
Abstract
Keywords
Introduction
Systematized Nomenclature for Medicine – Clinical Terms, or SNOMED CT for short, is the most comprehensive, multilingual clinical terminology in the world. It encompasses more than 350.000 concepts, which span across a diverse range of other concept types totaling 19 distinct hierarchies, including clinical findings, procedures, substances and body structures, and 17 other types of concepts. 1 SNOMED CT is used for structuring and standardizing documentation of care delivered by clinicians, including nurses. 2 SNOMED CT also supports cross-mapping to other international code systems, such as ICD (International Classification of Diseases) and LOINC (Logical Observation Identifiers Names and Codes). This allows healthcare professionals and organizations to exchange and share clinical information using different code systems without losing meaning of integrity of the data, as well as interoperability and seamless communication between different healthcare organizations. 1
The adoption of electronic health records (EHR) is on the rise across various healthcare settings, including hospitals, residential care facilities, and psychiatric facilities. 3 However, not every care setting uses the same terminology for documentation of care. Documentation of health care refers to the process of recording patient information, medical history, diagnosis, treatment plans, and progress notes in a secure and organized manner. It serves as a crucial tool for healthcare professionals to provide quality care, track the patient’s progress and communicate with other healthcare providers. Documenting patient care accurately and comprehensively is essential for delivering safe and effective healthcare, reducing errors, and protecting patient confidentiality. It is also vital for billing, research, and legal purposes, if necessary.4,5 Terminologies used for documenting nursing care are often derived from a Standardized Nursing Language (SNL), for example North American Nursing Diagnosis Association – International (Nanda-I), Nursing Intervention Classification (NIC), Nursing Outcome Classification (NOC), (ICNP) or the Omaha System (OMS). These provide a language for nurses which can be used consistently for documenting nursing care and exchanging this information. It is important for nursing documentation to be interoperable and unambiguous to avoid loss or misinterpretation of information during transfer of care between institutions, 6 which could result in inadequate patient care and safety risks.7,8
Care organizations can use different platforms or terminologies for documenting patient care. In order to understand each other’s workflow, interoperability is necessary. In the context of technology, interoperability refers to the ability of different systems working together seamlessly and effectively, independent of the used technology, platforms or interfaces. 7 Semantic interoperability ensures that data can be exchanged between different systems in a way that preserves its meaning and context, regardless of the language, format, or platform used by each system. A common terminology to document nursing care is an essential component of semantic interoperability in clinical care. 3 Next to the common terminology are digital information systems necessary that enable the use of a SNOMED CT reference set. This terminology must provide enough terms to describe the process of nursing care spanning across different nursing settings, ranging from psychiatric wards to the home care setting. SNOMED CT, which covers more than only nurse-specific concepts, can provide this common terminology for different nursing settings using a common nursing Reference Set. Examples of already existing nursing reference sets are the “International Classification for Nursing Practice” of the International Council for Nurses (ICN) and the Dutch “simpele referentieset met verpleegkundige interventies voor thema delier”. 9 Currently, there is no common terminology for documenting nursing care in Belgium. A SNOMED CT Reference Set can address this problem. A SNOMED CT Reference Set is a subset of SNOMED CT concepts that supports the implementation of SNOMED CT into the electronic health record.
The research question is the following: “Which SNOMED CT concepts are needed to standardize nursing documentation, provided by nurses across all care settings in Belgium”?
Method
Scope
The scope for this study is elaborated into three parts: - What: what are we describing in the Reference Set? - Where: for which areas of nursing care does the Reference Set apply? - Who: who is the target audience that will use the Reference Set?
What
In order to develop the Reference Set for documenting nursing care, the scope is further defined using “The Nursing Process” from Ida Orlando.
10
It provides a systematic approach towards nursing care, promotes critical thinking and helps to organize client-centered, holistic care.
10
The Nursing Process is a circular process - thus promotes the continuity of care - consisting of five steps: Assessment, Diagnose, Planning, Implementation and Evaluation (Figure 1). For the interest of the study, this process determines which concepts define nursing care and determines if a concept should be included in the Reference Set. The nursing process by Ida Orlando
10
.
The Assessment phase collects clinical measurements, symptoms and patient experiences to describe a patient’s situation. Information obtained from this phase contains both objective and subjective data from the patient and its environment. 10
During the Diagnosis phase, a clinical judgment is made. Collected information gets prioritized and formalized to get a diagnosis and the foundation for an action plan. A correct evaluation of previous clinical judgment is crucial within the process. 10 For example, Nanda-I provides nursing diagnoses which are further detailed in nursing problems. Nanda-I defines a nursing diagnosis as follows: “A nursing diagnosis is a clinical judgement concerning a human response to health conditions/life processes, or a vulnerability for that response, by an individual, family, group or community”. 11
Goals and outcomes are determined during the Planning phase. These guide further actions to be implemented in order to deliver patient care. Care plans aid in personalizing and tailoring actions to the specific patient needs. 10
The Implementation phase involves carrying out the actions that are planned during the planning phase. Planned interventions with specific actions are implemented in order to achieve the specified goals. 10
Last, during the Evaluation phase, the entire nursing process is evaluated. Are the specified goals achieved to resolve the nursing problems and diagnoses? Did new problems occur for the patient care? If necessary, new interventions are planned, implemented and re-evaluated. New problems will need adapted care plans to meet the needs of the patient. 10
Based on this circular process, several “Standardized Nursing languages (SNL) are developed. SNLs are based on nursing research and adapted according to the feedback received by the responsible working groups. These SNLs are examined for applicability in the Reference Set. The use of one or more SNLs provides an evidence-based foundation for developing a Reference Set that covers a broad range of concepts in nursing care.
Where
The Reference Set aims to cover all areas of nursing care: in a hospital setting, at home, nursing home and across all clinical disciplines: e.g.: pediatrics, psychiatry, cardiology, orthopedic surgery, intensive care, …
Who
The target audience is nurses delivering patient care across care settings. Adapting the Reference set to their specific documentation needs is therefore essential. Using the terminology provided in the Reference Set, nurses in Belgium should be able to document the entire process of nursing care at the point of care.
Construction of the reference set
Adapting an existing reference set
SNOMED CT published “Guideline to Reference Sets”, 9 a guideline on how to develop a Reference Set. For this project, the method “Adapt an Existing Reference Set” is chosen. This involves choosing an existing Reference Set and adapting it by adding relevant concepts or removing irrelevant concepts. Some SNLs have an existing Reference Set available via the SNOMED CT Browser or via a ‘mapping’ table of the institution of the SNL. A mapping is a table of the terms in the SNL that is linked to its semantically equivalent terms in SNOMED CT. This way, the terminology is available in both the terminology of the SNL and in SNOMED CT. If there is no semantically equivalent concept available in SNOMED CT, this results in a null-mapping for that concept and the official SNLs terminology is not fully available in SNOMED CT. If the mapping from an included SNL contains null-mappings, alternative SNOMED CT concepts are looked up via the SNOMED CT Browser and included in the Reference Set. If null-mappings still remain after this step, the concept from the SNL has no mapped concept available in SNOMED CT, this concept is therefore not included in the Reference Set.
Analysis of the SNLs
The evaluation of each SNL is done through a twofold study: an analysis and a face validity test. The analysis is done through examination of the manual of each SNL or via information obtained through internationally published peer-reviewed studies on one or more of the included SNLs.
A selection of the most used SNLs is made. These are NANDA-I, NIC, NOC, ICNP, International Classification for Functioning, Disability and Health (ICF), Clinical Care Classification (CCC) and The Omaha System (OMS).
12
During the analysis phase, the following six items are analyzed per SNL: • Number of concepts • Structure of the SNL • Intended healthcare providers • Existence of SNOMED CT mapping • Update frequency • Additional benefits/disadvantages (Table 1). Analysis of the SNLs.

The following items are handled as exclusion criteria for the SNLs: - Intended healthcare providers: If the SNL provides a terminology for healthcare professionals other than nurses, this could be confusing for nurses to use.
Face validity of the SNLs
In the next phase, the practical applicability of the included SNLs is further validated through a face validity test. The content of the remaining SNLs is further examined: does it cover the most important nursing care aspects (such as organ-related nursing care, self-care, emotional well-being, wound care, …), is there enough detail provided in the content of each terminology, is the content logically structured? If the SNL provides face validity in these aspects, it is included for further investigation for inclusion in the Reference Set. Finally, conclusions are drawn based on the results of the analysis and face validity of the SNLs and a decision is made which SNL or SNLs are included in the Reference Set. The analysis and face validity are conducted by JT; inclusion and exclusion of individual concepts is conducted by JT, KB and AD. Quality approval of the entire study’s methodology and its execution is monitored through the guidance committee.
Guidance committee
A guidance committee composed of five members will closely monitor the development process of the reference set. One member is a teacher from a bachelor-degree nursing education, the 4 other members are drawn from the nursing management of university hospitals in both the Dutch-speaking and French-speaking part of Belgium. Monitoring activities consist of design review and content review. The design review includes reviewing and approving the approach of developing the Reference Set. The content review will verify the structure of the Reference Set and the concepts that are added in the Reference Set. Feedback and considerations about the design and the content of the study will be verbally discussed and further implemented if unanimously deemed valuable by the members of the guidance committee. Multiple meetings were planned throughout the execution of the study to host the discussions. Preparatory material was sent via email prior to each meeting to review the current stage of the study: purpose and design of the study, intermediate results and final results. The results that were discussed encompass both the structure of the Reference Set, the included concepts and the excluded concepts. This approach of quality assurance is recommended by SNOMED International. 9
Results
Analysis of the SNLs
NANDA-I, NIC and NOC are often used together as NANDA-I/NIC/NOC to provide a standardized classification for nursing care with nursing diagnoses, interventions and outcomes. NANDA-I, NIC, NOC is the most widely implemented and researched nursing terminology in numbers of worldwide published research articles.3,6 NANDA-I currently has 267 diagnoses that are further detailed in nursing ‘problems’, ‘etiologies’ and ‘symptoms’. The same way, NIC 8th edition has 614 interventions that are further detailed in ‘activities’ and NOC 7th edition has 612 outcomes further specified in ‘indicators’. Nanda-I, NIC, NOC is currently not mapped to SNOMED CT concepts. Lastly, the structure model of Nanda-I, NIC or NOC is based on clinical themes, which can be applied for structuring the Reference Set.13–16
The International Classification for Nursing Practice (ICNP) is a nursing taxonomy with 2035 detailed concepts divided in two lists: ‘diagnosis/outcome’ and ‘interventions’. Most of these concepts have a matching concept in SNOMED CT presented in ICN’s “Equivalence Table” from 2019. The structure model has no clinical themes and is not applicable for structuring the Reference Set. 13
The Omaha System (OMS) has identified 335 care problems, 76 interventions and three outcomes. The problem classification scheme is structured through four “life domains” and 42 clinical and non-clinical subdomains. The interventions are structured through four categories of interventions and the outcomes are new ratings of the earlier determined problems. Originally, the Omaha System was developed for home care. 6 Nowadays, its use is multidisciplinary, not nurse-specific and across different care settings. The mapping of The Omaha System to SNOMED CT concepts is in progress and has not been updated since 2005.6,17
The Clinical Care Classification (CCC) contains 176 nursing diagnoses, 201 core interventions with four sub-interventions each and three outcomes for each nursing diagnosis. Its diagnoses and interventions are structured using 21 “Care Components”. The Care Components are clinical themes that include the psychosocial context of the patient. These care components offer a good structure model for the Reference Set. CCC is fully mapped to SNOMED CT concepts with no null-mappings, free to download and used in nursing care. The terminology is focused on nursing care across different care settings. The latest update is from 2012.6,18,19
The International Classification of Functioning, Disability and Health (ICF) from the World Health Organization is a framework to conceptualize a person’s health and disabilities. A person’s health is defined by describing four components: the body functions and structures, activities and participation, environmental factors and personal factors. These “components” are further specified into 30 “chapters” to describe a person’s health and functioning. These chapters are further detailed in 362 categories of concepts. In total, ICF counts 1424 codes to describe a person’s health. A qualifier scale is used to measure the extent of each concept that defines someone’s health. The framework of ICF does not include interventions or outcomes to define a process of care. The intended users of this framework are multidisciplinary healthcare workers, so it’s not exclusively made for nurses. The last update was in 2008.6,20
During the analysis of the SNLs, two are found to have a target audience that target all caregivers: The Omaha System
17
and ICF.
21
Since these SNLs are not nurse specific, they are excluded for further evaluation.
22
A face validity test was conducted on the remaining five SNLs as described in section “3. Methods”: NANDA-I,
11
NIC,
23
NOC,
23
ICNP
24
and CCC.
18
The result of the face validity test is summarized both descriptively and in Figure 2. Selection of Standardized Nursing Languages (SNLs) through analysis and face validity.
Face validity of the SNLs
The findings of the face validity of Nanda-I, NIC, NOC11,23 are comparable: Nanda-I, NIC, NOC offer all the concepts necessary to accurately describe nursing diagnoses, interventions and outcomes respectively. The 267 high-level concepts in NANDA-I (nursing diagnoses) are broadly formulated and need extra specification with lower-level concepts (problems, etiologies, symptoms) to further specify nursing diagnoses. The same extra specification is necessary in the interventions of NIC in ‘actions’ and the outcomes of NOC in ‘indicators’ to describe nursing care with sufficient detail. This results in more than 10.000 detailed concepts.11,23
ICNP 24 offers detailed concepts to accurately describe nursing care on one level of specification using the SNOMED CT Equivalence Table. This aids the intuitive use of the SNL to describe nursing care. The diagnosis/outcome concepts describe normal and abnormal findings of the patient. The intervention concepts use a variety of actions targeting different aspects of care. The meaning of each concept is clear for use in the electronic health record.
CCC 18 can accurately describe nursing care with nursing diagnoses, interventions and outcomes. CCC uses major and sub-levels for diagnoses and interventions to define nursing care. Three outcomes are used to re-evaluate the chosen nursing diagnosis. The concepts in the sub-interventions and sub-diagnoses are not as detailed as the concepts used in the problems of Nanda-I, the actions of NIC and the indicators of NOC. This aids in the intuitiveness of using the framework of CCC, but further detailed concepts are needed to document detailed nursing care.
Based on these findings, the use of two SNLs to develop the Reference Set is suggested: CCC and ICNP. The use of NANDA-I, NIC and NOC in the Reference Set would require the development of a mapping to SNOMED CT concepts. This would require mapping of more than 10.000 concepts from NANDA-I, NIC, NOC to SNOMED CT, this is not feasible for the purpose of this study. CCC offers a structured nursing process and provides broad concepts used in nursing care. ICNP provides detailed concepts which can add the detail necessary to further specify the diagnoses, interventions and outcomes. The combination of these two SNLs offers a structured nursing framework with broad and detailed concepts suitable for the documentation of nursing care. The combination of CCC and ICNP serve as the evidence-based framework of the Reference Set. An overview of this selection process is provided in Figure 2.
Exclusion of concepts
The mapping tables from ICNP to SNOMED CT concepts and the mapping from CCC to SNOMED CT concepts are used. After finding alternatives for null-mappings in the mapping tables of ICNP and CCC, 23 concepts from ICNP still resulted in a null-mapping. Using Excel, the mapping from ICNP offers 2035 SNOMED CT concepts and the mapping from CCC offers 979 SNOMED CT concepts. The overview of the number of concepts is shown in Figure 3. Identification of concepts in two SNLs: Clinical Care Classification and International Classification of Nursing Practice.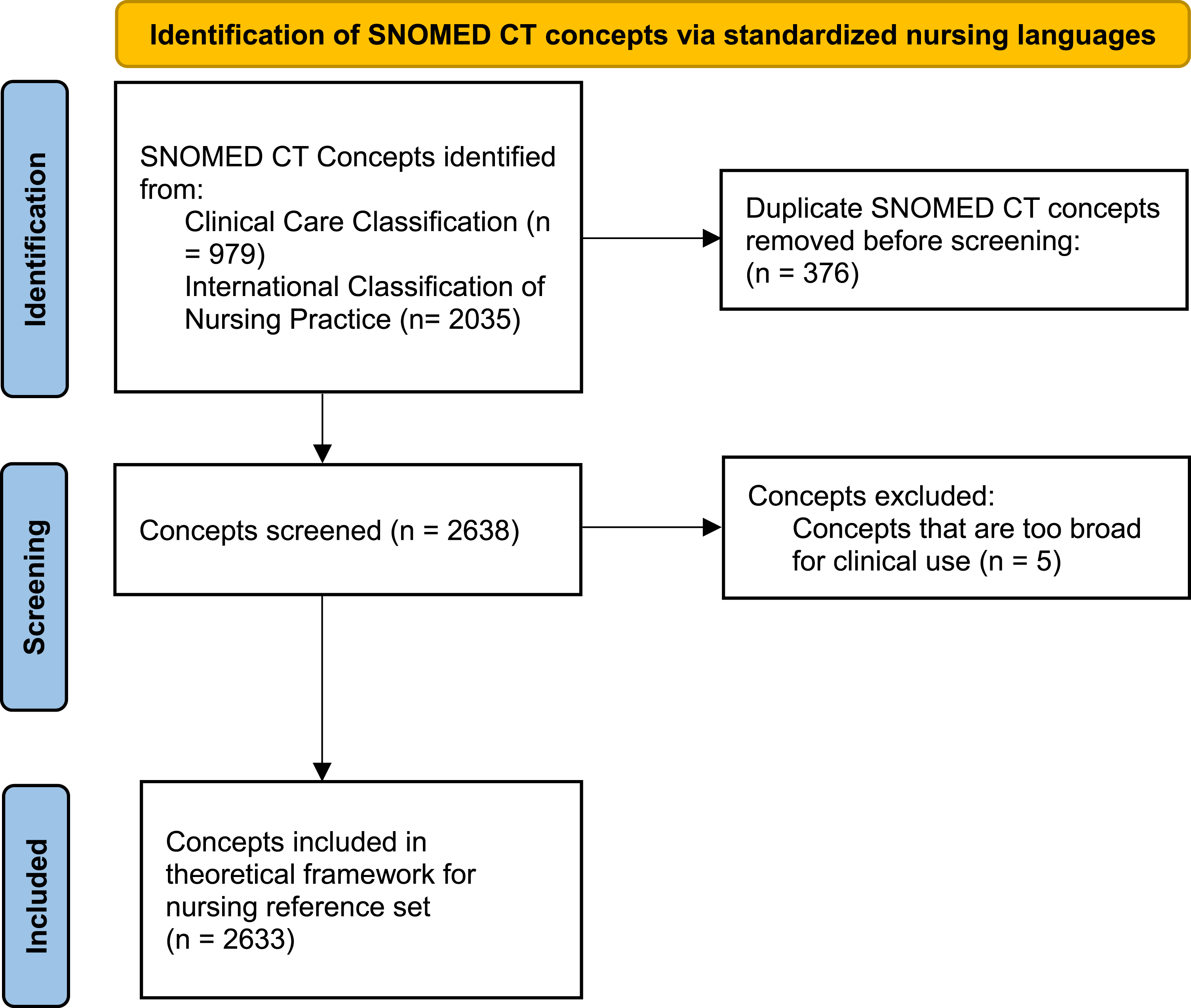
ICNP and CCC are both standardized nursing languages which describe nursing care. Duplicate target concepts in the mapping to SNOMED CT are present and must be removed. These are marked automatically using the ‘conditional formatting’ tool in Microsoft Excel. After this process, 376 duplicate target concepts are removed from the Reference Set.
Some target SNOMED CT concepts are excluded from the Reference Set because the clinical meaning is considered too broad. These concepts can be understood in many ways leading to wrong interpretation of the documented care. Examples are “assessment of physiological status (procedure)” and “physiological monitoring regime (regime/therapy)”. This step excluded 5 target SNOMED CT concepts from the Reference Set.
Discussion
The development of a SNOMED CT Reference Set for nursing holds immense potential in enhancing the documentation of nursing care across various healthcare settings. However, to support its widespread implementation and acceptance, continual maintenance and testing are necessary to ensure its completeness and efficacy. The following recommendations for the future refinement and validation of the proposed Reference Set can be made.
The current study describes a robust and evidence-based framework for developing a SNOMED CT nursing Reference Set. However, the use of SNLs to document nursing care is no common practice in Belgium. Most care institutions develop their local terminology with rules and concepts tailored to local needs. Therefore, the use of a SNOMED CT nursing reference set based on SNLs will require a thoroughly planned implementation, both on digital and educational aspects.
If the scope of the study was narrower (I.e. focus on general hospitals that use the same electronic health record), the development of the SNOMED CT nursing Reference Set could be tailored to that specific use case and local terminology. The scope of this study is broad: cover nursing care documented over all areas of nursing care in Belgium. This rationalizes the use of SNLs to develop a SNOMED CT Nursing Reference Set.
Refinement
Practical validation of the Reference Set is necessary for successful implementation. This should be based on SNOMED International’s guideline to Reference Sets: “Refinement approaches”. Using this technique, relevant concepts for the Reference Set are added and irrelevant concepts are removed. In this approach, clinical experts from different nursing domains must validate the evidence-based framework with additions or removals. This step will add value to reaching the goal: identifying all concepts relevant for documenting nursing care across different care domains. This goal supports looking up alternatives for the null-mappings in the original mapping tables of ICNP to SNOMED CT.
Translation
To support successful implementation in Belgium, translation of the description of included concepts in the Reference Set to both Dutch and French is necessary. Translation of concepts is the responsibility of the National Release Center. This can prevent health care institutions translating concepts in their own dialects. This can promote wrong use of the concepts through misinterpretation. Translation must be carried out through a rigorous process as provided by the editorial guide of the federal government agency. 25
Comprehensive coverage
Acknowledging that nurses work in diverse healthcare settings is crucial to further expand the Reference Set to cover the full spectrum of nursing care. Future maintenance should focus on incorporating concepts and terminology that are specific to various healthcare settings, such as acute care, long-term care, home care, and specialty areas like pediatrics or mental health.
Stakeholder engagement
Engaging key stakeholders, including nurses from different practice areas, nurse educators, nurse informaticists, and chief nursing officers, is essential. Soliciting their input through surveys, focus groups, or multidisciplinary meetings will ensure that the Reference Set addresses the needs and priorities of the nursing community, thus increasing its usability and acceptance.
Clinical validation
To establish the reliability and validity of the Reference Set, rigorous clinical validation processes should be conducted. This should involve implementing the Reference Set in real-world clinical settings to assess its feasibility, accuracy, and usefulness in documenting various aspects of nursing care. Gathering feedback and evaluations from nurses that document nursing care based on the Reference Set will help identify areas that need refinement.
Continual updates
Recognizing that the field of nursing is dynamic and ever-evolving is important to establish a framework for regular updates and expansions to the Reference Set. Permanent collaboration with relevant standardization bodies, such as SNOMED International, the National Release Center for SNOMED CT and Belgian Terminology Center, and ongoing engagement with nursing professionals will facilitate the incorporation of emerging concepts, technological advancements, and changes in nursing practice.
Interoperability and EHR integration
Future research should focus on facilitating the interoperability and seamless integration of the SNOMED CT Reference Set within existing electronic health record (EHR) systems. Exploring strategies to align the Reference Set with other standardized terminologies or classifications such as ICNP and CCC will enhance its interoperability potential and promote consistent documentation practices and support secondary use.
Education and training
Ensuring that nurses are adequately trained and educated on the importance of care documentation is crucial for the successful adoption of the Reference Set. Future research should investigate the most effective methods to educate and train nurses on the documentation of the nursing process using SNOMED CT and the Reference Set, including the development of educational resources, training programs, and integration into nursing curricula.
Conclusion
The development of this SNOMED CT Reference Set for nursing presents a significant advancement in nursing documentation in Belgium. However, to ensure its effectiveness and usability, further maintenance is recommended. By addressing the outlined recommendations, the Reference Set can be refined, validated, and ultimately contribute to improving the seamless exchange and reuse of documentation of nursing care across diverse healthcare settings.
Footnotes
Ethical considerations
This article does not contain any studies with human or animal participants.
Authorship contribution
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article’
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.