
Abstract
Keywords
Introduction
A Healthcare Information System (HIS) is an effective and economical solution that was introduced to solve problems encountered by healthcare providers by integrating ICT into the healthcare sector. 1 Although the term HIS may sometimes be used interchangeably for a hospital information system, 2 this research defines HIS as a healthcare information system that integrates computer systems throughout the hospital, which was developed to enhance a hospital’s clinical and administrative function. 3 HIS is a healthcare data management system that collects, stores, manages, and transmits a patient’s electronic medical record (EMR). 4 Additionally, HIS can serve as a hospital’s operational management system or a system supporting healthcare policy decisions.
Secured computer networks are used to produce EMRs from integrated HIS. Authorised healthcare professionals can access these networks for consultation and information exchange across healthcare settings.5–7 To achieve complete hospital automation and coordinated care delivery among multiple providers, HIS is employed in Malaysia to construct EMRs. Hospitals in Malaysia have been deploying a non-shareable electronic health records (EHR) system run by a single or several authorised care providers within a specific facility. 8 However, this is owing to policy limitations.9–11 Patients’ medical records are neither portable nor usable outside the hospital under this arrangement.
Healthcare and organisational interoperability
Healthcare interoperability is the ability of different information systems, devices and applications (systems) to access, exchange, integrate and cooperatively use data in a coordinated manner, within and across organisational, regional and national boundaries, to provide timely and seamless portability of information and optimise the health of individuals and populations globally. 12 In general, there are three different types of interoperability: syntactic, semantic, and OIoP. 13 According to the European Interoperability Framework (EIF), OIoP is focused on ensuring that different entities can work together effectively, even if they have different organisational structures or processes in place. 14
OIoP coordinates processes among different organisations to achieve mutually beneficial goals. This includes addressing legal, political, and cultural aspects,12,15 It standardises healthcare services across care providers or organisational units (e.g., departments, labs) based on predetermined norms and protocols. In healthcare, OIoP benefits hospitals by ensuring the transference of EMR to any health institution is possible 16 and allowing patients a safer way to access the HIS. 17 Additionally, understandable and usable information for patient treatment 18 can be exchanged between hospitals while reducing rework by care providers. 19
OIoP has many benefits, but challenges remain. Technology is often vendor-driven, and HIS vendors resist sharing ideas and technology. 20 HIS often have distinct standards and specifications, causing compatibility difficulties. The lack of healthcare interoperability rules makes the problem worse. 12 An interoperability framework is necessary to provide the conditions so that digital tools are adopted and used in a trustworthy manner. Previous studies have focused on technical interoperability (e.g., data formats21,22). However, studies focusing on organisational interoperability, particularly in healthcare, are scarce. Understanding the institutional factors affecting OIoP is crucial to identify and address any barriers or challenges that may arise in implementing interoperable systems in healthcare organisations, ultimately improving the quality of care and patient outcomes. 23 Therefore, to address this gap, this study seeks to discover institutional factors affecting HIS organisational interoperability, specifically in healthcare institutions in Malaysia.
Research questions
The study is guided by two research questions (RQs) as given below:
What are the institutional factors that affect HIS organisational interoperability?
What are the significant predictors of successful HIS organisational interoperability?
The paper is organised as follows: Background presents the background on the Interoperability Framework and factors that impact Organisational Interoperability. This is followed by Methodology, which outlines the research methodology. The following section presents the results, and the findings are discussed next. Finally, the paper acknowledges this study’s implications and limitations and suggests future research directions.
Background
Interoperability frameworks have gained importance in healthcare delivery and have become a government priority in several countries. 24 These frameworks provide standards, protocols, procedures, best practices, and regulations to enhance the cost-effectiveness of EMR solutions.25,26
Recently, there has been a growing focus on the importance of interoperability in HIS. This is partly due to the increasing use of HIS and the growing recognition of the benefits of interoperability. Frameworks such as eHealth European Interoperability Framework (eHealth EIF), Personal Health Systems Interoperability Framework (PHS IF) and Refined eHealth European Interoperability Framework (ReEIF) provide a set of principles, guidelines, and standards for the development of interoperable HIS. However, they are not specifically tailored to the Asian context. There is a need for more research on OIoP in Asian countries and research that uses different frameworks. 27
Research model and hypothesis
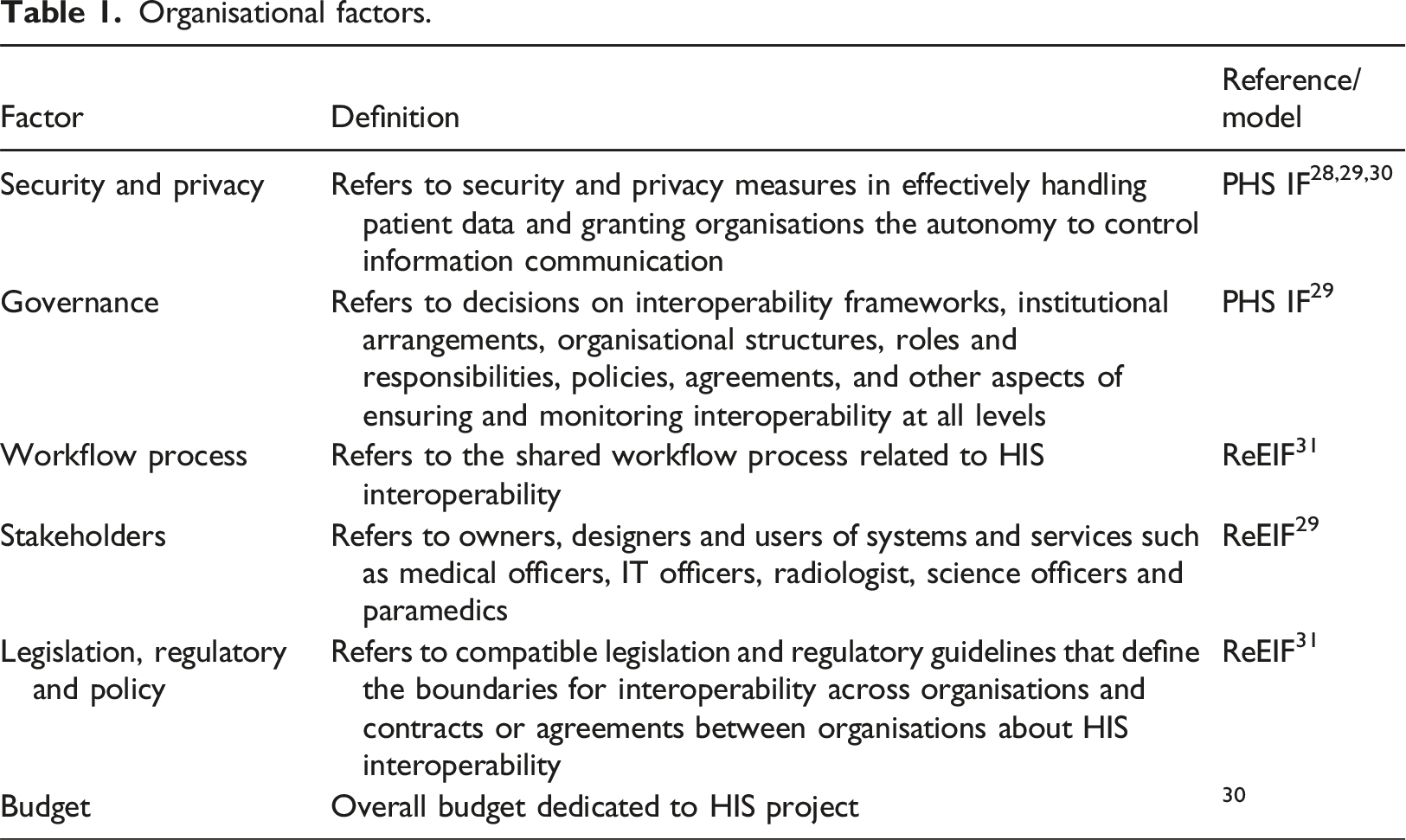
Organisational factors.
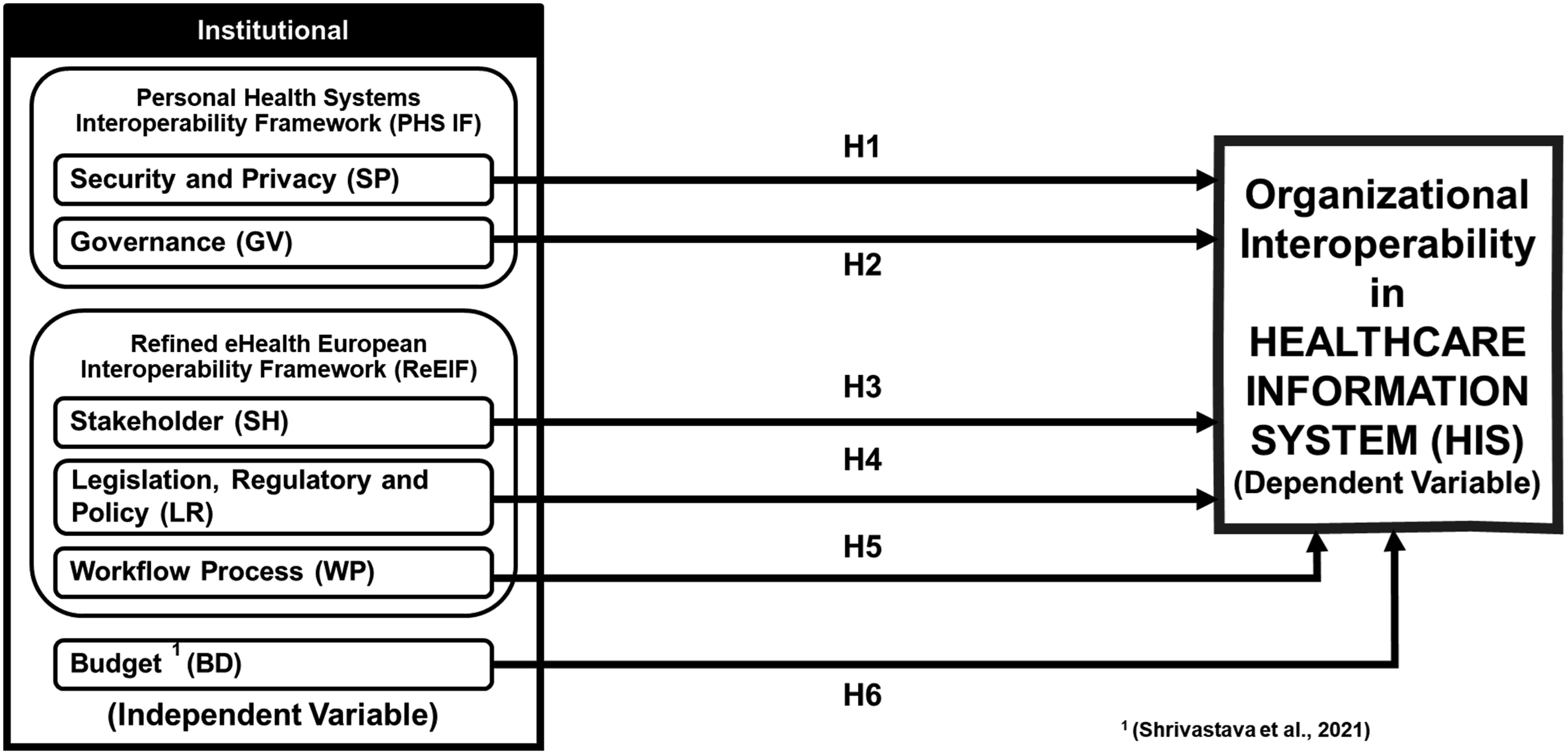
Conceptualised framework for HIS organisational interoperability.
Institutional factors
Institutional factors related to HIS interoperability include Security, Privacy, and Governance from Personal Health Systems Interoperability Framework (PHS IF), 32 Workflow Process, Stakeholders, Legislation, Regulatory, and Policy from Refined eHealth European Interoperability Framework (ReEIF). Budget is also included in this category.33–35
Security and privacy (SP)
HIS security and privacy are crucial. A HIS must safeguard patient data from unauthorised access, use, disclosure, disruption, modification, or destruction. According to extensive studies on security in healthcare IT infrastructure interoperability, robust and comprehensive security and privacy measures will directly affect multiple crucial aspects.36–38 Failure to address these concerns could endanger patient health and data integrity. We believe security and privacy will impact HIS Organisational Interoperability. The first hypothesis is:
Security and Privacy positively affect HIS OIoP.
Governance (GV)
Effective governance ensures interoperability initiatives align with organisational goals, meet regulatory requirements, and promote stakeholder collaboration.28,29 According to research, clear leadership and accountability for interoperability efforts in strong governance structures help HIS implementations succeed. Governance is crucial because it emphasises implementing stakeholder-focused strategies. Thus, hypothesis two is:
Governance positively affects HIS OIoP.
Stakeholders (SH)
Success in HIS interoperability projects depends on stakeholders. Identifying and involving all stakeholders during planning and implementation is crucial. This inclusive approach ensures that the project meets everyone’s needs and succeeds long-term. HIS has many benefits, but several barriers prevent its widespread use. These barriers include physician acceptance, authentication concerns, and a misplaced focus on technology rather than healthcare needs.39,40 These barriers can be addressed effectively by engaging stakeholders, including physicians, in developing and implementing HIS interoperability projects. Therefore, hypothesis three is formulated as follows:
Stakeholders have a direct positive effect on HIS OIoP.
Legislation, regulatory and policy (LR)
Legislation, regulatory frameworks, and policies affect e-health system implementation and success. Effective national and local processes are crucial. Legislation, regulations, and policies can help HIS interoperability. Laws that mandate EHRs can help create a data exchange platform. Regulations that set data exchange standards can improve interoperability 31 and policies that promote the sharing of data between organisations can help to break down silos and improve the quality of care. Hypothesis four is formulated as follows:
Legislation, Regulatory and Policy positively affect HIS OIoP.
Workflow process (WP)
To achieve HIS interoperability, workflow must take advantage of system capabilities. This may involve using EHR to track patient progress and communicate with other providers. There is little research on how standardised workflows improve healthcare delivery in interoperable environments. To achieve HIS interoperability, workflow must take advantage of system capabilities. This may involve EHRs to track patient progress and communicate with other providers. The fifth hypothesis is:
Workflow Process positively affects HIS OIoP.
Budget (BD)
Implementing and maintaining an HIS interoperability project incurs costs and can be significant. 30 Many organisations underestimate the long-term costs of maintaining and upgrading interoperable systems. Creating a realistic budget that includes hardware, software, training, and support is crucial. More research is needed to assess project cost-effectiveness. Studies could examine whether improved information sharing is worth the financial investment. Thus, hypothesis six is:
Budget has direct positive effects on HIS OIoP.
Methodology
This cross-sectional study employed self-administered surveys to gather data from healthcare professionals in Malaysian public hospitals, aiming to explore institutional factors and confirm their direct effect(s) on HIS OIoP through exploratory and confirmatory factor analyses. The materials and methods used are elaborated in the following sub-sections.
Instrument
A self-administered survey questionnaire in English and Malay assessed participants’ demographics, HIS experience, and drivers and barriers of OIoP in HIS. The questionnaire contained four main sections with the items adopted/adapted from past studies precisely.11,41,42 Section A focused on obtaining demographic information and the respondent’s background. Section B aimed to obtain information on the experience and knowledge of respondents in HIS.
Section C of the survey focused on the dependent variable, namely organisation interoperability in HIS, which was assessed using three items (i.e., My department/organization’s HIS interoperates effectively within our department/organization’s HIS, My department/organization’s HIS interoperates effectively with external department/organization’s HIS and The HIS Interoperability in my department/organization is satisfactory).
Section D examined the independent variables, Security and Privacy, Governance, Stakeholders, Legislation, Regulatory and Policy, Workflow Process, and Budget. These aspects were addressed by 36 questions to determine their presence in departments and organisations. Sections C and D were assessed using a 5-point Likert scale (1 – Strongly disagree; 2 – Disagree; 3 – Neutral; 4 – Agree; 5 – Strongly agree) where respondents indicate their levels of agreement/disagreement based on their individual perceptions of each item. The complete questionnaire is attached as Appendix A.
Before distributing the questionnaire for data collection, academics with over 15 years of IT, healthcare, and language experience validated it. This was done three times before the pilot study. In official emails, participants answered the link to the online questionnaire created and administered by Microsoft Forms. Initially, the questionnaire underwent a pilot test among 30 respondents from Hospital Tuanku Ja’afar, Seremban. The participants were instructed to identify ambiguous or difficult-to-understand words/sentences in the questions. Their feedback was collected to make necessary adjustments. According to most, the questionnaire was simple, and no significant issues were present.
After the pilot study, the reliability of the questionnaire is verified by the reliability test and Cronbach’s Alpha (CA). The study results show that all scales achieved a CA value that surpasses the minimum required threshold of 0.7 (>0.7), indicating good internal consistency.
Sampling
The final study involved eight Malaysian HIS-related local hospitals participating in HIS projects or using HIS modules. Stratified random sampling was used to ensure adequate subject selection from each employee category. The simple proportions formula developed by Goldsmith and Yamane
43
was employed to ascertain the sample size.
The appropriate sample size was determined to be 300 respondents from the population of 1200 employees (N), with a targeted limit of sampling error of 5% (e). 44
Procedure
The Medical Research and Ethics Committee (MREC) has approved this study. Besides, researchers also adhered to the principles of the Declaration of Helsinki and the Malaysian Good Clinical Practice Guidelines (MGCPG). Subsequently, the final survey was distributed to the hospital quality manager via an email with the online survey link for final data collection, who assisted in distributing the invitation to all eligible participants. The inclusion criteria for participation were public health sector staff. Written informed consent to participate were solicited through the questionnaire. Data collection took 12 weeks.
Respondents
Participants’ demographic and involvement in HIS (n = 300).
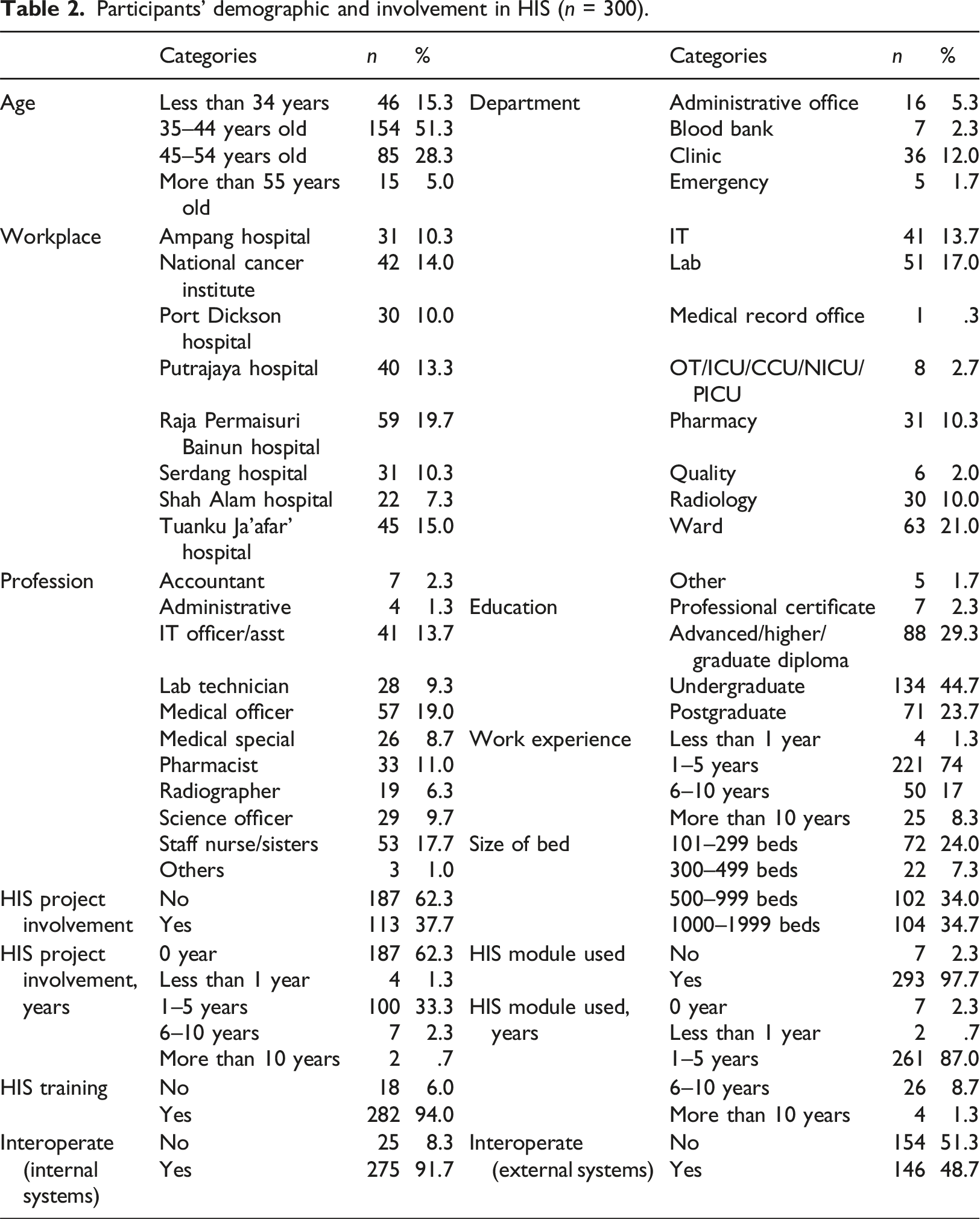
Medical officers made up the majority of responders (n = 57, 19%), followed by nurses (17.7%) and IT (13.7%). Survey responses may reflect healthcare IT stakeholders’ opinions due to the breadth of professions covered. The majority of respondents worked in hospital wards (n = 63, 21%), labs (17%), and IT (13.7%). The survey’s distribution across departments showed that it represented a variety of healthcare facilities and working experience, which is crucial in healthcare IT.
Most 293 participants (97.7%) had used HIS modules for one to 5 years (n = 261, 87%). Participants (n = 282, 94%) also received HIS training. Additionally, 37.7% (n = 113) of participants participated in HIS projects. Most HIS project participants had been involved for one to 5 years (n = 100, 33.3%). (n = 275, 91.7%) respondents said their HIS can communicate with internal systems, while (n = 146, 48.7%) said it can communicate with external systems. This suggests that most healthcare facilities have integrated their HIS with other internal systems to improve care coordination and information exchange. However, many healthcare facilities cannot share patient information, which could hinder coordinated care and information exchange.
Data analysis
The data were processed in two stages: EFA and CFA. EFA was performed using Statistical Packages for Social Sciences (SPSS) 23 whereas CFA (i.e., Partial Least Squared- Structured Equation Modelling, PLS-SEM) was done using Smart Partial Least Square (Smart PLS 4.1.0.3). Outliers, normalcy and distribution were checked before statistical analysis to confirm that the data met the criteria. Demographic profiles, experience, and respondents’ knowledge of HIS were analysed using descriptive statistics. The dataset was rigorously tested using the CA reliability coefficient, EFA, and other methods after data cleaning. Next, PLS-SEM was used to evaluate the model’s validity and regulatory efficiency.
The original dataset (n = 300) was divided into two sub-samples: 145 for EFA and the remaining 155 for CFA, following recommendations suggesting a random split of the dataset for EFA and CFA in the absence of two data collecting processes.45,46
Exploratory factor analysis (EFA)
Preliminary analyses were conducted prior to EFA. First, the data distribution was assessed using the Kolmogorov-Smirnov test, with all p-values showing significance (p < .05), indicating non-normal distribution. No multicollinearity issue was noted as all the values in the correlation matrix and communalities were within the required threshold (see Appendix B). Variance inflation factors (VIFs) were used to assess common method bias (CMB). According to Hair, Hollingsworth, 47 a VIF threshold of 3.3 was considered. In this study, all VIF values were below 3.3 (i.e., 1.495–2.226), suggesting CMB is not a significant concern. 48 The Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy and Bartlett’s sphericity test were performed prior to EFA as well.
Confirmatory factor analysis (CFA)
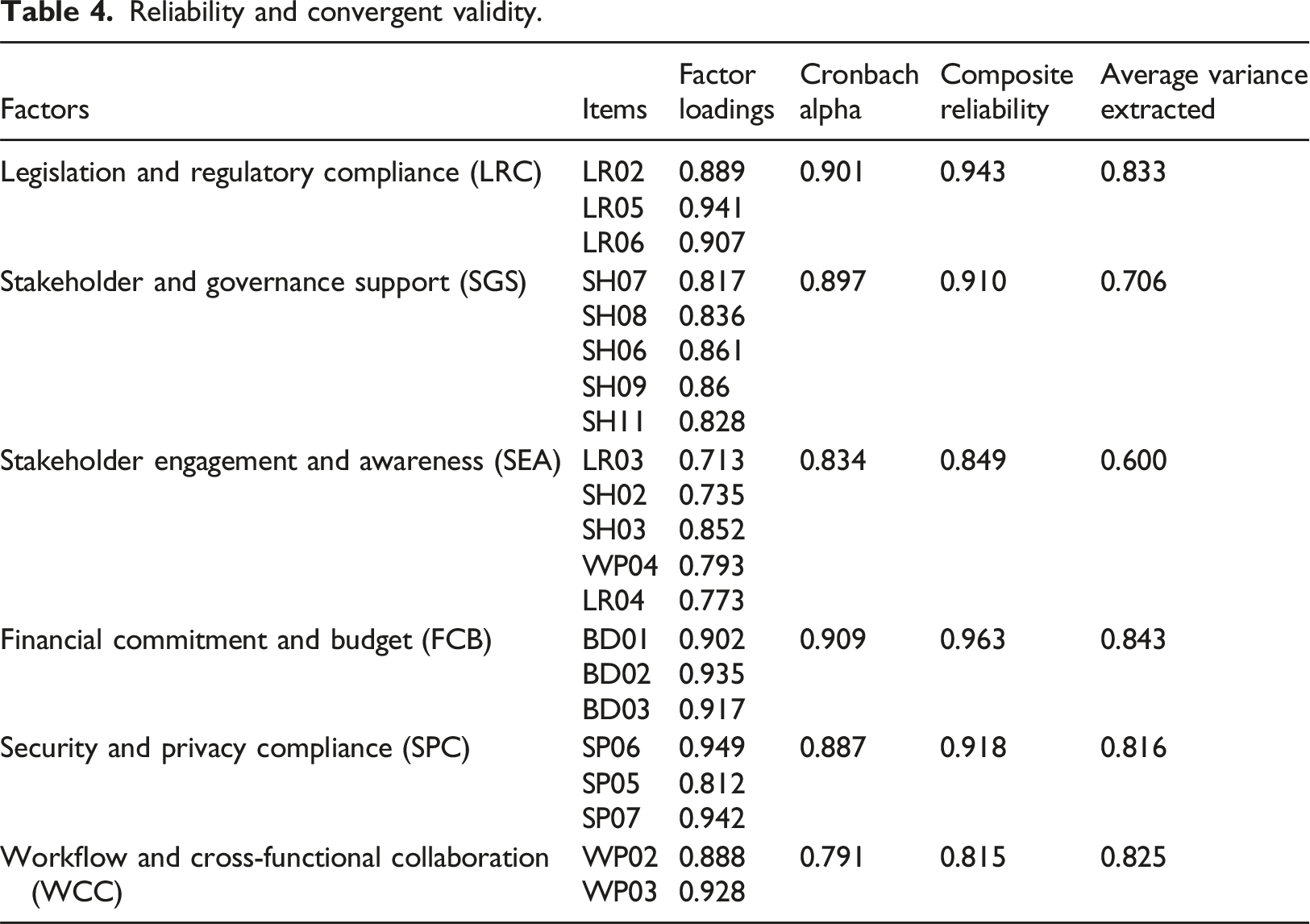
PLS-SEM, a multivariate method for evaluating structural models, was employed in the second phase of the investigation. Step one of the PLS-SEM process evaluates the validity and reliability of the proposed model, followed by its estimation. The components’ VIF values ranged from 1.327 to 2.135, indicating that Common Method Variance (CMV) is not a problem (i.e., <3.3). Conversely, factor loadings, CA and Composite Reliability (CR), which is at least 0.7, whereas Average Variance Extracted (AVE), which is at least 0.5, are the criteria utilised for reliability assessment. 49 Discriminant validity was assessed using two metrics: the recently developed Heterotrait-Monotrait Ratio (HTMT), which necessitates that all scores be less than 0.9, and the Fornell-Larcker criterion, which needs each factor’s AVE square roots to exceed its correlations with other factors. 50
Structured equation modelling (SEM)
The PLS algorithm was utilised to evaluate the path coefficients and predictive power, and the significance tests were carried out via bootstrapping (resampling = 5000). (i.e., two-tailed t-test with a cut-off value of 1.645).
Results
This section presents the results and discussion, beginning with the EFA, followed by the CFA.
Exploratory factor analysis (EFA)
Factor analysis using varimax rotation.
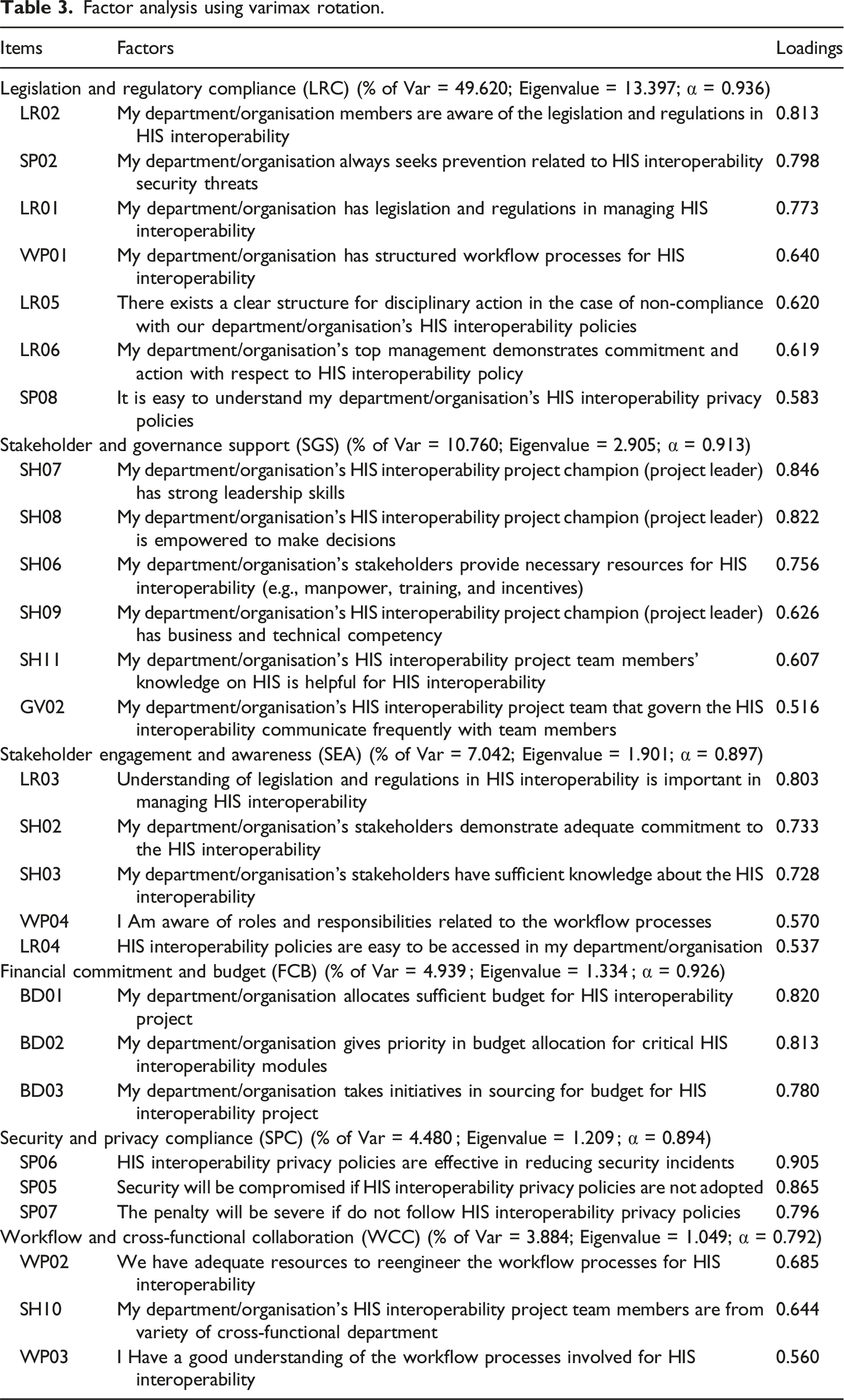
The first cluster, which included seven items from LR (4), SP (2), and WP (1), had the highest variance for HIS OIoP (49.620%). Hence, this factor was renamed Legislation and Regulatory Compliance (LRC). Items from SH split up into two factors, with items from GV, WP and LR to load as the second and third largest factor; therefore, the new factors were renamed as Stakeholder and Governance Support (SGS) with a variance of 10.760% (n = 6) and Stakeholder Engagement and Awareness (SEA) with the variance of 7.042% (n = 5). BD accounted for 4.939% of the variance, with all three items loading accordingly and renamed and Financial Commitment and Budget (FCB). Three split items from SP loaded with a variance of 4.480% as Security and Privacy Compliance (SPC), and the remaining three items from WP (2) and SH (1) formed as renamed factor Workflow and Cross-Functional Collaboration (WCC) with a variance of 3.884%.
All the CA values for the factors were larger than 0.8, indicating a high internal consistency of the survey items (Hair, 2011). All original hypotheses listed in Section 2.2 have been renumbered, and the following subsections reflect this.
Confirmatory factor analysis (CFA)
Reliability and convergent validity.
Discriminant validity – Fornell-Larcker criterion.
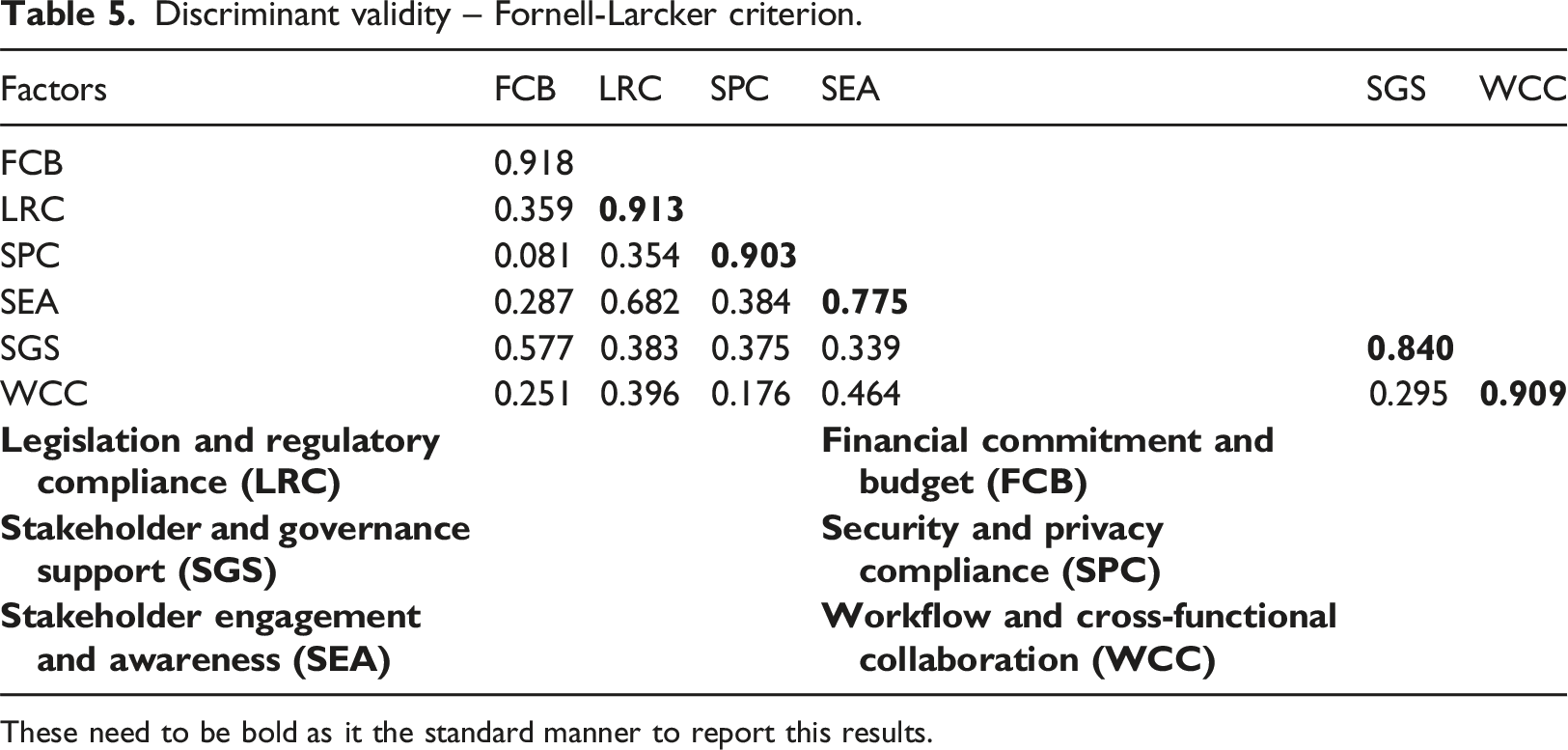
These need to be bold as it the standard manner to report this results.
Discriminant validity – heterotrait-monotrait ratio (HTMT).
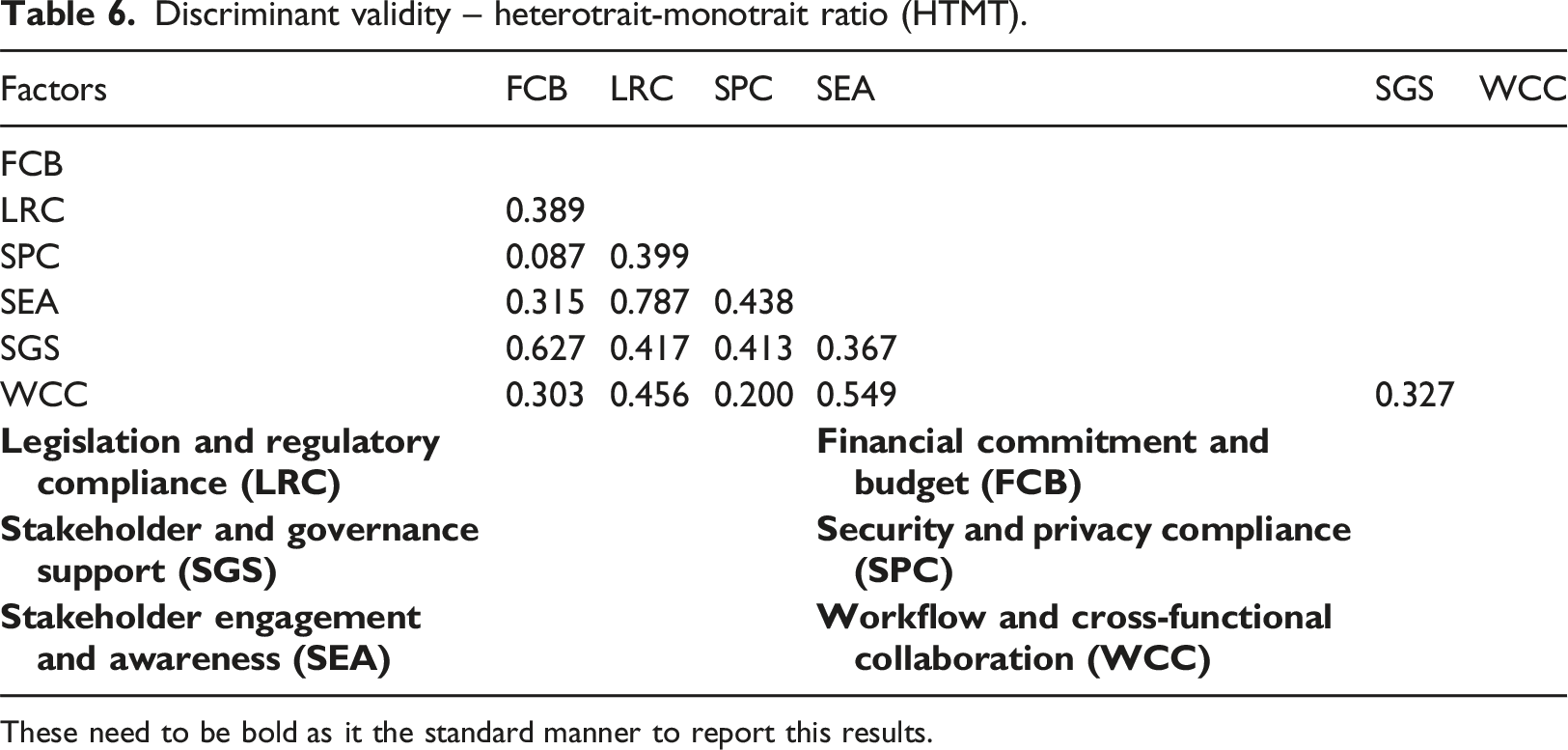
These need to be bold as it the standard manner to report this results.
Structured equation modelling (SEM)
Figure 2 shows the outcomes of the SEM analysis including path coefficients, the significance levels (p < .05), effect size and the R2 score for the dependent variable. Structured equation modelling for the OIoP model.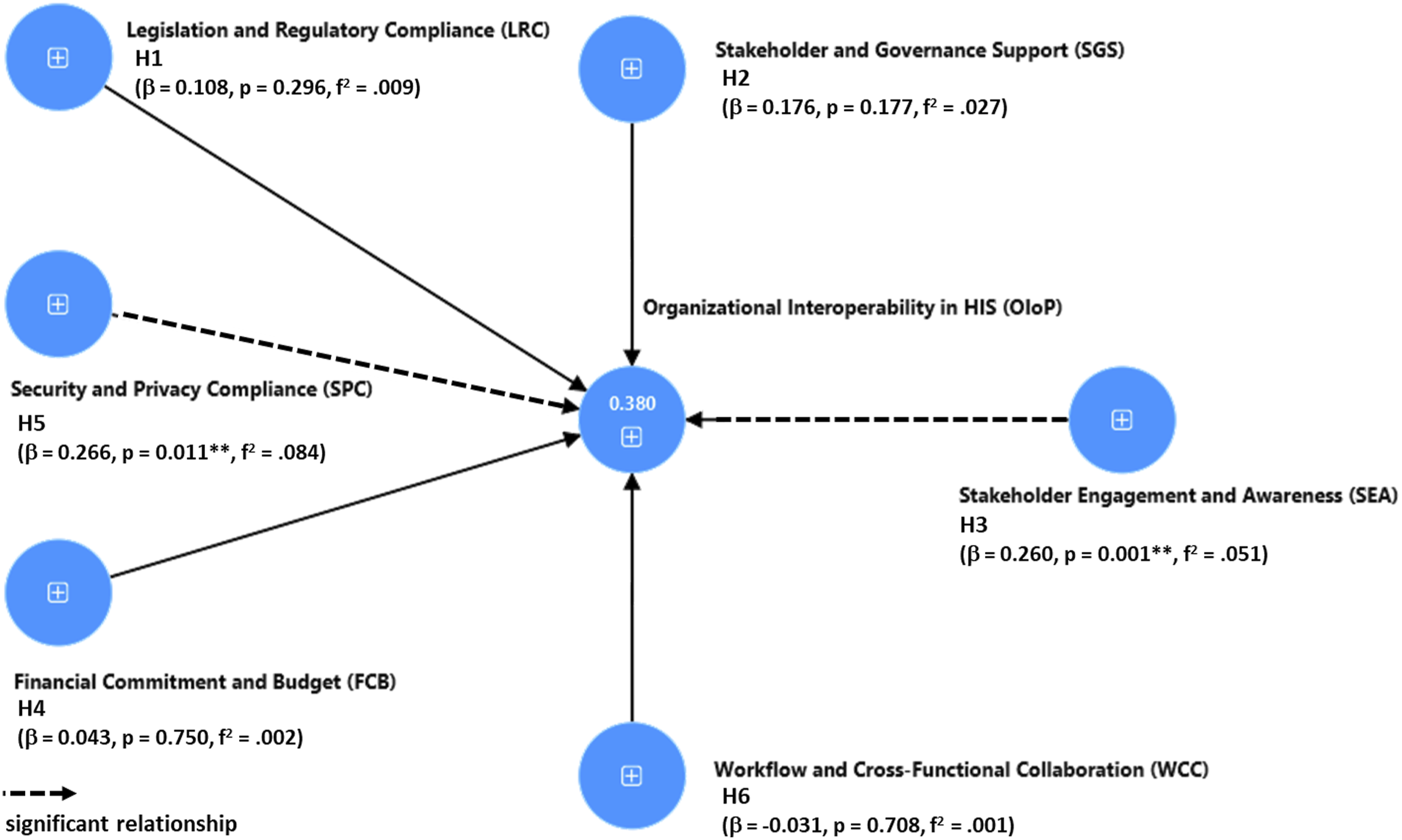
Summary of results and hypotheses testing.
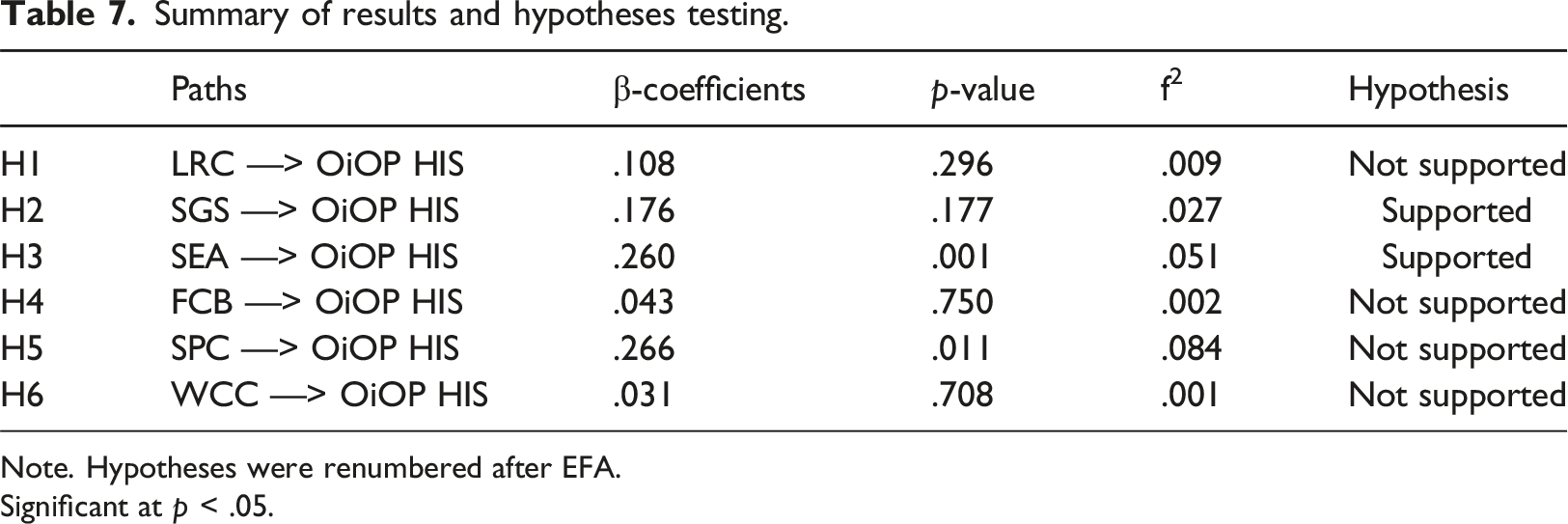
Note. Hypotheses were renumbered after EFA.
Significant at p < .05.
Discussion
HIS are essential for the delivery of high-quality patient care. The need for interoperability between different systems is critical to providing quality care to patients. The success of any organisation is dependent on its ability to effectively and efficiently share information across its different departments and stakeholders.51,52 The study was therefore undertaken to identify the institutional factors that affect the interoperability in HIS, focusing on the public hospitals in Malaysia.
Security and privacy concerns (SPC) were identified as the most significant factor influencing OIoP in HIS, hence underscoring the significance of SPC in safeguarding patient information and establishing trust in the success of HIS across several organisations. Implementing encryption, conducting regular security audits, and training staff on privacy can enhance OIoP by minimizing data breach risks. Analyzing the results, one can argue that compliance frameworks not only ensure legal requirements are met but also promote a culture of security awareness across all levels of healthcare provision. 53
Stakeholder engagement and awareness were found to be significant as well, indicating the importance of individuals including healthcare professionals, IT staff, policymakers, and patients, for the deployment and interoperability of HIS. Continuous dialogue, patient engagement, and education programs are key to creating interoperable, patient- centred systems and fostering a culture of innovation and adaptability in healthcare organizations. This finding is in line with Adus, Macklin 54 underscoring the value of patient engagement in designing systems that are not only interoperable but also patient-centred, thus enhancing the overall quality of care delivery.
Interestingly, the non-significant effects of local regulatory compliance (LRC), financial capacity/budget (FCB), and workforce competency/capacity (WCC) on OIoP suggest that, while necessary, these factors alone may not directly influence interoperability outcomes as much as one might assume. This could indicate that the quality of policies and the strategic alignment with external standards and expectations are more determinative of success in OIoP than simply having the financial resources or workforce capabilities. It may also suggest a threshold effect where, beyond a certain point, increases in financial resources or workforce capabilities do not correspond to significant improvements in interoperability. Moreover, the moderate positive impact of supportive governance structures (SGS) on interoperability, although just missing the conventional thresholds for statistical significance, suggests an area for further investigation. It indicates that governance structures which support open communication, collaboration, and shared decision-making could be instrumental in enhancing HIS interoperability.55,56
Practical implications
The study emphasises the critical need for comprehensive rules and regulatory frameworks to facilitate interoperability with HIS. It is imperative to prioritise the development of solid security and privacy policies, invest in stakeholder involvement and awareness, and gain strong governance support to improve HIS OIoP in Malaysian public hospitals. These measures will cultivate a culture of collaboration and compliance, which is crucial for the efficient sharing and management of patient information across healthcare environments. Ultimately, healthcare organisations may dramatically enhance the quality of patient care and operational efficiency in the digital healthcare ecosystem by addressing three critical institutional aspects.
Additionally, stakeholder participation and governance are crucial in achieving HIS interoperability. Healthcare organisations should prioritise stakeholder participation in decision-making processes related to HIS deployment and interoperability initiatives. This involves all key stakeholders, such as healthcare practitioners, IT experts, patients, and policymakers, to ensure successful communication and interaction. Effective governance structures, guided by a strong leader or project champion, can help ensure that all stakeholders share the goal of improving patient care through efficient information exchange.
Limitations and future recommendations
This study has several limitations: First, this study concentrated explicitly on institution-related factors, constituting only a part of a broader context. External factors unrelated to the institution, such as interoperability principles 57 and people-related factors, could also substantially impact HIS interoperability. These factors and their influence on attaining HIS interoperability could be the subject of future research.
Second, we employed self-reported data collected using surveys in this investigation. Future studies should adopt a multifaceted approach to address the issues of response and social desirability biases in research methodologies. This could include employing objective assessments, observational techniques, and self-report data to triangulate findings and enhance validity.
Finally, the study was done in Malaysia, specifically focusing on eight public hospitals. Therefore, our findings should be treated cautiously in terms of their generalizability. In generalizing to other countries including those from Southeast Asia that have similar cultural contexts, it is still important to consider similar healthcare information systems, and economic contexts that may influence healthcare outcomes across the region. 27 Therefore, adapting these findings requires careful consideration of each country’s unique demographic profiles, cultural nuances, and health priorities to ensure relevance and effectiveness.
Conclusion
Quality patient care requires HIS, but healthcare organisations may struggle with system interoperability, essential for effective patient care. An OIoP HIS model was developed and validated using a sample of 300 respondents through EFA and CFA. Results show the model to have an R2 of 38%, with two institutional factors having significant direct effects that ensure HIS organisational interoperability, namely SPC and SEA. By focusing on these factors, healthcare organisations can increase the likelihood of success in achieving OIoP and can ensure efficient information sharing, improve patient care, and safeguard sensitive data.
Supplemental Material
Supplemental Material - The direct effect of institutional factors on healthcare information systems (HIS) organisational interoperability in Malaysian public hospitals
Supplemental Material for The direct effect of institutional factors on healthcare information systems (HIS) organisational interoperability in Malaysian public hospitals by Saravanan Rajagopal, Vimala Balakrishnan and Yin Kia Chiam in Health Informatics Journal
Supplemental Material
Supplemental Material - The direct effect of institutional factors on healthcare information systems (HIS) organisational interoperability in Malaysian public hospitals
Supplemental Material for The direct effect of institutional factors on healthcare information systems (HIS) organisational interoperability in Malaysian public hospitals by Saravanan Rajagopal, Vimala Balakrishnan and Yin Kia Chiam in Health Informatics Journal
Footnotes
Acknowledgements
We would like to thank all participants for their time and effort in sharing their experiences and opinions in the survey.
Author contributions
SR, VB, and YKC contributed to the study conception and design. Data collection and analysis were performed by SR. SR wrote the manuscript and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.