
Abstract
Effective self-management of chronic obstructive pulmonary disease (COPD) can lead to increased patient control and reduced health care costs. However, both patients and healthcare professionals encounter significant challenges. Digital health interventions, such as smart oximeters and COPD self-management applications, promise to enhance the management of COPD, yet, there is little evidence to support their use and user-experience issues are still common. Understanding the needs of healthcare professionals is central for increasing adoption and engagement with digital health interventions but little is known about their perceptions of digital health interventions in COPD. This paper explored the perceptions of healthcare professionals regarding the potential role for DHI in the management of COPD. Snowball sampling was used to recruit the participants (n = 32). Each participant underwent a semi-structured interview. Using NVivo 12 software, thematic analysis was completed. Healthcare professionals perceive digital health interventions providing several potential benefits to the management of COPD including the capture of patient status indicators during the interappointment period, providing new patient data to support the consultation process and perceived digital health interventions as a potential means to improve patient engagement. The findings offer new insights regarding potential future use-cases for digital health interventions in COPD, which can help ease user-experience issues as they align with the needs of healthcare professionals.
Introduction
Chronic obstructive pulmonary disease (COPD) significantly affects patients’ quality of life and functional status. 1 Effective self-management is important for patients to gain a sense of control over their disease, leading to reduced exacerbations and costs to the health systems.2–4 Sustained participation in self-management regimes, such as exercise programmes or compliance with medications has proven to be problematic.5–7 COPD is associated with the existence of persistent and variable symptomology, and patients often do not possess the adequate levels of disease knowledge or self-efficacy to manage their disease independently.8–10 The management of COPD also causes difficulties for healthcare professionals (HCP), who have been found to experience a sense of powerlessness and frustration in the treatment of COPD, which is escalated by factors such as poor communication and interaction with patients, problems addressing preventive care and non-adherence, lack of time and the diagnostic complexity caused by the presence of multi-comorbidities.11,12
Digital health interventions (DHI), including mobile health applications and self-monitoring devices such as Bluetooth enabled oximeters and pedometers, have the potential to enhance patient self-management and the provision of care in COPD.7,13,14 They promise to motivate patients to positively adapt their self-management behaviours through increased access to symptom information to improve their awareness and knowledge of their disease.15–17 The on-going data sharing capabilities of DHI may benefit HCP by extending the opportunity to provide timelier interventions and support to patients. 18 The possibility to gather longitudinal health status indicators, such as actigraphy and self-reported measures, could provide a holistic picture of a patient’s status, with the potential to facilitate the provision of personalised care by complementing point-in-time investigations performed at a clinical visit or hospitalisation.19–22
However, systematic reviews investigating the effectiveness of DHI in COPD, have shown there is limited evidence to suggest they create better outcomes for the management of COPD.20,23–26 The DHI assessed in these studies included: computer and mobile technology20,23; oximeters 24 ; and wearable technology such as pedometers and accelerometers. 26 Such findings have been the springboard for recent reflections on digital health in COPD where a level of frustration has been demonstrated, for example, Pinnock and McKinstry’s point of departure is to ask, ‘What is going wrong?’. 27 For many, the issue relates to adoption and user-experience issues which are often overlooked because user-involvement in the development of DHI in COPD is not commonly practiced.28–30 To ease adoption and facilitate sustained engagement with DHI, it is important to employ a person-centred design approach to help thoroughly explore and understand the needs and preferences of patients and HCP.31–36 However, as Korpershoek et al., 37 have highlighted, little is known about patient and HCP perceptions of digital health in COPD. Recent work has highlighted the existence of workflow and clinical utility barriers facing DHI in routine clinical care, but this work has not focused on HCP working in COPD.38–42 To address this gap, there is a need to understand if HCP perceive if the management of COPD can benefit from DHI in the first instance? Therefore, this study employed a qualitative study design to explore the following research question: what are HCP’s perceptions of the potential benefits for using DHI in the management of COPD? The findings can contribute new insights to clinicians regarding the opportunities for using DHI in practice, and support researchers with new information to develop clinically relevant use-cases to guide the design of digital health interventions in COPD.
Materials and methods
Study design
The study design for this research was one-to-one in-depth semi-structured interviews with healthcare professionals.
Recruitment and sample
By means of snowball sampling, 32 participants were recruited. 43 All participants were fulltime professionals providing care to COPD patients at the time of the study. The sample consisted of: Four Respiratory Physiotherapists; four Respiratory Specialist Nurses; eight General Practitioners; eight Respiratory Consultants; eight non-consultant hospital doctors (n = 5 Specialist Registrars; n = 3 Senior House Officers). Participants were recruited from two Dublin university hospitals (n = 24) while the GP cohort were recruited from various Health Service Executive (Ireland) GP clinics in the greater Dublin area. The lead author (PS) was initially introduced to Respiratory Consultants at both hospital sites by co-authors MB and JC (both of whom are Respiratory Consultants) via email. They also introduced the lead author to Respiratory Physios, Respiratory Nurses and NCHDs within their respective hospitals via email. The lead author was introduced to a GP by co-author BC via email, and one GP was known to the lead author, subsequent GPs were recruited through snowballing through each of these participants. Each participant was invited to partake in the study via email by the lead author. There was no requirement for the participants to be familiar with DHI to partake. Participants provided written consent prior to their interview. Approval for this study was granted by the Research Ethics Committees at University College Dublin, St. Vincent’s University Hospital and Tallaght University Hospital, Dublin, Ireland.
Procedure
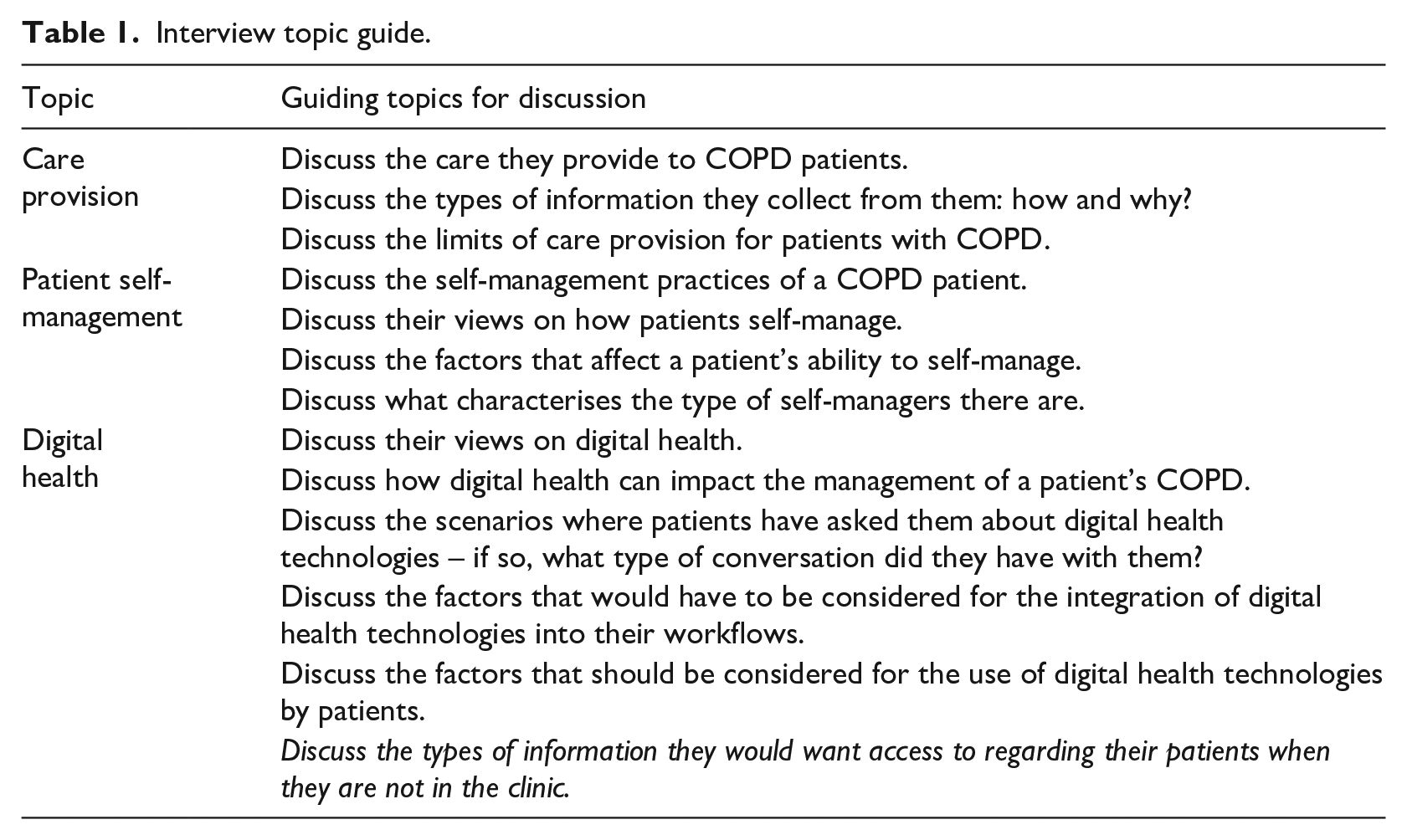
The in-depth semi-structured interviews were conducted by the first author (PS), an experienced qualitative researcher. Semi-structured interviewing was chosen as this approach employs open-ended questions to gain a deep understanding of human experience, perceptions, beliefs and/or motivations in relation to a social phenomenon. 44 A semi-structured interview topic guide (Table 1) was used to frame each interview and all interviews were conducted fact-to-face. These questions addressed participants’ perceptions regarding the potential benefit for digital health technology in the management of COPD. The use of open-ended questioning permitted the emergence of new topics to discuss and these were unpacked with the participants as they occurred.
Interview topic guide.
Data analysis
Each interview was audio recorded, transcribed verbatim and anonymised. Thematic analysis of the interview transcripts was conducted using NVivo 12 software (QSR International Pty Ltd, Victoria, Australia). The interview topic guide provided an early framework for the development of a codebook. 45 Using this early version, PS and TK then analysed a subset of transcripts to revise and finalise the codebook.46,47 Data analysis involved an inductive and cyclical approach of closely reading and rereading each transcript, identifying patterns that emerged, coding the data with labels and generating themes and sub-themes. 48 To practice analytical rigour, the data was coded independently by PS and TK, who then collaboratively examined, compared and deliberated the coding, any inconsistencies or differences were discussed until resolved. 49 Analysis was conducted after every ten interviews and data saturation was determined at 32 participants when no new patterns or themes were emerging from analysis. 50
Results
All 32 participants completed an interview. The duration of interviews ranged between 30 and 60 min with the average duration being 48 min. The following themes were identified from analysis: Interappointment Data; Role in Consultation; Patient self-management. Participant characteristics can be observed in Table 2. Please see supplementary material for further supporting data.
Participant characteristics.
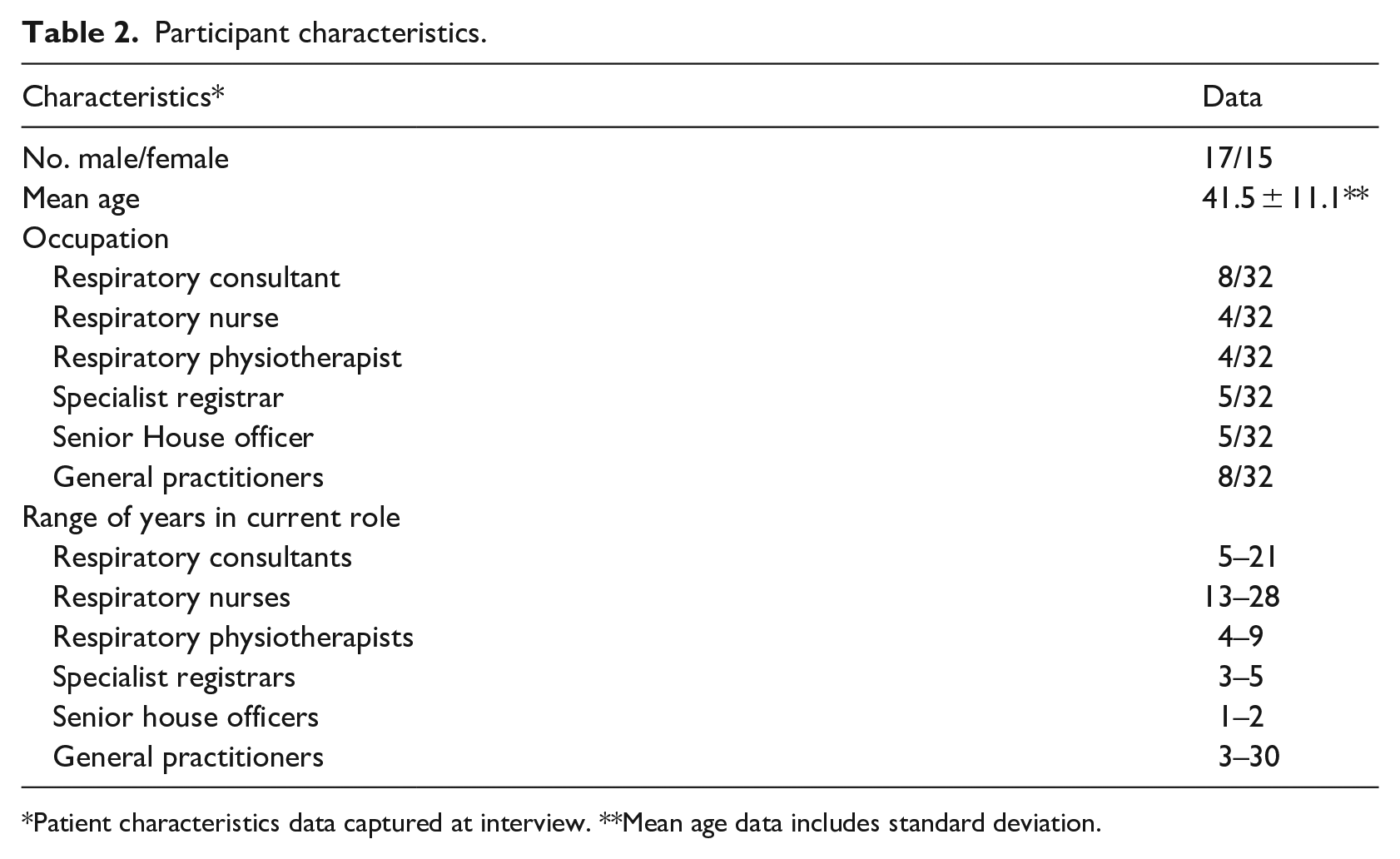
Patient characteristics data captured at interview. **Mean age data includes standard deviation.
Interappointment data
Participants discussed that having access to patient health data between appointments had the potential to facilitate timelier interventions. For example, they felt capturing health status indicators could allow them to review treatment efficacy.
If I have given a patient an inhaler, and I can now find out what’s happening at home with them, for example if they are simply inputting about activities of daily living and I see no improvement, but I know they should be more active and their exercise capacity should have increased, and if they are also inputting a dyspnea score but I see that hasn’t been affected along with their quality of life scores, that lends me the chance to intervene earlier. (Respiratory Consultant 7)
It was also highlighted by participants that interappointment data could augment existing care provision practices, such as check-ups conducted over the phone.
If we can contact the patient as we already do is some situations, with self-report information coming into us, we can advise them better. Now we have a scenario where I have improved my care and they also feel more attended to. That regular contact and advice, makes a huge difference to how patients manage because they are getting regular influence to keep up with their current management and just been told “Yes, keep it up”, that encourages them a lot, it’s hard to provide that to a patient when you don’t know if they are doing all they should be. (Respiratory Nurse 1)
Participants spoke about the potential for capturing multi-modal datasets between appointments. For instance, they felt healthcare utilisation data could inform the prioritisation of patient needs in terms of their next scheduled check-up.
Imagine having a symptom score, a measure of their lung function, be it saturation of oxygen, if they are having infections, if they are going to see their GPs regularly due to that, I’d want to know that is happening. So, if a patient is due to come back to see me in 6 months’ and then it turns out in 3 months’ that they’ve seen their GP 3 times and their symptom scores have gone up, then we definitely need them to come back in before 6 months to see if we can improve their treatment. (Respiratory Consultant 8)
Role in consultation
The potential impact of DHI to optimise the consultation process was discussed. Participants discussed the opportunity for patients to generate multiple health indicators, with the potential to offer HCP important contextual information to target for preventative intervention. They also spoke about the need for such information to support the development of personalised treatment plans.
I see them during an acute exacerbation but how they got to this point is mostly left unsolved. I see a place for self-reported aspects, like are they taking their inhalers and do think they are doing so correctly, are they using their short acting bronchodilators or are they on their nebs or their Ventolin, do they actually feel they are managing OK? If they could bring that information in, then that’d give me context for their exacerbation and we can make targeted changes with that. (General Practitioner 6)
Participants also perceived contextual data augmenting their assessment of a patient’s presentation which may reduce the time-burden associated with completing investigations.
I only get a maximum of 10-12 minutes with patients. A COPD patient needs, at minimum, 20 minutes, so we need a way to help with answering questions and issues they come in with, so our investigations don’t take up all that time. If they are coming in with self-report measures of management problems, complaints, inhaler technique, educational aspects, that usually can’t be done in 10 minutes, with this added information maybe we can prioritize the advice we need to address. (Respiratory Consultant 1)
Participants questioned the accuracy of subjective information provided by patients during consultations. They felt data generated in the home could provide a truer representation of the patient’s health status, for example, in situations where they are unwilling to share exact details for fear of hospitalisation. It was also felt longitudinal objective measures captured by DHI could help support information gathering when patient’s struggle with symptom recall.
But a lot of the time they’ll try and hold back because they just don’t want to go back to hospital again. So, there is a certain amount of your own examination that you need to use, as opposed to just what the patient is telling you. Because sometimes that’s when they go, “Yeah, I’m good, good.” But if we have other scores or measurements in front of us, we can see that they were coughing for three days in a row and they had lots of sputum, we can say, “hold on!” (General Practitioner 2) Unfortunately, it just doesn’t really work that well when a patient is trying to look back and give an accurate picture of what was happening in a certain point in time. They’re only going to remember the previous few days especially if they have just had an exacerbation, that will be more vivid and will also cloud their memory of the past few weeks. So that ability to collect information over a longer period time would mean patterns would show and that is what I want as a doctor, objective and accurate information over time. (Specialist Registrar 4)
Participants perceived DHI improving patient engagement levels in the consultation process. They felt the measurements captured by patients could act as new talking points, enabling the patient to take a more active role in the consultation as they begin to reflect on the data they are generating.
They become curious, and they start to question the variance in the numbers. Then when they come back, they often comment that they saw a difference and weren’t optimistic or were happy with it, so that means they are accepting the diagnosis and it allows for us to start from a place where they are ready for action. (Respiratory Consultant 5) The process of actually collecting information in the home gives patients something concrete as well to talk about. They can refer to the days they logged poorer levels of exercise and that they also felt increased breathlessness during that time too. So, it gives them a talking point, a prompter for discussing how they were which I see giving them more confidence in speaking about their disease. (Respiratory Nurse 3) I see it as being an enabling agent for the patient, for them to be more engaging and for them to feel they are more involved, because they are going to feel like they collected this, now I want answers and views, so that’s a win, win. (Respiratory Nurse 2)
Patient self-management
The participants perceived DHI can have a positive impact on patient self-management. They felt digital health practices, such as symptom tracking, can support patients to adhere to treatment plans. For instance, it was felt symptom data can become a motivational adherence tool as they offer patients the opportunity to see reassuring progress trends. Furthermore, participants felt capturing activity from a pedometer could increase patient self-efficacy through the encouragement they receive from seeing their progression.
The big difficulty with COPD patients is non-compliance and some will fall into the temptation of smoking again because they are not seeing improvement and get demotivated. But if they can see that their symptoms are changing for the better and are consistent, then they are more likely to keep with the plan and stay away from smoking. (Respiratory Consultant 3) Getting them to wear an activity band would do wonders to get them to continue their exercise programme or to try and walk. They are really poor adherers to exercise, they don’t think they can do it. If they can see the numbers, the amount of steps they can do, that would spur them on and give them confidence to keep at it, because self-confidence is so low in most patients and they are usually not great at keeping to their plans. (Respiratory Physiotherapist 2)
The potential for DHI to impact patient symptom management was also discussed by participants. They perceived DHI as a potential method to help patients develop their understanding of their symptom characteristics such as their individual baseline. Consequently, participants felt as patients’ understanding of their disease increases, this can empower patients to appropriately question changes in symptoms when they occur.
They could understand what symptoms they have when they are well, like to understand their personal baseline. For example, they only get shortness of breath during exertion and all of a sudden, they are short of breath sitting on a chair. They need support to think in that situation, “Do I think that’s a sign that things are better or worse?”, so they can recognise what they are looking out for, and to get them thinking critically about their symptoms. (Respiratory Nurse 4) It’s about reacting to how they perceive their symptoms, and if they feel worse than their usual variability they will present to us, but this often has no foundation other than perception and that can be skewed by panic and lack of understanding. Imagine the difference if a patient had to log information about their saturations or activity, they would start to see they are doing fine and get used to how it feels with their normal symptoms, I feel that would save them a lot of worry and trips to ED. (Respiratory Consultant 4)
Discussion
This is the first study to comprehensively explore the perceptions of HCP regarding the potential for DHI in COPD. Participants felt the capability of DHI to transmit multi-modal patient data from the home could facilitate timelier interventions. Our findings suggest there is the potential for inhaler efficacy to be identified in a more efficient manner if expected improvements in patient outcomes are not evident in self-reported data such as dyspnoea or activity levels. Patient-related factors affecting inhaler adherence include regular use, good technique and follow-up supervision, the latter corresponds with findings in this study as participants felt DHI could support the timely sharing of adherence indicators with HCP ensuring that optimal implementation of inhalers is performed.5,51,52 The results suggest participants perceive interappointment data having the potential to augment routine check-ups conducted over the phone. This may be particularly useful for a virtual clinic format in the hospital setting or for HCP providing care to COPD patients in the community, where caseloads are usually very high yet under-resourced, meaning the needs of every patient are difficult to address especially for those working with patients located in rural areas.53–57 This is the first study however to highlight the potential for DHI in COPD to address such issues.
Participants discussed the opportunity for DHI to capture multi-modal patient data such as objective measures, including oximetry and subjective, self-reported measures, including health care utilisation data, as having the potential to help HCP identify if a patient is coping sub-optimally. This information was perceived as a possible support to HCP to help prioritise those patients in need of support through the scheduling of an earlier appointment than that originally planned. This sentiment departs from previous work in COPD digital health studies which aim on the early detection of exacerbations.58,59 However, the evidence is poor for the detection of exacerbations, and there is still much debate regarding the value of predicting or detecting an exacerbation when reliable markers of an imminent exacerbation are still contested.27,60,61 Our findings are novel as they suggest future COPD digital health interventions may focus on identifying multiple data sources to determine if patients are managing optimally. These findings also offer new perspectives for future digital health studies in COPD aiming to harness DHI to reduce admissions.
There was a sentiment expressed by participants if patients are generating health-related data in the home, this could offer HCP contextual information to support the delivery of personalised care. Contextual information here, refers to modifiable risk factors contributing to ill health, these may include medication use, inhaler technique, exercise, sleep, or a patient’s sense of self-efficacy with managing their disease. Generally, HCP do not have access to information about a patient’s health status while they are in the home and are constrained to a very particular perspective of the nature and progression of their disease, afforded to them by the investigations conducted in the clinic or hospital. In COPD, these investigations frequently involve gathering important objective measurements, such as investigating lung function through spirometry which determines progression and disease classification. But clinic-based investigations are also limited, in that they capture data at a point in time, whether during a review appointment, an emergency admission, or a routine check-up, which in a sense offer a snapshot of the patient’s health status. Consequently, a significant knowledge gap exists regarding how patients live with and manage their disease daily, as well as what their natural symptomology and fluctuations look like in the community. 21 This situation further adds to the difficulties for HCP when determining the contributing factors that lead to an exacerbation of COPD,62,63 and our findings are the first to explore how HCP perceive DHI impacting this clinical need in COPD.
Participants felt if patients are presenting to a consultation with self-reported contextual data, HCP may be afforded the opportunity to establish the reason why a patient has exacerbated, in a more informed manner. Furthermore, they felt this data could be leveraged to offer personalised treatment, as HCP may have the opportunity to educate the patient in relation to the specific factor that caused their decline. The findings resonate with previous research which found COPD patients showing preference for personalised treatment, while it has also been highlighted that HCP recognise one of the primary barriers facing effective self-management is providing patient-centred treatment plans.64,65
Participants felt contextual data could reduce the duration of history-taking, and the need for time-intensive investigations, allowing them to optimise consultation time to address the patient’s specific needs. Time is an important factor in the development and maintenance of a patient-clinician relationship. 66 Research has shown patients place an emphasis on a feeling of being listened to in a consultation and were found to be dissatisfied with experiences where they felt hurried, elsewhere research has shown that treatment concordance is negatively affected if time is insufficiently granted to the patient.67–70 The role of DHI in COPD consultations has not been research before, and our findings suggest the opportunity for DHI to allow HCP to focus more time on the patient’s needs is promising, as a satisfactory patient-clinician relationship is linked to increased disease knowledge, improved self-management skills and better outcomes.71,72
The findings suggest the accuracy of subjective information gathered in consultations can be influenced by factors that bias how patients recall their symptoms, such as an unwillingness to share exact details for fear of hospitalisation or issues caused by efforts to recollect a history of symptoms over a long period. These findings correspond to previous research suggesting symptom recall problems are common in patient populations, while research has also shown COPD patients using long-term oxygen were shown to have poorer levels of verbal memory when compared to healthy adults of the same age.73,74 It was felt however longitudinal self-reported data could be used in conjunction with the patient’s verbal information to provide a more precise description of their symptoms. These findings highlight an important unmet need for HCP and patients, particularly, as the accurate recall of symptoms is a key factor for HCP when establishing the selection of treatment. 73 However, although barriers do exist with patient recall, it is an understudied area in digital health research with few studies demonstrating how clinicians can properly utilise the data generated by DHI when faced with common digital health barriers like data-overload. 38
Interestingly, participants highlighted the enabling quality of the data patients can generate using DHI. They felt as patients begin to reflect on the meaning behind their data, their measurements can become a talking point in consultations which may cultivate a sense of engagement to partake in conversations about their disease. Our findings are supported by previous research which demonstrating how patient generated health data from DHI can improve patient-clinician communication.75,76 This is a key consideration regarding the potential role of DHI in COPD, as the effective management of COPD requires successful patient-clinician communication to be achieved.77,78 Research has shown however, patients and HCP are often dissatisfied with communication concerning COPD treatment.79,80 For patients, it has been found this dissatisfaction stems from a lack of information regarding the nature and course of their disease, while HCP have been found to encounter barriers when trying to elicit symptom information from patients.79,81 It has been suggested facilitating the active involvement of the patient in the consultation through patient-centred approaches is central to improving patient-clinician communication. 82 Although information seeking behaviours vary, patient-initiated questioning is a simple form of information gathering that is practiced. 83 Healthcare professionals are encouraged to facilitate this type of information exchange as it helps the patient shape and manage their involvement in the conversation.83,84 Until now, the opportunities for DHI to enhance the patient-clinician communication in COPD consultations has received little attention. The findings of this study suggest patient data generated by DHI can potentially empower patients to initiate discussions regarding their measurements, providing a potential avenue to help address communication barriers affecting consultations in COPD.
Self-management in COPD has shown to be inconsistent, with non-adherence to treatment plans often contributing to unsatisfactory patient outcomes.3,6 The findings in this study suggest the capture of symptom data can potentially provide reassuring health status indicators of improvement for patients. As a result, the participants felt these data could reassure patients of treatment efficacy, motivating them to continue to adhere to their self-management plan. Similarly, self-tracking with a pedometer was proposed as a possible intervention to increase patient’s self-efficacy to perform exercise regimes. These findings could have future implications for how COPD patients self-manage, particularly, as previous research has shown poor levels of engagement and self-efficacy can demotivate patients from developing or adhering to basic self-management practices.9,85 Participants also felt DHI could increase individual’s symptom awareness and provide self-management encouragement to COPD patients through the real-time access to health status information, both of which are linked to better outcomes for patients self-managing.18,64,86–88
Participants also felt DHI has the potential to support patients with symptom management. Disease knowledge is an important aspect for the effective self-management of COPD and is particularly useful for how patients recognise and react to their symptoms. 89 However, studies have shown COPD patients often have inadequate levels of health literacy which can affect their control over their disease.90,91 Furthermore, this cohort are more likely to have worse symptom management and increased hospitalisation due to a higher prevalency of exacerbations.10,92 The results suggest HCP perceive symptom tracking with DHI can potentially enhance patient’s symptom knowledge, by empowering them with the information to support the identification of abnormal deviations and to manage these situations appropriately. Studies have shown COPD patients demonstrate consistently poor reporting of exacerbations, with 50% of patients failing to seek GP treatment before hospitalisation.93–95 The potential for DHI to increase the disease knowledge of COPD patients is a promising area for future research, as it presents an opportunity to improve patient safety and reduce healthcare utilisation.
Limitations
There are several factors that are important to consider when reviewing these findings. Although the sample is multidisciplinary, its relatively small size may impact the degree to which the findings are reflective of those working in the wider respiratory community. Participants were recruited from two hospitals and a number of GP clinics in the greater Dublin area, which may also affect the generalisability of the findings as healthcare systems and the delivery of care to COPD patients differs internationally. Healthcare professionals who were already interested in DHI may have been more likely to volunteer to take part in such a study, and similarly with the use of snowball sampling, more likely to recommend the study to colleagues who are also interested in DHI. Additionally, the purpose of this research was to assess the potential benefits for digital health technology in the management of COPD, future work is needed to explore the barriers and facilitators HCP perceive regarding the use of DHI, this research can inform the development of implementation and adoption strategies for the use of DHI in the clinical context. Moreover, this paper does not account for the perceptions of COPD patients, however, the authors have previously published research addressing this.30,96
Implications for clinical practice and conclusion
Our findings provide new insights to the literature regarding the potential role of DHI in the management of COPD. HCP perceive DHI as a gateway to generating new information about their patient’s health status in the home, where traditionally a knowledge gap exists. In practice, they felt capturing these data could afford them the opportunity to determine treatment efficacy and to make informed and personalised treatment decisions when the patient is not in the clinic. They also envisioned DHI as potentially enhancing the time and effectiveness of the consultation, as patients become more open to dialogue due an interest in their data. Finally, participants highlighted the opportunity for DHI to increase patient self-efficacy as they felt data captured by patients could improve symptom management and disease knowledge.
From a research perspective, these findings can be used to inform the development of DHI aiming to address clinically meaningful issues, as they highlight HCP have several unmet needs when managing COPD patients. As such, the findings can be leveraged to generate clinically relevant use-cases which have yet to receive adequate attention from digital health research in COPD. The findings will also help to mitigate digital health adoption and implementation barriers experienced by HCP as future research begin to align their aims with the needs of healthcare professionals working in COPD care.
Supplemental Material
sj-docx-1-jhi-10.1177_1460458221994888 – Supplemental material for A qualitative study of clinician perceptions regarding the potential role for digital health interventions for the management of COPD
Supplemental material, sj-docx-1-jhi-10.1177_1460458221994888 for A qualitative study of clinician perceptions regarding the potential role for digital health interventions for the management of COPD by Patrick Slevin, Threase Kessie, John Cullen, Marcus W. Butler, Seamas C. Donnelly and Brian Caulfield in Health Informatics Journal
Footnotes
Acknowledgements
The authors would like to thank the healthcare professionals who participated in the study for their time and openness.
Contributorship
PS and BC conceived the study. PS and BC were involved in protocol development while MB, SD and JC were involved in gaining ethical approval and patient recruitment. Data analysis was completed by PS and TK. PS compiled the first draft of the manuscript. All the authors reviewed and edited the manuscript and approved the submission version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was funded by Science Foundation Ireland (grant SFI/12/RC/2289).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.