
Abstract
Objective
Indigenous people face inequities when accessing primary care. It is critical to center Indigenous people and their lived experiences within primary care improvements to address these ongoing inequities.
Methods
Using the Theoretical Domains Framework (TDF), the purpose of this study was to understand the barriers and facilitators to implementation of an Indigenous patient experience tool in virtual care.
Results
Nineteen interviews were completed with participants that included 12 patients and seven physicians and data were analyzed using reflexive thematic analysis. Themes endorsed by participants were directly related to four TDF domains: 1) Beliefs about consequences; 2) Environmental context and resources; 3) Skills; and 4) Knowledge. This study found that both patients and providers found the implementation and use of the Access, Relationships, Quality, and Safety (ARQS) tool both useful and relevant.
Conclusion
Future research should explore if sustained and recurrent use of the tool within therapeutic relationships leads to improvements in the delivery of virtual primary healthcare.
Introduction
Disparities in access to high-quality healthcare services contribute to inequitable outcomes and widen health gaps between Indigenous and non-Indigenous populations. 1 Primary Health Care (PHC) is a foundational aspect of healthcare with its basis in core principles of universal access, health equity, community participation, and intersectoral approaches. 2 The provision of health-related services and information using telecommunications-based technologies including text, telephone, and video are approaches referred to as virtual care. Some of these approaches have been promoted to address challenges related to PHC access for Indigenous people, including those in remote or rural communities across Canada (e.g. individuals living on-Nation and/or in rural or remote areas).2–4
Literature exploring Indigenous patients’ attitudes and experiences of virtual care services have shown that virtual care is an acceptable modality to bridge health inequities.3,4 Research in Australia showed that participants appreciated personalized approaches to care embedded in virtual care services. 5 In Canada, work examining the acceptability of virtual care for health through mobile phones showed that it can support connections and relationships 6 and decrease travel distance and costs, thereby improving timeliness of access to care.7,8 A scoping review by Moecke et al. 9 specifically examining telehealth services found that 29 percent of the studies included in the review (n=231) listed cultural relevance or appropriateness as a facilitator for effective telehealth use. This means that a component of effective virtual care is the sustainability of this model of care and the ability for virtual services to be culturally tailored to suit the needs of the population using it.4,5,10–12 Conversely, operational feasibility has been found to be a barrier, 13 as well as privacy concerns and confidentiality. 14 Reported barriers to using virtual health services include having limited access to and/or familiarity with technology. 10
A rapid increase in the emergence of virtual care occurred during the novel coronavirus SARS-CoV-2 (COVID-19) pandemic in late 2019. 15 In response to global public health restrictions, including physical distancing and minimizing in-person contact to mitigate COVID-19 transmission, healthcare delivery, including PHC services, rapidly shifted to virtual delivery modes. 16 As a swift and direct response to the COVID-19 pandemic, the Alberta Indigenous Virtual Care Clinic (AIVCC) was deployed to meet the needs of Indigenous people across the province of Alberta, Canada. Indigenous people make up approximately 6.5% of the Alberta population (258,640 people) which include 45 different First Nations, Métis people in all urban, rural, and remote areas including Métis settlements, and a small Inuit population. The AIVCC continues its aim to provide culturally safe virtual care to Indigenous people (defined by the service as any self-identified First Nations, Métis, or Inuit person). In an effort to facilitate culturally safe care, the healthcare providers for the AIVCC have had previous experience working with Indigenous patients and/or are Indigenous themselves. Due to the rapid formation and mobilization of the AIVCC, it was implemented before developing plans to measure and monitor the quality and impact of virtual care delivery from the perspective of Indigenous people.
As a precursor to the current study, PR completed previous research to develop an Indigenous-centred understanding of virtual high-quality PHC. Grounded in Indigenous patient experiences and worldviews, a conceptual framework was developed that included access, relationships, quality, and safety (ARQS) as central components of virtual high-quality and Indigenous-specific PHC. As a follow up to that work, a qualitative study with Indigenous patients and PHC providers was completed to co-create an Indigenous patient experience tool for virtual PHC.
17
Building on the ARQS conceptual framework, the ARQS tool was developed to collect data and improve the experience of quality PHC for Indigenous patients. Through a series of cognitive interviews and guidance from an Indigenous advisory committee, the ARQS patient experience tool is grounded in Indigenous experiences and perspectives and includes 12 strengths-based statements that assess virtual care across all four domains of ARQS. The ARQS tool is displayed in Figure 1. ARQS patient experience tool.
The next step in continuing to improve Indigenous virtual care is implementing and evaluating patient experience tools with patients and providers to ensure that high-quality, culturally safe virtual care can be sustainably measured and monitored to support ongoing clinical quality improvement. Creating virtual health care services that include patient experience measurement tools and co-designing these tools with patients is an effective way to improve health outcomes, adherence, and safety.18–21 Additionally, implementation science frameworks suggest that understanding the barriers and facilitators (determinants) to adopting of a new tool from the perspective of both patients and providers is an important first step in implementation. 22 The Theoretical Domains Framework (TDF) 23 is an effective way to explore determinants of adopting a new tool, how to refine it, and how to successfully evaluate implementation.24,25 Previous studies have established that refining specific factors in the TDF is key to successful implementation of new tools.25,26 The aim of this study was to understand determinants of successful implementation of the tool to inform improvements and plan for ongoing use, spread, and scale of the tool to support monitoring and improve the quality of Indigenous virtual PHC.
Methods
Ethics and guiding principles
This pilot implementation study was informed by principles of participatory action and patient-oriented research.27,28 Participatory action research is patient-oriented research conducted in partnership with patients, their care partners, and families. 27 This research facilitated a collaborative model where patients, families, clinicians, researchers, policymakers, and health systems-leads worked together throughout the research process supporting patient-identified priorities with the ultimate goal of better health and systems outcomes. 29 The Indigenous ethics that guided this study also support a framework grounded in ethical space.30,31 This concept facilitates partnership between Indigenous worldviews (epistemological understanding from an Indigenous standpoint) and western health services while upholding ethical principles that are appropriate for engaging Indigenous partners appropriately throughout the research process.31–33 An Indigenous advisory group was formed to guide the project. This advisory group included an Elder, two Indigenous community representatives who had accessed virtual care, two Alberta Health Services (AHS) clinical managers, and a member of leadership from the AIVCC. This group contributed to the study design and research plan at the outset of the project, in addition to advising throughout the study on data collection, analysis, and interpretation. The project team was Indigenous-led by PR the Principal Investigator, with both Indigenous and non-Indigenous team members with experience in Indigenous health research and implementation science. This study received ethics approval through the University of Calgary Conjoint Health Research Ethics Board (REB22-0007).
Implementation description
The implementation of the ARQS tool was examined from the perspective of both patients and physicians. The tool was included in a survey that was sent to all patients who had attended a virtual care appointment since the AIVCC opened in fall 2020. The survey was open from January 13 – March 6, 2023, and 355 patients responded. The survey has been distributed to patients again in September/October 2025 and is planned to be distributed again in 2026. The actual data collected by the clinic through the ARQS tool is clinic data and not accessible to the study team but through the team’s ongoing relationship with the AIVCC the team has been made aware that the ARQS tool is being used for continuous clinical quality improvement.
Recruitment and sampling
Patients were considered eligible to participate if they identified as Indigenous, lived in Alberta, had accessed care with AIVCC at any point since its inception in 2020, and had previously completed the ARQS tool, which had been distributed a month before recruitment began (see above). Physicians were eligible to participate in interviews if they had provided virtual and/or remote PHC through AIVCC. Information on the current study was included at the end of the ARQS survey when sent out from the clinic as part of their regular process. This included study team contact details so that interested clinic patients could contact the research team directly. Study information was provided to physicians through clinic leadership and administrative staff affiliated with the AIVCC. Physicians were similarly able to contact the research team if they were interested in participating. Convenience and purposive sampling were used in order to recruit participants able to provide rich description of the experience of completing the ARQS patient experience tool. 34 Informed written or oral consent was obtained prior to the start of each interview. Both patient and physician participants were compensated for their time.
Data collection
Qualitative semi-structured interviews were completed with patients and physicians from the AIVCC to understand the determinants of the implementation of the ARQS tool. Interviews are a commonly used research method within healthcare settings and are proven as a way of obtaining in-depth accounts of personal experiences. 35 Such in-depth interviewing techniques have advantages when exploring how people make and attach meaning to events in their lives, as they allow for ‘guided’ conversations in order to elicit responses through a natural setting.35–37 The interview guide (Appendix 1) was developed through prior knowledge of virtual care studies17,38 informed by the TDF, 23 and reviewed by the study team and the Indigenous advisory group at the project’s outset. 39 All participants were asked about their experiences with the ARQS tool. Questions about the tool were designed around acceptability (“Does the tool address the needs of Indigenous people?”), utility (“Is the tool easy to use?”, “Do you think this tool provides useful feedback to the clinic/healthcare team?”), and facilitators and barriers to using the tool (“Does using this tool affect your appointment in a negative way? i.e. communication, time, autonomy”).
All interviews were completed via secure web-conferencing software and were audio-recorded for transcription purposes. Data were transcribed verbatim using an REB-approved and secure third-party service.
Data analysis
Qualitative interviews were analysed using reflexive thematic analysis40,41 and NVivo software was used to organize and manage data. 42 Reflexive thematic analysis is an approach which involves aligns with Indigenous ways of doing research and includes reflection and interpretation by the researcher. 43 Initial coding was done by PR, who is an Indigenous Associate Professor in Family Medicine, first author and project Principle Investigator, and LZ. Coding was completed both deductively and inductively, mapping descriptive codes onto the TDF domains while also creating codes describing experiences within, and in addition to each domain, to capture patient and physician experiences. Codes were generated individually by both coders before comparing codebooks and discussion for consensus building. Additionally, member checking, peer debriefing, and triangulation of the patient and physician data were employed to enhance rigor. 44 This included iterative discussions of the findings and implications with the Indigenous advisory group and with participants to ensure the interpretations of the research team were guided by Indigenous worldviews and relevant to clinical experiences. The qualitative analysis was applied to the TDF to ensure that understandings of implementation of the ARQS tool for both patients and physicians were framed in a way to support ongoing utility to clinic practice and performance.
Results
TDF domains with themes and example descriptive codes.
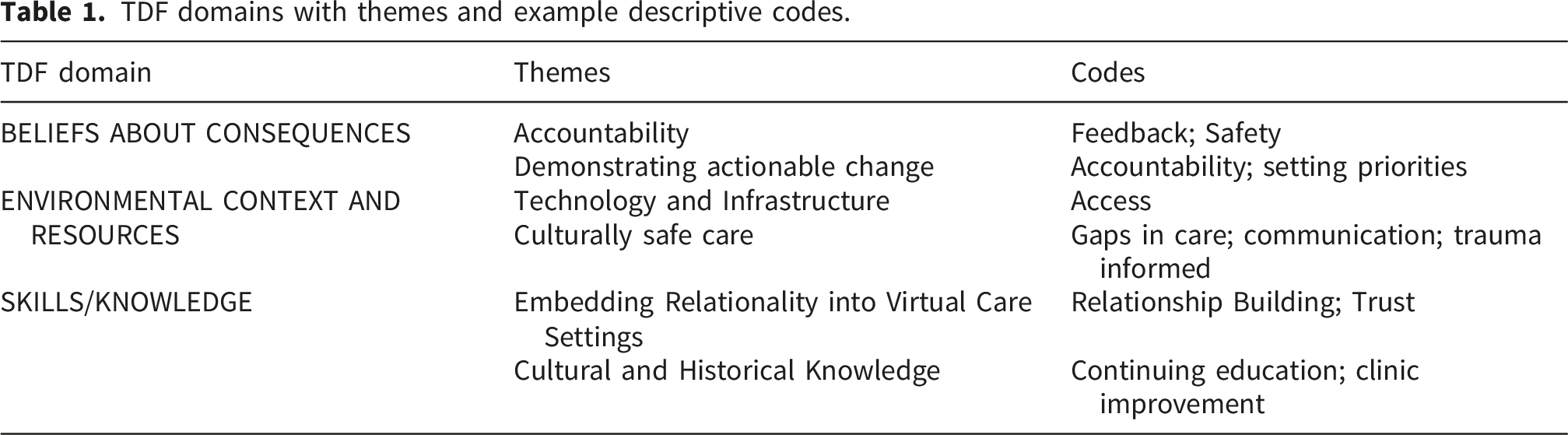
Beliefs about consequences
This domain included patient and physician perspectives on the need for accountability during and after the implementation of the ARQS survey. Themes included Accountability and Demonstrating Actionable Change. Interestingly, all participants initially saw the value in reporting survey outcomes at the clinic level as means of promoting collaboration in the clinic, and before considering implementing any reporting at the level of individual physicians, which could be a means of tracking outcomes.
Accountability
Patient participants had positive feedback on the implementation of the tool into regular clinic processes, including their willingness to complete it in the future for feedback on how the virtual services address the needs and relevance of Indigenous peoples. Participants reported that they would complete the survey again to give feedback about their experience if it could lead to clinical improvements and increased accountability on the part of the health services. Physician participants agreed that feedback on clinical care was important for implementing improvements. They emphasized that this is especially important for Indigenous patients whose experiences are often overlooked in healthcare generally and that if the system were asking for this information, it was important to create change from that information. This is articulated in the following quotes from a patient and physician. “I think knowing that there’s some kind of accountability, that there’s just somebody watching, that I have the opportunity to have my voice heard on this afterwards is really important.” - Patient 9 “And then as a clinic though, I think that we also have the same idea of we want to be able to provide really high-quality virtual care within the limitations of virtual health. So being able to know where we're maybe not stacking up would be helpful to try to address it at a clinic level.” - Physician 5
Demonstrating actionable change
Both patient and physician participants indicated that in addition to the need for accountability, there was a need for clear communication and demonstration of actioning change. The implementation of an Indigenous patient experience tool is only valuable if improvements are driven by the survey results. “I think it’s a way to have accountability and it’s some kind of a barometer to have accountability. My concern is always that some people won't use it, seeing that as a colonized tool as opposed to being able to see past that and see that somebody somewhere is trying to see if this system's working properly.” - Patient 9 “If we get back feedback, we’ll have to figure out what we’re doing wrong and make it better.” - Physician 6
Environmental context and resources
This domain included the context of access to PHC for Indigenous people and included the themes of Technology and Infrastructure and Culturally Safe Care. Patient participants reported that using the tool affected their appointment in a positive way as they could provide feedback to a service they valued.
Technology and infrastructure
Patient and physician participants recognized that the technological requirements of an online tool may be a barrier for some Indigenous people, depending on the infrastructure available community to community. This may hinder some patients in completing the tool, highlighting the importance of making the tool available via telephone or other methods. “I think it boils down to the accessibility of it…. I did a lot of travel around to the First Nations in Alberta and not all of them have service, whether that be great internet service, or even cell service, where some nations are just really cut off.” - Patient 2 “There might be an issue for certain demographics, especially for elderly people. How is the tool going to be completed? Is it an online tool that going to be done online? That will take out a lot of elderly people. A lot of elderly people in communities don't have access to a computer or don't use a computer on a regular basis.” - Physician 3
Culturally safe care
Patient participants discussed how the tool directly addressed their needs as Indigenous people and shared how relevant the questions were to their own experiences of marginalization and discrimination. Similarly, physicians recognized the critical importance of culturally safe care in ways that can be patient-centered and tailored to the needs of every patient. “I think it was the way the wording was, it felt very caring rather than, I don't know what word to use, but usually with medical spaces it's more, I guess, cold. And these questions felt warmer and more caring about the patient… They’re culturally appropriate. They come from an Indigenous worldview. They talk specifically about healthcare providers as being almost like its one part of your holistic health.” - Patient 6 “Some patients are using traditional practices, but they're also seeking western medicine. So I think that's a really important part. It's relevant to Indigenous people for incorporating that and making sure that those people are able to say whether or not they felt safe sharing that they were using traditional practices, whether they felt judged or whether they felt like this was a really accepting space for them.” - Physician 6
Skills and knowledge
This domain included the themes of Embedding Relationality into Virtual Care Settings and Cultural and Historical Knowledge. Patient participants discussed how using the tool positively impacted the quality of their appointment because it made them feel safe, heard, and listened to. Both patients and physicians noted how the tool promoted improved skills in relationships and the need for ongoing education about Indigenous history, worldviews, Ways of Knowing and Doing, and approaches to healing and wellness.
Embedding relationality into virtual care settings
Participants identified that having the tool available made them feel more cared for and respected. Receiving the tool at the completion of the visit was seen as an invitation to engage in a relationship with the care team and the clinic. Physicians also stated that they appreciated the opportunity to receive feedback in a new way that made them optimistic it reinforced a caring relationship. “There was one here that I really liked. It was my virtual healthcare provider understands who I am and why I want to talk to them. I think that’s a really good Indigenous worldview and a way to develop that relationship with your healthcare provider.” - Patient 6 “I would hope that even just having this implemented would provide patients with some sense that we really care about this and give them an opportunity to give feedback and maybe in other healthcare settings where they may not have given an opportunity or have a chance to do that.” - Physician 2
Cultural and historical knowledge
All participants emphasized the importance of education on Indigenous culture, history, and traditions for healthcare providers. This knowledge was important in creating a relational and safe clinical environment. It was beneficial to include questions in the tool that reflected provider knowledge about Indigenous history and culture. It was reported that healthcare settings become accessible when they feel safe, and that ongoing education is a critical step towards improving safety. “What we know about ways of increasing safety is around education, knowledge, awareness, improvement. This tool has the potential of doing that or offering that to a range of health professionals.”- Physician 7 “There’s so much more that a lot of healthcare providers have to learn about Indigenous people in general. And there's so much more to learn… so much more that a lot of people need to be trained in with regards to awareness, the trauma aspect of it, the actual healthcare side of it.” - Patient 10
Discussion
This study aimed to examine the determinants of the implementation of an Indigenous virtual PHC patient experience tool. All participants felt that the ARQS tool was of benefit to patient experiences and clinical practice, and they could see the value of continuing to use it. The value of the tool was reflected in four of the TDF domains: Beliefs About Consequences; Environmental Context and Resources; Skills; and Knowledge. Corresponding themes were identified in each domain that emphasized accountability and actionable change (beliefs about consequences); access to technology and culturally safe care (environmental context and resources); and ongoing support to embed skills and knowledge around relationality and Indigenous culture (skills and knowledge). Facilitators of using the tool included patients believing the tool gave them a voice and autonomy on their own healthcare journey. The use of the TDF was beneficial for understanding how the TDF can be used to understand the implementation of a patient experience tool into practice. However, the TDF is limited in the ability to assess cultural safety and Indigenous specific aspects of care due to the fact it is, itself, a tool developed using a western paradigm. The advisory group was essential in guiding the domain mapping decisions by ensuring important concepts such as relationality and cultural safety were represented despite not being explicitly included in the TDF. These results highlight the importance of self-determination for Indigenous peoples’ health. The United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP) identifies “the urgent need to respect and promote the inherent rights of Indigenous people” while upholding “the fundamental importance of the right to self-determination of all peoples”. 45 Specific to health, Article 23 of UNDRIP states that Indigenous peoples’ have a right to be a part of “developing and determining health, housing and other economic and social programmes affecting them.”. 45 Article 24(1.) states Indigenous peoples “have the right to their traditional medicines and to maintain their health practices” while having the right “to access, without discrimination, all social and health services.”. 45 Furthermore, Article 24(2.) states that Indigenous peoples have the right to the “highest attainable standard of physical and mental health”. 45 This right explicitly includes access to cultural and traditional healing practices. This makes research such as the study reported here even more critical, as although there are professional policy statements such as the Canadian Medical Association (CMA) code of ethics and professionalism, 46 we know that Indigenous patients continue to experience harm within the health system and from physicians with self-reported anti-Indigenous bias. 47 Therefore, embedding the expectation to the right to culturally appropriate care into patient experience measures such as the ARQS tool becomes an important way to work toward structural change. In addition to the inherent right to autonomy and self-determination, participants identified accountability as another facilitator to using the AQRS tool because it held healthcare providers accountable. The importance of this accountability is highlighted in the Truth and Reconciliation Commission of Canada Calls to Action, specifically #43, which calls for “fully adopt and implement the United Nations Declaration on the Rights of Indigenous Peoples as the framework” for reconciliation. 48
Our findings suggest the tool had many positive impacts on Indigenous patients’ experiences of virtual care and on the physicians providing virtual care. Patient participants hoped that by filling out the tool, they could provide feedback that would contribute to ongoing improvement for the virtual PHC clinic. This is important as Indigenous peoples face many barriers to healthcare including travelling outside their communities, difficulties getting referrals, and healthcare services not being offered in their area. 49 Patient participants felt the tool helped them feel more respected and cared for. Relationality plays a crucial role for Indigenous patients when seeking healthcare, and this is especially important in the context of virtual care.17,38,50,51 Physician participants stated that the act of asking for feedback in a way that is grounded in Indigenous worldviews and having the opportunity to respond to it strengthened the clinical relationship with patients and helped build trust. Both patients and physicians reported that a facilitator to using that the tool was that the questions were viewed as safe and trustworthy, while sharing their hopes that it would increase cultural safety. This aligns with the literature that trust is important to the patient-physician relationship when considering experiences of racism and discrimination Indigenous peoples face when accessing healthcare.52,53 This work also addresses the measuring and monitoring requirements to provide safe virtual care, as recently recommended by the Alberta Virtual Care Working Group. 54
Previous literature highlights the limitations of virtual healthcare delivery including a lack of integration of traditional languages, barriers with access to technology and digital literacy, and limited access for those with hearing or vision loss.8,12,51 It is important to note these accessibility barriers are similar to the barriers identified in completing the ARQS tool. Future research with regards to spread and scale of tools such as ARQS could explore innovative ways to advance inclusivity so that all Indigenous patients have an opportunity to share their voice. This could include having paper copies sent to patients who request them, having support available to complete the tool over the phone, or integrating accessibility adaptations for those that are hard of hearing or vision.55,56
An important consideration is the interconnectedness of the domains described here, and the themes generated within. Accountability and actionable change are driven by results, while results are facilitated by access to culturally safe care. Culturally safe care and improvements are achieved through skill acquisition and knowledge building. In order to support physicians and other clinic staff to address areas of needed improvements, it was a project priority to provide resources through which to do that. Measuring and monitoring patient experiences are important to healthcare improvement, but without resource and direction, it can be challenging to make improvements where needed. It is important to recognize that the environment and resources available in the virtual care context can substantively impact feasibility of continued use of the tool and therefore monitoring of patient experience and improvements in care. The research team and clinic team have maintained a relationship to further support ongoing improvements and identify resource needs to continually advance feasibility. To facilitate this within the scope of this project, the project team completed an environmental scan of literature and available training resources, mapped these resources to the questions included in the ARQS tool, and returned this resource to the clinic team for their use (see example content from this resource in Figure 2.) Content from physician resource package.
Resources included a variety of options to suit individual physician capacity, interest, and available time, and included articles/publications, books, films, podcasts, webinars, and online courses. Each resource listed the following: the approximate time required, a summary of the content, where the resource were located, and the ARQS domain addressed. Anecdotally, the resource package has proven to be useful for physicians but the virtual providers have identified time constraints as a significant limitation to engagement with the materials. Ongoing logistical supports have been made available to build the ARQS tool into the clinical electronic systems so that the clinic can continue to use this tool as part of their continuous clinical quality improvement processes.
Limitations
This study looked specifically at evaluating the implementation of an Indigenous virtual care quality tool, not the clinic or care received. Further research to understand how responses and feedback shared via the tool facilitate changes to delivery or care received will be important to enhance care and patient experience. In the ARQS tool itself, statement 12 contains two concepts regarding provider acceptance of both cultural needs and/or traditional healing practices. It may be useful in future work to explore these concepts as separate items as culture is extensively varied, and not all Indigenous people are connected in the same way to culture or traditional healing practices. Understanding the nuances between these would ensure provider understanding and implications to patient outcomes and satisfaction. Participants who had positive experiences may be more likely to participate; therefore, future research should try to reach individuals less likely to participate to understand broader views. Furthermore, this study may not be transferrable to other Nations or Indigenous Peoples as virtual care and delivery may vary between clinics, communities, and healthcare systems. Future work could use the ARQS tool as a foundation to develop patient experience tools in other local contexts to improve virtual care with Indigenous patients. It may also be of benefit for future research to examine the barriers and facilitators to the inclusion of this type of work into large-scale electronic medical records. The research team also recognizes the limitations of using the TDF to determine domains of improvement when working with Indigenous communities and individuals. Developing Indigenous-specific domains such as cultural safety and relationality would be of benefit to the scientific field and to implementation of service improvements. 57 Further research is needed to develop decolonial approaches to implementation science and the team is planning to explore opportunities to undertake this work.
Conclusion
The purpose of this study was to understand the determinants of the implementation of the ARQS Indigenous patient experience of virtual PHC tool. Grounding the work in practice contexts and guiddance from an Indigenous advisory group helped establish what we believe is a sustainable tool for clinical care providers and systems to measure Indigenous patient experiences. Which can then be used to inform continuous improvement in care provision and contribute to plans to spread and scale similar initiatives. The ARQS tool was co-designed and co-developed to help capture, monitor, and measure continuous learning and improvement in the virtual care setting. Our results suggest both patients and providers found the tool useful and relevant to their experiences within the AIVCC. Future research could incorporate more quantitative research to explore how ongoing use of the tool can lead to continual improvements to the delivery of virtual PHC while addressing the health inequities faced by Indigenous people in health systems.
Supplemental material
Supplemental Material - “They felt like safe questions in a safe environment”: A qualitative study examining the implementation of an Indigenous virtual primary care patient experience tool
Supplemental Material for “They felt like safe questions in a safe environment”: A qualitative study examining the implementation of an Indigenous virtual primary care patient experience tool by Pamela Roach, Lisa Zaretsky, Meagan Ody, Michelle Hoeber, Stephanie Montesanti, Rita Henderson, Richard Oster, Sonya Regehr, Cara Bablitz, Cheryl Barnabe, Khara Sauro in Health Informatics Journal.
Footnotes
Acknowledgements
We would like to acknowledge Melissa Scott for her contribution to the data collection phase of the project.
Ethical considerations
This study received ethics approval through the University of Calgary Conjoint Health Research Ethics Board (REB22-0007).
Consent to participate
Informed consent was obtained from study participants prior to research activities.
Author contributions
PR led the project design with input from KS, SM, RH, RTO, CB, CB. Data analysis was completed by PR and LZ. Manuscript writing, organisation and editing were done by PR, LZ, KS and MO, and all authors read, edited, and approved the final manuscript. PR acts as the guarantor for the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the CIHR Operating Grant competition: Indigenous Peoples and COVID-19 Rapid Research Operating and Knowledge Mobilization Grants Funding Opportunity. Grant Number: F01-181133.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
In accordance with our ethics approval and due to the personal nature of the data collected, we cannot release full data sets outside of the study team.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.