
Abstract
Background
Data quality encompasses completeness, accuracy, integrity, timeliness, and confidentiality. In many low- and middle-income countries, including Somalia, data from RHIS are often poor, limiting their usefulness for public health actions. This study assessed the quality of RHIS data and associated factors among public health facilities in the Banadir region, Somalia.
Methods
A facility-based cross-sectional study was conducted from October to December 2024 across 36 public health facilities using a multistage sampling approach. Data were collected through document reviews, interviews, and observations using PRISM-based standardized tools. Data were analyzed in SPSS version 27 after checking logistic regression assumptions. Data quality was assessed by the dimensions of accuracy (≥80%), completeness (≥85%), and timeliness (≥85%). Bivariable and multivariable logistic regression analyses identified associated factors.
Results
A total of 398 healthcare workers (59.5% female) participated, yielding a 98% response rate. Overall, good-quality data were observed in 65.3% of departments. Departments in health centers were 2.7 times more likely to report good-quality data than hospitals. Feedback, refresher training, and user-friendly reporting formats were significantly associated with better data quality.
Conclusion
Data quality across the three dimensions was scored at (65.3%). Strengthening supervision, feedback, and context-specific training can improve data reporting and management.
Background
Data quality is a multidimensional concept that encompasses completeness, accuracy, integrity, precision, timeliness, and confidentiality. 1 Reliable and timely data are crucial for monitoring population health, evaluating system performance, and guiding evidence-based policy and program decisions that support the achievement of health-related Sustainable Development Goals (SDGs). 2 A well-functioning health information system aims to routinely generate quality data that are accurate, consistent, and timely for effective health system planning and management. 3
The Routine Health Information System (RHIS) is one of the six essential building blocks of health systems in low- and middle-income countries (LMICs), and serves as the primary mechanism for generating and using health data to strengthen other system components. 4 It provides a framework for decision-making across multiple areas, including policy development, governance, regulation, human resource planning, education and training, service delivery, and system support.1,5 In low- and middle-income countries (LMICs), routine health data represent the primary source of information for shaping health policies, monitoring programs, and improving service delivery. 6
However, in many LMICs, RHIS remain fragmented and poorly coordinated, with widespread concerns regarding the quality, accuracy, timeliness, and completeness of their data. 7 Weak data management, limited supervision, and inadequate communication practices have been widely reported in developing countries, contributing to poor RHIS data completeness and timeliness. 8 The magnitude of this problem is significant, as studies from across Africa indicate data quality performance ranging from 34% and 72%, revealing substantial deficiencies. 9 This poor quality directly leads to the underutilization of data in public health facilities, undermining effective planning and management. 10
Similar challenges have been reported across African countries, where studies assessing routine health information systems have documented substantial variations in data accuracy, completeness, and timeliness. The accuracy of routine data was found to be 74%, 1 76%, 11 79% 12 of studies conducted in West Gojjam Zone, northwest Ethiopia, Hadiya Zone of Ethiopia and Nigeria, respectively. Content completeness rates were observed in studies conducted in West Gojjam Zone (70%), Hadiya Zone (83.2%), Addis Ababa (96%), Harare Zone (93%), and Rwanda (98%).1,4,13,14 In the neighboring country of Ethiopia, the data quality is problematic for many indicators, with data quality falling below the national anticipation of 80%. 4 Data completeness, accuracy, and timeliness varied across different regions of the country, ranging from 33% to 78%.4,15
However, studies on HIS data quality are limited in number and scope. 16 Most studies have used small-scale facility assessments and did not investigate technical or behavioral factors influencing data quality. 16 Where such factors have been examined, research indicates data quality is affected by a range of technical, behavioral, and organizational factors, including staff knowledge and expertise, 4 negligence in keeping data quality and data manipulation, 17 staff motivation,17,18 user-friendliness of reporting tools, standardized indicators, 19 DQA training, 20 feedback, 19 supervision, 21 staff responsibility, 22 and HIS data use. 23
In Somalia, the Health Management Information System (HMIS) was established between 2011 and 2012. 24 During this period, multiple data collection systems were implemented to gather information from healthcare facilities, many of which were managed by non-governmental organizations. 24 In 2017, Somalia rolled out the District Health Information Software 2 (DHIS2) across all districts, marking a major step toward improving its HIS system, and between August 2020 and December 2021, the HIS tools underwent a significant revision. 25 Workshops to review proposed indicators and data collection tools were conducted with the Ministry of Health (MOH) and stakeholders in Mogadishu, Hargeisa, and Garowe, aiming to refine draft tools and offer feedback to Oslo university experts. 26 District Health Information Software, version2 (DHIS-2), an adaptable and open-source platform with a user-friendly interface, was developed by the University of Oslo and is widely adopted for managing routine health information in more than 70 low- and middle-income nations (LMICs). 27
Despite these developments, limited empirical evidence exists regarding the quality of data produced by routine health information systems in Somalia. 28 Most available reports focus on system implementation or digital rollout rather than assessing data accuracy, completeness, or timeliness. To justify the evidence gap, we searched peer-reviewed publications and, in addition, grey literature and preprints (e.g., institutional reports, theses/dissertations, conference abstracts, and preprint servers). This approach ensured a comprehensive review of available literature, as some relevant studies may not have been formally published yet.
This study, therefore, aimed to assess the data quality of routine health information systems and associated factors among departments in public healthcare facilities, Banadir Region, Somalia. This study contributes to the field of health informatics by highlighting how routine data quality challenges in conflict-affected, low-resource settings such as Somalia, can undermine decision-support systems. It provides practical, system-level recommendations to enhance digital health reporting and strengthen the performance of health information systems.
Methods and materials
Study design and study area
A facility-based, quantitative cross-sectional study was conducted from October to December 2024 in public healthcare facilities, Banadir Region, Somalia. The initial participants consisted of 403 healthcare workers drawn from 36 public health facilities located in eight randomly selected districts: Wadajir, Kahda, Daynile, Dharkenley, Abdiaziz, Hamarweyne, Boondheere, and Wardhigley.
The study was conducted in the Banadir Region, one of Somalia’s 18 administrative regions, which serves as the country’s political, economic, and cultural center. It includes Mogadishu, the national capital city. It is geographically bordered by the Indian Ocean to the east and south, Lower Shabelle Region to the west and southwest, and Middle Shabelle Region to the north.25,28 It is composed of 20 administrative districts which are located in an entirely urban area. The study focused on eight of these districts, chosen to represent a diverse range of healthcare environments. Banadir is home to 2,846,043 people, accounting for 13.4% of Somalia’s total population, with a gender distribution of 49.3% male and 50.7% female. 29
This region has the highest concentration of healthcare facilities in Somalia, with a total of 205 health facilities. 30 These include a range of national, regional, and district hospitals, specialty hospitals, health centers, and private clinics. In addition, about 40% of these facilities are privately owned, reflecting the region’s significant private healthcare sector.30,31 Banadir Region also boasts the highest density of healthcare workers in Somalia, with approximately 17 core health workers (including physicians, nurses, and midwives) per 10,000 population. 30
Study population
The study population comprised departments within the selected public health facilities whose heads had at least six months of experience in their respective roles. Departments that were on leave, absent during data collection, or declined to participate were excluded from the study.
Sample size determination
The sample size for this study was determined using the formula for a single population proportion. Since no prior study on RHIS data quality was available in Somalia, a 50% proportion (p = 0.5) was assumed as a conservative estimate to yield the maximum possible sample size. The use of a 50% proportion (p = 0.50) for sample size calculation is a widely recommended approach when reliable prevalence estimates are unavailable, as it maximizes the statistical efficiency for a given margin of error. This method has been commonly applied in health system studies with no prior prevalence data.32,33 A 95% confidence level and a 5% margin of error were applied. Additionally, a 5% non-response rate was included to ensure sufficient representation despite potential participant dropout. Based on these assumptions, the sample size calculation followed the formula:

n_final= 384 + non-response rate (5%) is equal to 403. Therefore, the final sample size used in this study was 403 participants. The sample size of 36 health facilities (33 health centers and 3 hospitals) was selected as a census of all public health facilities in the chosen districts to minimize selection bias. Given the logistical constraints and the availability of all eligible public health facilities, this number was deemed sufficient for a robust analysis of data quality across departments. The sample size was distributed across health facilities using unequal proportional allocation. Although a multi-stage cluster sampling technique was employed to ensure geographic representation, a design effect was not applied, consistent with previous RHIS data quality assessments in low-resource settings such as Tanzania. 10 In these field-based studies, sample sizes were primarily guided by feasibility and available resources, rather than theoretical adjustments for clustering.
Sampling procedure
A multistage cluster sampling method was used across Banadir districts. Health facilities were defined as public hospitals and public health centers, the only public facility types in the selected districts. After selecting districts, we included all eligible public facilities (a census) to minimize selection bias, yielding 36 facilities (33 health centers, 3 hospitals). Participant sample size was allocated unequally by the number of health personnel per facility (Figure 1). Schematic illustration of the sampling procedure, 2024 (n = 403).
Variables and measurements
Dependent variable
The dependent variable was data quality (Good/Poor). Data quality was computed using three dimensions accuracy, completeness, and timeliness. For each facility, these dimensions were measured, summed, and averaged. A facility was classified as having good data quality (Yes) if it met all three minimum thresholds: ≥80% accuracy, ≥85% completeness, and ≥85% timeliness. Facilities not meeting these criteria were classified as having poor data quality (No).
Independent variables
The independent variables were categorized into three groups: Technical factors: Presence of standard indicators, report formats, and trained personnel able to fill formats. Organizational factors: Training, feedback, supervision, computer availability, internet access, rewards, engagement in HIS activities, performance review meetings, and data use. Behavioral factors: Motivation, attitude, data manipulation for competition, negligence, and data quality checking skills.
Because respondents represented different departments within each facility, the technical, organizational, and behavioral characteristics were assessed at the department level. 34 Since the data were collected from various departments, some variability in responses was expected due to differences in workflows, roles, and staff familiarity with RHIS practices. This variability was considered during data analysis, and departmental-level analysis was employed to capture these differences. However, facility-level data quality was assessed using routine reports and records, which helped minimize any bias introduced by department-level variations.
Operational definitions
To assess HMIS data quality, three key dimensions like accuracy, completeness, and timeliness were measured, summed, and averaged to generate data quality.13,35
Data accuracy is the extent to which reported data correspond to the original records in source documents or registers. It was evaluated by comparing figures recorded in source documents or registers with those reported to higher levels. A 10% margin of error was used to interpret the results: a ratio below 0.90 indicated over-reporting, between 0.90 and 1.10 was considered acceptable, and above 1.10 signaled under-reporting. 36
Completeness is the degree to which required data fields in reporting forms or registers were filled in. Completeness was evaluated by examining the number of cells in the register were left blank without a “zero” entry. If 90% or more of the cells were properly filled out, the report was considered complete.36,37
Good Data Quality is defined as meeting the minimum acceptable thresholds across all three dimensions. Data was considered to be of good quality if it met all three criteria: at least ≥ 80% accuracy, ≥ 85% completeness, and ≥ 85% timeliness. 6
Report Timeliness is the extent to which data reports were submitted on time, as defined by the reporting deadline. Determined by the number of reports submitted by the facility head before the deadline, the end of each month 38 divided by the total number of expected reports.
A data item: A single health indicator (for example, the number of ANC 4 visits, malaria cases, or vaccines) is a chosen routine health indicator used to measure the accuracy of reported data. 34
Data quality measurement
The three dimensions of data quality assessed in this study accuracy, completeness, and timeliness were selected based on internationally recognized frameworks. Both the World Health Organization WHO-DQR Toolkit39,40 and the Performance of Routine Information System Management (PRISM) framework recommend these as core indicators for evaluating the performance of RHIS, particularly in low- and middle-income countries. 41
To assess accuracy, a total of 36 health facilities were included. According to the Somali National HIS Strategic Plan, reviewing six to seven data elements from each health facility provides a reliable measure of data accuracy. 37 Accordingly, six indicators (Pentavalent 3, BCG, ANC4 visits, deliveries, pneumonia, and malaria) were selected because they are included in Somalia’s national HIS core indicator list for DHIS2 reporting28,35 and are also among the core facility indicators recommended by the WHO DQR Toolkit. 42 Completeness and timeliness were evaluated using a 90% threshold, based on filled report fields and timely submissions, respectively.
Data collection instrument
A structured self-administered questionnaire was adapted from the validated PRISM assessment tools (version 3.1; see Additional file 1),16,41 with minor contextual modifications to collect quantitative data. It included sections on sociodemographic characteristics of department heads, and the organizational, behavioral, and technical factors associated with the quality of routine health information system data. In addition, observations, interviews, and document reviews guided by a standardized observation checklist were conducted to assess data quality at the departmental level. Data were collected from the respective department heads or designated representatives to ensure accurate and comprehensive responses.
Data collection procedure and data quality control
The instruments were pretested in a public health facility outside the study area using 10% of the total sample (n = 40). Based on the pretest results, adjustments were made to improve item clarity, and question sequencing. Tools were initially developed in English, translated into Somali to ensure conceptual equivalence, and then back-translated into English to verify accuracy.
A total of eight health professionals with prior data collection experience and training in data management, along with two HIS monitoring team members, were recruited from districts outside the study area to minimize potential bias. The data collectors and supervisors underwent two days of intensive training covering study objectives, data collection procedures, ethical principles, and confidentiality. The training also emphasized neutrality, accuracy, and strict adherence to data verification procedures.
Data were collected in person through on-site visits to the selected health facilities. At each visit, the study objectives were explained, confidentiality was assured, and written informed consent was obtained from facility heads and respondents. Self-administered questionnaires were completed privately to minimize response bias, while direct observation and document review were conducted to verify responses.
Supervisors conducted daily reviews of completed questionnaires and checklists to verify completeness, consistency, and accuracy. Immediate feedback was provided to data collectors to correct any omissions or errors. In addition to these reviews, regular checks were performed to ensure that data entries matched the original records, with any discrepancies addressed immediately. Incomplete tools were returned the same day for correction during the facility visit. Prior to analysis, all data were checked for completeness, cleaned, and examined for statistical assumptions relevant to the analytical models.
Data processing and analysis
The collected data were cleaned in excel, and then exported to SPSS version 27 for coding and statistical analysis. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to summarize key variables, participant characteristics, and departmental data across public health facilities. Results were presented using tables and figures.
The dependent variable (overall data quality), was computed using three dimensions of accuracy, completeness, and timeliness as outlined in the WHO Data Quality Review Toolkit. Each dimension was scored as a percentage, and health facilities achieving an overall (accuracy, completeness, and timelines) score of 90% or above across all three dimensions were classified as having good data quality, whereas those scoring below this threshold were categorized as having poor data quality.
Because the dependent variable was dichotomous (good vs. poor data quality), binary logistic regression was employed for inferential analysis. Initially, bivariate logistic regression was conducted to identify variables associated with data quality. Variables with a p-value less than 0.25 in the bivariate analysis were considered for inclusion in the multivariable logistic regression model. The multivariable model was then used to control for potential confounding and to determine the independent predictors of routine health data quality. Results were reported using adjusted odds ratios (AORs) with 95% confidence intervals (CIs), and statistical significance was set at p < 0.05.
Prior to the final analysis, model assumptions were verified. Multicollinearity was assessed using the Variance Inflation Factor (VIF), applying a cutoff value of 10, and no multicollinearity was detected among the independent variables included in the model. The Hosmer–Lemeshow goodness-of-fit test was used to evaluate model fitness.
Results
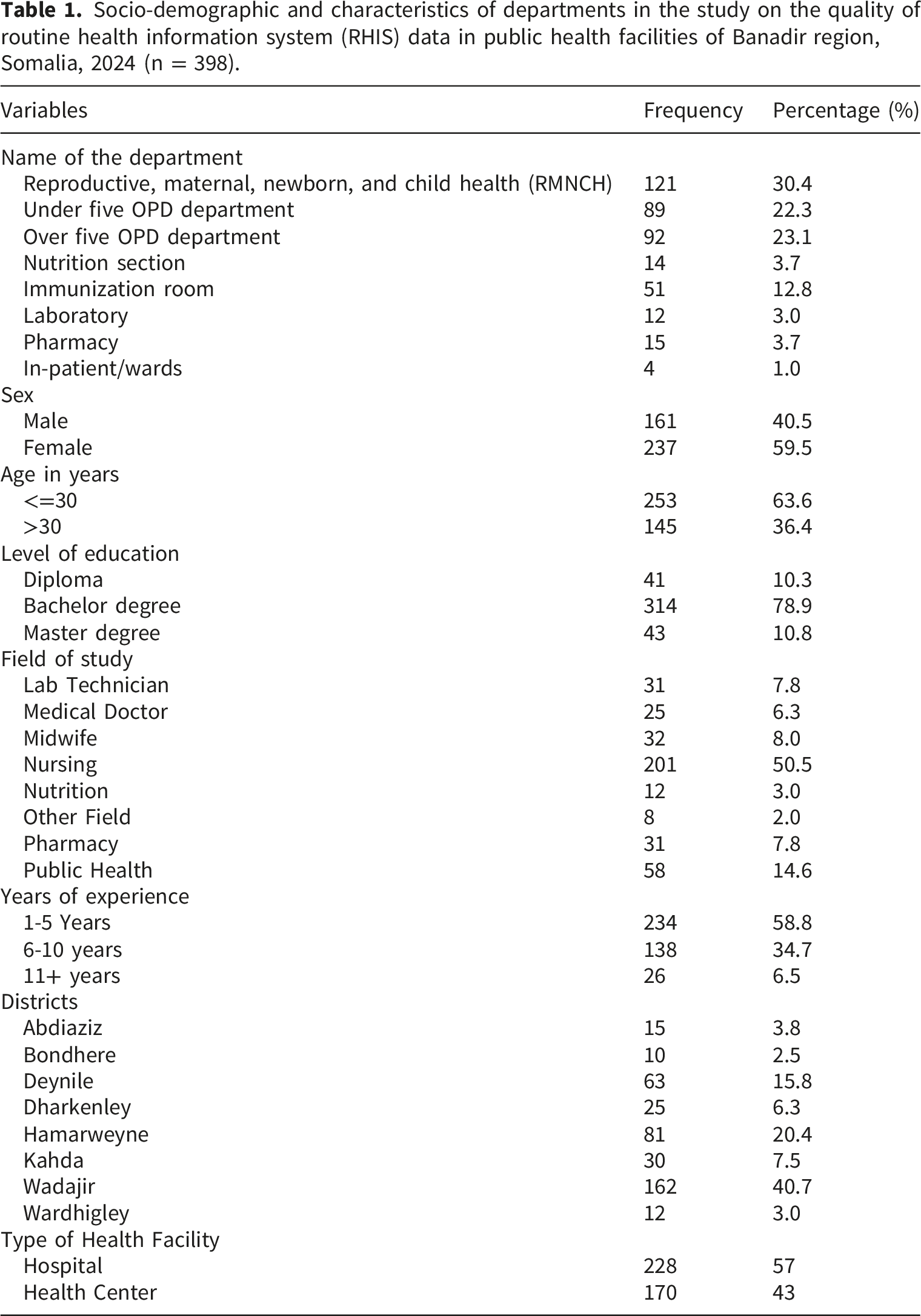
Sociodemographic characteristics of the departments in public health facilities in Banadir region
Socio-demographic and characteristics of departments in the study on the quality of routine health information system (RHIS) data in public health facilities of Banadir region, Somalia, 2024 (n = 398).
Organizational factors
Organizational factors influencing the quality of routine health information system (RHIS) data among departments in public health facilities of Banadir region, Somalia, 2024 (n = 398).

Technical and behavioral level factors
Technical and behavioral factors influencing the quality of routine health information system (RHIS) data among departments in public health facilities of Banadir region, Somalia, 2024 (n = 398).

Data quality level details
Data quality of accuracy
Out of the 398 departments for which data correctness was verified, 239 (60%) had accurate data, with hospitals exhibiting the lowest accuracy at 57% (Figure 2). Level of data accuracy among departments of public health facility types of Banadir region, Somalia, 2024 (n = 398).
Data quality of completeness
Out of 2,388 data elements reviewed for report content completeness, 1,630 (68%) were fully completed in the reporting forms. For registration content, only 49.4% of the 1,180 cases reviewed contained all the necessary information. Overall, the study found that 758 departments (32%) had incomplete data (Figure 3). Level of completeness of data among departments of public health facilities in Banadir region, Somalia, 2024 (n = 398).
Data quality of timeliness
In this study, reporting timeliness refers to the percentage of reports submitted by facility departments on or before the official reporting deadline (end of each month) out of the total number of expected reports. Regarding reporting timeliness, the study found that 161 (95%) of health center departments, and 222 (97%) of hospital departments were assessed (Figure 4). Level of data timeliness among departments in public health facilities of Banadir region, Somalia, 2024 (n = 398).
Overall data quality
Out of the participants assessed, 65.3% had good data quality. This included 52% of hospital departments and 48% of health center departments (Figure 5). Timeliness was highest at 96%, followed by accuracy at 60% and completeness at 55%. The level of overall data quality among departments of public health facilities in Banadir region, Somalia, 2024.
Multivariable Logistic Regression Analysis of Factors Affecting the Quality of Routine Health Information System Data in Public Health Facilities, Banadir Region, Somalia, 2024.
Multivariable logistic regression analysis of factors affecting the quality of routine health information system data in public health facilities, Banadir region, Somalia, 2024 (n = 398).
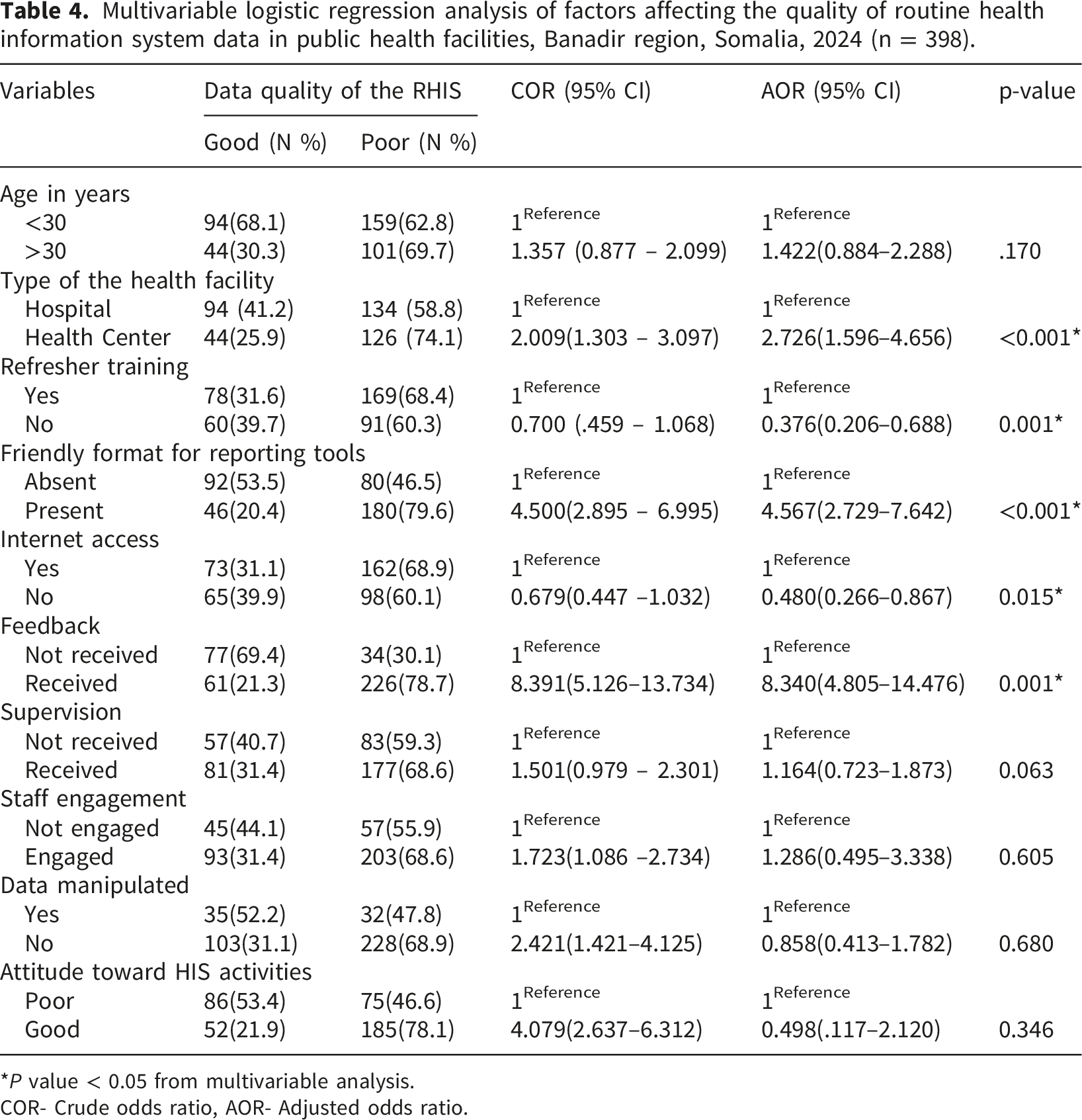
*P value < 0.05 from multivariable analysis.
COR- Crude odds ratio, AOR- Adjusted odds ratio.
Discussions
This study aimed to assess the quality of routine health information system (RHIS) data and the factors influencing it among public health facilities in Banadir region, Somalia, using the PRISM framework. The findings provide valuable insights into the technical, behavioral, and organizational factors affecting data quality in the region. Data quality in terms of accuracy and completeness were 60% and 55%, respectively. The data accuracy in this study was 60%, which is consistent with a study conducted in Ethiopia, where the accuracy was reported as 58.1%. 4 However, it is below the accuracy levels reported in other Ethiopian regions, such as 74% 1 in West Gojjam Zone, 76% 43 in Southern Ethiopia, and 89.4% 44 in Gofa Zone, Southern Ethiopia.
Somalia faces a unique challenge that contribute to the lower data accuracy observed in this study. Decades of conflict and political instability have resulted in a fragmented healthcare system with limited resources, directly impacting the accuracy of health data. The absence of comprehensive digital systems and standardized reporting methods exacerbates these issues. Health data collection in Somalia is largely manual, and the lack of adequate training for health workers leads to inconsistent and sometimes inaccurate data reporting. This challenge is compounded by the limited capacity for regular data audits and supervision.
While Somalia’s data accuracy is lower than more developed regions, it is still better than in certain Ethiopian settings, such as the 48% accuracy found in other areas. 45 This suggests that despite significant barriers, improvements in data accuracy are possible with targeted interventions, such as capacity-building, better supervision mechanisms, and gradual implementation of digital health solutions. In high-income countries like Denmark and the United States, RHIS accuracy and completeness consistently exceed 85% due to strong governance, digital integration, and accountability structures. 46 In contrast, Somalia’s fragmented administrative systems and limited digitization impede accurate reporting, resembling challenges observed in India’s less digitized regions. 47
Content completeness in this study (68%) was lower than that reported in other regions, such as West Gojjam (70%), Hadiya Zone (86%), Harari Zone (93%), and Rwanda (98%).1,4,13,14 The lower completeness, particularly in registration records, suggests that health workers often prioritize clinical care over data documentation due to heavy workloads and limited motivation. Similar challenges were observed in East Wollega, where lower registration completeness was attributed to time pressure and limited commitment to data recording. In contrast, countries like Denmark, the United States, and Canada, with electronic health record (EHR) systems, achieve completeness rates above 90% through automated data capture and standardized formats.46,48
The observed 96% timeliness in Banadir surpasses reported figures from Southern Ethiopia (88.42%) and Rwanda (90%),43,49 potentially due to the region’s compact geography and enhanced facility accessibility. In contrast, Uganda’s Kampala reported significantly lower timeliness rates (44% in 2020, 65% in 2021), 50 highlighting regional disparities. This study’s timeliness is consistent with the findings in Harari Region, Ethiopia (93.7%). 4 High-income countries like Canada and the United Kingdom maintain near-perfect timeliness through integrated digital systems. 48 These comparisons underscore the importance of infrastructure, system integration, and regional factors in determining the timeliness of health data reporting.
Our study found that 65.3% of departments have good levels of RHIS data quality, but deficiencies persist, leading to inaccurate analyses, weak service delivery, and ineffective decision-making. This may be due to a shortage of personnel responsible for data processing and management. The findings align with data from other developing countries, where data quality typically ranges from 34% to 72%. 9 However, they are lower than findings from Ethiopia (74%). 1 Our study is also consistent with studies reporting data quality of 51.35% 4 and 69.6%. 51
The departments in health centers were 2.7 times more likely to have good-quality data compared to those in hospitals. This is supported by findings from Ethiopia regions, where data quality was found to be better at health centers. 4 This may be attributed to the focused attention from the Ministry of Health and other stakeholders, including capacity-building efforts. Our study found that training and feedback were significantly associated with good-quality data. These findings align with a study conducted in Ethiopia, where trained staff and feedback were significantly associated with data quality, with Adjusted Odds Ratios (AOR) of 2.25 (95% CI: 1.08–4.69) and 2.48 (95% CI: 1.26–4.85), respectively.4,52 A recent scoping review also showed that combining feedback with other capacity-building activities contributes to data quality improvement. 21
Another predictive factor identified in our study was the format used for reporting. Departments with a -friendly reporting format were 4.5 times more likely to report high-quality data compared to those without such a format (AOR = 4.57, 95% CI: 2.73–7.64). This finding aligns with a study conducted in Dire Dawa, Ethiopia, 52 where departments with a friendly reporting format were 2.25 times more likely to achieve good data quality compared to those without (COR = 2.25, 95% CI: 1.18–4.31). Training enhances the understanding of Health Information System (HIS)-related activities and tools, increasing familiarity with essential HIS tools such as registers and reporting formats.
Although supervision was associated with data quality in the bivariate analysis, it was not significantly associated in the multivariate analysis in this study. This finding is consistent with a study conducted in the Harari region, Ethiopia, 4 where supervision was found to be associated with data quality in the bivariate analysis. However, it contrasts with a study conducted in Gurage Zone, Ethiopia, where supervision was significantly associated with data quality in both analyses. 25 One reason for this discrepancy is that, supervision is often more focused on identifying mistakes rather than offering constructive support. A more focused and supportive supervisory approach can significantly improve areas such as data recording, processing, analysis, reporting, and overall data quality management.
Policy implications and impact on health outcomes
Somalia’s health system has been deeply affected by decades of conflict, leaving it fragmented and under-resourced. Inadequate infrastructure, reliance on donor-driven mechanisms, and weak connectivity constrain RHIS performance. Health workers face high workloads, staff shortages, and limited incentives for accurate reporting. 53 These challenges, along with limited digitalization and weak governance, contribute significantly to deficiencies in RHIS data quality. Addressing these issues through targeted policy interventions can lead to substantial improvements in both data quality and health outcomes.
Institutionalizing RHIS training within national workforce frameworks will equip health workers with the skills to accurately collect and report data, improving data quality for informed decision-making and resource allocation, which directly enhances health outcomes. 28 A more skilled workforce will lead to more accurate data, helping providers identify health trends and improve service delivery. Strengthening supervision and mentorship will improve accountability in data reporting, ensuring high-quality data for better monitoring, targeted interventions, and improved health outcomes. 54 Expanding the use of digital tools like DHIS2 will streamline data collection, reduce errors, and provide real-time data, allowing quicker responses to health trends. 55 Strengthening national data governance through audits and performance management will ensure data accuracy and accountability, enabling better resource allocation and improved health services and outcomes. 56
Study strengths and limitations
This study provides valuable insights into RHIS data quality in the Banadir Region of Somalia. As the first of its kind in the country, it contributes important evidence to inform future public health initiatives. However, several limitations must be considered. The study was conducted only at public health facilities, which may limit the generalizability of the findings to all types of health facilities. The reliance on self-reported data introduces recall and social desirability biases, and non-response bias may have affected the results, particularly if facilities with lower data quality were less likely to participate. The lack of design effect adjustment and the use of the same questionnaire across facilities with different service types may have influenced the precision and contextual relevance of the findings.
Additionally, the cross-sectional design limits the ability to establish causal relationships between the factors examined and RHIS data quality. Furthermore, while the study was purely quantitative, it did not include qualitative data, which could have provided deeper insights into the behavioral and contextual factors influencing data quality, particularly in Somalia’s fragile health system. Lastly, the representativeness of the facility selection could be a limitation, as the facilities included may not fully capture the diversity of healthcare settings across the Banadir region.
Despite these limitations, the study provides a critical baseline for understanding RHIS data quality in Somalia and highlights areas for improvement in the health information system.
Conclusion
Data quality across the three dimensions was scored at 65.3%. Refresher training for healthcare professionals was inadequate, highlighting the need for context-specific training in data management and digital health tools. Health facilities should implement regular, localized training, while district health offices and the Ministry of Health should enhance supervision and feedback mechanisms to support continuous improvement. Factors like the type of facility, Internet access, and reporting tool friendliness were significantly associated to data quality. The Ministry of Health should prioritize improving digital infrastructure and Internet access to ensure health workers have the necessary tools. Development partners should support capacity-building efforts at the district and zone levels to enhance data reporting and management. Future research should use mixed-methods approaches to explore the behavioral and contextual factors influencing RHIS data quality in Somalia.
Supplemental material
Supplemental material - Data quality of routine health information systems and associated factors among public health facilities in Banadir region, Somalia: A cross-sectional study
Supplemental material for Data quality of routine health information systems and associated factors among public health facilities in Banadir region, Somalia: A cross-sectional study by Nor Haji Osman, Abdisalan Mohamed Roble, Ibrahim Mohamed Abdi, Abdiweli Mohamed Abdi, Aweis Ahmed Moallim, Osman Abubakar Fiidow, Abdirahman Mohamed Jimale, Jamal Hassan Mohamud, Abdikarim Abdi Adam, Abdirahman Ahmed Mohamud in Health Informatics Journal
Footnotes
Acknowledgements
We extend our sincere gratitude to the supervisors, data collectors, respondents, and the Banadir Regional Health Departments for their valuable contributions to this study.
Ethical considerations
This research has been approved by the ethics committee from the Ethical Review Board of the Somali National Institute of Health (Ref: NIH/IRB/58/DEC/2024). Before participation, all participants were fully informed about the study’s objectives, procedures, and potential benefits.
Consent to participate
Written informed consent was obtained from each participant prior to data collection. To ensure confidentiality, data were collected anonymously, with no identifying information recorded or disclosed.
Author contributions
NHO, AMR, and AMA conceptualized the study and designed the research methodology. They were responsible for data collection, data analysis, interpretation, and drafting the manuscript. OAF, AAM, and AAM conducted proofreading and provided interpretation of the results. AMJ, IMA, AAA, and JHM oversaw the overall research process. All authors read and approved the final version of the manuscript for submission
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.