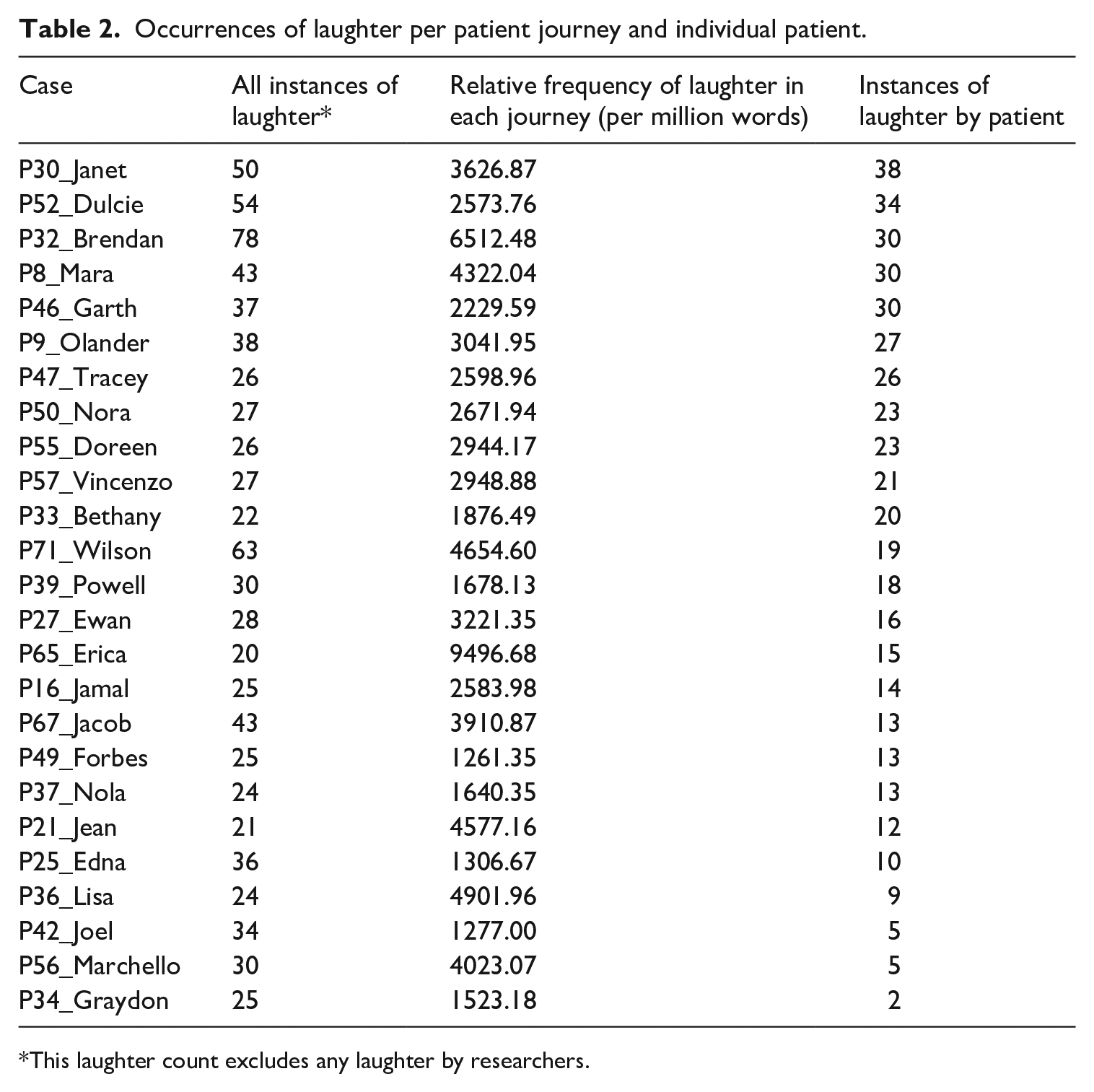
This laughter count excludes any laughter by researchers.
Stage 2 findings: Exploration of laughter in two patient journeys
We saw in Stage 1 that laughter occurred in the EDs and that it was frequently patients who did the laughing. In Stage 2, two patient journeys (Graydon and Janet) were analysed in detail to explore the individuals’ patterns of laughter and the role of laughter in the moment-by-moment unfolding interactional contexts – who laughed, when and why – in other words, looking around the laughter. The patient journeys offer a temporal dimension, allowing us to consider how, when and why a patient tends to laugh during their many hours in the ED. Thus, this analysis is concerned with the contextualised affective dynamics of the interactions in the ED timescale as indicated by instances of laughter as a signal of affect.
The analytic procedure aimed to identify and interpret the conversational episodes that are relevant to the laughter in the context of the specific patients and their ED experiences. First, laughter episodes, defined as the utterances surrounding the instance/s of laughter which appear to be relevant to the laughter, were identified. As Glenn and Holt (2013) observe, ‘laughter is indexical: when it occurs, people hear it as having a referent, pointing to something in the immediate environment, typically just preceding or concurrent’ (p. 3). Therefore, episodes typically span several turns produced by any participants who contributed to the topic development and include the referent that appears relevant to the laughter. Because the researchers were always recording from the patient’s close proximity, it can be assumed that the patient was either an interactant or a known audience. Laughter episodes mostly included the patient, but not always. Laughter episodes often contain more than one instance of laughter and more than one laugher, reflecting the often responsive or contagious nature of laughter.
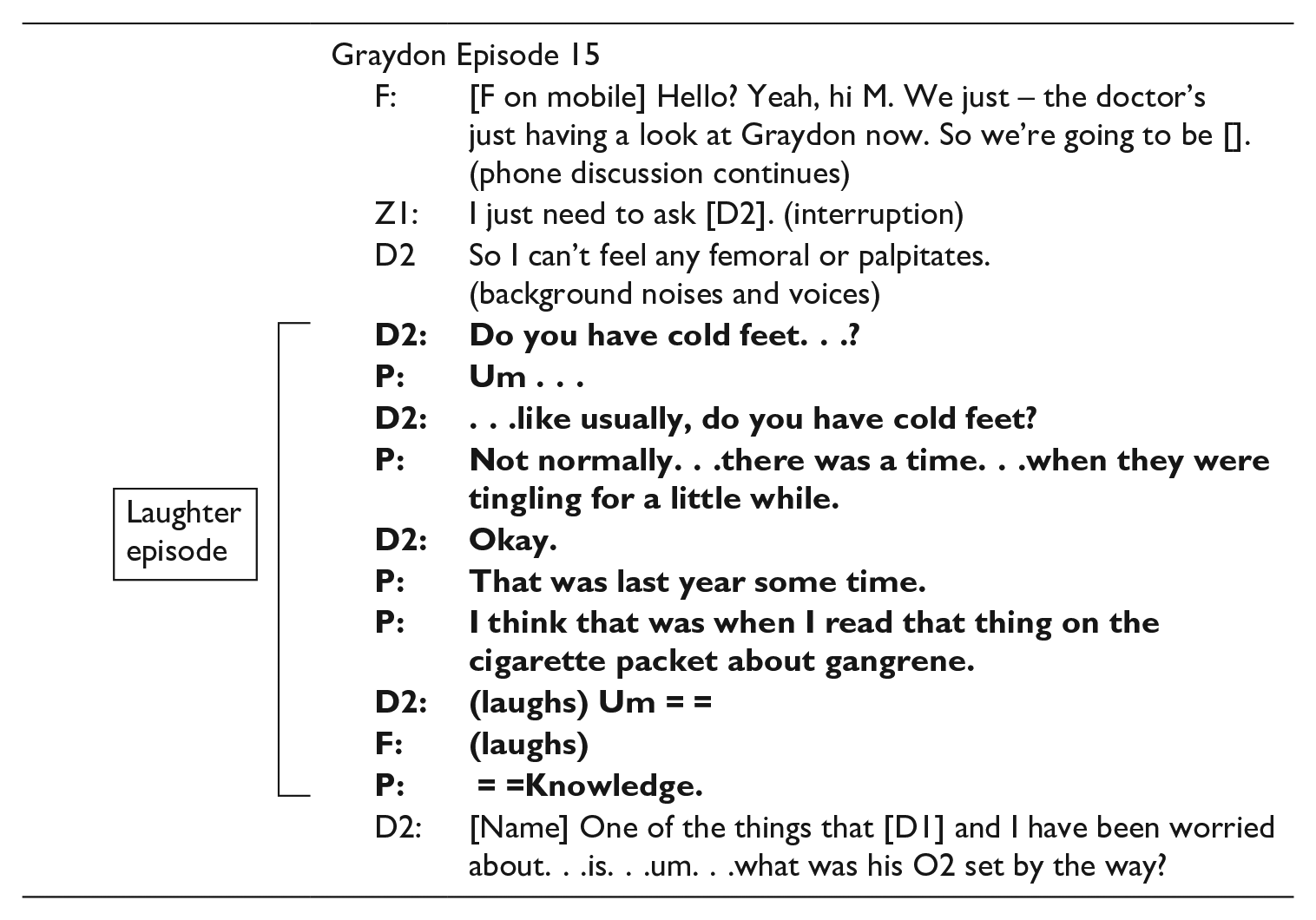
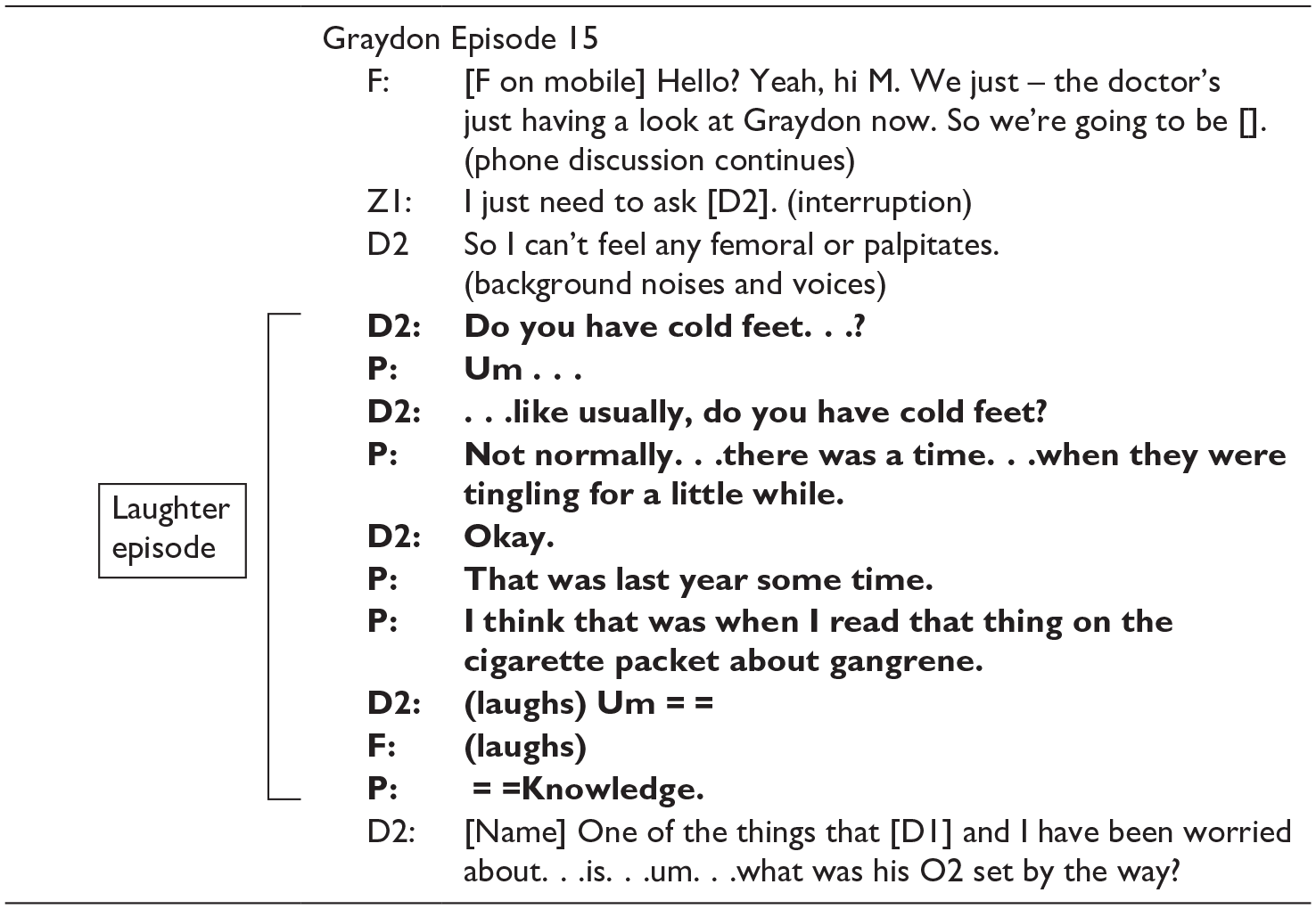
Second, laughter episodes were examined by two analysts separately and together in terms of (1) what appeared to be the referent of, or impetus for, the laughter in terms of topic and affect; and (2) the apparent broader function of the laughter within the institutional discourse of the ED. An example is provided below (Graydon’s Episode 15). The shaded line indicates the referent of the laughter, which was Graydon’s utterance, an example of incongruous humour: ‘I think that was when I read that thing on the cigarette packet about gangrene’. This elicited laughter from both the doctor (D2) and the patient’s wife (F). The turns shown in bold demonstrate the boundaries of the laughter episode, from the initial ideational point (‘Do you have cold feet?’) that develops into the interpersonal conditions in which the laughter referent arises, until the affective dynamic changes and/or the topic shifts. In this case, the episode appears to close when the doctor introduces a serious new topic (‘One of the things that [Doctor 1] and I have been worried about is. . .’). In this episode, the humorous referent and the laughter create an opportunity for a mutual, non-serious focus, as discussed below.
Each patient journey was examined for patterns in relation to topics and interactants, for example topics that tended to co-occur with laughter for each patient. These patterns were contextualised in light of other relevant information in the transcripts, such as the time spent in the ED.
Focus journey 1: Graydon
Graydon presented at the ED with heart failure, having already visited the ED the day before. He was accompanied by his wife. The observation notes indicated that the ED was particularly noisy that afternoon with many interruptions. Graydon encountered 21 different staff members throughout his stay. During this time, there were 17 laughter episodes across the 6 hours 45 minutes he was in the ED, many of which also involved his wife, in addition to eight staff members. Graydon laughs in only 2 of the 17 laughter episodes (12%).
Discussing serious topics
In the example of laughter in Episode 3 below, which occurred early in his journey, Graydon’s laughter appears to punctuate serious information during history-taking with his first Doctor 1 (D1), a male resident.

Having his final cigarette in the carpark outside the hospital was clearly a very significant personal event: later, it was revealed that Graydon had smoked for 33 years and currently smoked around 25 cigarettes a day. His affirmative response ‘I do’ indicates that he still considers himself to be a smoker, and his use of ‘apparently’ suggests that the idea of quitting (‘I had my last cigarette’) has an unreal quality at this early stage. His laughter appears to make light of the personal significance of quitting in the face of a serious medical emergency. In Episode 15 above, he elicits laughter from the second doctor (D2), a senior staff specialist and Graydon’s wife (F) with an incongruous treatment of the effects of smoking and the experience of ‘tingling feet’. Graydon’s laughter (Episode 3) and humorous treatment (Episode 15) of the topic of his smoking may be an indication of his awareness of the relevance of smoking to his current condition, and the significance of quitting a life-long addiction. At the same time, his ironic treatment of having ‘knowledge’ about the relationship between gangrene and smoking demonstrates that he is well aware of the health risks of his habit and their current relevance. This episode is the second time Graydon has described his tingling feet, having previously recounted it, unhumorously, to a junior doctor who had also asked if he got cold feet. At that time, Graydon asked the doctor about the relevance of tingly feet to his heart condition (‘Would that be the direct result of my heart not working too efficiently?’) and was given an extensive explanation about blood flow. Perhaps, in this later iteration of the question, Graydon feels adequately informed and focuses instead on lightening the emotional load of his condition.
The history-taking also reveals that Graydon is a regular drinker who has recently had a period of heavy drinking following the death of his brother. At this point, he reported another significant personal step: ‘I haven’t had a drink for a week now [. . .] and I’m not climbing the walls so it’s good’. Here, he uses metaphorical exaggeration (‘not climbing the walls’) which may concomitantly place his actual physical response in perspective, downgrading it. It is followed with a laughter sequence (bolded) in which Graydon and his wife (‘F’) cooperatively lighten the burden of this serious topic in Episode 4:
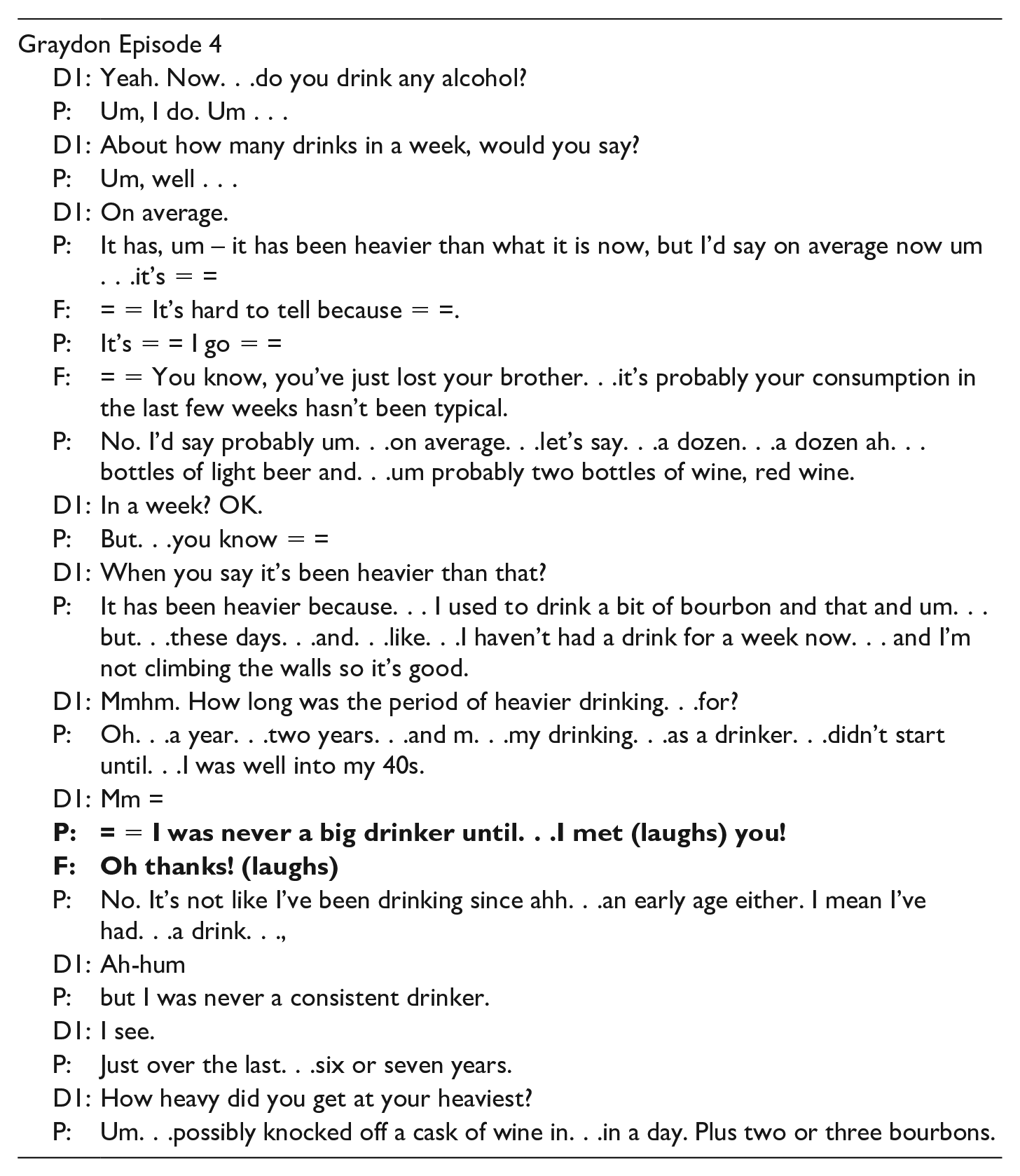
In Episode 4, Graydon’s humorous tease and laughter, and his wife’s responding sarcasm and laughter appear to ease tension during the history-taking in which Graydon and his wife collaboratively describe and explain his history of drinking to the doctor (‘D1’), including a recent heavy-drinking period which followed the death of his brother. Graydon’s wife contributes to the history-taking by offering an explanation for his drinking and the difficulty of coming up with an average weekly consumption figure: ‘You know, you’ve just lost your brother. . .it’s probably your consumption in the last few weeks hasn’t been typical’. The tease occurs 16 turns after the topic of drinking was raised and is part of Graydon and his wife’s pattern of collaborative talk within the institutional activities (history-taking, diagnosis delivery, etc.). As can be seen in Episode 4, Graydon’s tease is obviously not congruent with the surrounding history-taking, either in terms of addressee (his wife) or institutional register. By initiating teasing in this context, Graydon is using a style more typical of casual conversation, which inserts informality into the institutionalised medical domain (a ‘register play’, see Partington, 2017: 326). His brief resetting of the conversational context through the ‘contextualisation cue’ (Gumperz, 1992) of a tease and laughter may have been a call for support from his wife or, at least a means of gaining time-out from dealing with the increasingly sensitive, unfolding disclosure. The laughter is immediately followed with a description of his heaviest consumption. In terms of broader patterns across all his interactions, it is only in relation to these two serious matters – his drinking and smoking – that Graydon himself laughs.
Co-constructing humour
Laughter also signalled the presence of humour that served to build rapport and empathy by acknowledging and validating the patient’s experience and concerns. In Episode 16 below, more than 6 hours into his ED visit, the nurse (N3) has brought Graydon a sandwich but he is not sure if he is allowed eat it, despite being very hungry and arriving at the hospital having ‘missed lunch’.
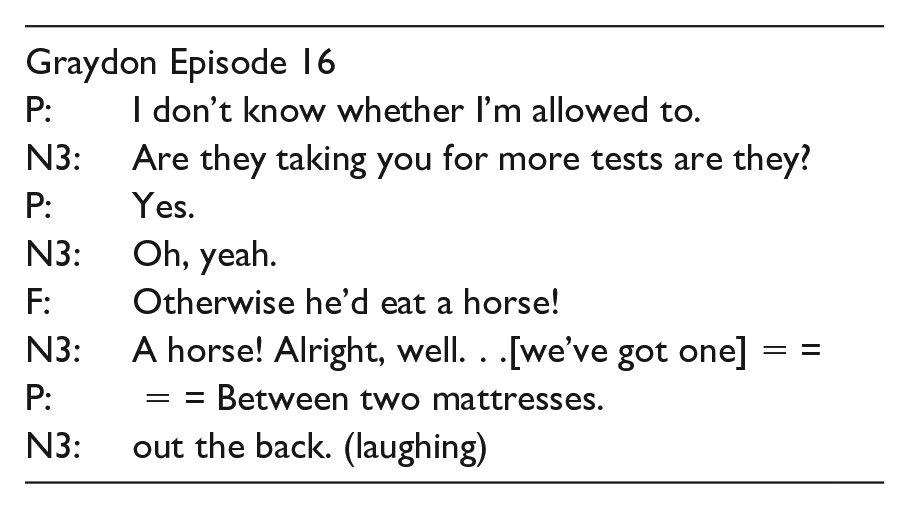
In this sequence, Graydon, his wife and the nurse collaboratively play with the literal meaning of the English idiom ‘so hungry he could eat a horse’. The scenario is jointly constructed: images of an actual horse ‘out the back’ (from the nurse) ‘between two mattresses’ (from Graydon) are based on a shared idiom (from Graydon’s wife). The verbal play in this incongruous scenario shows a high level of ‘mutuality’ – a dynamic process involving ‘a feeling of intimacy, connection, understanding of another’ (Henson, 1997: 79). Such a degree of collaboration may be an indication of how much their interactional and care relationship had evolved over the time (this episode starts this nurse’s 68th interaction with Graydon and his wife). Henson (1997) explains that mutuality is ‘not necessarily equivalent but is a mutating, changing, synchronous pattern of give and take which facilitates the movement toward a shared purpose’ (p. 79). Indeed, the humour may also serve to reduce the face threat to the nurse, as the institutional representative, who has to concede that, despite being very hungry, Graydon is correct in suggesting that he cannot eat the sandwich she has brought him. Thus, all three interactants are carrying out communicative ‘work’ in their institutional roles towards the goal of effective physical and psychological care.
Focus journey 2: Janet
In contrast to Graydon, Janet produced the highest number of laughter occurrences (38), which occur in 30 of the 35 laughter episodes (86%) we identified across the 6 hours and 41 minutes she was in the ED. She presented with stomach pain and was accompanied by her husband. She encountered 12 different staff members during her visit, 4 of whom are noted as laughing in the transcript.
Being a patient
Janet’s laughter episodes are notable in that they signal her extensive efforts to generate jocularity. Janet used self-deprecating humour, punctuated by laughter, on several occasions to frame the fact that she had not sought help for her stomach pain despite experiencing it intermittently for 12 years. This is exemplified in Episode 1 with the triage nurse (N1):
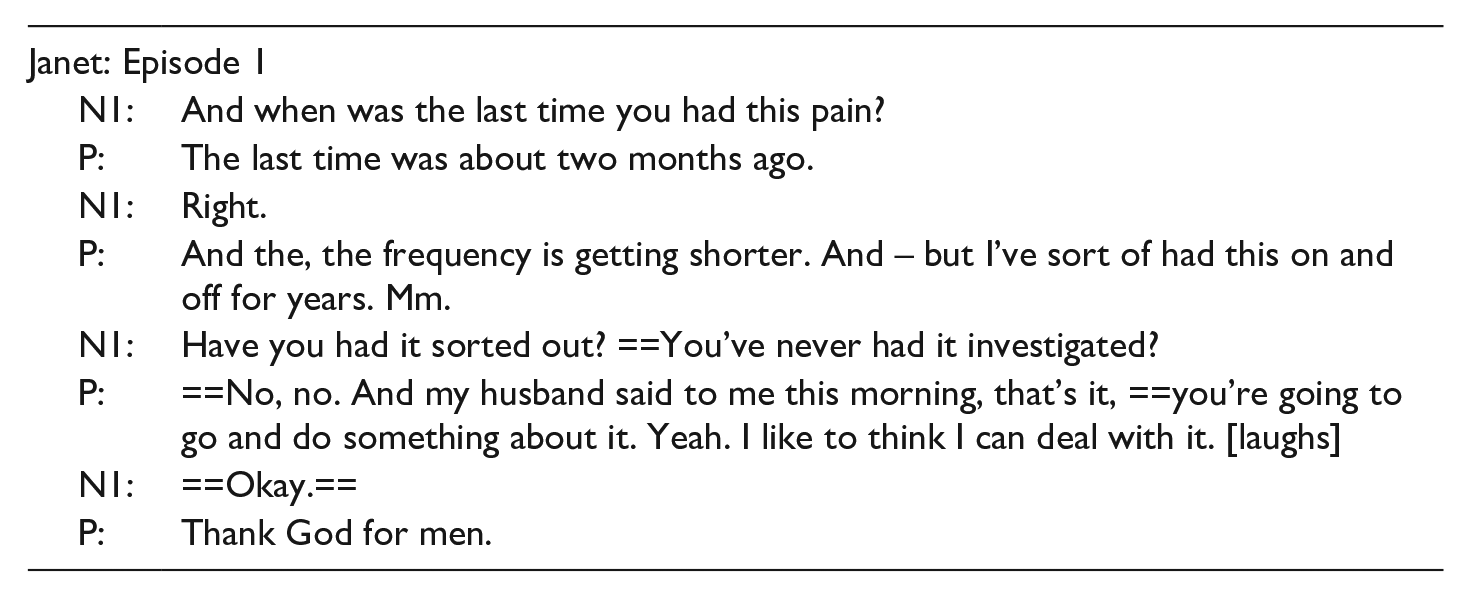
In Episode 1, two aspects of Janet’s identity appear to become salient upon her entry to the new hospital context (the triage process): being a non-patient (‘I like to think I can deal with it [laughs]’) and being female (‘Thank God for men’). Even at this early stage, she uses self-deprecation, marked by laughter to assert her non-patient identity in the institutional context. The nurse’s questions (‘Have you had it sorted out? You’ve never had it investigated?’) may have heightened her sense of inadequacy. Several turns later, the same triage nurse validates Janet’s feelings of fear in relation to seeking medical attention, offering personal empathy:
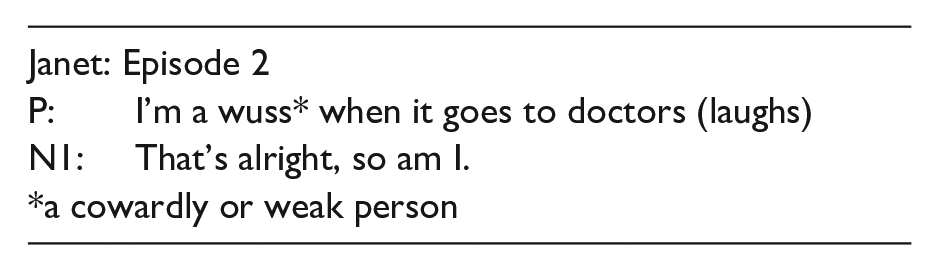
The triage nurse’s validation occurs just after Janet has detailed the extent and dynamics of her recent and regular pain patterns. She notes that is it ‘recurring’, having ‘had it on and off for years’. Here, she uses the colloquial phrase ‘a wuss’ to disclose her weakness or fear. N1’s response shows mutuality by making the same ‘wuss’ disclosure. Through laughter cues, Janet made light of the fact that she does not tend to seek medical help in six laughter episodes (e.g. ‘you’re the first doctor I’ve seen for a few years. [laughs]’). She explained to the doctor that she ‘usually waited it out and it’s fixed itself’ and that she is ‘very fortunate’ with her health, among other mentions of general wellness. Her pattern of signalling her new patient status with laughter may be an indication of her discomfort with the role, and chimes with her admission of fear in Episode 2.
The general prevalence of laughter (35 laughter episodes) in Janet’s journey is explained by her stated approach to managing the doctor-patient relationship: ‘it’s up to me and make him welcome [. . .] I’m actually asking him for his help, I need to let him know that it’s okay, he can touch me and things’ (in conversation with the researcher). She also expressed a desire not to impose, which prevented her from asking for help: ‘Why didn’t I ask? That’s me isn’t it, I just don’t want to uh – I don’t know, impose on them I suppose’. These beliefs resonate with the fact that Janet did not to seek medical attention until told to by her husband, and with her repeated attempts to de-institutionalise the context by recruiting the doctor into her humour frame, such as in Episode 15:
This incongruous wordplay on ‘run’ occurs just after the doctor has completed a physical examination of her abdomen area. It appears as a humour invitation to the doctor, who does not take up the humour in an explicit manner. This pattern of humour invitation (Janet) and decline (doctor) occurred in all 17 laughter episodes involving them both, and demonstrates the very limited mutuality between them.
Co-constructing humour
In contrast to her interactions with the doctor, Janet’s interactions with Nurse 3 1 were notable for their bouts of co-constructed humour signalled by shared laughter, as can be seen in their first encounter with Nurse 3 who had just come in to take a blood sample:
This episode involves playing with a shared idea (only thinking to repair windscreen wipers when it is raining). This discursive play emerges from Janet’s self-deprecating theme of being a non-patient who seeks attention too late (‘it’s always usually after the fact when you get to the doctor, isn’t it?’). The nurse responds to Janet’s call for support with an exaggeration about child patients (‘you bring them in to hospital and they’re miraculously absolutely wonderful’) which doesn’t appear to align completely with Janet’s situation. Nonetheless, the humour frame is safely established, and Janet introduces incongruity via an analogy with windscreen wipers which both interactants subsequently improvise on with theatrical intertextual borrowings (‘Hey, I’m off to get those wipers!’) and syntactic completions (‘or the water in my wipers’). The episode culminates in Janet’s near-tease about their joint humour (‘Oh, we’re funny aren’t we?’). The collaborative elaboration demonstrates a high level of mutuality, with both nurse and patient verbally playing on the topic of only thinking to fix something when it is most needed. It occurs at the same time, or immediately prior to the taking of blood and may also serve to distract the patient from the potential unpleasantness of the immediate task, as well as Janet’s more general discomfort with being a patient.
Discussion
In this mixed-methods investigation of laughter in Australian EDs, a number of previous findings are corroborated and interesting patterns arise. Patients laugh relatively often compared to staff, echoing other studies that have found that patients tend to laugh more than doctors (Haakana, 2002; West, 1984). This finding may reflect the fact that laughter which marks sensitive matters is not always intended or appropriate for responsive laughter (Beach and Prickett, 2017). This is not to say that ED doctors did not respond empathically, but the laughter distribution suggests that they do not always join in with laughter. The laughter distributions also show that nurses laugh more than doctors. As nursing remains a gendered profession (Australian Government Department of Health, 2017), the higher distribution of laughter from nurses may reflect the more general finding that women tend to laugh more than men (Provine, 1993; Provine and Emmorey, 2006). In clinical contexts, the patients of female physicians have been found to use more humour than those of male physicians (Sala et al., 2002), though same-sex pairings also appear more amenable than mixed-sex pairings to the elicitation of laughter through humour (Phillips et al., 2018; Roter et al., 1999). However, nursing duties are distinctive; tuning into patients’ laughter and humour invitations may be a regular part of a nurse’s therapeutic toolkit. Indeed, it was interactions with female nurses in the two patient journeys that displayed the most laughter and collaborative humour, despite the fact that the two patients under focus exhibited very different propensities to laughter. Nurses may have a wider scope of discourse relations available to them, between displaying power and showing solidarity which allow them to engage in verbal play more freely (Grainger, 2004: 40).
A broader question arising from these findings is why there is so much laughter, particularly that of patients and their companions, when a visit to the ED would be a bad day for most people. Glenn and Holt (2013) observe that laughter is versatile: ‘moving between polarities of serious and not serious, hostile and affiliative, self- and other-referential’ (p. 2). Using the patient journey as a contextual narrative affords us a unique view of the function of laughter as an ‘affect key’ for concomitant affective dynamics in the unfolding interaction (Ochs and Schieffelin, 1989: 15). Instances of laughter are just one, embodied component of co-constructed gestalt ‘emotional displays’ which we glimpsed in the laughter episodes (Ruusuvuori, 2013: 331). A useful analytic concept is Wetherell’s notion of affective practice, which refers to the emotional imbuement of ordinary social activities. ‘Affective practice’ encompasses the ‘rules’ of how one should feel (e.g. brave in the face of illness) as well as the ‘atmosphere’ compelling an emotional response (e.g. the vibe of a busy ED) (Wetherell, 2013: 237). As Wetherell (2013) writes, ‘people adjust their affective conduct moment to moment, moving in and out of a sense of the self and the body as object, and as acting subject’ (p. 226).
Given that the affect key of laughter is prevalent in patient talk, and that both laughter and humour appear to help patients manage difficult topics and changes to identity, it is worth considering how these affective resources might foster patient-centred relationships in clinical interactions. A key component is the development of mutuality, which is considered a cornerstone of genuine shared decision-making and patient participation in their own care (e.g. Conger, 2011). Mutuality can be considered a therapeutic version of affective practice. As mentioned earlier, mutuality is a sense of joint understanding and connection between people engaged in a common purpose (Henson, 1997). In health care, mutuality is ‘shaped by power relations, by culture, custom and practice’ (Brown, 2016: 1473), and, we would add, linguistic repertoire. As we have seen, mutuality can be strongly present in some moments with some interactants, and not evident at all in others. A key point is that laughter, as with affect more generally, can be more controlled and therefore agentic, or more uncontrolled and impulsive (Wetherell, 2013; Wild et al., 2003). The laughter episodes in the case studies provide evidence that different institutional roles (patients, patient companions, clinicians) can actively work on achieving mutuality through displaying affect, as well as benefit from and contribute to the mutuality efforts of others.
In the two patient journeys we analysed, laughter appeared to smooth over difficult admissions and adaptations; as Scott et al. (2014) suggest, ‘helping to “de-escalate” negative emotional experience, with a positive role in both the short-term affective state of the interaction and in the longer-term state of relationships’ (p. 620). Graydon’s only laughter accompanied his statements about smoking and drinking indicating the significance, and possibly discomfort, of his new identity as a non-smoker and non-drinker. Janet, who had never sought medical attention for her 12-year recurring pain, used laughter alongside her repeated statements about being a healthy non-patient to display wellness, perhaps allaying her discomfort about her new identity as a patient and having to impose on others (for other examples of ‘wellness stances’, see Beach and Prickett, 2017: 798). Although their personal propensities to laughter and their humour strategies were very different, both patients managed to create opportunities for others to show their validation and support. Janet constantly attempted to recruit the doctor into her humour (to no avail) to promote a level of mutuality that would enable him to provide the best care. As Janet put it, she agentively works with people’s ‘energies’ to make them feel okay about helping her. Thus, her laughter cues and use of humour are not necessarily an unconscious response to difficult circumstances, but rather, they are deployed deliberately, for example, to reduce the face-threat involved in medical procedures (see also Ragan, 1990). Lindquist (2013) proposes that our ‘ability to construct emotion’ may be one of our ‘most adaptive traits’ (p. 364). The patients’ efforts to adapt to their new identities, marked by their displays of laughter and humour, show how the construction of emotion might be, at least partly, scaffolded through semiotic means in interpersonal interaction.
While the doctor repeatedly declined Janet’s humour invitations, there were many examples of collaborative laughter episodes between patients, family members and staff. Clinicians and patients worked creatively and collaboratively on humour sequences signalled by laughter with the ideational content (e.g. elaborating on literal interpretations of a known idiom) and structural content (e.g. completing each other’s syntax) distributed between people and across turns. Co-construction of humour occurred as participants played with shared metaphors and analogies imported from non-institutional discourse; the ‘eat a horse’ episode (Graydon is hungry but can’t eat) and the ‘windscreen wipers’ episode (Janet should have sought medical help earlier). In each case, the serious interpretation relates to the patient’s actual physical and psychosocial state. Choosing to play with non-serious figurative meanings, then, is concurrently an acknowledgement of the seriousness of the alternative interpretation and a means to de-escalate that seriousness. Such verbal play is both a means of bonding and soothing, as well as a potential risk in the context of asymmetrical institutional power (Grainger, 2004), reflecting the fact that mutuality does not presume equality, though it may enable power relations to be questioned (Brown, 2016).
In the patient journeys, laughter occurred in the context of difficult topics as well as with different humour strategies (e.g. wordplay, metaphor, exaggeration, teasing, self-deprecation) at the level of the utterance and surrounding turns. In theory, strategies might be any type of conversational humour (e.g. those listed in Dynel, 2009) that is within the shared communicative repertoires of the interactants. As demonstrated in the case studies above, these strategies can be mobilised, often collaboratively, to serve therapeutic functions in the broader institutional context, such as easing stress, building rapport, showing empathy and alleviating discomfort. Arguably, these functions are not all ends in themselves; they serve care goals which are core needs or intended actions that motivate the uses of laughter, humour and other interactional resources, such as the obvious goal of a desire for effective care or, a less obvious one such as the need to adapt to an uncomfortable new identity.
The episodes in the two patient journeys demonstrate just a few of the ways in which laughter, humour strategies, therapeutic functions and care goals might be configured in interactions in the ED context. However, there are myriad possibilities for how laughter, humour strategies, functions and goals might occur in the ever-unfolding discursive dynamics of relationships, personalities, physical needs and institutional roles and processes. Recent theorising in affective science has reconceptualised emotions as dynamic, contextualised ensembles of signals within the brain, the body, the immediate environment and broader culture (Barrett, 2022). This chimes with the notion that emotions are dynamically constructed through ‘situated practices lodged within specific sequential positions in interaction’ (Goodwin and Goodwin, 2000: 33). As Pratt (2023) suggests, ‘a more thorough consideration of affect can deepen our understanding of meaning making as it occurs in everyday interaction in institutional settings’ (p. 1).
Conclusion
This study has explored the interactional dynamics of ‘emoting’ (Mesquita, 2010: 91), as indicated by laughter, as an affective signal, in the interactions of staff, patients and their support people in EDs. A bird’s-eye view of the spread, frequency and producers of laughter in the interactions revealed that laughter occurs across all participant roles (e.g. doctors, ambulance officers) in the ED setting, but is especially prevalent in the interactions of patients and nurses. Case studies of the interactions of two patients who demonstrate contrasting frequencies for laughter, showed how laughter often co-occurs with humour to serve a range of interpersonal functions in adapting to and dealing with the patients’ conditions and the affective demands of the ED contexts. In the patient journeys, micro-level emotional displays involve, amongst other things, laughter, various humour strategies and topics which are often derived from the patients’ serious physical circumstances (e.g. intermittent pain, heavy smoking). This assemblage of semiotic, psychosocial and physical components is woven into institutional hierarchies, timescales and procedures: for example, waiting for test results, working out the staff roles and interpersonal styles, remembering and providing a coherent medical history. A practical implication of these findings is that a sensitive responsiveness to patient-initiated laughter and humour may enhance mutuality as a basis for compassionate, patient-centred relationships in clinical interactions.
Footnotes
Appendix A: Transcript conventions
We have transcribed clinician–patient interactions using standard English spelling. Nonstandard spellings are occasionally used to capture idiosyncratic or dialectal pronunciations (e.g. gonna). Fillers and hesitation markers are transcribed as they are spoken, using the standard English variants, Ah, uh huh, hmm, mmm.
What people say is transcribed without any standardisation or editing. Nonstandard usage is not corrected but transcribed as it was said (e.g. me feet are frozen).
Most punctuation marks have the same meaning as in standard written English. Those with special meaning are: . . . indicates a trailing off or short hesitation. == means overlapping or simultaneous talk [. . .] — indicates a speaker rephrasing or reworking their contribution, often involving repetition [. . .] [words in square brackets] are contextual information or information suppressed for privacy reasons. Examples: [Loud voices in close proximity] contextual information Z1 And your mobile number I’ve got [number]. (words in parentheses) were unclear but this is the transcriber’s best analysis. ( ) empty parentheses indicate that the transcriber could not hear or guess what was said [. . .]
(Slade et al., 2015: xi).
Acknowledgements
We would like to acknowledge the contributions of the Communicating in Hospital Emergency Departments research team: Diana Slade, Marie Manidis, Jeannette McGregor, Hermine Scheeres, Eloise Chandler, Jane Stein-Parbury, Roger Dunston, Maria Herke and Christian M.I.M. Matthiessen for the data collection and transcription which constitutes the EDCOM corpora as well as their insightful analyses (see Slade et al., 2015).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The original research project was funded by the Australian Research Council (grant number LP0775435). The contributions by Gavin Brookes, Luke Collins and Elena Semino were funded by the Economic and Social Research Council, part of UK Research and Innovation (grant number ES/R008906/1).