
Abstract
Keywords
Introduction
Inflammatory Bowel Disease (IBD), which includes Crohn’s disease and Ulcerative Colitis, are immune-mediated conditions characterised by chronic inflammation of the gastrointestinal tract. These conditions typically present with symptoms such as diarrhea, rectal bleeding, abdominal pain, fatigue, and weight loss. IBD can have a profound lifelong impact on a patient’s physical, psychological, and social well-being.1–3 Clinicians must therefore foster an open and responsive relationship with the patient, providing comprehensive clinical care management that addresses the patient’s concerns and needs promptly and efficiently.
Digital Patient-Reported Outcomes (PRO) utilize electronically administered questionnaires to gather health information from patients, enabling them to gain insights into their symptoms and concerns regarding quality of life. Patient-Reported Outcome Measures (PROMs) capture a patient’s perception of health and well-being,4,5 offering valuable insights that assist clinicians in optimizing disease screening, monitoring, and management.6–9 Integration of digital PROs into the clinical care model of IBD patients has the potential to reduce the necessity for periodic face-to-face consultations. Moreover, it provides an interactive platform for patients to promptly communicate concerns about their disease-related emotional and social well-being to the treating clinical team.
A few studies have highlighted the potential benefits of integrating digital PROs into the care of patients with IBD. In 2009, Shafran et al. emphasized the importance of real-time symptom reporting in a web-based study focused on IBD patients, demonstrating its potential to improve understanding of the timing and reasons behind symptom flare-ups. 10 Van Dee et al. conducted a study in 2014, concluded that e-health PRO solution held significant potential for self-monitoring, enabling early detection of disease activity. 11 In 2015, a mixed method study conducted by Khan et al. explored the effectiveness of a PRO application in enhancing the quality of life for IBD patients by addressing their informational needs. The application effectively collected information on symptoms and the social impacts of the disease, which were not routinely shared with treating physicians during regular consultations. 12
Denmark has one of the most advanced digital healthcare systems in the world with a well-established PROM service. Since 2017, the Danish government has implemented the standardized use of PROs across all healthcare sectors. 13 In contrast, digital PROs utilisation in the Australian Health System is limited to only a few metropolitan centres with poor standardization across the country. 14 To successfully promote digital PROs in Australia, it is essential to identify and address potential barriers to implementation. A key factor is patients’ readiness to engage with the technology, as the success of adopting and adhering to new digital health solutions often depends on it. In 2022, Nielsen et al. conducted a study at Regional Hospital Silkeborg, Denmark, a tertiary referral centre with a dedicated IBD outpatient service, comparing the characteristics and readiness of IBD patients who engaged with a digital PRO system to those who did not. 15 This comparison was facilitated by the application of the “Readiness and Enablement Index for Health Technology” (ReadHy) tool, an externally validated tools to assess the health technology readiness of individuals. 16
Western Health is a tertiary health service in Melbourne, Australia, with an IBD outpatient service caring for over 800 patients annually. Currently, digital PROs are not utilized within the service, though their implementation could significantly enhance patient care. Our aim was to assess the readiness of our IBD cohort for digital PRO adoption and to identify potential barriers to implementation. To achieve this, we compared our cohort with the Danish IBD cohort from Nielsen et al. using the ReadHy tool to evaluate similarities and differences between the two groups.
Material and methods
Setting
This study was a descriptive, questionnaire-based, cross-sectional study conducted at the Western Health IBD outpatient clinic. The study spanned 7 weeks, from November 9, 2022, to December 21, 2022. During the study period, all eligible patients attending IBD clinic appointments were invited to participate in the survey by a research assistant. After obtaining verbal consent, willing participants were provided with a printed ReadHy questionnaire along with a plain language statement explaining the study’s rationale and that participation was voluntary. Since all questionnaires were anonymous, written consent was not required. Completed questionnaires were collected and securely stored in a locked research office for data analysis.
Study population
All patients attended the IBD clinic during the 7 weeks of data collection. We included adult patients aged 18 years and above, who were proficient in speaking and reading English. We excluded patients with cognitive impairment. Due to uncertainty regarding the standard deviation of the sample, a precise sample size was not calculated. However, Nielsen et al. drew meaningful comparisons between PRO users and 58 non-PRO users; therefore, we aimed to recruit a similar sample size for our study. We planned to recruit 70 participants (10 participants per clinic session), accounting for a 20% incomplete questionnaire rate, with an expected final sample of 56 participants.
Measures
Our data collection followed the methodology outlined by Nielsen et al. to facilitate comparison with the Danish cohort. All questionnaires were administered anonymously. Participants self-reported demographic information including age, gender, educational status, and the duration of IBD since diagnosis. We also collected data on participants’ general and healthcare-specific use of information technology.
Readiness and enablement index for Health technology (ReadHy) profiles of Footscray cohort and non-PRO users.
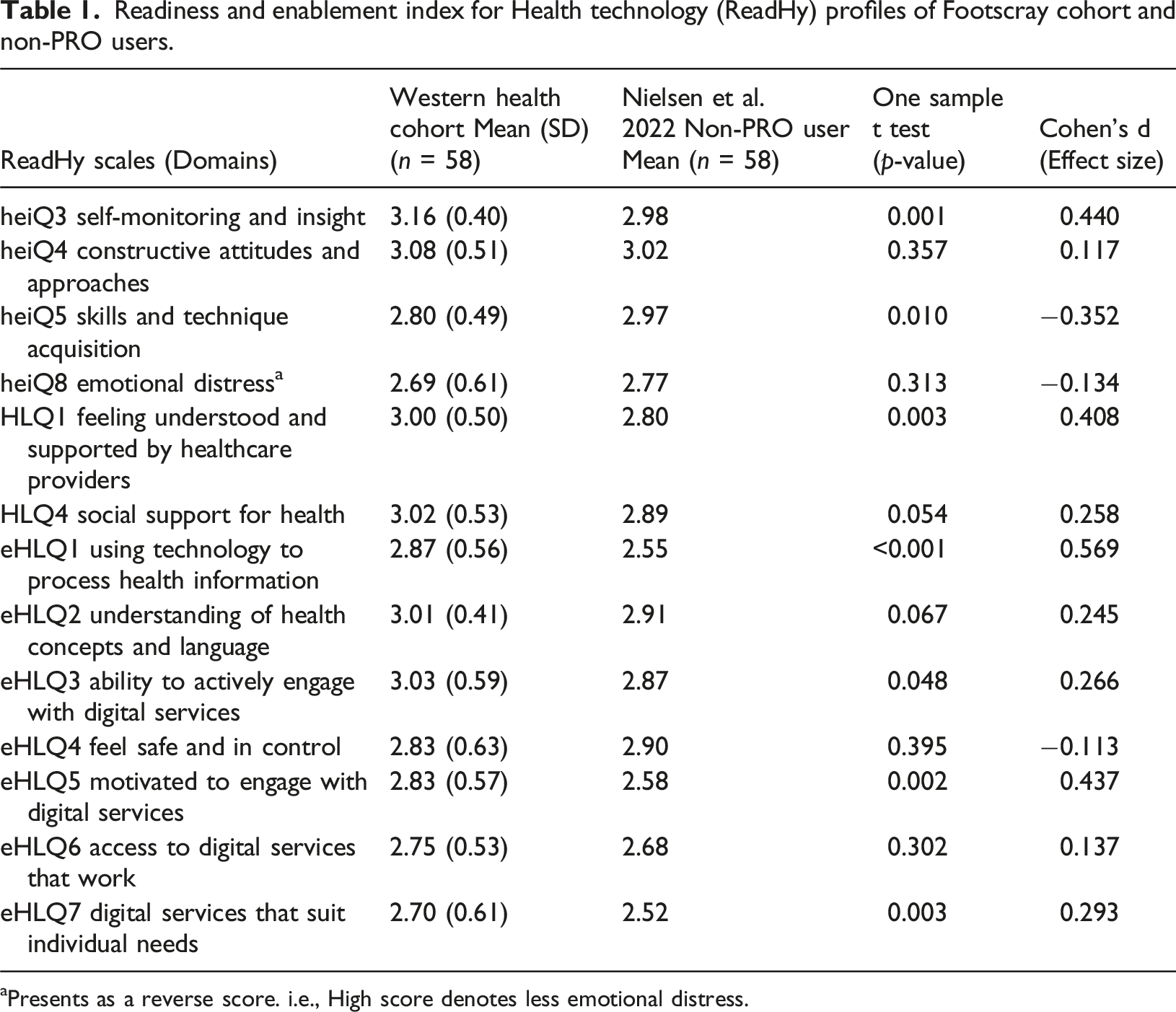
aPresents as a reverse score. i.e., High score denotes less emotional distress.
Readiness and enablement index for Health technology (ReadHy) profiles of Footscray cohort and PRO users.
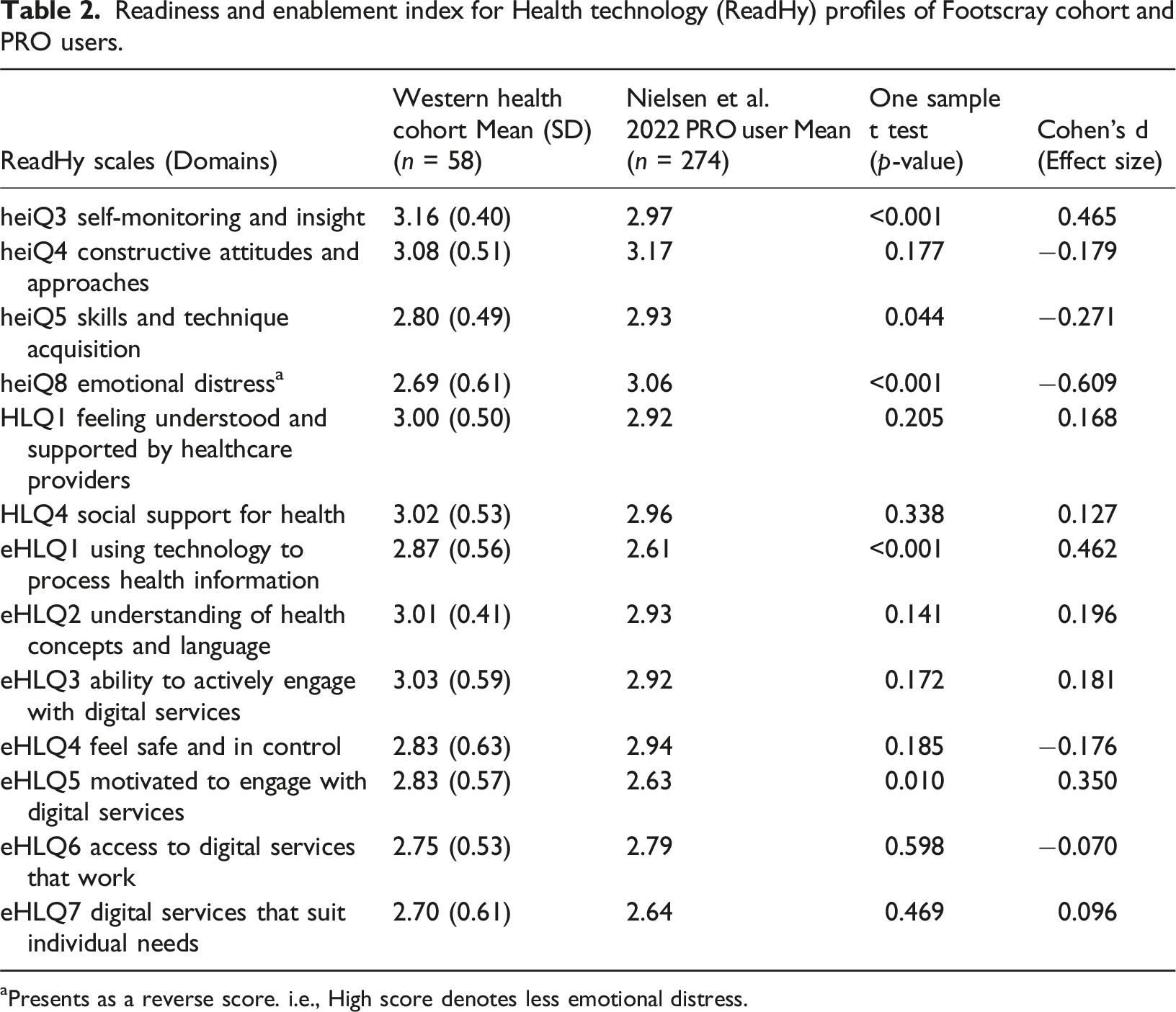
aPresents as a reverse score. i.e., High score denotes less emotional distress.
Statistical methods
For each participant, an average dimension score was calculated if over 50% of the items were answered. The mean scores and standard deviations for each dimension of the ReadHy in the Western Health cohort were calculated using Microsoft Excel Version 16.78.3 functions. Subsequently, mean scores were compared with those of PROs users and non-PRO users in the Danish study. As the average dimension scores represent continuous variables, one-sample t-test was conducted using statistical software Jamovi 2.3.21.0. Statistical significance was defined as p < 0.05. The effect size of the observed differences was assessed through Cohen’s d, where an effect size greater than 0.5 was considered large, 0.2 to 0.5 was deemed medium, and less than 0.2 was classified as small. 21 This statistical analysis aimed to identify differences in readiness for engaging with digital health technologies between the Western Health cohort and the Danish cohort.
K-means clustering, employing the Hartigan-Wong algorithm, was conducted using Jamovi 2.3.21.0. The primary objective was to categorize individuals into distinct sub-groups based on their ReadHy scores, allowing us to analyse the characteristics associated with high ReadHy scores. Given our sample size, the number of clusters was limited to 2. Cluster 1 included individuals with lower ReadHy scores, while Cluster 2 comprised those with higher scores. The K-means algorithm was executed multiple times to identify the solution with the lowest total within-cluster sum of squares.
Ethical approval
This study was approved by the local ethics committee (reference number stated on title page).
Results
Characteristics of the included and excluded participants.

When comparing the baseline characteristics of the Western Health cohort with the Danish cohort, notable differences were observed. The Western Health cohort had a lower mean age of 42.3 years compared to both Danish PRO users (52.5 years) with a mean difference of −9.9 (95% CI: −13.8 to −6.0, p < 0.001), and Danish non-PRO users (60.5 years) with a mean difference of −17.9 (95% CI: −21.8 to −14.0, p < 0.001). Additionally, the Western Health cohort showed a higher level of adaptation to electronic devices, with 93% reporting daily usage of information technology, surpassing the rates observed in Danish PRO users (75%) and Danish non-PRO users (53%). Moreover, Western Health cohort displayed a higher prevalence of using information technology for health-related issues (83%), contrasting with the percentages of 60% in both Danish PRO and Danish non-PRO users.
Comparing the ReadHy profile of the Western Health cohort with the non-PRO users in the Danish cohort
Significant differences were observed across various dimensions of the ReadHy, favouring the Western Health cohort in comparison to the Danish non-PRO users. Noteworthy differences included “heiQ3 Self-monitoring and insight,” where the Western Health cohort scored a mean of 3.16, as opposed to 2.98 for the Danish cohort (p = 0.001, Cohen’s d = 0.44). Similarly, in “HLQ1 Feeling understood and supported by healthcare providers”, the mean score for the Western Health cohort was 3.00 compared to 2.80 for the Danish cohort (p = 0.003, Cohen’s d = 0.408). In the dimension of “eHLQ1 Using technology to process health information”, the Western Health cohort scored a mean of 2.87, while the Danish cohort scored 2.55 (p < 0.001, Cohen’s d = 0.569). Additionally, “eHLQ5 Motivated to engage with digital service” showed a mean score of 2.83 for the Western Health cohort versus 2.58 for the Danish cohort (p = 0.002, Cohen’s d = 0.437). Lastly, in “eHLQ7 Digital services that suit individual needs”, Western Health cohort had a mean score of 2.70 compared to 2.52 for the Danish cohort (p = 0.003, Cohen’s d = 0.293). Detailed profiles of the ReadHy for both the Western Health cohort and the Danish non-PRO users are presented in Figure 1 and Table 1. Readiness and enablement index for Health technology (ReadHy) profiles of Western Health cohort and the Nielsen et al. cohort.
Comparing the ReadHy profile of the Western Health cohort with the PRO users in the Danish cohort
Compared to the Danish PRO users, the Western Health cohort exhibited higher scores in two key dimensions. Specifically, in “heiQ3 Self-monitoring and insight”, the Western Health cohort achieved a mean score of 3.16, surpassing the PRO users who scored 2.97 (p < 0.001, Cohen’s d = 0.465). Additionally, in “eHLQ1 Using technology to process health information”, the Western Health cohort scored 2.87, while the PRO users scored 2.61 (p < 0.001, Cohen’s d = 0.462).
A notable difference however emerged in the dimension of “heiQ8 Emotional distress”, which served as a significant distinction between PRO and non-PRO users in the Danish study, where PRO users in the Danish study scored higher than non-PRO users. The Western Health cohort more closely resembled the non-PRO users, showing no statistically significant difference from them (2.69 vs 2.77, p = 0.313) but scoring lower than the Danish PRO users (2.69 vs 3.06, p < 0.001, Cohen’s d = −0.609). The lower score of the Western Health cohort in heiQ8 contrasts with their otherwise high readiness for the implementation of digital PROs, as suggested by the other domains. Details of the ReadHy profiles for both the Western Health cohort and PRO users are outlined in Figure 1 and Table 2.
K-mean clustering
Clustering profiles based on ReadHy (Readiness and enablement index for Health technology).

Characteristics of profiles shown in Table 4.

Discussion
Digital PRO has demonstrated benefits in managing IBD. However, this tool remains underutilized by most health services in Australia, including Western Health. A crucial factor for the successful implementation of digital PRO is patients’ readiness to engage with the technology. This study is the first in Australia to assess digital PRO readiness in IBD patients. We compared our IBD cohort with a Danish cohort, where standardized PROM services are integrated across all healthcare sectors. Our goal was to evaluate the similarities and differences between the two groups and identify potential barriers to implementing this technology in Australian IBD care.
The Danish study revealed that the PRO user group tended to score higher on most dimensions in ReadHy, indicating a positive correlation between higher scores and readiness for digital PRO implementation. 15 In our study, the Western Health cohort outperformed both PRO users and non-PRO users in two dimensions. These differences were notable in “Self-monitoring and insight,” and “Using technology to process health information,” with Cohen’s d values indicating medium to large effect sizes. A high score in “self-monitoring and insight” suggests that the Western Health IBD cohort possesses a keen awareness of their disease and the ability to self-monitor their disease state, crucial for successful adherence to and the implementation of digital PRO. Furthermore, a high score in “using technology to process health information” highlights the proficiency of our cohort in information technology.
The k-means clustering results reinforced this perspective, highlighting those characteristics that correlate with higher ReadHy scores including younger age, higher education level, and more frequent use of information technologies in daily life or for health-related matters. Since Western Health IBD cohort are young patients with high information technology usage, we anticipate that they are likely to embrace the use of digital PRO in clinical care.
Nielsen et al. identified the level of emotional distress as a distinction between the Danish PRO and non-PRO users. The authors hypothesized that individuals with poor mental health were less inclined to engage with new interventions, with clinicians also being more cautious about inviting such patients to participate in trials for new interventions. Our findings indicated that the Western Health IBD cohort exhibited a similar level of emotional distress as the non-PRO users but a higher level of emotional distress compared to the PRO users. If the Danish study’s explanation holds, this suggests that the Western Health cohort might be less prepared for the implementation of digital PROs. However, since causation cannot be established, it is equally plausible that the successful integration of digital PRO in Danish Health Service achieved positive influence of patients’ mental health, resulting in lower emotional distress among PRO users compared to non-PRO users. This theory is supported by evidence that suggested self-management tools in IBD could improve psychological well-being.8,9 Another possible explanation for the elevated emotional distress in the Western Health cohort could be the impact of the COVID-19 pandemic. While the Danish study was conducted in 2018, our study took place in 2022, shortly after the pandemic began. Research has shown that the COVID-19 pandemic can have enduring effects on mental health, including post-traumatic stress symptoms arising from quarantine and social distancing, as well as the repercussions of post-pandemic economic recession. 22 D'Amico et al. proposed that individuals with IBD may be more susceptible to mental distress during the pandemic due to concerns about the immunosuppressive nature of their treatments, which could increase their perceived risk of contracting COVID-19 or experiencing a poorer outcome if infected. 23
Although our study did not conclusively determine the underlying cause of the high emotional distress domain, our result offers valuable insights into potential barriers of digital PRO implementation in the Western Health IBD patients. Integrating psychological care to assess and support emotional well-being will be essential for the successful adoption of digital PROs in this cohort. As the first Australian study to examine digital PRO readiness in the IBD population, we have established a research framework for other centres to assess patient readiness and barriers to adoption. Future research in settings where digital PROs are already in use may help clarify potential causal relationships between emotional distress and digital PRO readiness, ultimately facilitating the broader integration of digital health technologies into clinical care across Australia.
Strengths
Our study has several strengths. Firstly, we utilise the ReadHy tool, which has undergone validation to assess users’ health technology readiness level and degree of enablement. 16 Notably, we excluded the Service User Technology Acceptability Questionnaire (SUTAQ), which is part of the assessment utilised in Nielson et al. to investigate acceptability among users of PROs, as the evidence supporting SUTAQ is less definitive. SUTAQ has not undergone psychometric evaluation, and the correlation with the results from ReadHy is reported to be poor. 15 In our study, we exclusively employed ReadHy, strengthening our focus into the readiness of the Western Health cohort for the implementation of digital PRO.
Secondly, this study aligns with the established methodology of the Danish study, 15 which strengthens our exploration of the mechanisms and concepts behind patients’ readiness for digital PRO. By conducting a comparative analysis of the ReadHy results between the two studies, the Danish study serves as a valuable benchmark, offering a reference point for our exploration. Additionally, our use of the k-means clustering method employed in the Danish study further enhances the credibility of our findings. The consistency between our results and those of the Danish study provides further evidence supporting the characteristics identified as strong correlations with patient readiness for digital PRO in our study.
Limitations
Our study has several limitations. Firstly, our sample size was relatively small, with 58 participants, which constrains the statistical power of our findings.
Secondly, this is a single-centre study, which limits the generalizability of our findings.
Thirdly, there was a 19% exclusion rate of participants due to incomplete questionnaires. Notably, there existed a considerable disparity between the included and excluded cohorts in terms of the rate of infrequent use of information technology (7% vs 23%, respectively). This variance introduces a potential source of sampling bias, as less tech-savvy participants were excluded. However, it is crucial to recognize that no single health tool can cater to the entire population. Despite the potential bias stemming from excluding less proficient participants, our findings suggest that the majority of IBD patients in our cohort exhibit characteristics conducive to the adoption of digital PRO, thus providing a strong justification for integration into IBD clinical care models.
Fourthly, the absence of an equivalent PRO user group for comparison hindered our ability to establish a causal relationship between emotional distress levels and PRO implementation. This arises from the challenges of introducing a new program in a resource-conscious Australian public health service without evidence of its feasibility.
Finally, comparisons between the Australian and Danish cohorts may have been influenced by unquantifiable factors such as cultural differences. The lack of equivalent Australian benchmarking data prevented a within-country comparison. In this context, the study by Nielsen et al., conducted in Denmark where a mature, nationwide PRO service is established, provided the most appropriate available surrogate for benchmarking.
Conclusion
The benefits of digital PROs in managing IBD are well-documented, yet they remain underutilized in Australia. Our study is the first in Australia to employ the ReadHy tool to assess the readiness of an Australian IBD cohort to adopt digital PROs, comparing findings with a Danish IBD cohort who are managed through an IBD care model with mature integration of digital PROs. Our study has identified favourable characteristics of the Australian cohort namely younger patients with greater exposure to information technology, promising strong potential for acceptance of digital PRO. However, emotional distress in Australian IBD cohort has been flagged as a potential barrier to implementation, although this may have been confounded by Covid-19 pandemic. Elaboration of our study framework in future studies will provide valuable information regarding the feasibility of integration of digital PROs into the Australian IBD care landscape.
Supplemental Material
Supplemental Material - An assessment of patient readiness to engage in digital patient reported outcomes in an Australian inflammatory bowel disease cohort
Supplemental Material for An assessment of patient readiness to engage in digital patient reported outcomes in an Australian inflammatory bowel disease cohort by Tsz Hong Yiu, Sarah Rouse, Caitlin Hausler, Kerrie Curin, Nicola McGuinn, Joanna Petrunic, Amalie Søgaard Nielsen, Bodil Rasmussen, Christopher F. D. Li Wai Suen, and Elizabeth Chow in Health Informatics Journal
Footnotes
Acknowledgements
I would like to express my gratitude to the Western Health Gastroenterology department for providing me with the opportunity to conduct this research project and for all the resources and support they provided. I would also like to extend my appreciations to Sara Vogrin for her invaluable guidance on our statistical analysis.
Ethical considerations
The Low-Risk Ethics Panel of the Ethics and Governance Office at Western Health granted approval (approval code: QA/64889/WH-2020-240188(v3)) for our interviews on 9th November, 2020. Since no identification was necessary, no signature was required. Respondents provided verbal consent upon recruitment, and the plain language statement clarified that by completing the questionnaire, they consented to the use of their data in scientific research. Our research adhered to the ethical guidelines outlined in the National Statement on Ethical Conduct in Human Research, ensuring ethical standards were maintained for participants, the research team, and Western Health. The collection and storage of our data followed the Western Health Intellectual Property Rights guidelines.
Author contributions
ASN, EC, SR, BR and TY conceived the study. CH, KC, NM, and JP were responsible for data collection. TY conducted the data analysis. TY, EC, CL and SR contributed to drafting and revising the manuscript. All authors have reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author EC, upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.