
Abstract
In recent years, digital health care and social welfare services have been spreading rapidly and partly replacing face-to-face services, particularly in developed countries. This may lead to a pronounced digital inequality. This population-based study of Finnish adults (N = 4495) examined the associations of offline resources with perceived benefits from online services and the mediating effects of access, skills and attitudes in these associations. The results indicated that those with lower personal, economic and social offline resources perceived online services as less beneficial. This was largely explained by poor access to the services, poor digital skills and negative attitudes towards online services. To increase equality, it would be important to improve Internet access and digital skills and implement means to address negative attitudes, especially among vulnerable groups. Moreover, online health and social welfare services should be designed to be more inclusive.
Keywords
Introduction
Digital health care and social welfare services are increasing rapidly, particularly in developed countries. The COVID-19 pandemic in particular has given an unprecedented boost to the digitalization of these services. Apart from saving unnecessary face-to-face visits, digital services support self-management and self-service of health and wellbeing, requiring a more capable and active role among clients. Digital risk tests and health form-based analytics have also been established as gatekeepers to more traditional services. However, people do not have equal possibilities to use these services and take more responsibility for their health. Especially those who have high needs for health care and social welfare services are at risk of having difficulties in adopting and adapting to digital services. This deepens the existing inequalities in society.
Social and digital exclusion are closely intertwined: differential access to information technologies affects socioeconomic stratification or inclusion, and vice versa (Warschauer, 2004). Thus, a vicious cycle may emerge where social exclusion leads to digital exclusion, which in turn contributes to deeper social inequalities (Warschauer, 2004). This interaction is also reflected in the resources and appropriation theory (van Dijk, 2005). The theory proposes that inequalities in society are linked to an unequal distribution of resources, which may cause unequal access to the Internet. The theory suggests that differences in access reinforce inequalities of participation in society, which in turn leads to greater overall social inequalities. However, as the Internet has diversified and diffused widely over the past 10 years, it can be assumed that Internet non-use is currently far more common among vulnerable groups, and that a lack of access has become a less important reason for Internet non-use than a lack of skills (van Deursen and Helsper, 2015).
According to the diffusion of innovations theory (Rogers, 1986), some people adopt new technologies and develop competence more easily than others, which enforces the gap between advanced users and those who adapt to new technologies more slowly and are limited in their skills. Because digital skills are thought to be cumulative by their nature, this may result in a situation where those who are more competent in selecting and processing information will outpace those who possess only basic skills (van Dijk, 1999). Correspondingly, the knowledge gap hypothesis (Gaziano and Gaziano, 1996) suggests that people in a higher socioeconomic position acquire and master information streams in society more rapidly than those in a lower position. This leads to knowledge gaps in society. Moreover, there is a risk that those who are less connected also give up on having influence in society. This leads to inequality, where those who have many resources to utilize information and communication technology (ICT) become the influencers and negotiators in society, whereas those with fewer resources are more likely to be excluded from opportunities to influence (Castells, 2000).
Helsper’s corresponding fields model
Helsper’s (2012) corresponding fields model suggests that digital and social exclusion influence one another and that a person’s offline resources influence the resources to use digital online solutions as well. The model proposes four fields (i.e. domains) of offline resources – economic, cultural, social and personal – which are assumed to be linked most strongly to corresponding fields of digital resources. The lack of offline economic resources related to exclusion includes poverty, joblessness and low education. Indicators of cultural offline resources comprise gender, generational, ethnic and religious affiliation. Social resources include participation in societal activities and involvement in social networks. Personal resources include psychological and physical health and wellbeing. The corresponding fields model predicts that a lack of offline resources in one field will lead to a disadvantage in the corresponding digital field, and vice versa. Thus, the model suggests that the links between corresponding fields are stronger than between non-corresponding fields. However, the fields of offline and digital exclusion are assumed to be related to each other, and a person excluded from one field is supposed to be likely excluded from another.
The model characterizes access, skills and attitudes as important social impact mediators in this context. That is, they are seen as barriers and enablers in the relationship between the offline fields of exclusion and the digital fields of exclusion (but not between the opposite relationships). The Internet or other ICT cannot be used without access, which makes access the most basic mediator between the offline and digital fields of exclusion. Similarly, certain skills on a basic technical and operational level are required for the handling of ICT and the Internet. Attitudes about the usefulness, appropriateness and dangers of ICT may encourage or impede its use.
This theoretical model merits dealing with the complexities of the links between social and digital exclusion. The model differentiates from other related models in that it views access, skills and attitudes as enablers or barriers, that is, they mediate the influence of offline social exclusion fields on digital fields, whereas other models usually view these factors as indicators of digital exclusion.
The concept of the digital divide
Digital inequality is closely related to the concept of the digital divide. The terminology and concepts related to the digital divide and its determinants are vague and not properly defined (Scheerder et al., 2017). The actual origin of the concept of the digital divide is ambiguous, but it was introduced by the US Department of Commerce’s National Telecommunications and Information Administration in the late 1990s (NTIA, 1999). They referred to the digital divide as the gap between those who have access to new forms of information technology and those who do not (NTIA, 1999). Castells (2002) has defined the digital divide as inequalities in access to and use of ICT, such as the Internet. Access can narrowly be seen as referring to physical access or (more recently) as widely reflecting motivational, physical, skills and usage access (van Dijk, 2006). The term ‘digital divide’ has been criticized as being originally equivocal, irreducibly plural and constantly flexible (Gunkel, 2003).
The digital divide can be seen to include at least three levels (van Deursen and Helsper, 2015). The first-level digital divide refers to many types of infrastructural access, such as having an Internet connection (van Deursen and van Dijk, 2019). The second level has to do with differences in skills and usage patterns (Hargittai, 2002). The third level refers to disparities in the outcomes of Internet use, thus relating to differences in the ability to transform Internet access and its use into advantageous offline benefits (van Deursen and Helsper, 2015; Wei et al., 2011). The concept of the third-level digital divide is particularly relevant in the current study because we focus on the perceived benefits from online services.
Determinants of digital inequality
There is a risk that digital exclusion might affect the poorest and most marginalized groups already from the outset (Castells, 2001). One reason for this can be that the Internet strengthens already existing social inequalities (Helsper and Reisdorf, 2015). Indeed, key determinants of digital inequality have been found to originate from socio-demographic, economic and geographic factors (Taipale, 2013).
Regarding the economic domain, several studies show that the lack of economic resources is associated with digital inequality. The less educated and the unemployed are generally less likely to use the Internet and computers (Creschi et al., 2010; Helsper and Reisdorf, 2015). Low education has also been associated with poorer skills to use the Internet for health-related information and services (van Deursen and van Dijk, 2011). Moreover, the less educated are more likely to experience computer anxiety (Yoon et al., 2016).
In terms of economic factors and receiving benefits from the Internet, those with higher education and higher income have been reported to benefit more from the Internet (Blank and Lutz, 2016; van Deursen and Helsper, 2015). In contrast, poverty and a low level of education have been associated with lower levels of perceived benefits from online services, although the association of education with benefits was at least partly explained by differences in access, skills and the extent of use (Heponiemi et al., 2020). However, findings also show that economically disadvantaged groups may benefit from the Internet. For example, the Internet may offer benefits in a job search for those unemployed (Fieseler et al., 2014).
As for personal and social resources, previous evidence supports the hypothesis that fewer personal and social resources are a risk for digital inequality. Older age, poor self-assessed health, hospitalization and disability have been associated with lower computer and Internet use, whereas membership in leisure-time organizations and participation in voluntary work has been associated with higher use (Creschi et al., 2010; Helsper and Reisdorf, 2015). Elderly people have been found to benefit less from Internet use than young people (van Deursen and Helsper, 2015), but the opposite finding also exists (Blank and Lutz, 2016). A recent study showed that those with low health literacy and physical health problems are less likely to benefit from the Internet in the COVID-19 crisis (van Deursen, 2020). However, the opposite finding also exists. For example, it has been shown that people with disabilities in the United States were more engaged with the Internet during the first weeks of the COVID-19 epidemic than people without disabilities (Dobransky and Hargittai, 2021). Living without a partner and low social participation have been associated with fewer perceived benefits from the Internet and online services (Heponiemi et al., 2020).
The present study
It has been suggested that research should focus more on the outcomes of digital technology use, such as the benefits of Internet use (Scheerder et al., 2017). Scheerder and colleagues have pointed out that research on social and cultural determinants of benefitting from Internet use needs more attention. Examining the digital inequalities regarding health care and social welfare services is especially urgent because of the rapid digitalization of these services and the risk that the groups that need these vital services the most are in danger of dropping out. Whereas previous research has identified some specific social determinants of digital inequality among the users of health care and social welfare services (Heponiemi et al., 2020), whether and to what extent access, skills and attitudes together explain (i.e. mediate) the effects of these determinants – as proposed in Helsper’s (2012) corresponding fields model – remains to be investigated. In contrast to many other theoretical models on digital inequalities that consider access, skills and attitudes as indicators of digital exclusion, the corresponding fields model regards them as mediators for the effects of offline resources. This means that they could be important targets for interventions that aim to mitigate inequalities in digital societies.
The present study examined the mediating effects of access, skills and attitudes in the association between offline resources and perceived benefits of online health care and social welfare services in the personal health-related, economic and social domains. More specifically, our research questions included whether access, skills and attitudes would act as mediators in the associations of (1) personal offline resources concerning health and wellbeing with corresponding perceived personal health-related benefits, (2) economic offline resources with corresponding perceived economic benefits and (3) social offline resources with corresponding perceived social benefits. In light of Helsper’s (2012) corresponding fields model, we hypothesized that access, skills and attitudes would act as mediators in the associations of corresponding offline resources with corresponding perceived benefits. Because low economic offline resources can be assumed to be particularly strongly associated with the mediators (van Deursen and van Dijk, 2019; van Deursen et al., 2019), we also expected that if mediation is present, the mediated effect would be largest in the economic domain.
Methods
Sample
The present sample included 10,000 people representative of the adult population (over 20 years of age) living in Finland. The sample was drawn from the registers of the Population Register Centre of Finland. The data gathering and questionnaire development have been reported previously (Hyppönen and Aalto, 2019). A double picking method was used for people 75 years old or older, which guaranteed a sufficient number of older respondents. The paper questionnaire was mailed to the sample in 2017 with three reminders to those who had not answered. Respondents also had the option to respond online, which was indicated in the paper form.
Altogether 4495 persons responded (56.8% women), corresponding to a response rate of 45%. The analyses of non-response showed that we received more responses from older respondents, women and those with higher education than from the eligible population (Hyppönen and Aalto, 2019). Therefore, we used an inverse probability weighting (IPW) correction based on age, gender, marital status, education level, region of residence and degree of urbanization of the residential municipality. Previous studies have shown that this is a sound method for adjusting possible non-response bias among the Finnish population (Härkänen et al., 2014).
Measurements
Perceived benefits (dependent variables)
The perceived benefits of online health care and social welfare services were measured in terms of perceived personal health-related (4 items, α = .90), economic (4 items, α = .90) and social benefits (3 items, α = .87). Example items include ‘Electronic services help people self-manage their health’ (personal health-related benefits), ‘Electronic services save time or money that making transactions in person would take’ (economic benefits) and ‘Electronic services support collaboration and information flow between the patient and the social and health personnel in charge of the person’s treatment’ (social benefits). All items were rated on a 5-point Likert-type scale ranging from 1 (completely agree) to 5 (completely disagree), with higher scores reflecting lower perceived benefits. For a full list of all items, see Supplementary Table 1.
Offline resources (independent variables)
Offline resources were measured in the personal health-related, economic and social domains. Composite (i.e. cumulative) score variables for resources in each domain were constructed as the total (sum) of four domain-specific indicator variables that reflected lower resources. The composite scores thus ranged from 0 to 4, with higher scores reflecting a lack of offline resources and the severity of offline resource deprivation. The indicators were selected based on available measures in the data and their relevance to the construct in question.
The indicators for personal health-related resources included self-assessed poor health, long-term illness, mental distress and obesity. Poor health was measured by asking how respondents would describe their current state of health (coded as 0 = good or fairly good; 1 = average or worse than average). Long-term illness was measured by asking whether the respondent had any long-term illness or health problem (0 = no; 1 = yes). Mental distress was measured using the five-item Mental Health Inventory (MHI-5; Stewart et al., 1988). An MHI-5 score of ⩽ 52 was used as the cut-off point for mental distress (0 = no distress; 1 = distress). Obesity (0 = no; 1 = yes) was measured as a body mass index (BMI) of 30 or above (standard for obesity), calculated based on self-reported weight (kg) and height (m), according to standard protocols.
The indicators for economic resources included unemployed status, low education and experienced financial hardship related to food and medical care. Unemployment was assessed with self-reported current labour market position (0 = currently working/old-age pension/disability pension/student/other; 1 = unemployed). Low education was measured using self-reported years of education, dichotomized into high and low using a median split (0 = higher education; 1 = lower education). Financial hardship related to food was measured by asking whether the respondent had worried about running out of food before getting money to buy more within the past 12 months (0 = no; 1 = yes). Financial hardship related to medical care was assessed by two items asking whether the respondent had (a) not been able to buy medicines for lack of money and (b) not been able to visit a doctor for lack of enough money during the past 12 months (0 = none; 1 = yes, to at least one of these two).
The indicators for social resources included social isolation, living alone, loneliness and political participation. Social isolation was measured by asking whether the respondent kept in contact with friends or relatives at least once a week (0 = yes; 1 = no). Living alone was measured by asking whether the respondent lived alone (0 = no; 1 = yes). Loneliness was measured by asking whether the respondent ever felt lonely (0 = sometimes or less often; 1 = fairly often or all the time). Political participation was measured by asking whether the respondent had voted in the most recent municipal elections (0 = yes; 1 = no).
Access, skills and attitudes (mediators)
We measured access (7 items, α = .83), skills to use (4 items, α = .87) and attitudes towards online health care and social welfare services (4 items, α = .82). The respondents were asked to rate statements about factors that make it impossible or difficult for them to use the online social and health care services. Example items include ‘I do not have a computer and Internet connection of my own’ (access), ‘I do not have sufficient technical skills to use the e-services’ (skills) and ‘Electronic services do not interest me’ (attitudes). All items were rated on a 5-point Likert-type scale ranging from 1 (completely agree) to 5 (completely disagree) and reverse coded so that higher scores reflected poorer access, poorer skills and more negative attitudes. For a full list of items, see Supplementary Table 1.
Analyses
The associations were examined using structural equation modelling (SEM) in Mplus version 7 (Muthén and Muthén, 2013). The mediators (skills, access and attitudes) and outcomes (perceived personal health-related, economic and social online benefits) were modelled as latent variables, whereas the predictors (personal health-related, economic and social offline resources) were modelled as manifest variables. First, missing data were imputed using the multiple imputation procedure in Mplus. The rate of missing values ranged from 8% (offline social resources) to 35% (online economic resources). For the analyses, ten imputed datasets were created.
Next, a measurement model was specified for each corresponding field domain to examine the associations between the latent constructs and their indicators. Then, multiple mediation structural models were fitted for each corresponding field domain to determine the extent to which access, skills and attitudes mediate the association between (1) personal health-related offline resources and personal perceived online health-related benefits, (2) economic offline resources and perceived economic online benefits and (3) social offline resources and perceived social online benefits. The different corresponding field domains were analysed separately because we wanted to avoid fitting an overly complex, difficult-to-interpret model with a high number of parameters and the potential problems associated with multicollinearity. An overly complex model with highly correlated variables could lead to misleading results or unattainable parameter estimates due to non-convergence (Deng et al., 2018). Indirect effects were tested using the product-of-coefficients approach with the model constraint command in Mplus. The product-of-coefficients approach is suitable for testing mediation in large samples (Koopman et al., 2014; Preacher and Hayes, 2008). Age and gender were included as covariates in all models. To correct for different sampling probabilities, all analyses were conducted using sampling weights.
Model fit was assessed using the comparative fit index (CFI), the Tucker–Lewis index (TLI) and root mean square error of approximation (RMSEA). Following current conventions, acceptable model fit was defined by the following criteria: a CFI and a TLI value of ≧.90 and an RMSEA value of ⩽ .08 (Hu and Bentler, 1999). We do not report or evaluate chi-square test values because the test is oversensitive in large samples (Cheung and Rensvold, 2002). Because many of the study variables were not normally distributed, the models were estimated with mean- and variance-adjusted weighted least squares (WLSMV) estimation.
Results
Descriptive statistics
The respondents (N = 4495, 51% female) were on average 33.43 years old (SD = 18.38, range = 19–97). As for the personal health-related offline resources (M = 2.14, SD = 1.10), 35% of the respondents reported having average or worse-than-average health, 50% had a long-term illness, 10% were mentally distressed and 19% were obese. With regard to economic offline resources (M = 1.89, SD = .86), 7% were unemployed, 10% had experienced financial hardship related to food and 15% had experienced financial hardship related to medical care. In terms of social offline resources (M = 1.81, SD = .86), 18% were socially isolated, 28% were living alone, 10% felt lonely fairly often or often and 26% did not vote in the previous municipal elections.
Using a mean score of 4 or higher as the cut-off in the respective domains, 7% of the respondents reported that lack of access prevents them from using online health care and social welfare services, 17% reported lacking the necessary skills to use the services and 22% had a negative attitude towards the services. A total of 6% of respondents reported that they do not perceive the use of online services as beneficial in terms of perceived personal health-related benefits, 3% reported that they do not perceive the services beneficial in terms of economic benefits and 4% reported that they do not perceive the services beneficial in terms of social benefits.
Direct and indirect associations from offline resources to perceived online benefits through access, skills and attitudes
Before examining the structural models to study the research questions, we fitted measurement models for the latent variables. The factor loadings and the correlations between the latent constructs are shown in Supplementary Tables 1 and 2. In brief, all factor loadings were positive, high and statistically significant (p < .001), and the models had an acceptable fit (RMSEA = .08, CFI = .97, TLI = .96 for all models). The mediators (access, skills and attitudes) were highly correlated with each other (r = .86–.94), and all mediators were also correlated with the outcomes (r = .34–.53).
We additionally examined the correlations between the independent, mediator and dependent variables in a single model that combined variables from the three domains (personal health-related, economic and social domains. For all correlations, see Supplementary Table 2). Offline resources across the three domains were relatively weakly correlated (r = .19–.24) as also were offline resources and perceived online benefits (r = .09–.21). Among the offline resource variables, personal health-related offline resources were most strongly correlated with the mediators (r = .30–.33). Perceived online benefits were highly correlated across the domains (r = .85–.97).
Figure 1 summarizes the results of structural models for personal health-related, economic and social domains. The model fit was acceptable in all models (personal domain: RMSEA = .07, CFI = .94, TLI = .93; economic domain: RMSEA = .07, CFI = .93, TLI = .92 and social domain: RMSEA = .07, CFI = .94, TLI = .93). The variance explained (R2) was 31% for perceived personal health-related online benefits, 27% for perceived economic online benefits and 25% for perceived social online benefits. Lower offline resources were associated with poorer skills, poorer access, more negative attitudes towards online services and lower perceived online benefits. The hypothesized associations between the offline resources and mediators and between the offline resources and perceived online benefits were thus supported across all domains.
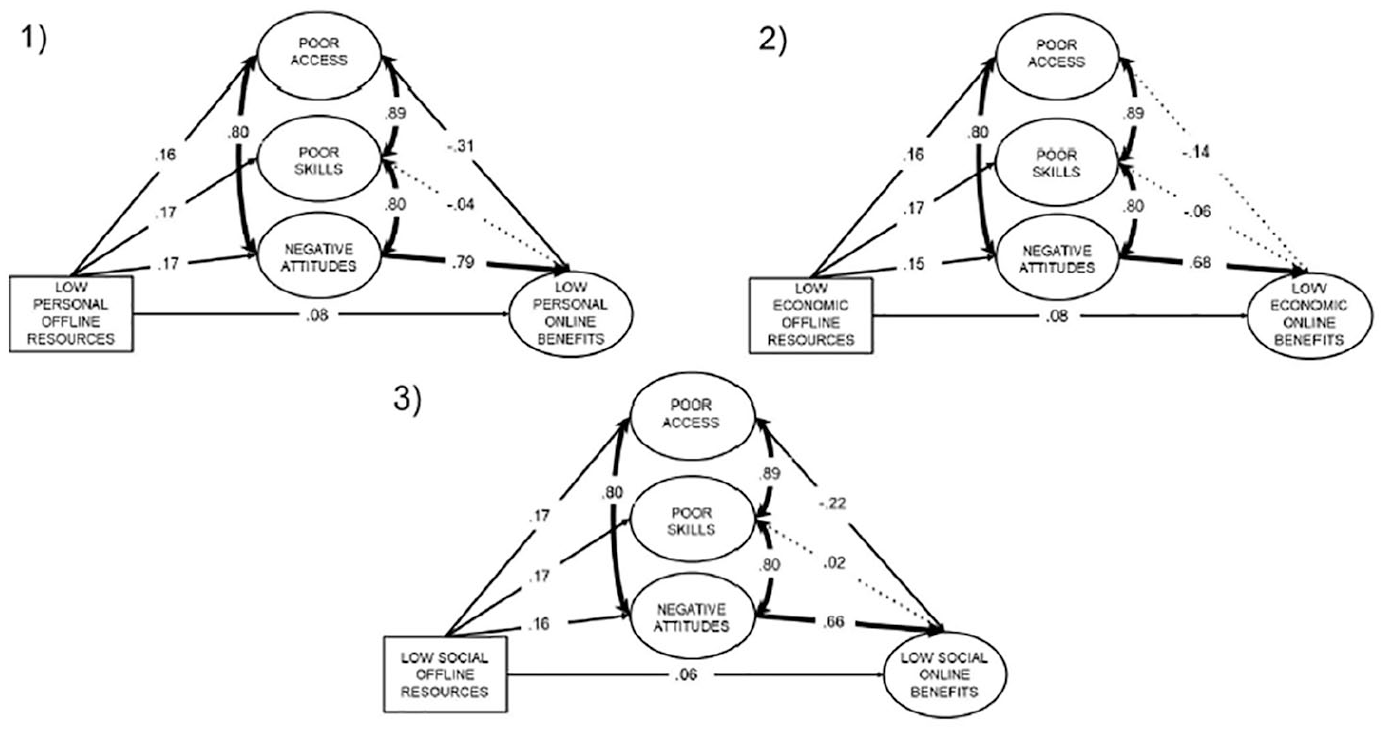
Direct and indirect associations from offline resources to perceived online healthcare and social welfare service benefits through access, skills and attitudes in the (1) personal health-related, (2) economic and (3) social domains. The factor loadings of the latent constructs are omitted for clarity. The dotted line indicates a nonsignificant association (p > .05). The thickness of a line reflects the strength of the association. All significant associations are significant at p < .01.
As for the indirect effects, the total indirect effect of offline resources on perceived online benefits through access, skills and attitudes was significant in the personal health-related, economic and social domains (p < .001). With regard to individual mediator-outcome associations, only negative attitudes were consistently associated with a lower level of perceived online benefits, whereas the associations of access and skills with perceived online benefits were either nonsignificant or of the opposite sign than expected. Consequently, the mediator-specific indirect effects of offline resources on perceived online benefits had either a positive or negative sign, depending on the mediator. This phenomenon, called inconsistent mediation, refers to a situation where at least one indirect effect has a different sign than other mediated or direct effects (MacKinnon et al., 2000). Inconsistent mediation is not uncommon in multiple mediation models where the mediators share a substantial amount of variance (i.e. highly correlated), as in this study. Due to the high correlation between the mediators, the results do not allow for direct comparison of the mediated effects between the mediators, but rather describe unique mediator effects above and beyond the other mediators in the model (Preacher and Hayes, 2008).
As a supplementary analysis, we examined the three mediators in combinations of two (Supplementary Table 3) as well as in isolation (Supplementary Table 4). If access and skills were included as mediators, the mediator-outcome-path coefficient was positive and significant in all domains for skills but only in the economic domain for access. However, if access or skills were paired with attitudes, the effects of access and skills on the outcomes were negative, while the effects of attitudes on the outcomes were larger than the zero-order correlations between attitudes and the outcomes. Because the path coefficients represent partial correlation coefficients, it is typical that the sign and magnitude of the coefficients vary, depending on the set of other variables included in the model. Finally, when examined separately (see Supplementary Table 4), all mediator-outcome associations were significant and had the same (positive) sign. Furthermore, the direct effects were of a similar magnitude, regardless of which individual mediator was included in the model, suggesting that the negative effects of access and skills in the multiple mediator model did not reflect suppressor effects (i.e. their inclusion did not increase the predictive power of offline resources on online benefits) (Maassen and Bakker, 2001). Overall, the results thus supported the hypothesis that lower offline resources were indirectly associated with lower perceived online benefits through poorer skills, poorer attitudes and more negative attitudes.
The effect size of the total mediated indirect effect was defined as the total proportion mediated, that is., the ratio of the total indirect effect to the total effect: abtotal/(c'+ abtotal), where a is the association between the predictor and mediator, b is the association between the mediator and the outcome, and c' is the direct association between the predictor and outcome, controlling for the mediators. Following the recommended approach for inconsistent mediation models by Alwin and Hauser (1975), we used the absolute values of the direct and indirect effects when calculating the proportion mediated. The proportion mediated was 72% for the personal health-related and social domains and 64% for the economic domain, indicating that substantial proportions of the total effects were mediated. Because it has been argued that using the absolute values may lead to biased estimations of the proportion mediated in inconsistent mediation models (MacKinnon et al., 2000), as a supplementary analysis, we calculated the proportion mediated from models in which the mediators were modelled as a single common latent factor rather than as three separate factors. The proportion mediated was somewhat smaller in the common-factor models in comparison with the multiple mediator models, yet still substantial (for details, see Supplementary Figure 1), which supported our conclusion about the large size of the mediated effect.
Because the corresponding fields model proposes that the different fields are interrelated, as a final supplementary analysis, we examined the sensitivity of our results to an alternative modelling strategy where we examined a model that incorporated variables from all three fields. In this model, offline resource variables for each domain predicted a mediator that was modelled as a single common factor for access, skills and attitudes, and a dependent variable that was modelled as a single common factor for perceived online benefits across all three domains (see Supplementary Figure 2). The model had an acceptable fit (RMSEA = .07, CFI = .93, TLI = .93), and all the path coefficients were significant except the direct path from social offline resources to online benefits. Based on the results, the effects of social offline resources on online benefits may be fully mediated by access, skills and attitudes – at least when online benefits are considered across the personal health-related, economic and social domains.
Discussion
Main findings
The present study found that third-level digital inequalities related to health care and social welfare services are more likely to occur among unprivileged individuals who lack personal, economic and social resources. This is partly explained by their poor online access, poor digital skills and negative attitudes towards digital services.
Our findings show the importance of personal, economic and social background variables and suggest that poverty, unemployment, social isolation, poor health and low education are risk factors for third-level digital inequality. However, these associations were largely explained by pronounced negative attitudes, poor access and low skills regarding online services. Thus, according to our results, access, skills and attitudes act as important social impact mediators between offline resources and the digital field in benefitting from online services.
Contrary to our expectations, low economic offline resources were not the most strongly associated with poor skills, lack of access or negative attitudes, and the mediation effects were not strongest in the economic domain. Our expectation was based on numerous studies showing that economic resources are associated with these social impact mediators and digital inequality (Blank and Lutz, 2016; van Deursen and Helsper, 2015; van Deursen and van Dijk, 2019; van Deursen et al., 2019). However, social resources – such as keeping in touch with friends and relatives – are less studied in this context. Our findings call for further studies related to this issue and highlight the importance of also studying domains other than the economic domain.
A previous study using the same data set suggested that the effect of age, education and degree of urbanization for perceived benefits of online services were at least partly explained by differences in access, skills and the use of online services (Heponiemi et al., 2020). Skills and health literacy are necessary for online patient portal use. Moreover, access and digital skills are crucial for ensuring the success of personal health records and their diffusion to wider user groups besides those who have high health literacy and familiarity with the Internet (Kahn et al., 2009).
Previous studies show that attitudes are important for preventing digital inequality. For example, perceived uselessness of the Internet and no interest in the Internet has been associated with Internet use (Donat et al., 2009). Older adults with positive attitudes towards technology have been found to be more willing to share their information with device developers (Kim and Choi, 2019). A study by van Dijk (2020) highlights that adoption of digital media is psychological, and that without sufficient motivation and positive attitudes, people will not develop needed skills and competence.
Our results give support to many theoretical frameworks related to digital inequality, such as the knowledge-gap hypothesis (Gaziano and Gaziano, 1996), the resources and appropriation theory (van Dijk, 2005) and Helsper’s (2012) corresponding fields model. Another previous study has also found support for the corresponding fields model, showing that differences in economic outcomes were related to economic resources such as education and income, whereas differences in social outcomes were related to social resources such as marital status (van Deursen and Helsper, 2015). Because we did not examine the associations between non-corresponding fields, future studies should examine these associations and whether some particular offline field is more strongly related to third-level digital inequalities than others.
Implications
Our result of the tight interlinkage of off- and online resources implies that tackling the fundamental causes of health inequalities – such as social and economic inequalities between population groups – is essential in preventing digital inequalities. There is ample evidence of the importance of social and economic factors in health inequities (Marmot et al., 2008; Stringhini et al., 2017). According to our results, a lack of personal, social and economic resources may reinforce inequalities also by affecting the access and ability to use online services in health and social care to improve one’s own health. Because health and social welfare services are increasingly provided digitally, socioeconomic disparities may increase and eventually lead to increased health inequalities if not given more consideration and efforts to mitigate this problem.
Our result that personal health, economic and social offline resources are associated with third-level digital inequalities partly through attitudes, access and skills implies that another way of preventing a third-level digital divide would be to reduce the first- and second-level digital divides. The availability of digital services has boomed during the COVID-19 pandemic. Access to digital systems and services to use digital services requires access to Internet technologies and networks. Increasing awareness of the services, supporting their usage skills and attitudes, is also required. A recent National Health Service (NHS) study revealed that people are not motivated to use digital health services until they are ill (Orcha, 2017). They also need more awareness of existing services and their potential. Many are concerned about their privacy, worried about losing face-to-face contacts and need support to realize the benefits of digital services (Orcha, 2017). Thus, improving access, skills and attitudes entails a magnitude of different measures.
However, it should be noted that social impact mediators did not fully explain the association between the lack of offline resources and third-level digital inequalities. Inequalities remained even after controlling for access, skills and attitudes, the proportion explained by mediators being slightly smaller (64%) for economic fields than for personal health-related and social fields (72%). Thus, to overcome inequalities in digital societies, a more systematic change in inequalities is needed – both in offline resources and social impact mediators (access, skills and attitudes).
Strengths and limitations
One of the strengths of our study is that we were able to use a large representative sample of the Finnish adult population. Moreover, we addressed the gaps in previous research (Hargittai, 2002; Scheerder et al., 2017) by focussing on examining the perceived benefits of online services. Our study provides much-needed information about the social determinants of benefitting from online health and social welfare services (Scheerder et al., 2017). Our study shows that there are groups that do not perceive benefits from digitalized health care and social welfare services and are therefore in danger of missing out on the services that society offers. Another strength of our study is that we used SEM to study the hypothesized associations. A major advantage of SEM over other approaches, such as regression, is its ability to simultaneously model direct and indirect associations among multiple factors without measurement error (Kline, 2016). To the best of our knowledge, no previous study has examined the indirect associations between offline resources and online benefits through access, skills and attitudes in a multiple mediator model.
There are also limitations that need to be considered when interpreting the results. The present findings are based on self-reported data, which can lead to problems associated with common method variance and inflation of the strengths of associations. Our measures showed good reliability, which helps to reduce these problems. However, there may be some conceptual inaccuracies in some of the measures; for example, the attitude measure could be seen as motivational, and the skills measure may also reflect confidence. Moreover, our benefit measures reflected subjective (i.e. perceived) benefits on a general level rather than objective benefits for them as individuals. Because the data were from a population study representative of the Finnish adult population and not from a survey among electronic service users, benefits were measured on a general level rather than on a personal level.
Because resources are often intangible, they are hard to explicitly measure and quantify. Despite the usefulness of the composite score approach adopted in the present study, composite scores are a crude measure of resources. Because the data were cross-sectional, causal inferences cannot be drawn based on the results. Moreover, even though we controlled for age and gender, a possibility of residual confounding still exists. In addition, we did not include technology use in our model, although it is potentially an important factor regarding third-level digital inequality. This was because we focussed on perceived benefitting from online services instead of usage patterns. Helsper’s (2012) model proposes that digital inequality is defined less by the actual use of technology and more by whether the nature of technology use improves one’s life.
Caution should be applied when generalizing our findings to countries with other types of healthcare and social welfare systems or online services. Finally, with the present data, we were not able to exclude reverse causality as an explanation for our results or to examine reciprocal relationships. Further studies are needed to test the potential bidirectional relationship between offline resources and third-level digital inequality as well as the mediating mechanisms underlying the potential reciprocal effects.
Conclusion
According to our results personal, economic and social offline resources are associated with the third-level digital inequalities largely through attitudes, access and skills. Thus, to improve equality, these issues should be addressed particularly among those who lack any of these resources. This is more important now more than ever, given the rapid expansion of online services due to the outbreak of the COVID-19 pandemic. Social and health care service providers should improve the availability of online services – especially for specific illnesses – to increase the motivation to use them. Public authorities should increase and facilitate access to the Internet and related technologies among the most vulnerable groups in the communities. Social and health service providers that offer digital services are responsible for making sure that their clients are aware of the offered services and their potential and are able to use them.
Skills can be improved by ICT training that includes working in pairs, device training, the possibility to influence what is taught and material that enables communication and learning (Lopez Segui et al., 2019). The health and social service providers as well as non-governmental organizations should consider ways to improve health literacy among vulnerable groups as this is likely to have an effect on attitudes towards using digital services for health benefits. It is important that online health and social welfare service designers increase their understanding of the needs of people in vulnerable positions to develop the usability and benefits of the services to also meet the needs of less informed population groups. An important measure to improve the position of vulnerable population groups would be to tackle the root causes of these problems in terms of inequities in economic and social resources as they are related both to health inequalities and – according to our results – seem to widen the digital gap.
Supplemental Material
sj-docx-1-nms-10.1177_14614448211023007 – Supplemental material for Digital inequality in Finland: Access, skills and attitudes as social impact mediators
Supplemental material, sj-docx-1-nms-10.1177_14614448211023007 for Digital inequality in Finland: Access, skills and attitudes as social impact mediators by Tarja Heponiemi, Kia Gluschkoff, Lars Leemann, Kristiina Manderbacka, Anna-Mari Aalto and Hannele Hyppönen in New Media & Society
Footnotes
Acknowledgements
This study was supported by the Strategic Research Council at the Academy of Finland (project 327145) and the Ministry of Social Affairs and Health (project 112241).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Strategic Research Council at the Academy of Finland (project 327145) and the Ministry of Social Affairs and Health (project 112241).
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.