
Abstract
Background
Influenza is often self-limiting but leads to avoidable emergency department visits. This study describes the development of inFLUence, an online self-administered tool for stratifying influenza-like illness risk.
Methods
The tool was developed using a user-centered design approach, informed by a systematic review of existing risk stratification tools. A prototype was iteratively refined across three rapid prototyping cycles with 18 participants and evaluated by seven clinical experts through an online survey.
Results
Across three testing cycles, nearly all participants (5–6 out of 6 per round) found the tool easy to use, understandable, useful, and effective. Feedback informed consensus-based adjustments at each iteration. Clinical experts rated the relevance of the proposed questions on a 9-point scale, with median scores ranging from 5 to 9, where 9 indicated extreme relevance. The final product is a bilingual, self-administered web application for individuals aged ≥5 months, providing personalized recommendations for users presenting with influenza-like illness, regardless of the underlying viral pathogen.
Conclusion
inFLUence is a promising digital tool that could enhance patient autonomy and support more efficient use of healthcare services.
1. Introduction
Influenza is an acute respiratory infection responsible for seasonal epidemics and occasional pandemics, representing a major cause of medical consultations. It is primarily caused by influenza A and B viruses, and more rarely by type C. 1 Transmission occurs through respiratory droplets, aerosols, and contact with contaminated surfaces. The incubation period is usually short, ranging from one to four days. Typical clinical manifestations include abrupt fever, cough, sore throat, myalgia, headache, chills, and marked fatigue.1,2 In most cases, the illness is mild and resolves spontaneously within seven to ten days, but serious complications such as viral or secondary bacterial pneumonia, acute respiratory distress, or decompensation of chronic conditions can occur.2,3 These complications particularly affect young children, older adults, pregnant women, and individuals with chronic diseases or immunosuppression, and the presence of comorbidities is a major predictive factor for poor outcomes.4–6
Beyond its clinical burden, influenza also poses a major economic challenge. In the United States, the annual cost has been estimated at more than 10 billion dollars in direct medical care and nearly 87 billion dollars in total.4,7–9 In Canada, influenza is responsible for more than 12,200 hospitalizations and 3,500 deaths annually, along with approximately 227,935 emergency department (ED) visits, making it one of the leading causes of hospital-based consultations.10,11 Periods of intense viral circulation exacerbate ED overcrowding, reducing the ability of healthcare facilities to respond effectively to patient needs. To optimize the resource management, health authorities encourage patients at low or moderate risk to practice self-management at home, thereby reducing avoidable contacts and viral transmission.12,13 However, many patients with influenza-like illness (ILI) struggle to judge the severity of their symptoms and the need for medical evaluation, leading both to unnecessary ED visits and, conversely, to delays in care for those truly at risk.
Several approaches have been proposed to address this challenge, including clinical prediction rules, nurse triage algorithms, electronic decision-support systems integrated into electronic medical records, and risk stratification models.14,15 These tools classify patients according to their likelihood of complications, thereby helping direct them toward the appropriate level of care.5,16 Yet most of them are designed for clinicians and rarely adapted for autonomous use by the public, especially across both pediatric and adult populations. 17
In this context, we developed inFLUence, a bilingual, self-administered online tool designed for both adults and children presenting with ILI symptoms, regardless of the underlying viral pathogen. Its originality lies in integrating pediatric and adult pathways within a single application, offering a user-friendly interface accessible to the public, and generating personalized recommendations based on symptoms, severity indicators, comorbidities, and regular medications. The objective of this study is to describe the development process of this tool and its operational framework.
2. Methods
The development of the inFLUence tool followed a user-centered design approach and was structured around four key steps: a systematic review, prototype creation, rapid prototyping, and an expert survey (Figure 1). Development process of the inFLUence tool.
2.1. Phase 1: Related works (systematic review)
The first step in the development of inFLUence consisted of conducting a systematic review, which had been carried out and published previously by our team. 18 The objective of this review was to identify risk stratification tools developed to predict complications, in particular hospitalization and mortality, among patients presenting with ILI in ambulatory or ED settings.
The literature search was performed in Medline, Embase, Cochrane Library, and CINAHL from their inception until July 20, 2023, restricting the selection to publications in French and English. Eligible studies were required to report the development or validation of a risk stratification score or algorithm for influenza-related complications. Studies focusing on untested algorithms, undifferentiated composite outcomes, exclusively hospitalized populations, or methodological designs that did not allow an evaluation of tool performance were excluded.
Article selection was first conducted by four reviewers who screened titles and abstracts, followed by full-text analysis by two independent reviewers. Disagreements were resolved by a third reviewer. The risk of bias of included studies was assessed using the PROBAST tool. The results were summarized descriptively and displayed with plots illustrating the sensitivity and specificity of each tool. No meta-analysis was performed due to heterogeneity across studies.
In total, fourteen tools (8 predictive scores and 6 predictive models) were identified. They provided the conceptual basis for selecting candidate variables, including symptoms, severity indicators, comorbidities, and medications, and for guiding prototype development in the subsequent phases. The full methodology and detailed results of this review have been published elsewhere and are available in open access. 18
2.2. Phase 2: Prototype creation
Based on the tools identified through the systematic review, an initial prototype was developed using a decision-tree structure. The selected questions formed the foundation for designing algorithms tailored to all age groups, enabling identification of infected individuals, assessment of disease severity, and stratification of both adult and pediatric patients distinguishing those requiring urgent medical attention from those likely to recover without intervention.
To ensure linguistic and conceptual consistency, the questions were first translated into English and then back-translated into French by two independent professional translators. A collaborative effort involving the two translators, a computer scientist, an information designer, a graphic designer, a research coordinator, and a clinical expert led to the creation of a digitized prototype designed to deliver personalized risk stratification for ILI based on user input. Upon completing the questionnaire, the tool instantly generates a tailored recommendation indicating whether a consultation in the ED or a primary care setting is necessary.
2.3. Phase 3: Rapid prototyping
Three iterative rapid prototyping cycles were conducted with potential users of the inFLUence tool. This approach enables prototype testing through user involvement and feedback, aiming to refine both the design and content, and to identify potential usability issues. This phase was conducted in the ED of the Centre Hospitalier de l’Université Laval (CHUL) from September 2019 to February 2020. CHUL is an academic hospital located in Québec City that provides general and specialized tertiary care to both adults and children. As part of its tertiary mission, it serves the greater Québec City area, as well as eastern Québec and northern New Brunswick. Its ED handles over 77,000 visits annually, including approximately 33,000 stretcher cases, with children under 18 accounting for 44% of all visits.
In each testing round, two adult patients, two parents of pediatric patients, and two triage nurses were invited to use the tool on tablets. Nurses were included as potential end-users, given that the tool could complement the ED triage process by supporting the initial assessment of patients with ILI. Previous evidence indicates that a minimum sample of 15 participants is sufficient to detect more than 90% of usability and ergonomic issues. 19
Patients and parents with suspected ILI were identified via the ED management software (SIURGE, Logibec, Montréal, Canada) and recruited by a research assistant after triage, during weekdays. Eligibility criteria included being at least 18 years old, consulting for themselves or their child, presenting with symptoms of acute respiratory infection, and remaining ambulatory throughout their ED stay. Exclusion criteria comprised severe respiratory distress requiring urgent care, visual impairments preventing tablet use, language barriers limiting comprehension of the tool, and any cognitive or consciousness impairment.
Triage nurses were recruited a few days before their scheduled shifts and asked to use the tool twice per session on convenience-selected patients with acute respiratory infection: once for an adult and once for a child. These patients were not considered study participants, as they did not interact directly with the tool or provide feedback.
During each cycle, participants used the tool independently on a tablet without external assistance, verbalizing their reflections throughout the process (think-aloud technique). A research assistant observed and documented both verbal and non-verbal reactions. At the end of each session, individual semi-structured interviews were conducted using a pretested interview guide (Supplemental Material) with adult patients and parents of pediatric patients. For nurses, interviews were conducted at the end of their shift. Interviews explored four predefined usability criteria: (1) ease of use (simplicity, navigation, format, length), (2) comprehension (clarity of vocabulary and instructions), (3) appreciation (perceived usefulness and overall acceptability), and (4) perceived purpose achievement (extent to which the tool was considered effective for risk stratification). Participants were also invited to suggest improvements. To avoid influencing clinical care, the tool’s outputs were concealed from both participants and healthcare providers. This methodological approach was informed by previous studies. 20
All interviews were audio-recorded, transcribed, and analyzed using a descriptive qualitative approach. Participation in the study was voluntary, and written informed consent was obtained from all individuals prior to their involvement. The study received approval from the Research Ethics Committee of CHU de Québec-Université Laval (reference number: 2020-4562). After each test cycle, a multidisciplinary team meeting was held to review participant feedback and improve the tool before the next cycle. The team consisted of a computer scientist, designer, linguist, research coordinator, and the principal investigator.
2.4. Online expert survey
To refine the prototype, a panel of seven medical experts was assembled based on recommendations or personal contacts of the research team. The panel included pediatricians, infectious disease specialists, emergency physicians, and internists. Each expert was invited to assess the relevance of the prototype’s questions via an online survey (REDCap),21,22 using a 9-point scale where 1 indicated not at all relevant and 9 indicated extremely relevant.
A videoconference was subsequently held to review items with median scores between 4 and 7, indicating uncertainty about their relevance, with the aim of reaching a final classification or making modifications to improve their usefulness. 23 The evaluation focused on severity signs of ILI, comorbidities and medical conditions likely to influence disease progression, as well as regular medications that may justify a medical consultation. Experts were also invited to suggest additional elements, such as other relevant severity signs, comorbidities, or medications. The prototype was further revised based on their comments and suggestions.
3. Results
3.1. Prototype creation
A series of questions was developed to address age, ILI symptoms, severity signs, health conditions, comorbidities that could worsen disease progression or support the initiation of antiviral treatment, as well as the regular use of medications that may influence prognosis. 24 The questions about medical history and medications were specifically designed to identify patients who might benefit from antiviral treatment, based on local guidelines in effect at the time of the tool’s development. The initial prototype was divided in 3 different algorithms for the following age groups: 5 months to 5 years, 5 to 12 years, 12 years and older. Immediately after the first classifying question, patients under 5 months of age are advised to consult a healthcare provider. The final recommendations provided to patients upon completing the tool were based on the Québec Ministry of Health’s guidelines for self-care in cases of ILI. 25
3.2. Rapid prototyping
A total of 18 participants took part in the three iterative testing cycles of the tool, with 6 participants per cycle: 2 adult patients, 2 parents of pediatric patients, and 2 triage nurses in each round. The mean age of participants was 36.1 years, with 12 women among the 18 participants.
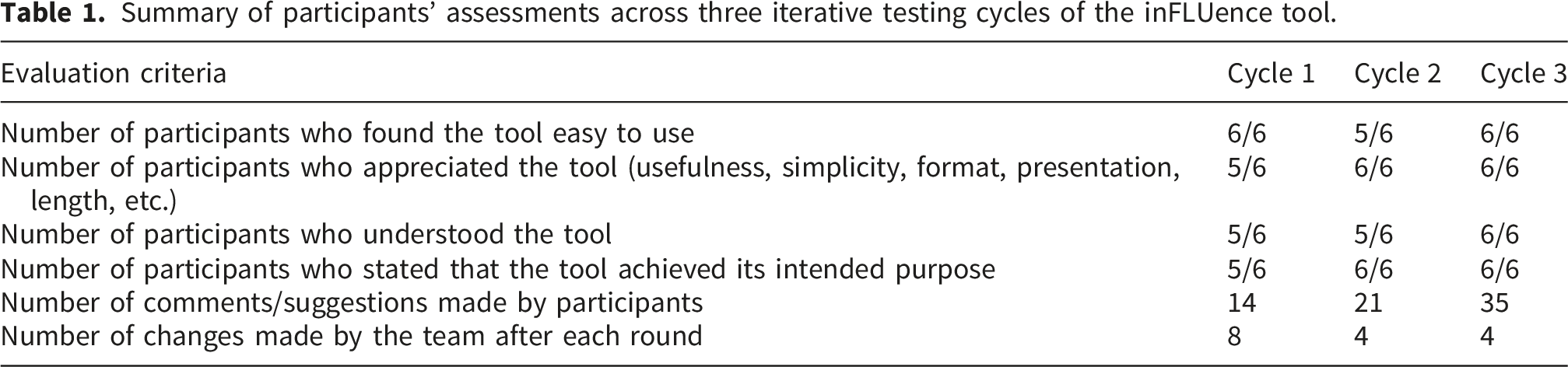
Regarding ease of use and overall appreciation, across all cycles, all participants, except one in the second cycle, found the tool easy to use and intuitive at first attempt. Only one older participant, unfamiliar with tablet technology, experienced some hesitation but successfully completed the test. In the first cycle, 5 out of 6 participants appreciated the tool, while all participants found it satisfactory in the subsequent two cycles. The format, presentation, and user-friendliness were widely praised. Understanding of the tool also improved from 5 out of 6 participants during the first two cycles to 6 out of 6 in the third cycle. Some technical terms were unclear to certain users, leading to adjustments favoring more accessible language for the public.
Summary of participants’ assessments across three iterative testing cycles of the inFLUence tool.
Participant feedback on the inFLUence tool across three user testing rounds.
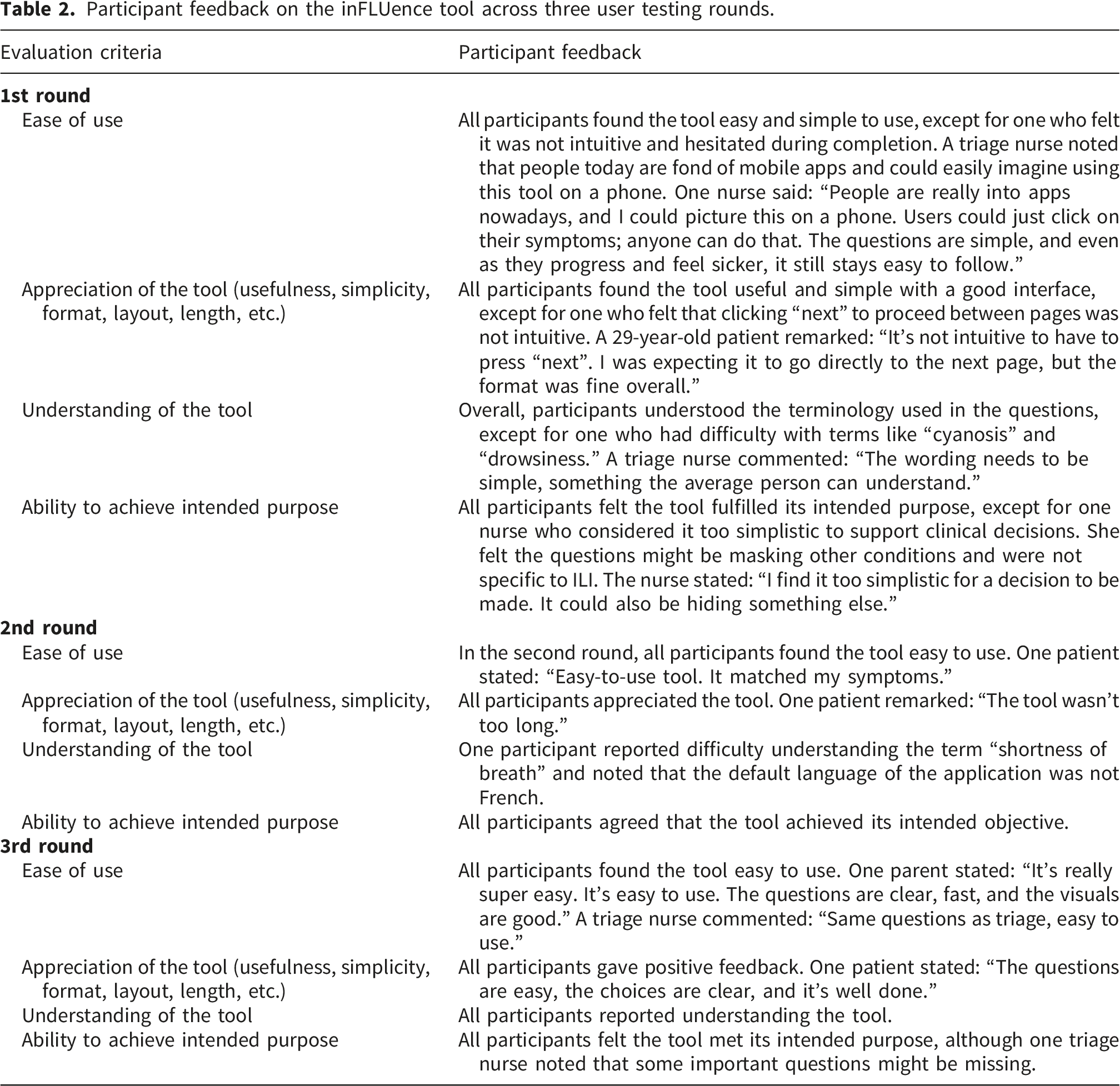
Moreover, numerous positive comments emerged, highlighting that the tool could help reduce ED workload and spare patients’ unnecessary travel. Triage nurses noted that the questions included in the tool corresponded to standard triage criteria, which reinforced their endorsement of the project.
3.3. Online expert survey
Expert evaluation of the relevance of severity signs of influenza-like illness.
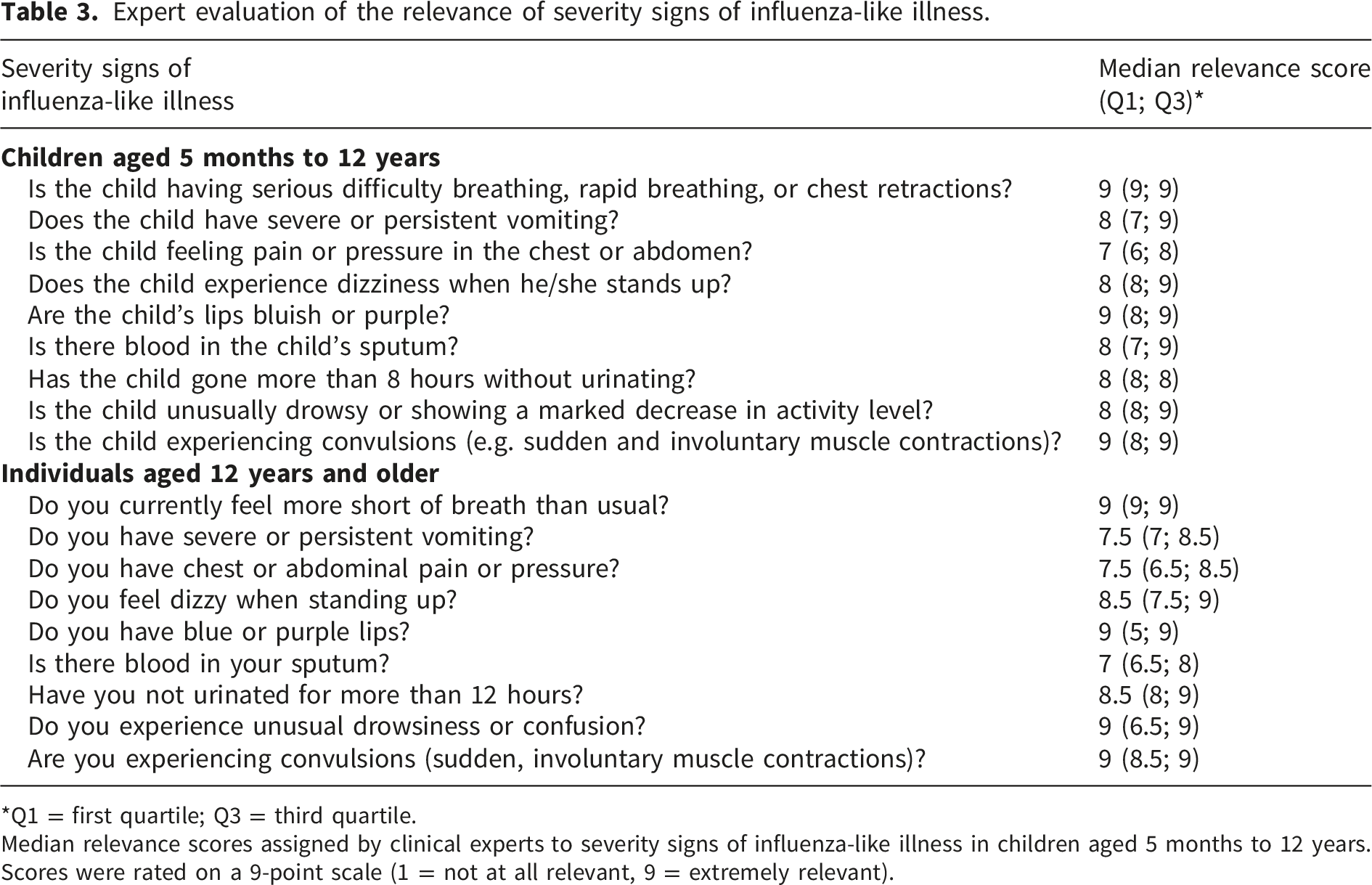
*Q1 = first quartile; Q3 = third quartile.
Median relevance scores assigned by clinical experts to severity signs of influenza-like illness in children aged 5 months to 12 years. Scores were rated on a 9-point scale (1 = not at all relevant, 9 = extremely relevant).
Expert evaluation of the relevance of comorbidities and regular medications.

*Q1 = first quartile; Q3 = third quartil; ** BMI = Body Mass Indexe.
Median relevance scores assigned by clinical experts to comorbidities and regular medications potentially complicating influenza-like illness. Scores were rated on a 9-point scale (1 = not at all relevant, 9 = extremely relevant).
Regarding regularly used medications, median scores ranged from 7 to 9, with three medications receiving a median score of 9 (Table 4). Additionally, the experts’ comments and suggestions were reviewed by the research team to assess their relevance and consider their incorporation into the tool.
3.4. Description of the final tool
Following all design stages, the final tool, titled inFLUence, was developed as a web application offering a self-administered digital questionnaire. Its programming ensures compatibility across all devices, including computers, smartphones, and tablets. The hosting and deployment of the application were managed through the OpenShift platform, 26 while server infrastructure and data storage were handled by Valeria. The beta version of the application in both French and English can be accessed online via the following link: https://ul-val-prj-influence-frontend.dev.valeria.science/.
The interface, intentionally minimalist with black text on a light background and enhanced by dynamic animations, facilitates navigation. Questions are presented sequentially and tailored to the selected age group: under 5 months, 5 months to 5 years, 5 to 12 years, or 12 years and older.
Questions and recommendations of the inFLUence tool.


Decision-making algorithm of the inFLUence tool.
It should be emphasized that, in its current form, inFLUence is intended solely as a self-assessment tool to guide patient orientation. It does not provide a clinical diagnosis and is not designed to support or replace medical decision-making at this stage.
4. Discussion
Using a user-centered design approach and rapid prototyping, we developed inFLUence, a self-stratification tool intended to help patients determine whether they should seek medical care for an ILI. Adapted for patients 5 months and older, the tool recommends either to go immediately to the ED, to consult a care provider in a community clinic in the next 48 hours or to self-care at home. inFLUence was designed as a web-based application accessible anytime, anywhere.
In contrast to inFLUence, PMEWS and CURB-65, identified as the two best-performing tools for predicting hospitalization in our previous systematic review, remain essentially clinician-oriented scores. Although they demonstrated good discriminative ability and are available as online calculators, their use requires either clinical evaluation in the case of PMEWS or biological data such as blood urea measurement for CURB-65. These requirements make autonomous use by lay patients unrealistic and limit their applicability outside clinical settings. Self-stratification tools truly designed for the public remain rare, particularly those developed through an iterative user-centered design approach.15,27 Among the few precedents, the SORT (Strategy for Off-Site Rapid Triage) tool, implemented in the United States during the 2009 H1N1 pandemic, is a notable example. 28 Like inFLUence, it aimed to alleviate ED overcrowding by directing low-risk patients toward self-management at home. Its design was inspired by the CURB-65 score 29 and its algorithm shared several similarities with inFLUence: it began with ILI symptom screening, assessed severity signs and comorbidities, stratified patients into low, intermediate, and elevated risk categories, and provided recommendations based on risk level. However, it relied on two separate tools for adults and children.
inFLUence therefore distinguishes itself by relying exclusively on self-reported information, covering a broader range of symptoms and comorbidities, incorporating regular medication use into risk assessment, and unifying pediatric and adult triage pathways within a single bilingual interface.
inFLUence also presents several additional advantages. Its simplicity and accessibility make it easy to integrate into daily life, without time or location constraints. Its clean interface, available in both French and English, was designed to accommodate varying levels of digital literacy. Furthermore, its algorithms can be updated by the development team to reflect new scientific evidence or clinical guidelines, ensuring that the tool remains relevant and reliable in a constantly evolving healthcare context. By collecting anonymized data on usage and self-reported symptoms, inFLUence could also contribute to the epidemiological surveillance of ILI in the general population, particularly among individuals who do not seek healthcare services.
The next step will be to conduct large-scale prospective studies to evaluate the tool’s performance, including sensitivity, specificity, predictive values, task completion time, and error rates, as well as user trust in and adherence to its recommendations. The objective will be to confirm that the application effectively fulfills its triage function without compromising patient safety. If results are favorable, integration into existing digital health systems, whether governmental or organizational, could be considered. In this context, developing a mobile version of the application appears essential, since smartphones are now the predominant means of accessing the web for most of the population. Such a strategy would encourage adoption by both healthcare professionals and the public, while enhancing interoperability with other frontline digital tools. Finally, future research should also examine whether the tool’s performance varies depending on the viral agent responsible for the respiratory infection that prompted its use.
Some limitations of this study must be acknowledged. First, the content validation process relied on a relatively small panel of seven experts, all based in Québec City. This may limit the diversity of perspectives and the adaptability of the tool to other socio-healthcare contexts. Second, user testing was conducted with 18 participants, a modest sample size which, although useful for improving the tool’s ergonomics and clarity, may not fully capture all usability challenges encountered by a broader and more heterogeneous population. Nevertheless, according to Virzi’s work, a sample of approximately 15 participants is typically sufficient to identify over 90% of usability issues, which lends robustness to the findings obtained. 19
In addition, the use of self-assessment tools carries inherent risks. Patients with severe symptoms may underestimate the seriousness of their condition or be falsely reassured by the recommendations provided, potentially delaying appropriate care. 30 As with any self-reporting tool, this limitation highlights the importance of deploying the application with clear messages encouraging users to seek medical attention in case of doubt or persistent symptoms. Conversely, some users may overestimate the severity of their symptoms due to anxiety or lack of knowledge, leading the tool to systematically direct them toward consultation as a precaution. While this conservative approach helps ensure patient safety, it may reduce the tool’s effectiveness in limiting avoidable healthcare visits.
Ultimately, inFLUence represents a meaningful advancement in the field of digital risk self-assessment for respiratory infections, with anticipated benefits for both patients and the healthcare system.
5. Conclusion
The inFLUence tool was designed through a participatory, user-centered approach, integrating user needs and expectations throughout the development process. This approach promotes optimal adoption of the tool by patients and contributes to its future acceptability. By offering an innovative, accessible solution focused on patient autonomy, inFLUence empowers individuals to assess their own risk of complications related to ILI. To validate its effectiveness and performance under real-world conditions, a large-scale prospective study is the essential next step before its widespread deployment to the public.
Supplemental material
Supplemental Material - inFLUence: Development of a self-administered risk stratification tool for patients with influenza-like illness using a user-centered approach
Supplemental Material for inFLUence: Development of a self-administered risk stratification tool for patients with influenza-like illness using a user-centered approach by Judicael Adadja, Myriam Mallet, Sean Johnston, Maude Ballou, Éric Kavanagh, Maurice Boissinot and Simon Berthelot in Health Informatics Journal.
Footnotes
Ethical considerations
This study was approved by the Research Ethics Committee of Québec (reference number: 2020-4562) on 2019-07-24. Respondents gave written consent for review and signature before starting interviews.
Consent to participate
Written informed consent was obtained from all participants prior to their inclusion in the study. Participants were provided with all necessary information, had the opportunity to ask questions, and voluntarily agreed to the collection and use of their personal data for research purposes.
Author contributions
SB and MM designed the study. SB, MM, MBa, SJ, EK and MBo supervised its conduct and contributed to the tool development. JA and SB were involved in the analysis and interpretation of the data. JA drafted the initial version of the manuscript. All authors critically reviewed the manuscript and approved the final submitted version. SB assumes full responsibility for the integrity of the data and the accuracy of the analyses performed.
Funding
This work was supported by the Fonds d’accélération des collaborations en santé of the Ministère de l’Économie et de l’Innovation du Québec (Bergeron-FACS-004). The authors declare having received private funding from Meridian Bioscience to develop point-of-care molecular tests; however, this funding was not used to develop the tool presented in this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The main data from the study are available in the manuscript. The full dataset will be made available upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.