
Abstract
Keywords
Introduction
Transitional care (TC) encompasses the provision of healthcare services tailored to facilitate smooth transitions for patients across their care continuum. These transitions could involve discharge from a hospital setting, transfer to a primary care facility, a rehabilitation unit or alternative hospital, or transfer between different units within the same hospital. 1 The transitional care process is inherently complex and can be disrupted by poor coordination among healthcare providers or between providers and caregivers. Insufficient collaboration and coordination in transitional care pose risks to the continuity of care.2,3 Furthermore, inadequately implemented transitional care can cause delays in discharge 4 and increase unplanned re-admissions. 5 Effective transitional care often requires a holistic approach that considers how an illness or condition impacts daily life and how patients and caregivers can manage symptoms at home. 6 The accountability for successful transition care should rest collectively with the clinical team and organization, in collaboration with patients and caregivers. While there has been growing recognition of the importance of transitional care in recent years, it remains an underemphasized area in health policy.7,8
To address these challenges, different interventions have been developed for transitional care.9,10 Interventions can be delivered pre- and post-discharge, or they can be bridging interventions.9,11,12 Pre-discharge interventions typically contain elements such as patient education, discharge planning and advanced care planning, while post-discharge interventions can be based for example on home visits and telephone follow-ups.9–11 Decision support tools are increasingly used in transitional care as bridging interventions to assist healthcare professionals in managing the complexities of patient transitions, such as facilitate communication, improve and standardize clinical decision-making, and enhance patient outcomes. They have been implemented in various healthcare contexts, including acute care discharge planning, 13 long-term care facilities, 14 and hospice care. 15 They have demonstrated potential in improving medication management, preventing pressure ulcers, and reducing hospital readmissions. 14
Among the various forms of decision support, digital tools offer significant potential for improving transitional care by enhancing information flow, enabling risk stratification, and assisting clinicians in making data-driven decisions. Many transitional care interventions now leverage technology such as electronic medical record-integrated tools, electronic discharge summaries, and electronic patient instruction notes. 12 Mobile applications16,17 and remote monitoring systems12,18 further expand the capabilities of decision support by providing continuous patient oversight beyond clinical settings. These digital solutions can also identify overlooked issues and reduce biases inherent in single time-point assessments 19 ensuring a more comprehensive overview for the healthcare professional.
While new technologies hold great potential, their introduction to clinical practice must be approached with caution, as they can significantly impact clinicians’ roles, workflows, and workforce dynamics. 20 Ensuring that digital decision support tools are user-friendly, seamlessly integrated into existing systems, and supported by adequate training is essential for successful implementation.15,21 Moreover, actively involving healthcare professionals in the design and implementation of these technologies is crucial to ensuring their relevance, usability, and effectiveness in real-world clinical settings. 22
Despite the growing recognition of the importance of incorporating healthcare professionals’ experiences in the development of transitional care interventions, research addressing this issue remains limited. 23 Existing studies have examined healthcare professionals’ perspectives in various phases of care, such as triaging emergency calls 24 and the use of AI in triage, 25 hospital to home care 26 and virtual care delivery. 27 However, these studies often focus on specific aspects of care and do not take a holistic view of the entire transitional care process. Several studies have investigated clinicians’ perspectives in transitional care28,29 but these often neglect to explore the role of technology in supporting healthcare professionals during care transitions. Given the evolving landscape of healthcare technology, it is crucial to consider healthcare professionals’ perspectives when identifying the barriers and enablers of technology in transitional care. Their insights are vital for ensuring that technological solutions are appropriately designed and integrated into existing workflows. 30
Study rationale & objectives
To bridge this gap, this study aimed to explore healthcare professionals’ perspectives on the use of technology in supporting decisions during transitional care processes. We aimed to:
Aim 1: Understand the challenges healthcare professionals face in transitional care, Aim 2: identify key steps and procedures needed to address these challenges, Aim 3: examine the key factors for the adoption of technological tools in transitional care to address these key reforms. We should clarify that this study focuses on transitional care processes within adult healthcare settings and does not address transitions from paediatric to adult care.
Methods
Theoretical underpinning
This study follows a Generic Qualitative Inquiry (GQI) approach, guided by pragmatism to explore real-world perspectives on technology in transitional care. 31 Data were collected through semi-structured co-creation sessions. We argue that co-creation sessions facilitate the creation of shared meanings, aligning with social constructionism 32 and further supported by pragmatism, as it prioritizes practical problem-solving through real-world engagement. Additionally, saliency theory 33 suggests that participants naturally prioritize issues that are most relevant to their experiences and concerns which allows us to capture the lived experiences of healthcare professionals in transitional care.
Study design
This study represents the first phase of a transnational feasibility study 34 , using a prospective qualitative multisite design. A common protocol was developed to harmonize co-creation sessions, allowing consistency while accommodating the specific needs of participants and settings. Sessions were aligned with the study’s research questions and focused on two core themes: clinical decision-making and the use of technology in transitional care. Each theme was explored from three angles: current status, challenges, and future developments.
No standardized or validated questionnaires were used in this study. Instead, a shared session template was created based on the Living Lab Harmonization Framework, 35 including themes, perspectives, guiding questions, and reporting guidelines (see Appendix A). These guides were designed for exploratory, dialogic engagement rather than quantitative assessment and were not intended to function as validated instruments. Consequently, no copyrighted or proprietary tools were used. The sessions were held in person and took place within the physical environments of each Living Lab. Each session was conducted once and no repeat sessions were held. Each session lasted for about 2 h and began with an introduction to the broader study aims and co-creation session goals, followed by an introduction to the concept of transitional care to ensure a shared understanding.
Sessions were led by trained facilitators and assistant moderators from established research infrastructures with co-creation expertise. All participating organizations were certified Living Labs by the European Network of Living Labs (ENoLL) and recognized Research Infrastructures in the VITALISE H2020 project, ensuring methodological rigor. A working relationship was established prior to the start of the study, as participants were recruited through the networks of each participating Living Lab.
Researcher characteristics and reflexivity
The research team included members with diverse backgrounds, including engineering, biomedical engineering, innovation management, psychology, and medicine. The lead researcher (DP) has an engineering background, which may have introduced a bias toward viewing technology as a solution. To address this, data coding and interpretation were carried out collaboratively with an innovation manager and a biomedical professional. Input from psychologists and medical professionals ensured a balanced, multidisciplinary perspective. Reflexive discussions were held throughout the research process to critically examine assumptions and enhance the credibility of the findings.
Data collection
Data collection was performed between April to December 2022. All participants were asked to complete a demographic questionnaire capturing key background information, including age range, gender, education level (classified according to the ISCED framework), 36 self-reported digital literacy, and years of experience in medical practice. Participants were also asked to specify their area of specialty in an open-ended field. Notably, demographic data were not collected for participants from Finland, as they were nursing students. Given their status as trainees rather than established professionals, their insights were considered valuable in understanding future workforce perspectives. Furthermore, all nursing students had clinical placement experience in various healthcare settings.
Given the nature of the study, reflective diaries were maintained by the facilitator and assistant moderator throughout the process to capture insights, reflections, and observations related to the discussions. Instead of transcripts, detailed notes were taken during each co-creation session. These notes included group data focusing on collective views and shared experiences, rather than individual opinions. The notes captured key themes, points of agreement or disagreement, and non-verbal cues that emerged during the discussions. The data analysis was based on these notes, including a thorough review of the co-creation sessions data, and any summary comments made by the facilitator or assistant moderator after each session. 37
Participants
This study utilized convenience sampling combined with purposive sampling methods to select participants who could provide rich insights. The target population includes healthcare professionals who are directly involved in or have experience with the transitional care process. Participants were selected based on their expertise, role, and experience in clinical or rehabilitation settings.
The following groups were targeted. • Doctors: Regardless of discipline, to capture a diverse range of medical perspectives on transitional care. • Nurses: Working in hospitals, rehabilitation centres, or any clinical settings, as key figures in patient care transitions. Nursing students with clinical placement experience were included • Psychologists and Social Workers: Those working or having worked in clinical or rehabilitation settings, to explore the psychosocial factors affecting transitional care. • Healthcare Technology Designers/Researchers: Individuals involved in the design and development of healthcare technologies, to understand the alignment of technology with care needs and challenges.
Data analysis
The constant comparison analysis method
38
was employed to systematically examine the data. The analysis followed three major stages. • Open Coding: A descriptive code assigned to each smaller data chunk to capture its meaning. • Axial Coding: The codes were then grouped into categories based on conceptual similarities • Selective Coding: The final step involved refining these categories into overarching themes expressing the content of each of the groups
Three independent researchers conducted the analysis using a manual coding approach developed in Microsoft Excel. Each researcher independently coded the data, and discrepancies were resolved through a consensus meeting to define the final themes. The constant comparison analysis method was selected as it aligns with the study’s focus on capturing shared understanding among participants and producing real-world experiences through an iterative process. Participants did not provide further feedback on the findings.
After the definition of the main themes, the data assigned to each theme were grouped into challenges and issues corresponding to research Aim 1, and potential solutions were extracted corresponding to research Aim 2. To further explore the interconnections between themes, an impact relationship analysis was performed, drawing from the methodology of axial coding 38 corresponding to research Aim 3 and the identification of key technological reforms. Each independent researcher examined how improvements in one area might trigger improvements in another, based on the collected data. Specifically, the analysis focused on “if improves… then … will improve as well” reasoning. Following individual assessments, a consensus meeting was conducted, where researchers compared and validated their findings, to conclude a common mapping.
Ethics
Information about ethics applications and approvals.

Results
Participants
Co-creation session participants per country.
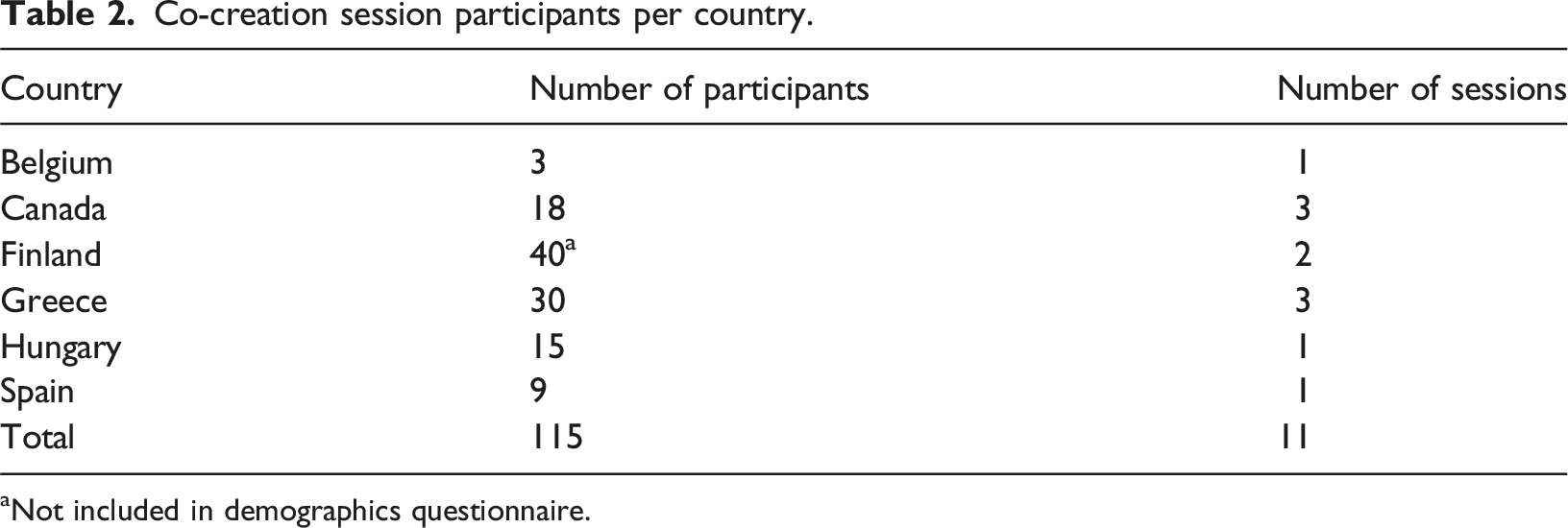
aNot included in demographics questionnaire.
The most common age range was 30–35 years (13/75, 17.34%), with a relatively uniform distribution across other age groups. The majority of participants were female (38/75, 50.67%) and held a Master’s degree or higher (51/75, 68.00%). In terms of technological knowledge, 27 participants (36.00%) reported having advanced or excellent proficiency, while 30 participants (40.00%) chose not to respond to this question. The participants had an average of 14.06 years of professional experience (SD = 12.21). The participants represented a diverse range of specialties, with a notable emphasis on Research, Development, and Innovation (R + D + I) (23 professionals), Social Care (18 professionals), and Medical Practice (13 medical doctors). Additionally, Psychology (7 professionals) and Medical Education (4 professionals) were also represented, reflecting a multidisciplinary perspective in the study. Detailed participant characteristics are presented in Table B1 of Appendix B.
Themes and findings
Summary of findings.

Detailed description of findings is presented in Appendix C.
Impact relationships.

arefers to indirect impact, through improving digital tools.
Discussion
Main findings
This qualitative, multisite study explored healthcare professionals’ perspectives on the existing challenges in transitional care, the key steps required to address these challenges and how technology can support this transitional care reform. In line with our research aims, Aim 1 (understanding the challenges) is addressed through the identification of five key processes in transitional care, highlighting associated technology-driven challenges. Aim 2 (identifying key steps and procedures) is addressed through the mapping of potential solutions and improvement strategies, while Aim 3 (examining factors for technology adoption) is addressed by identifying five themes related to technology and three overarching themes influencing these processes (Table 4). Our findings identify five key processes in transitional care, highlighting associated technology-driven challenges and potential solutions. Also, we identified five themes related to technology and how they can affect these processes as well as three overarching themes (Figure 1). Transitional care processes.
Our findings highlight the critical role of collaborative decision-making at all stages of the transition. However, it remains largely professional-centered, with physicians making discharge and follow-up decisions in the absence of clear protocols 39 often excluding patients and families. Healthcare professionals advocate for greater patient and caregiver participation but acknowledge that fragmented or insufficient information often hinders informed choices. This aligns with previous studies39,40 highlighting the technological barriers older patients face in digital decision-making processes. However, this may shift with the next generation of older adults, as their engagement in health is expected to grow alongside a narrowing digital divide. 41
A common theme that arose across the processes was the lack of protocols or the lack of harmonized practices. Standardization is considered an essential goal of care pathways. 6 While standardization can exist within specific levels of care, inconsistencies across settings disrupt smooth transitions and create challenges for developing and implementing decision support tools. Even when protocols are available, they are often either not used or not uniformly applied.
Regardless of the care setting or country, healthcare professionals have highlighted significant concerns regarding resources, privacy, and trust in technological tools. Resource shortages are global issue, 42 affecting also technology integration. Privacy concerns, particularly regarding the security of personal data, were emphasized, highlighting the delicate balance between protecting patient information and enabling efficient data exchange. While patients have also expressed privacy concerns,43,44 evidence suggests that patients recognize the potential benefits of data sharing and may perceive them as outweighing the risks of data breaches. 45 Furthermore, trust in healthcare technology emerged as a critical factor, underscoring the need for reliable and up-to-date information to support decision-making.
Our findings highlight the critical role of digital tools in supporting transitional care reform (Table 4). Mobile applications enhance communication between patients and healthcare providers, facilitating collaborative decision-making and post-discharge follow-up, including homecare services. 46 Wearables and dashboards support pre-discharge assessments by integrating physical, mental, psychological, and socio-economic factors into comprehensive care plans 47 and integrating mental, psychological, physical, and socio-economic factors into the evaluation process. ICT literacy is considered essential for interpreting information from such devices, enabling more informed, holistic clinical decisions. Digital literacy further strengthens post-discharge support, as many services depend on technology and limited skills may hinder engagement.
According to our findings, interoperability can play a critical role in the improvement of follow-up and post-discharge support by ensuring seamless data exchange across different levels of care. Lack of interoperability was identified by healthcare professionals as key challenge in similar studies. 40 Similarly, a well-structured data strategy enhances collaborative decision-making, discharge protocols, and patient assessment. Centralized patient tracking systems can provide real-time data access, supporting informed, interdisciplinary decisions 48 while digital records and continuous monitoring offer objective insights into patient status. However, a recent systematic review 49 indicates that none of the 15 reviewed transitional care models (TCMs) used electronic health records to to share information across settings, and only 5 used electronic medical records (EMRs) to facilitate communication between health care providers.
User-friendliness seems to have an indirect impact on transitional care processes by improving the adoption of digital tools and digital literacy. By providing simpler and more understandable information to users, user-friendliness is closely linked to the emerging concept of explainability. 50 Co-creation has been proposed as a strategy to enhance user-friendliness, aligning with previous research that highlights participatory design as a key factor in promoting the adoption of digital health technologies. 44
Alignment with existing transitional care frameworks
Our analysis relates to the Screening component of the Transitional Care Model, 51 which emphasizes the importance of identifying patients at risk of poor outcomes and tailoring personalized interventions. Our findings suggest that advancements in digital tools can support the development of a holistic, explainable, and patient-centered approach that provides healthcare professionals with insights into patients’ capacities and recommends appropriate care pathways. While aligning with the Transitional Care Model’s focus on physical, mental, and cognitive health, our findings also highlight the importance of incorporating social status as a key factor in care planning.
Our findings align with the SELFIE framework, particularly in the domains of “Information & Research” and “Technologies & Medical Products”. 52 At the micro level, both our study and the framework emphasize the role of ICT in facilitating information exchange. At the meso level, we highlight the critical need for interoperability to ensure seamless transitions in care. While the micro-level perspective in SELFIE includes care pathways and the concept of a ‘patient journey record,’ our findings advocate for a more holistic patient evaluation—one that goes beyond disease management to consider the individual’s overall capacities, including mental, physical, and social factors. Furthermore, our results reinforce the importance of multidisciplinary research, aligning with the co-creation approach promoted in the SELFIE framework.
Study considerations
This study does not aim to exhaustively address all issues and facilitating factors related to transitional care and technology adoption. Although participant numbers varied across sites, the multisite approach offers a broader perspective on healthcare systems, supporting the generalizability and relevance of our findings across different contexts. While cultural and systemic differences between sites were not explicitly analysed, we focused on identifying overarching themes that emerged across diverse settings.
We acknowledge that formal strategies to assess data saturation were not employed. Given the exploratory nature of the study and the focus on collective dialogue within co-creation sessions, our primary aim was to capture a breadth of perspectives rather than reach thematic saturation. This approach was also influenced by resource constraints and the methodological choice to prioritize depth and context over quantity. We deliberately chose not to produce full meeting transcripts, as our interest lay in group dynamics and shared experiences rather than individual statements. Another limitation of this study is the absence of formal translation protocols for the interview guide. We would also like to acknowledge that no formal translation protocols were applied, which may have influenced the contextual interpretation of certain terms or concepts across different linguistic and cultural settings.
In addition to healthcare professionals, some participants were nursing students. Despite their limited clinical experience, gained through placements and substitute roles, they contributed valuable insights, offering fresh perspectives on transitional care and technology use.
Conclusions
This study addresses the gap in understanding the role of technology in transitional care from the perspective of healthcare professionals.
Key challenges are captured within the overarching themes of trust, resources, and privacy, while specific aspects of the transitional care process also present distinct challenges, such as the lack of harmonized protocols and limited involvement of patients and family members in the transitional care process. Digital tools have emerged as a critical means to address these challenges and support transitional care reform. They can facilitate better communication among all actors, enable holistic and harmonized evaluations using tools such as wearables, ensure continuous information flow, and support centralized decision-making. The design of technology and digital tools should prioritize user-friendliness and adopt user-centric methodologies, such as co-creation.
Future research should evaluate the implementation and effectiveness of technology-driven interventions in transitional care. Studies could examine how technology enhances information flow across settings and stakeholders, and its impact on decision-making and standardization. Further research should also explore strategies to improve user-friendliness and assess the effectiveness of co-creation approaches in technology design. Overall, technology in transitional care requires a dedicated agenda and tailored strategies to address the multiple and complex factors affecting adoption, in order to realize its full potential benefits.
Supplemental Material
Supplemental Material - Healthcare professionals’ perspectives on technology in transitional care: A multisite qualitative study on current practices, challenges, and future directions
Supplemental Material for Healthcare professionals’ perspectives on technology in transitional care: A multisite qualitative study on current practices, challenges, and future directions by Despoina Petsani, Teemu Santonen, Beatriz Merino Barbancho, Eva Kehayia, Mika Alastalo, Dorra Rakia, Vasileia Petronikolou, Sofia Segkouli, Rosa Almeida, Gloria Cea Sanchez, Sofía Ballesteros, Sara Ahmed5, Enikő Nagy, Leen Broeckx, Michael Doumas, Panagiotis Bamidis and Evdokimos Konstantinidis in Health Informatics Journal.
Footnotes
ORCID iDs
Ethical considerations
As this was a multisite study conducted across six countries (Belgium, Canada, Finland, Greece, Hungary, and Spain), each organization handled the process independently. Written informed consent was obtained from participants in all countries. The ethics approval process is summarized in the following ![]() .
.
Author Contributions
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
*Authors marked with an asterisk contributed equally as senior authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partly supported by the VITALISE (Virtual Health and Wellbeing Living Lab Infrastructure) project, funded by the Horizon 2020 Framework Program of the European Union for Research Innovation (grant agreement 101007990).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.