
Abstract
Background
Telerehabilitation (TR) has been increasingly used to deliver psychological and neuropsychological care remotely, especially since the COVID-19 pandemic. As health services continue to shift toward telehealth, ensuring ethical and equitable TR delivery is essential to establish sustainable TR models.
Objective
The objective of this review is to synthesize existing evidence on the ethical and equity-related benefits and pitfalls associated with the use of TR in a psychological and neuropsychological context for individuals with physical disabilities.
Methods
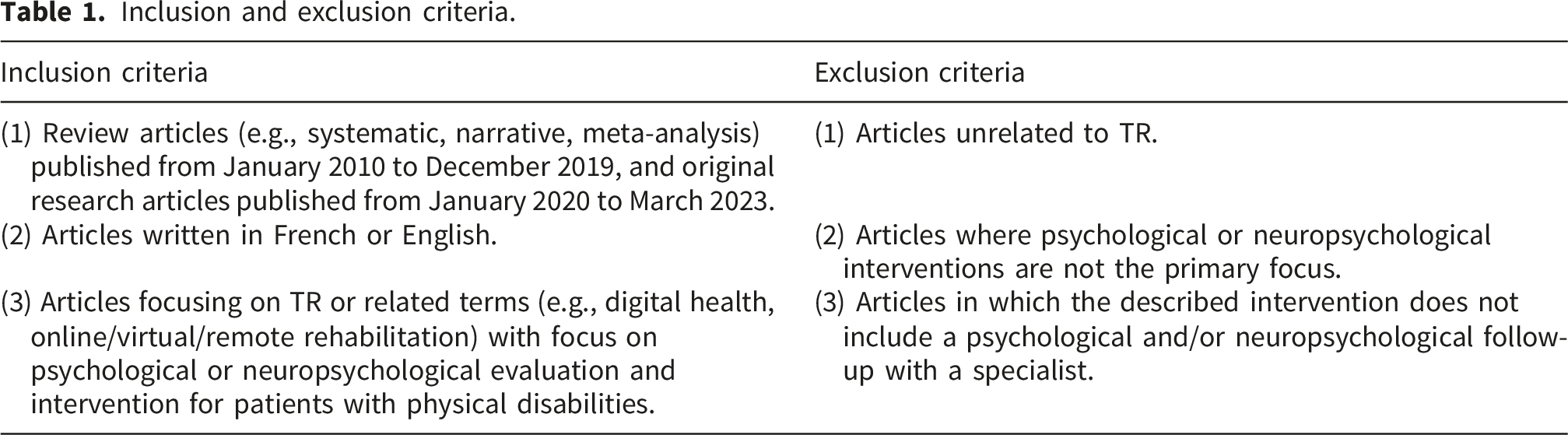
This rapid review included reviews (2010–2020) and original studies (2020–2023) that focused on TR interventions for people with physical disabilities in the context of psychology and neuropsychology rehabilitation.
Results
A total of 16 reviews and 82 original articles were included. Key ethical concerns centered around privacy, confidentiality, caregiver burden, and clinician-patient relationship quality. Equity concerns centered around access disparities (e.g., geographic location, income), digital literacy, and demographic underrepresentation.
Conclusion
This review is part of a pan-Canadian initiative aimed at informing policy development and clinical practice in TR. Findings highlight the need for clear guidelines and targeted interventions to ensure that TR in psychology and neuropsychology is both ethically sound and equitable.
Introduction
In the last few years, telehealth has been increasingly used as a means to deliver rehabilitation services, especially in the context of the COVID-19 pandemic. Rehabilitation refers to the wide range of training and therapeutic practices aimed at helping individuals recover from injuries, illnesses, or disabilities. 1 Telerehabilitation (TR) is the application of information and communication technology to deliver rehabilitation services at a distance. 2 TR uses various communication technologies to facilitate interactions between clinicians and patients,3,4 including real-time interactive sessions (synchronous) with audio and/or video, and interactions that do not occur in real time (asynchronous) such as exercises links or educational videos. TR can serve as a substitute for or a complement to face-to-face visits, reducing the need for in-person appointments, travel, and hospital stays, while also providing additional education and support.5–7 The use of TR in recent years has been particularly accelerated by the COVID-19 pandemic. During this period, the public health system had to adjust its services in response to the emerging health crisis, including adapting care delivery methods.8,9 With strict distancing measures in place, TR emerged as a viable alternative to conventional in-person visits, ensuring continued delivery of essential rehabilitation services. 10 Evidence shows that TR achieves patient outcomes and satisfaction levels comparable to traditional face-to-face care11–14 and is effective for patients with diverse conditions across the lifespan.15–22
Psychology and neuropsychology services have long been provided online for therapy, assessment, and diagnosis, 23 and are also used within TR for individuals with physical and cognitive disabilities or injuries.24–26 Online psychology and neuropsychology services help maintain continuity of care, and may reduce healthcare costs.21,27,28 Early on, online psychology and neuropsychology services faced ethical concerns, including doubts about their effectiveness and feasibility, unclear regulations, and barriers related to users’ digital literacy and internet access. These concerns were amplified by the limited empirical research on these issues.21,27,28 Today, as the use of TR continues to expand and create new healthcare opportunities, it simultaneously raises additional concerns about its ethical and equitable use. 29 Yet, guidance on how to address these emerging ethical and equity-related issues remains scarce and inconsistent.
Ethics refers to moral principles of conduct such as integrity, accountability, and respect for privacy and confidentiality. 30 In the context of online psychology and neuropsychology service delivery, ethical challenges include risk management, particularly when working with clients who could pose a risk to themselves or others. 31 The remote format can limit the clinician’s ability to detect warning signs and ensure the client’s safety in real time. Concerns also arise regarding privacy, as online sessions may take place in varied settings such as shared spaces where others can overhear or interrupt. These issues also extend to the confidentiality of digital information: without strong safeguards, sensitive information may be exposed during transmission, storage, or disposal of data. 31
Equity-related issues are also prominent in the context of online psychology and neuropsychology service delivery. Equity refers to fair access to healthcare regardless of background (e.g., social, economic, or demographic background). 32 TR is promoted as a mean of improving access to healthcare, particularly for individuals who face barriers to in-person visits such as limited time, resources, or means to travel (e.g., those living far from clinics, with mobility issues, or with demanding work or caregiving obligations).33–37 Unfortunately, telehealth services simultaneously may exacerbate social and cultural disparities by requiring patients to have access to private, high-speed internet and sufficient digital literacy. 38 For instance, individuals from ethnic minority groups have been shown to be less likely to have high-speed internet access, which could hinder their use of telehealth services and widen disparities. 39 Given these concerns, clinicians and clients need to remain vigilant about the ethical and equity-related risks of TR. As a model that is still in development, unguided or inconsistent TR practices may compromise quality of care, which could be particularly harmful for the most vulnerable in our society. Clinicians, managers, and decision-makers face ethical dilemmas regarding its broader implementation, 40 while individuals with disabilities require support and resources to adapt to this evolving reality. Developing and implementing clear, robust guidelines and tools is essential to prevent unethical and inequitable practices. This involves addressing critical challenges for both healthcare providers and patients, and proactively identifying and resolving potential disparities that may further disadvantage certain groups. 3
This rapid review aims to examine how psychology and neuropsychology services are practiced in the context of TR, focusing on ethical and equitable considerations. This review is part of a larger pan-Canadian initiative aimed at informing policy and clinical practice to provide ethically sound and equitable virtual rehabilitation care. 41 The project includes a series of rapid reviews on TR practices across multiple disciplines (e.g., psychology and neuropsychology, physiotherapy, occupational therapy), surveys and focus groups to capture the experiences, challenges, and needs of clinicians, patients, and caregivers, and partnerships with stakeholders to establish guiding principles and create support tools. This project is led by a team of twenty-eight researchers across Canada specializing in several disciplines including psychology, neuropsychology, physiotherapy, occupational therapy, and speech therapy.
Methodology
We employed a rapid review approach, which is an accelerated form of evidence synthesis that streamlines the systematic review process by simplifying or omitting specific methods. While systematic reviews offer the most rigorous form of evidence synthesis, they can be time-consuming and resource-intensive, making them less suitable for fast-evolving fields like TR. 42 Rapid reviews maintain core systematic principles but narrow the scope to deliver timely, actionable findings. This process supports efficient evidence synthesis for stakeholders. This review aims to offer up-to-date and contextualized scientific and ethical guidance to enhance the integration of high-quality TR services into clinical practice. Full methodological details are available in a published protocol. 43 This review is reported according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 statement 44 (see PRISMA checklist in supplemental files).
Search strategy and eligibility criteria
The search process for this rapid review was designed by an experienced health sciences librarian in collaboration with the research team, following the PICOTSS framework. Search terms included synonyms and keyword variants to identify articles related to virtual care (e.g., virtual care, telehealth, online health), psychology and neuropsychology (e.g., psychology, neuropsychology, psychologist), and rehabilitation (e.g., rehabilitation, physical therapy, telerehabilitation). Search terms were combined with Boolean operators and adapted to the indexing vocabulary of the three comprehensive databases where the search was conducted (Medline, CINAHL, and EMBASE), selected for their broad coverage of health literature related to TR. Searches were conducted in July 2022 (for reviews) and May 2023 (for original articles). The included studies were assessed for risk of bias in relevant outcomes, following guidelines from the Cochrane Rapid Reviews Methods Group.45,46
Inclusion and exclusion criteria.
Data screening and extraction
Data screening and extraction were performed by two independent reviewers (authors DMG and JB) using the online systematic review and extraction software Covidence, while discrepancies were resolved through discussion. After identifying reviews and articles through keyword searches, data screening against the eligibility criteria involved three main steps: 1) title and abstract screening, 2) full-text screening, and 3) extraction of data from the included articles into a customized data extraction spreadsheet developed by author JS and adapted by authors DMG and JB based on the framework used for the series of rapid reviews and tailored to the needs of the psychological and neuropsychological fields. Key characteristics of each included study (title, authors, publication year, study type, and other characteristics extracted) are presented in the supplementary material (Supplemental Table 1). Data were then analyzed by the reviewers for overarching themes in characteristics of interest, including 1) the field of practice, 2) clinical features (e.g., number of participants, patient population, technology and tools used, outcome measures, frequency and length of the intervention), 3) study objectives and findings, 4) limitations, and 5) ethical and equity-related considerations. Author JB conducted data extraction for the review articles and author DMG conducted data extraction for the original articles. To ensure accuracy and completeness of the extraction process, 10% of the articles were cross extracted by both authors, and disagreements were resolved through discussion. Data collection and analysis were guided by the Equity-Based Framework for Implementation Research, 48 the Quadripartite Ethical Tool, 49 and the Consolidated Framework for Implementation Research. 50 Moreover, the PROGRESS-Plus framework was employed to identify potential inequities in TR. 51 This framework examines dimensions such as place of residence, ethnicity, culture, language, occupation, gender or sex, religion, education, socioeconomic status, social capital, age, disability, and sexual orientation.
In addition to predefined extraction categories, ethical and equity considerations were noted not only when drawn from the study’s explicit content, but also when inferred from contextual information interpreted by our team as ethically relevant, even when not labeled as such by the study authors. Given the focus on ethical and equity dimensions during data extraction, such omissions were flagged as relevant concerns. These elements were identified inductively during the data extraction process and discussed among reviewers. No predefined checklist or appraisal grid was used for this process. For an ethical or equity consideration to be regarded as “not reported”, we verified that it was absent from all sections of the article, including the introduction, methods, results, and discussion.
Data analysis and synthesis
The included articles were analyzed using a narrative synthesis approach to categorize and summarize data, a process that facilitated the organization of findings. We organized findings into themes and categories and conducted subgroup analyses to examine variations and similarities across disciplines, patient populations, settings, and TR characteristics. For example, reviews and original articles were analyzed separately. Additionally, separate categories were created for articles related to COVID-19 and oncology patients due to the distinct patient populations and substantial volume of literature. This analysis provided insights into factors influencing TR practices, helping to identify best practices and areas for improvement.
Results
Search results
The initial literature search identified 566 reviews and 2,751 original articles, which were exported to Covidence for screening and data extraction. After excluding duplicates, 561 reviews and 2,427 original articles were screened for eligibility by two independent reviewers. 475 reviews and 1,969 original articles were excluded after title and abstract screening, and 87 and 376, respectively, were excluded after full-text review (e.g., psychology or neuropsychology was not the primary focus; the study was not related to rehabilitation or TR; the study lacked physical rehabilitation components). Ultimately, 16 reviews and 82 original articles that met the eligibility criteria were included for data extraction. The PRISMA flowcharts below outline the study selection process for both reviews and original articles (see Figures 1 and 2). Prisma flow chart of the study selection process for review articles. Prisma flow chart of the study selection process for original articles.

Study design
Review articles included systematic reviews and meta-analyses (n = 10), literature reviews (n = 3), narrative reviews (n = 2), and a scoping review (n = 1). Original articles included randomized controlled trials (n = 37), single-arm trials (n = 16), mixed-methods studies (n = 9), observational studies (n = 7), cohort studies (n = 3), and other designs (n = 10 including a participatory study, an intervention development study, a discrete choice study, a perspective study, a descriptive exploratory study, a clinical case report, a quasi-experimental study, an open pilot study, and a preliminary study).
Field of practice
The main fields of practice in the included articles were psychology (n = 77), neuropsychology (n = 11), or both (n = 10). Articles also addressed other practices (n = 21) such as occupational therapy, physical therapy, speech and language therapy, and psychiatry.
Health conditions
Included studies had participants diagnosed with conditions such as neurological disorders (n = 29; e.g., multiple sclerosis, stroke, traumatic brain injury), pain disorders (n = 12; e.g., fibromyalgia, chronic pain), cardiovascular conditions (n = 10; e.g., hypertension, coronary artery disease, heart failure), cancer (n = 15; e.g., prostate, breast, skin cancer), COVID-19 (n = 12; e.g., confirmed COVID-19 cases, hospitalization following COVID-19 infection, long COVID) and other mixed diagnoses (n = 16; e.g., kidney failure, scoliosis, disorder of gut-brain interaction).
Technology
Original articles used synchronous interventions (n = 28), asynchronous interventions (n = 20), or a combination of both (n = 34). All review articles (n = 16) included studies using various TR modalities, including synchronous and asynchronous interventions. Synchronous interventions included interviews, psychological and neuropsychological assessments, and education via videoconferencing platforms, while asynchronous interventions were mainly delivered through web-based applications providing exercises and educational material, or through text messages and emails communication with healthcare providers.
Ethical concerns
Ethical concerns highlighted by the authors of the included studies were examined, along with potential ethical issues identified by our team (Figure 3 and Table 2). Articles were analyzed not only for ethical issues, but also for examples of positive ethical practices. Prominent ethical dimensions included privacy, confidentiality, burden of care, and quality and accessibility of patient-clinician relationships. First, privacy concerns were identified in ten articles, including challenges in maintaining privacy during home-based interventions, particularly for those with no access to a private or distraction-free environment. Positive practices included providing participants with a private space when none was available at home. Second, confidentiality concerns were identified in eighteen articles, focusing on safeguarding patient data and the need for secure methods of digital data collection and storage. Third, burden of care was identified as a potential issue in ten articles, which discussed the increased responsibilities placed on caregivers (such as reliance on family members to support access to online intervention platforms), as well as potential benefits of TR in alleviating responsibilities (such as facilitating communication and offering remote support). Fourth, concerns about the quality and accessibility of patient-clinician relationships were emphasized in eight articles, including difficulties maintaining therapeutic relationships in a remote setting, such as lack of face-to-face interactions and limited support for building patient-clinician connections. Number of studies including ethical aspects. Ethical concerns and examples in included studies.

Equity concerns
Equity concerns raised by the authors of the included studies were explored across multiple dimensions, along with those identified by our research team (Figure 4 and Table 3). Articles were screened for equity issues, as well as examples of positive practices. Prominent equity dimensions included access to care, digital literacy, and socio-economic disparities. First, access to care was identified as an equity issue in fourty-nine articles. This aspect highlighted the influence of geographic location (n = 15), socioeconomic status (n = 9), and health condition (n = 11) regarding access to TR services. TR was identified as a factor that may amplify social and cultural disparities because it requires adequate equipment and technological literacy. Second, digital literacy was identified as an equity concern in fourty-five articles. Digital skills were often required as an inclusion criterion to participate in the study; even when this was not the case, participants with low digital literacy frequently dropped out or faced technological difficulties. Third, sex (n = 41) and ethnicity (n = 15) were identified as potential equity issues, with an imbalance between male and female participants (n = 26 articles with substantially more females, n = 15 articles with substantially more males) and with predominantly white participants. These demographic imbalances limit the generalizability and applicability of findings across broader, more diverse populations. Number of studies including equity aspects. Equity concerns and examples in included studies.

Discussion
This rapid review explored psychology and neuropsychology practices in the context of telerehabilitation, with a particular focus on ethical and equitable considerations. The review included 16 reviews and 82 original articles that met the eligibility criteria for data extraction and analysis. Psychology TR interventions accounted for 79% of the included studies, while neuropsychology TR interventions represented 11%, with the remaining 10% addressing both. Studies addressed various health conditions, including neurological disorders, pain disorders, cancer, COVID-19, cardiovascular disorders, and other conditions. Ethical issues were identified across multiple dimensions, including privacy, confidentiality, burden of care, and the quality of patient-clinician relationships, while equity concerns related to access to care, digital literacy and demographic representation. Results highlight the disproportionate impact of ethical and equity issues on vulnerable populations, reflecting barriers to both service delivery and patient outcomes. While some of these issues were explicitly acknowledged by the authors of the studies, others were identified by our team, suggesting that many challenges remain underexplored in the literature, and other unidentified considerations might be relevant.
Ethical considerations
Ethical considerations need to be acknowledged to mitigate risks and ensure the effectiveness of TR. While no perfect solution exists to address them, raising awareness of the potential limitations and risks of TR can help safeguard both providers and patients (Guy et al., 2021).
First, privacy issues were identified as key concerns, as TR interventions often require access to a distraction-free environment, potentially creating barriers for individuals sharing a living space without access to a private room, either compromising their privacy or preventing them from participating altogether. This challenge, while prevalent in TR more generally, 67 is particularly acute in telepsychology and teleneuropsychology, where assessments often demand strict environmental control to ensure reliability and validity. 29 Strategies to address these issues include raising awareness among research and clinical teams 52 and providing participants with a private space when necessary. 68
Second, confidentiality concerns were highlighted through examples of good practice, such as the use of secure internet platforms to maintain confidentiality of patient data 69 and staff training emphasizing ethical practices and the handling of protected health information. 70 These concerns echo across various fields of TR, including occupational therapy and physical therapy, where secure digital platforms and adequate staff training are emphasized to maintain ethical standards. 8 However, the lack of reporting of confidentiality issues underscores a potential gap in transparency. For example, other risks include unauthorized access or misuse of personal data, which would not be reported in the articles.
Third, burden of care concerns were highlighted since some studies require the presence or active involvement of caregivers in the intervention. For instance, caregivers are often required to assist with technical issues, digital platform navigation, or questionnaire completion,56,57 potentially increasing their responsibilities and preventing participation of patients whose caregivers are unavailable or facing competing demands. Conversely, TR has also been shown to decrease burden of care and reduce caregiver anxiety by improving communication at least in situations where direct contact with patients is restricted. These findings underscore the nuanced interplay of TR’s benefits and challenges, which may vary according to individual circumstances. Fourth, it has been shown that online interventions can strain the relationship between the patient and the clinician, with participants reporting feelings of disconnection or frustration due to a lack of human contact compared to face-to-face interventions.38,71 The relational loss caused by TR interventions was highlighted as a barrier to maintaining therapeutic relationships.56,62,72 These findings align with broader literature on telepsychotherapy, which states that videoconferencing can alter therapeutic relationships by fostering a sense of disconnection and making it more challenging to establish interpersonal connections.73,74
Equity considerations
Because disparities can exacerbate preexisting inequities affecting vulnerable populations, 75 it is important to raise awareness of potential equity issues of TR and work toward reducing them. For example, marginalized populations’ perspectives can be gathered on how to improve TR, provide digital support to people in difficulty, reduce bias, and advocate for policies to make TR more accessible. 76 TR, including but not limited to psychology and neuropsychology, is conceptualized and recognized as overcoming geographical limitations. However, findings suggest that it may inadvertently reproduce or even amplify disparities for patients living in underserved areas.
First, barriers affecting access to care were identified. Geographic barriers mostly affect participants living in remote areas due to limited access to stable, high-speed internet connection and devices required to participate in TR. These barriers could be exacerbated by in-person recruitment, while the inclusion of participants from diverse geographic locations, including both urban and rural areas, 77 was recognized as a more equitable approach. Socioeconomic disparities also seem to further exacerbate inequities, as individuals from lower-income backgrounds often lack financial resources to obtain adequate equipment and digital infrastructure. Efforts to address these inequities include the provision of TR information in various formats (e.g., written or audio formats)78,79 to meet participants’ health or educational needs. Lastly, health-related barriers were identified for individuals with physical or cognitive limitations: one the one hand, it was highlighted that patients feeling too unwell to participate or experiencing illness recurrence might not have enrolled in the studies, 80 and on the other hand, high-functioning patients might have competing demands leaving them insufficient time to participate. 61 Adaptation to patients’ needs, such as session length depending on the level of cognitive deficits, 81 was identified as an effort toward equitable practices. Collectively, these barriers demonstrate how TR can inadvertently amplify existing inequities in access to care. It is important to note that these concerns do not seem to be unique to TR in psychology and neuropsychology, as similar issues have been reported in multiple areas of telemedicine. 82 Moreover, most articles raising concerns about access to care were identified by our research team rather than by the study authors, indicating that access issues are often overlooked.
Second, digital literacy was a significant equity challenge, either as an explicit inclusion criterion or implicit expectation: even when inclusion was attempted, low technological skills could lead to drop out of the study. 83 This can inherently disadvantage populations with limited technological familiarity such as older adults and people with limited education, which are populations already underserved by healthcare systems. These findings underscore the importance of deploying strategies to bridge this digital divide, such as technological support and user-friendly interfaces.
Third, demographic factors such as sex and ethnicity were found to be important equity considerations. Identified studies presented skewed participant demographics, such as lack of representation of diverse racial and ethnic groups, and an imbalance between female and male participants, therefore limiting the generalizability of findings and raising concerns about the applicability of interventions to diverse populations. Although some authors acknowledged sex (27%) and ethnicity (60%) imbalances, these issues remain important. To address these disparities, studies could adopt inclusive recruitment strategies to ensure representation across diverse demographic groups and analyze outcomes by sex and ethnicity to understand differential impacts of interventions.
Practical recommendations for TR research, policies, and practices
Our findings lead to several practical recommendations to support the ethical and equitable implementation of TR. This review underscores the importance of recognizing and proactively addressing ethical concerns related to patient privacy, data confidentiality, caregiver burden, and potential disparities in access to care and digital literacy. Key recommendations include providing funded equipment to individuals lacking personal access; establishing community-based access points to improve access to telemedicine services; implementing shared decision-making frameworks to assess, inform, and compensate for inequalities such as low of digital literacy and restricted access to care; co-designing adapted TR models that consider the needs of individuals with culturally and linguistically diverse backgrounds; and offering targeted training for clinicians to minimize privacy and confidentiality risks and promote high-quality patient-clinician relationships. These recommendations aim to support the development of structured TR services that promote ethical care delivery and reduce equity gaps.
This rapid review is part of a broader pan-Canadian initiative aiming to inform ethical, equitable, and evidence-informed TR policy and practice. While this study is embedded in a Canadian initiative, the ethical and equity considerations it addresses are broadly applicable across health systems, especially because this review included international literature and was not restricted to Canadian studies. Moreover, our findings and recommendations align with the World Health Organization and International Telecommunication Union global standard for accessibility of telehealth services. 84
Limitations
We recognize that the rapid review format, by design, is inherently less rigorous than a systematic review, potentially excluding relevant studies. In particular, the exclusion of grey literature limits the comprehensiveness of our findings and could have provided valuable insights. These decisions were made because of practical constraints, including the sheer volume of literature and time limitations to provide efficient and actionable evidence on this emerging topic.
The inclusion of reviews (from 2010 to 2020) and original articles (from 2020 to 2023) through different time periods could have led to overlooked information. For instance, reviews summarize broader trends but may lose the contextual richness of original articles, particularly regarding ethical and equity considerations in original studies.
Many included articles lacked standardized reporting of ethical and equity considerations. This required interpretive judgment from our research team during data extraction. Ethical and equity considerations that were not explicitly discussed by the original authors were identified and interpreted by our team based on the context of the study rather than being explicitly reported by study authors. While this approach allows for the recognition of relevant underreported elements, it also introduces subjectivity, as these themes were noted without a formal checklist.
Finally, as the field of telerehabilitation continues to evolve rapidly, some technologies, practices, or implementation barriers may have shifted since the time of publication. This poses a risk that some findings may already be outdated or incomplete in light of ongoing developments.
Conclusion
As TR continues to evolve, it is important for clinicians, health organizations, and policymakers to collaborate to create a framework adapted to promoting ethical and equitable TR services. This review highlights the emerging need for robust and clear guidelines to address the growing ethical concerns related to TR delivery and outcomes. It is important to ensure that clinicians are trained to provide high-quality TR services and that resources, such as digital literacy training and tailored interventions, are available for patients and caregivers. More research is needed to address the gaps in ethical and equitable care delivery within psychology and neuro-psychology TR, such as the long-term outcomes and practical strategies to address these challenges. The widespread adoption of TR demands careful consideration of ethical, cultural, and equity-related issues. By proactively addressing these challenges, TR can be a powerful tool for enhancing accessibility and providing high-quality rehabilitation services.
Supplemental material
Supplemental material - Paving the road for more ethical and equitable policies and practices in telerehabilitation in psychology and neuropsychology: A rapid review
Supplemental material for Paving the road for more ethical and equitable policies and practices in telerehabilitation in psychology and neuropsychology: A rapid review by Dorothée Morand-Grondin, J. Berthod, J. Sigouin, S. Beaulieu-Bonneau, D. Kairy in Health Informatics Journal.
Footnotes
ORCID iDs
Ethical considerations
Given the nature of this article (rapid review involving no human or animal participants), no ethical approval was needed to conduct the study. However, this rapid review is part of a broader pan-Canadian study involving surveys, rapid reviews, and focus groups. This study was approved by the Comité d’éthique de la recherche en réadaptation et en déficience physique of the University of Montreal (project number MP-50-2022-1610, approval form number F9 - CCSMTL-10171).
Author contributions
Dahlia Kairy and Jennifer Sigouin developed the protocol.
Dorothée Morand-Grondin and Jeanne Berthod led the rapid review (data screening and extraction).
Dorothée Morand-Grondin wrote the first draft and subsequent versions of the manuscript.
Jennifer Sigouin, Simon Beaulieu-Bonneau and Dahlia Kairy provided editing and comments for the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is funded by the Canadian Institutes of Health Research – Canadian Medical Association (project grant #463290) and the Réseau québécois de recherche en adaptation-réadaptation (REPAR, project grant #178354).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Registration information
This review was not registered.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.