
Abstract
Background
Cognitive function is a broad term for the mental processes involved in acquiring knowledge, manipulating information, and reasoning. Cognitive function includes the domains of perception, memory, learning, attention, decision-making, and language skills. 1 The decline in cognitive function in the advanced stages can be diagnosed as dementia according to the Diagnostic and Statistical Manual of Mental Disorders V (DSM-V). However, 50-67% of dementia conditions were undiagnosed in patients aged over 65 years2–4 With the increasing prevalence of dementia, intervention in the form of early detection and appropriate and immediate follow-up is needed. Early detection can be predicted by analyzing the patient’s cognitive complaints record, especially complaints of forgetfulness or memory disorders which are the most common cognitive complaints of dementia patients (54%). 5
Several studies have explored the use of telemedicine for diagnosing patients, including those with cognitive impairment. It can support history taking, cognitive and language assessment, and follow-up management.2,6 Telemedicine delivers healthcare through electronic communication, including phone calls, video conferencing, web platforms, and chat applications. In Indonesia, most chat-based telemedicine services rely on text messaging for history taking, with video calls added when needed for further assessment. 7
Telemedical service chat-based with internet and smartphone access allow patients to consult with doctors or other paramedics without having to meet in person. 8 Telemedicine helps overcome distance and geographic barriers, improving access to healthcare without the need for face-to-face contact. It offers a wide range of services and can expand care to large populations. However, limitations remain, including differing expectations between patients and clinicians, restricted physical examination capabilities, and concerns about data security and confidentiality.7,9
During the COVID-19 pandemic in Indonesia, many memory and high-function clinics suspended face-to-face services, leading to a decline in consultations for cognitively impaired patients and a risk of worsening illness. Telemedicine emerged as an effective alternative, enabling diagnosis, monitoring, management guidance, and referral for patients with memory complaints despite the limitations of in-person visits. To date, no research has examined the use of telemedicine for cognitive function in Indonesia, making this study the first of its kind. Globally, there is also a lack of research analyzing chat-based telemedicine for cognitively impaired patients using big data approaches. Such research is increasingly important, particularly during and after the COVID-19 pandemic, when health services have had to adapt to chat-based telemedicine to maintain care access. Telemedicine can capture outpatient complaints, support early detection, and provide timely management for patients with cognitive concerns. 6 This study describes the characteristics of patients with cognitive complaints who used chat-based telemedicine services in Indonesia and the factors that affect the physicians’ treatment and referral decisions.
Methods
This was a retrospective cross-sectional study using secondary data from the chat databases of four Indonesian telemedicine providers (Halodoc, Alodokter, Good Doctor, and Milvik) (Figure 1). Formal permission was obtained from each provider, and ethical approval was granted by the Health Research Ethics Committee. Flowchart of study procedures for data collection and analysis.
Chat-based teleconsultations begin when a patient or caregiver selects a consultation topic (e.g., forgetfulness) and is connected to a general practitioner (GP) or neurologist. The clinician conducts structured text-based history taking, exploring symptom onset, severity, daily impact, and red-flag features. When appropriate, the GP provides preliminary advice, prescribes treatment in accordance with regulations, or issues a referral to a neurologist or hospital.
Data were collected by total sampling from March 2020 to October 2021. For this study, the term “patients” refers to adult users (≥18 years) or their caregivers who submitted cognitive complaints which includes forgetfulness, memory loss, difficulty concentrating, word-finding difficulty, and related symptoms. Cases with incomplete demographic data or interrupted consultations were excluded.
Data retrieval
Secondary data were obtained by searching the chat database of each participating telemedicine provider using keywords such as “forgetfulness,” “memory loss,” “difficulty concentrating,” “difficulty focusing,” “difficulty getting words out,” “getting lost easily,” “difficulty understanding conversation,” and “difficulty finding objects.” All retrieved conversations were reviewed, and data were collected from records that met the inclusion criteria.
The independent variables, coded as categorical data, included: age (<40, 40–59, ≥60 years), sex (male or female), previous diagnosis of cognitive impairment (yes or no), complainant (patient or caregiver), responder type (general practitioner, neurologist, other specialist), patient’s cognitive complaint (forgetfulness/memory loss vs other symptoms), and whether an early cognitive screening test was performed (yes or no). The dependent variables were treatment decision and referral decision.
Data analysis
Data analysis was performed using IBM SPSS Statistics Version 20. Univariate analysis was used to describe patient characteristics as frequencies and percentages. Bivariate analysis was conducted to examine the association between patient characteristics and the two outcome variables (treatment decision and referral decision). Chi-square tests were used for categorical variables. When the expected cell count in the contingency table was too low to meet the assumptions of the Chi-square test, we used Fisher’s exact test instead. Variables with p < 0.25 in bivariate analysis were included in a multivariable logistic regression model to identify independent predictors. Results from logistic regression were reported as odds ratios (ORs) with 95% confidence intervals (CI), and p < 0.05 was considered statistically significant.
Result
Demographic data
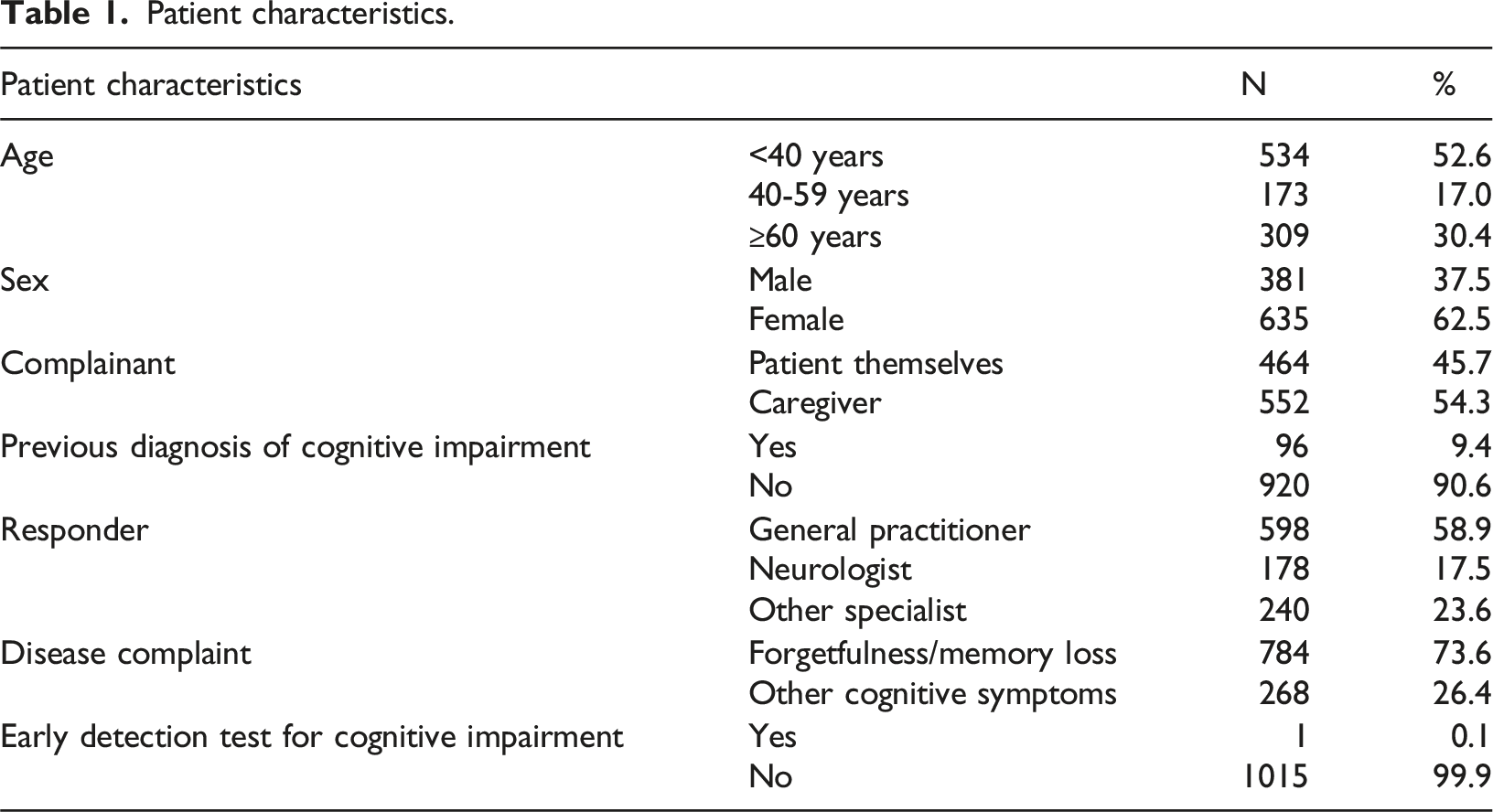
Patient characteristics.
Patient consultation outcome.

Bivariate analysis
Bivariate analysis of patient characteristic on treatment decision.
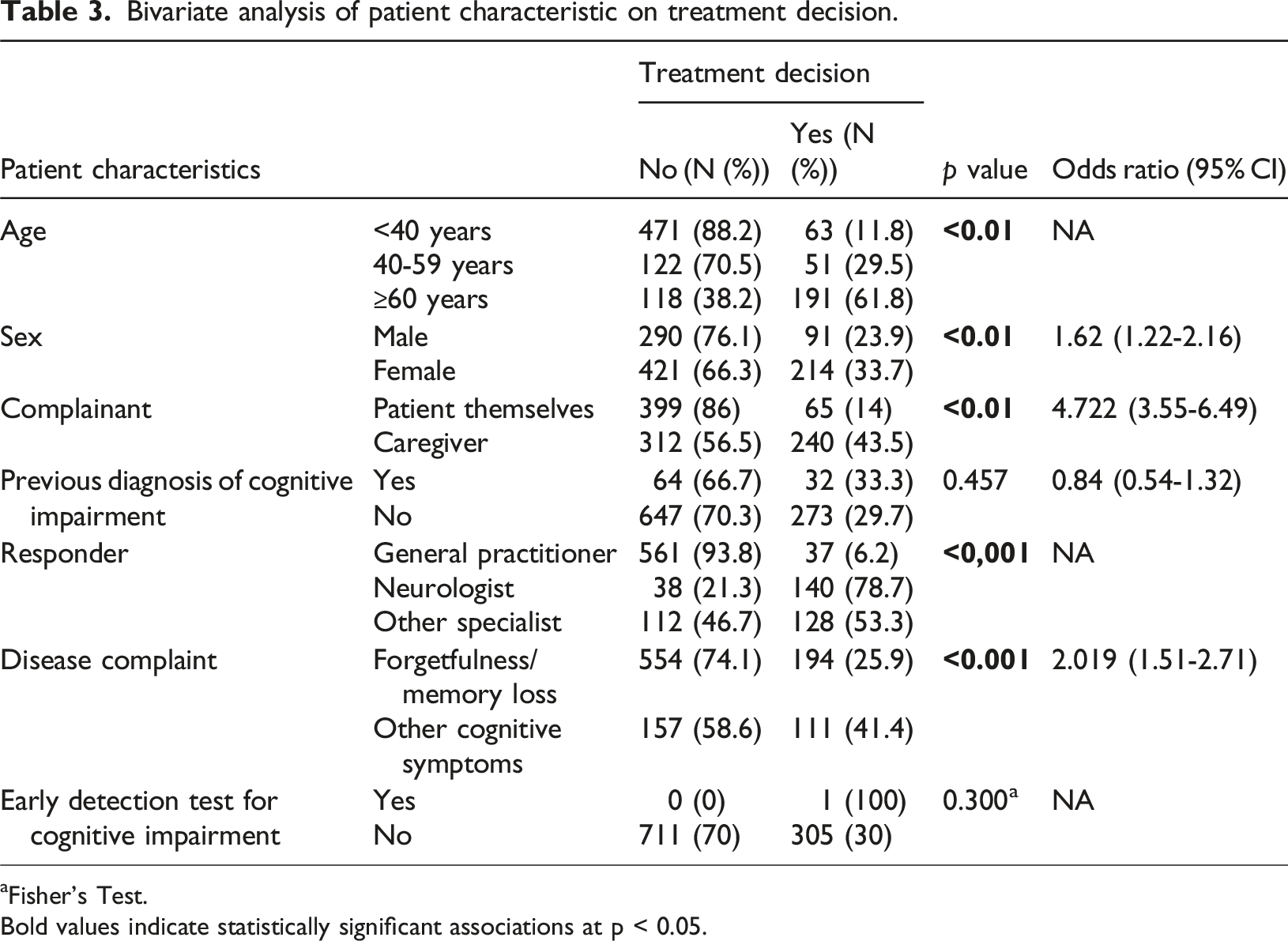
aFisher’s Test.
Bold values indicate statistically significant associations at p < 0.05.
Bivariate analysis between groups of patient age and respondents on treatment decision.
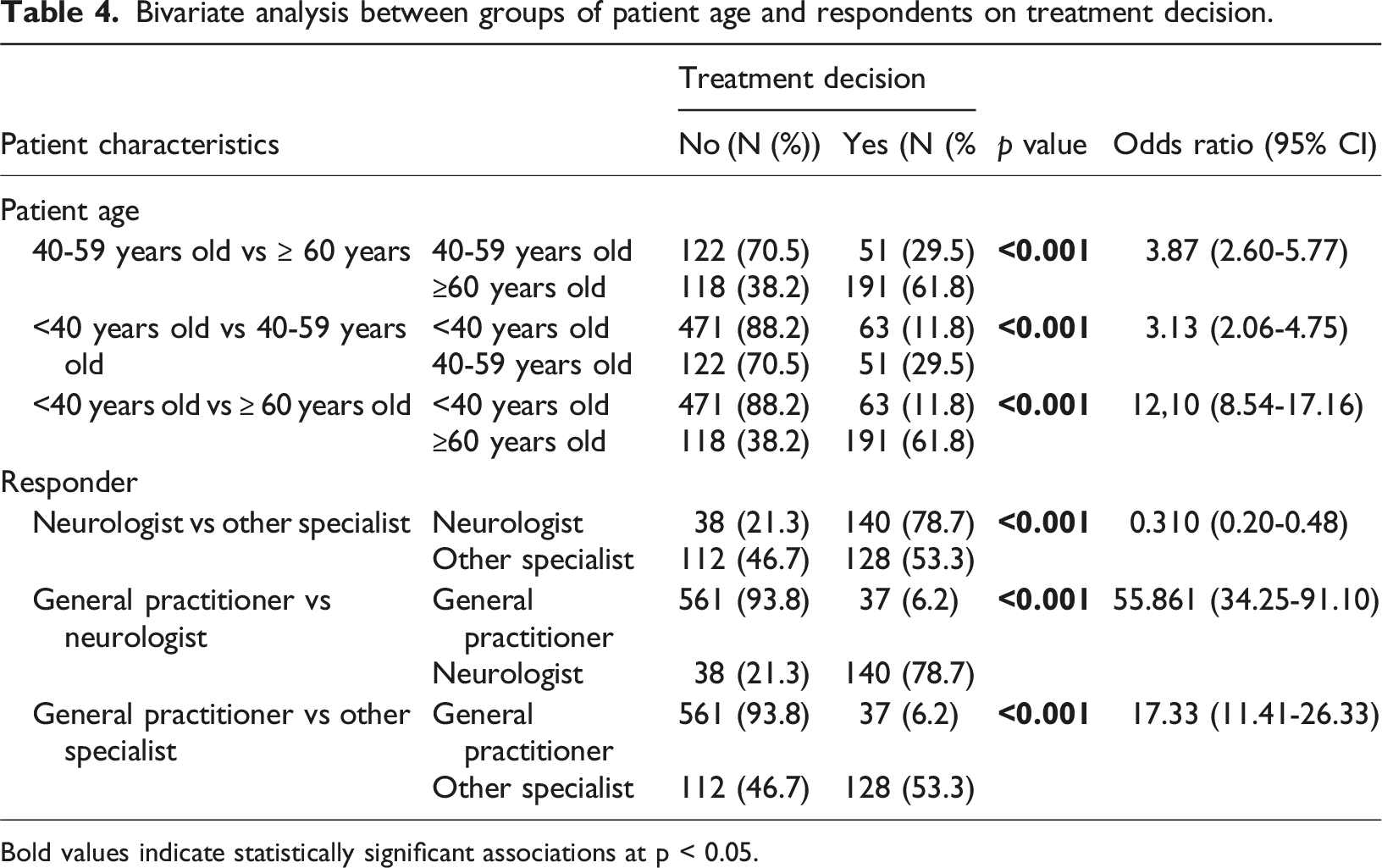
Bold values indicate statistically significant associations at p < 0.05.
Bivariate analysis of patient characteristic on referral decision.

aFisher’s Test.
Bold values indicate statistically significant associations at p < 0.05.
Bivariate analysis between groups of patient age and respondents on referral decision.

Bold values indicate statistically significant associations at p < 0.05.
Multivariable analysis
Multivariate analysis on treatment decision.

Bold values indicate statistically significant associations at p < 0.05.
Multivariate analysis on referral decision.
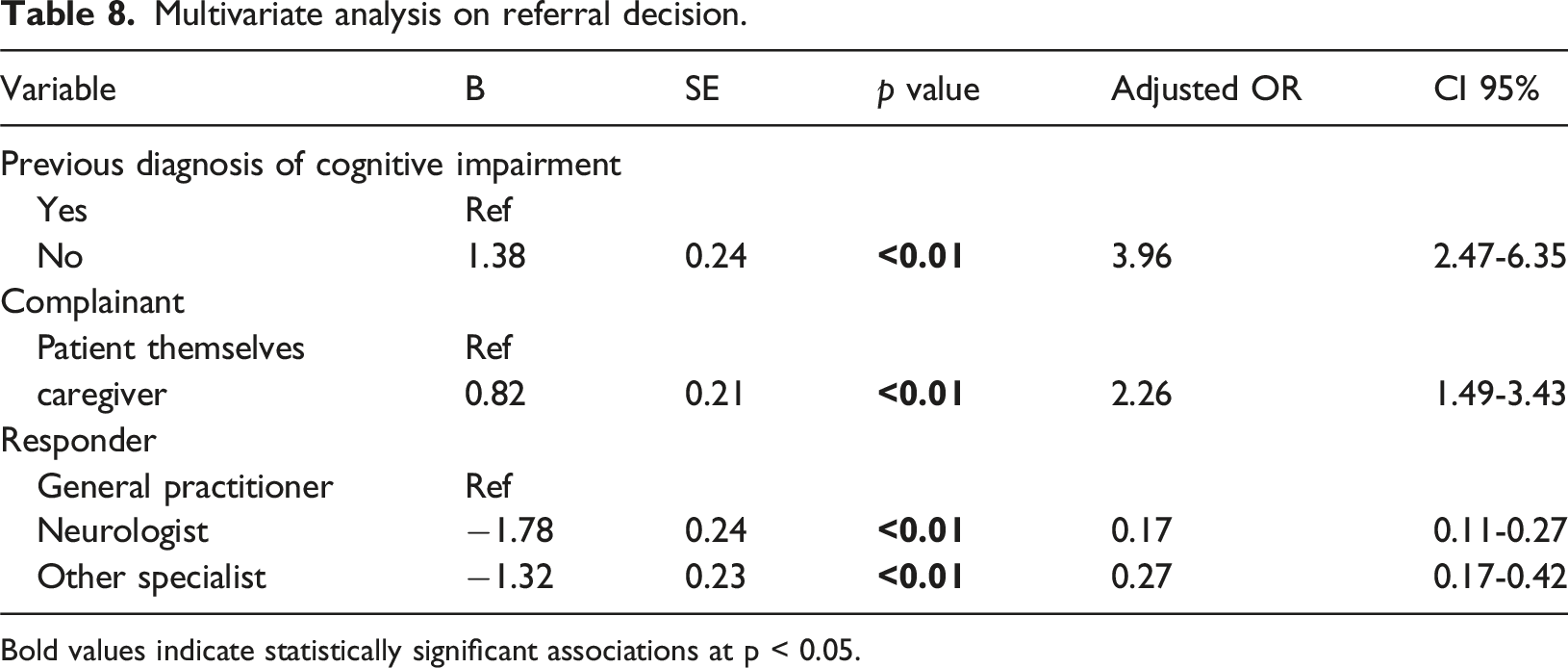
Bold values indicate statistically significant associations at p < 0.05.
Discussion
In this study, 1,016 consultations with cognitive complaints were identified from 1,801,996 total consultations, representing a prevalence of 4 per 10,000. This figure is lower than reported in a systematic review, which found that the global prevalence of cognitive disorders ranges from 5.1% to 41% and the incidence from 22 to 76.8 per 1,000 person-years. 10 These results differ from the global epidemiological data where the prevalence of dementia is 6.4%. 11 In addition, WHO also notes that there are 50 million people in the world who have dementia with 60% living in low to middle-income countries. 12 The low proportion of cognitive complaints observed in this study may reflect limited familiarity among Indonesian adults with using chat-based telemedicine to report memory concerns. Cultural perceptions that forgetfulness is a normal part of aging may also lead to underreporting and delayed medical attention. Among younger patients, forgetfulness is often attributed to depression rather than cognitive impairment, which may further inhibit diagnosis. Limited caregiver awareness can contribute to delayed recognition and reporting of cognitive problems. These findings are important because cognitive complaints can signal serious underlying conditions such as dementia, psychiatric disorders, or delirium.13–15
This study found that most patients with cognitive complaints were under 40 years of age, followed by those aged ≥60 years. This distribution differs from WHO data, which report that 5–8% of the general population aged ≥60 years have dementia at any given time. 12 Data from Central Norway also show an incidence of early-onset dementia of 14.8 per 100,000 person-years, suggesting possible underrepresentation of older patients in our sample. 16 This may reflect limited technology adoption among older adults, a finding similarly reported in U.S.-based telemedicine studies. 17
Female patients accounted for 1.7 times more consultations than males. This contrasts with previous studies on early-onset dementia, which report little difference between sexes.18,19 However, our finding is consistent with Hale’s study, which reported a slightly higher prevalence of cognitive impairment in females compared with males (21.2% vs 21.0%) and a higher prevalence of dementia in females (7.0% vs 5.4%). 20 This finding is also consistent with global data showing that dementia is more than twice as common in females as in males. In a recent study across 12 European populations, the prevalence of dementia ranged from 5.9% to 9.4%. 11 The higher proportion of females reporting cognitive complaints through telemedicine may reflect greater awareness and utilization of telemedicine services among women, a trend also observed in studies from the United States. 17
Over half of the complaints (54.3%) were submitted by caregivers, while 45.7% were submitted by patients themselves. Caregiver involvement is likely higher because patients with cognitive impairment may have difficulty using chat-based telemedicine platforms and are often more familiar with hospital-based services. Additionally, patients may have limited awareness of their deficits or provide minimal information about their symptoms. In those with subjective cognitive complaints, coexisting depression or anxiety may further influence the accuracy and reliability of the reported complaints.21,22 Cognitive complaints submitted by patients without cognitive impairment are often more accurate. Moreover, individuals with moderate to severe cognitive impairment may be unable to participate meaningfully in chat-based telemedicine consultations, limiting the quality of information obtained.
In this study, 9.4% of patients had previously been diagnosed with a cognitive disorder by a neurologist before their telemedicine consultation. The rise in telemedicine use for cognitive complaints during the COVID-19 pandemic likely reflects the greater vulnerability of cognitively impaired patients, especially older adults, who face higher risks of severe illness, ICU admission, and death when infected with COVID-19.23–25 This concern may make caregivers hesitant to bring patients for in-person consultations. In such cases, application-based telemedicine that combines mobile messaging, video, and chat features can help address the needs of patients and caregivers. Internet-based tools can also provide additional support through electronic reminders, cognitive stimulation activities, and daily task management.23,24 Beyond being cost-effective, remote telemedicine assessments can help protect cognitively impaired patients and their families from the risk of COVID-19 exposure in hospital settings.23,26 Telemedicine has also supported the implementation of public health strategies during the COVID-19 pandemic. 27
Of the 1,016 patients, 73.6% reported forgetfulness or memory loss. Patients aged ≥60 years were the second largest age group with cognitive complaints, consistent with a descriptive study by Mesiano and Samino (2010) of 56 older adults (>60 years) in Jakarta, which reported that 59% experienced cognitive impairment, with forgetfulness being the most common complaint (54%). 5 This also aligns with community-based studies reporting memory complaints prevalence of 25% to 50% in older adults. 28
In this study, 58.9% of cognitive complaints were managed by general practitioners, while only 17.5% were handled by neurologists. This reflects the triage process in chat-based telemedicine, where patients are typically directed to consult a general practitioner first, particularly when they are unsure which specialist to choose. Based on the consultation, the general practitioner may then refer the patient to a neurologist or other specialist as appropriate.
Most patients did not receive treatment (70.1%), either pharmacological or non-pharmacological. Bivariate analysis showed significant associations between treatment provision and age, sex, complainant, prior diagnosis of cognitive impairment, responder type, and type of complaint. In the multivariable model, sex, responder type, complaint type, and prior diagnosis remained significant predictors. Neurologists and other specialists were more likely to provide treatment compared with GPs, consistent with their role in definitive management. General practitioners tended to focus on initial recognition and referral, which may be due to limited familiarity with cognitive disorder therapies and regulatory restrictions on prescribing psychiatric medications via chat-based telemedicine.29,30
Sex may have influenced treatment decisions, as most telemedicine users in this study were female, making women the largest group to receive treatment. Patients with a prior diagnosis were also more likely to receive treatment, likely because physicians continued established therapy. Clinicians may have been more confident treating cognitive complaints other than forgetfulness or memory loss, whereas the high volume of memory-related complaints may have prompted more referrals rather than direct treatment.13–15,30,31
Referral decisions were common (81.1%), most often to neurologists (31.8%). Age was a significant predictor, with patients ≥60 years more likely to be referred, consistent with the higher dementia prevalence in this age group.12,32 In multivariable analysis, prior diagnosis, responder type, and complainant were independent predictors of referral. Referrals were more frequently given to patients with prior diagnosis of cognitive impairment, often after being assessed by a general practitioner. A clear diagnosis facilitates referral for further examination or follow-up therapy to a neurologist, in line with dementia management practices in Indonesia. 30 Patients treated by a neurologist were less likely to receive a referral, as neurologists can manage and monitor non-emergency cases directly through telemedicine. 33 Complaints submitted by family members were more likely to result in referral, as they were generally clearer and more detailed, giving physicians greater confidence to make referral decisions.21,22
The high proportion of referrals observed in this study aligns with the role of telemedicine as an initial point of consultation, focusing on prevention, early detection, and timely diagnosis before definitive treatment. Telemedicine is particularly valuable for elderly patients with cognitive complaints, allowing neurologist consultations and follow-up therapy, both pharmacological and non-pharmacological, without the need for face-to-face visits. This approach is especially beneficial during the COVID-19 pandemic and for patients in rural areas with limited access to neurologists, thereby improving continuity of care.34,35
During the study period, cognitive assessment relied on history taking and patient- or caregiver-reported complaints, as no validated telemedicine-adapted MoCA (t-MoCA) was available in Indonesia. Objective cognitive screening was not systematically performed, which may introduce variability in clinical judgment and limit comparability between cases. Although some clinicians advised MMSE or MoCA testing during offline follow-up visits, this was not consistently performed or recorded. Future telemedicine workflows should integrate validated screening tools with clear threshold values to ensure standardized and reproducible cognitive assessments. Objective screening using validated thresholds (MMSE <24/30, MoCA <24/30, AD8 ≥2) would allow for a more standardized and reproducible assessment. 36
MMSE and MoCA examinations can be performed using telemedicine services. Research shows that MMSE can be carried out with the help of collaborators, and patient responses are recorded between remote nurses and direct nurses so that the results can be compared. Meanwhile, visual items are obtained with photos or fax copies.37,38 For MoCA testing, video teleconferencing is preferable as it allows patients to interact visually with the physician and view test materials in real time. Physicians also benefit by observing facial expressions, assessing visuospatial functions, and confirming patient comprehension during the examination.39–42 Even with videoconferencing, factors such as video and audio quality, camera positioning, and internet connectivity must be optimized to ensure accurate and reliable assessment.40,42,43 High inter-rater reliability has been demonstrated between face-to-face and telemedicine-administered MoCA, supporting its use in remote settings. 33
Limitations
This study is the first to characterize cognitive complaints in Indonesian telemedicine services using chat-based user data, and as such, there was limited literature available for direct comparison. This study has several limitations. First, the cross-sectional design of this study precludes causal inference. Second, the data were derived from chat transcripts, and detailed clinical diagnoses were not available for most participants, limiting the ability to stratify by specific cognitive disorders. Third, age was recorded in broad categories (<40, 40–59, ≥60 years), and raw data were not retained outside the telemedicine providers’ secure servers, preventing reanalysis with finer age bands, which may have captured greater variability in technology use and cognitive risk among older adults. Fourth, our data were derived from chat transcripts, detailed clinical diagnoses were not available for most participants. As a result, the findings should be interpreted as reflecting patterns of telemedicine use and decision-making for cognitive complaints rather than outcomes in a specific, confirmed diagnostic group.
Additionally, keyword search results were categorized on-site at the telemedicine providers’ offices, and raw data could not be taken off-site. As a result, we were unable to retain the exact number of hits for each individual keyword. Because most retrieved complaints were related to forgetfulness or memory loss, other cognitive complaints were grouped together, limiting our ability to explore the diversity of less common complaints. Finally, because data collection occurred during the COVID-19 pandemic, utilization patterns may not fully reflect post-pandemic telemedicine trends.
Conclusion and future directions
This study is the first to describe cognitive complaints in Indonesian chat-based telemedicine services using large-scale user data. This study revealed that treatment decisions were more likely when patients were aged ≥60 years, female, had complaints other than forgetfulness/memory loss, no prior diagnosis of cognitive impairment, and were consulted by a neurologist or other specialist rather than a general practitioner. Referral decisions were more likely when complaints were submitted by caregivers and when patients already had a prior diagnosis of cognitive impairment, but were less likely when consultations were handled by neurologists or other specialists (who often completed management in the same session). Together, these findings show that both patient characteristics and provider type strongly influenced whether patients received treatment or referral through telemedicine.
Chat-based telemedicine plays an important role in early detection and triage for cognitive complaints and may improve care access, particularly for older patients and those in underserved areas. To optimize its use, telemedicine platforms should integrate standardized diagnostic pathways, validated cognitive screening tools (MMSE, MoCA, t-MoCA, AD8), and structured referral workflows. Training healthcare providers to recognize cognitive deficits and deliver individualized interventions is crucial for improving care quality. Future research should also examine post-pandemic data and explore more granular age categories to better capture variability among older adults.
Footnotes
Ethical approval
This research has been approved by the Ethics Committee of the Faculty of Medicine, the University of Indonesia with the number-letter: KET-669/UN.2F1/ETIK/PPM.00.02/2021 and conducted in accordance with the Helsinki Declaration. Researchers were not involved with the patients or the telemedical service providers directly.
Inform consent
As researchers were not directly involved with patients or telemedical service providers and the study utilized anonymized secondary data, informed consent was not required.
Author contributions
Pukovisa Prawiroharjo, Irma Widyasari, and Iskandar Purba Geraldi conceptualized the study. Yetty Ramli and Adre Mayza conducted data analysis. Diatri Nari Lastri prepared the initial draft. Dinda Nisrina helps conceptualize and writing of the final manuscript. All authors reviewed and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The author affirms that the journal is committed to facilitating openness, transparency, and reproducibility of research.