
Abstract
This study describes the development and design of the Joint Transition Clinic, a collaborative solution designed to support adolescents with epilepsy (AWE) in their transition from pediatric to adult healthcare. Using a participatory design (PD) approach, the study involved AWEs, parents, nurses, and physicians in an iterative development and co-design process. Through a series of workshops, users suggested three ideas: “The Bridge,” “The Knowledge Giraffe,” and “No rules app.” After considering all three ideas, the research team and participants agreed to proceed with the development of “The Bridge,” integrating elements from “The Knowledge Giraffe.” This process led to the creation of the Joint Transition Clinic, encompassing many of the AWEs’ needs and wishes. The PD approach proved effective in creating an organizational-based intervention that addresses patient needs and supports self-management while ensuring AWEs and their parents had a voice in its development, leading to a solution ready for pilot testing.
Background
The transition of adolescents with epilepsy from pediatric to adult healthcare is more than a relocation; it is a complex transition due to co-occurring neurological, neurodevelopmental, and psychiatric comorbidities experienced by AWEs. 1 Furthermore, it encompasses challenges such as vulnerability in physical and mental health, social relations, and educational achievement2–5 as epilepsy also impacts mental well-being, social inclusion, quality of life, and care beyond physical symptoms.5–9 As is the case for adolescents with other chronic illnesses, research highlights the crucial role of close collaboration between adolescents and healthcare professionals (HCPs) from various disciplines in facilitating a successful transition from pediatric to adult healthcare.10–13 Chu et al. (2015) 14 describe that supporting adolescents’ arrival in adult care was as important as preparing them for the transfer. Others have emphasized the importance of acknowledging the need to properly prepare for the transition and the adolescent’s needs upon arrival in the new care culture. 15 A seamless transition from pediatric to adult healthcare is essential for the long-term health and well-being of AWEs. However, evidence shows that this transition tends to perform poorly due to inadequate preparation, poor service coordination, a lack of resources, and insufficient education and training.16,17 If the arrival is neglected, HCPs share concerns that the adolescents might feel displaced among the elderly patients in the new environment, 18 or they might disregard checkups with fatal consequences for their health. 19 AWEs lack adequate coping strategies to address specific transitional problems during the development of autonomy and independence. 20 From a transition theory perspective, greater self-identity and growing independence characterize the transition.21,22 This experience is interwoven with developmental, health-illness, organizational, and situational transition issues, emphasizing that transitioning from pediatric to adult healthcare coincides with other significant life-course transitions and needs. Meeting these needs requires changes in clinical practice; however, involving the practice’s stakeholders is essential to finding new ways to meet their needs. 23
A recent study revealed that AWEs seek independence, acceptance, and understanding in managing their epilepsy and transitioning to adult care. 24 However, research indicates that most HCPs primarily focus on epilepsy diagnoses, treatment, and side effects when transitioning adolescents from pediatric to adult healthcare. 25 Further, transition issues like psychosocial and developmental issues receive limited attention, such as finishing education and finding a suitable job, achieving independence and separation from parents, and building a social network. Additionally, AWEs experience a gap associated with the inflexible standardized transition to adult care, mainly consisting of a transfer in a referral letter instead of an organized and gradual transition process. 24 This is despite research establishing that transition and transitional care are recognized as critical components of care, emphasizing continuity, coordination, medication management, symptom recognition, self-management, complete communication of information, patient education, outpatient follow-up, and tailored care based on individual patient needs.26–28 How AWEs perceive and are involved in the process will likely influence a successful transition. Discussion and understanding of AWEs’ views and preferences about transition could help HCPs and AWEs develop personalized planning for transition as a whole. There is potential to optimize the transition of AWE from pediatric to adult healthcare and to involve the primary stakeholders in finding new ways to organize and deliver healthcare. In this study, we aim to describe the collaborative development and design of the Joint Transition Clinic in clinical practice. We emphasize the co-design process, involving AWEs, their parents, and HCPs through a participatory design approach. The results of an evaluation of the developed solution will be presented in a separate article.
Material and methods
Study design
A participatory design approach guided the development of the transition solution.23,29,30 PD evolved from action research introduced by Kurt Lewin in the 1940s,23,31 which focused on collaboration between researchers and participants to solve practical problems, aiming not only to study practice but also to change it,32,33 allowing stakeholders to define problems, identify causes, and develop solutions. The goal is to describe users’ knowledge to design solutions that empower them, 31 fostering mutual understanding among stakeholders and enhancing their ability to manage different situations collaboratively. Users and designers engage in continuous mutual learning, with users providing essential insights into their needs and practices. 23 The cornerstone of PD is collaboration, transitioning users from passive data providers to active co-researchers with a voice in the process. 23 We endeavored to give the AWEs a voice at a time when they may have felt excluded. Their perspectives and experiences were essential in developing the intervention. Stakeholder contributions informed each step, ensuring that findings from one stage shaped the next. Through mutual learning, key stakeholders co-created and refined the intervention, resulting in a solution that was developed and endorsed by all participants.23,29,34
This project involved a three-step iterative process: (1) identification of needs, (2) design and development, and (3) pilot test and evaluation.
29
Figure 1 illustrates these phases. The study employed iterative processes for all phases. Phase 1, which describes users’ needs, was reported in two prior studies: a systematic review and meta-synthesis
35
and a qualitative exploratory study with field observations and stakeholder interviews.
24
This article reports on Phase 2, during which an organizational intervention was co-created through workshops utilizing creative tools and techniques.
36
The three phases in participatory design.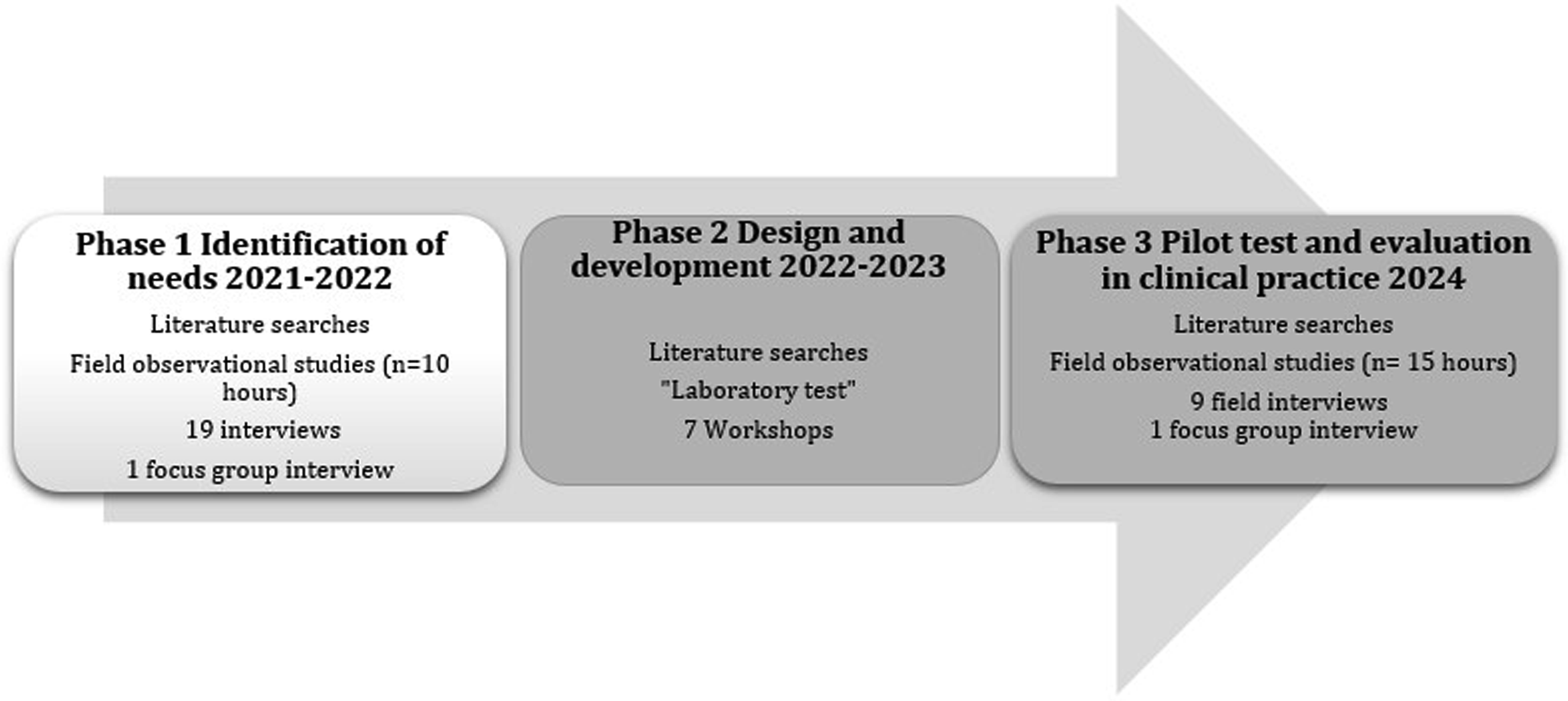
Setting
The study was conducted in an outpatient clinic at a University Hospital, a secondary epilepsy center in Denmark, where adolescents’ routine epilepsy clinic appointments and regular follow-ups were completed as part of the patient pathway. In Denmark, young people with epilepsy are managed at the children’s ward until they reach 18 years of age. Pediatric clinical management involves outpatient treatment, with follow-ups by a doctor and nurse every six months. Adult neurology has one formal scheduled consultation within 6–12 months, followed by predominantly “on-demand” appointments. 37 Each year, around 18–20 AWEs are transferred to adult healthcare. The transition occurs by referring AWEs to the adult department following assessment by a senior neurologist.
Participants
Overview of participants’ characteristics and participation in workshops and pilot test.

PD, pediatric department; ND, neurology department.
The reflective and iterative process during the stages of workshops
Inspired by the PD approach, we applied the iterative cycles of planning, acting, observing, and reflecting, following the methodology of iterative processes in analyzing the data material.
38
Each cycle was built upon the previous one, enabling researchers to refine their methods, enhance their understanding, and adapt interventions based on observed outcomes and reflections. This led to continuous improvement and deeper insights. This ongoing stepwise integration of analysis, design, and development facilitated the planning of the next workshop based on the results and experiences of the just-completed workshop. Member checking was conducted in every workshop to verify the findings, enhance data analysis accuracy, and provide transparency and trustworthiness.
39
Furthermore, we employed various activities to design and develop a solution, as illustrated in Figure 2. Phases 2 and 3 activities summarized. The iterative nature of participatory design involves repeated cycles of plan-act-observation-reflect iterations throughout all phases. Each cycle builds on the previous one, allowing continuous feedback loops, improvement, and deeper insights.
Workshops
Workshops were conducted from April 2023 to April 2024. These workshops were held on the University Hospital. Originally, workshops were derived from creative methods of solving problems group-wise, such as “brainstorming”
40
and reflecting and learning about a predetermined issue to be addressed.
41
As a research method, workshops aim to generate data regarding future design processes and organizational changes.
40
Each workshop had a script with a precise aim and activities. The scripts included the workshop’s aim and a description of all user activities following a rhythm of opening, working, and summarizing. The first author illustrated script parts, such as the day’s agenda and participant’s assignments. The first author created visual illustrations for each workshop that summarized the results of the previous workshop (Picture 1). The workshops were planned and facilitated by the first and last authors and included approaches from future workshops.
42
Each workshop was planned one activity at a time due to the uncertainty of how many iterations would be needed to develop a final solution. Workshops 1 and 2 had working stations facilitated by a researcher who initiated the discussions and participated in the emerging mutual learning process in the groups. All workshops were audio-recorded and documented through field notes, posters, post-its, and photos by the moderator, facilitators, and observer. Throughout the process, the facilitators compiled summaries of the groups’ work. Illustrations from the workshops summarizing results.
Workshop 1: Generating ideas toward a solution concept
Workshop one was arranged as a 2-h session aiming to generate innovative strategies and new ideas for enhancing the transition process, ensuring improved consideration of the needs and wishes of AWEs and their parents. The findings from Phase 1 of the PD project24,35 (Figure 3), informed the initial workshop’s critique and fantasy stages processes. The workshop commenced with visual illustrations of the PD project’s findings derived from Phase 1. During Workshop 1, the participants were encouraged to keep an open mind and embrace a “the sky is the limit!” mindset. Needs and preferences emerging from Phase 1.
Workshop 2: Refining and actualizing ideas and solutions
Workshop 2 was arranged as 2-h sessions, aiming to refine and actualize concepts and solutions from the fantasy stage in Workshop 1 and work towards their realization in the transition, ensuring that the needs and wishes of AWEs and their parents are better addressed. The participants were asked to generate ideas limited to those informing a solution concept based on the ideas that received the most votes at the end of Workshop 1.
Workshop 3–7: “Laboratory test” - developing the joint transition clinic with HCPs
Laboratory testing should be viewed as a step in the ongoing development process 43 and as part of a learning process. 44 Workshops 3–7 were arranged as four-hour sessions to develop the organization of the new patient pathway related to the Joint Transition Clinic. The patient perspectives were represented by data from the ethnographic investigations and workshops 1 and 2. The participants brainstormed, shared, and reflected on different points of view and experiences to best meet the users’ needs, as facilitated by the first author. Pictures, posters, and headings on paper, along with participant comments, were used to illustrate and discuss how the solution could support the workflow as the new patient pathway was reviewed step by step. In this study, laboratory testing of the solution in a clinical setting was planned to support its implementation in a real-world context.
Ethics
The Scientific Ethics Committee granted an exemption from full assessment under Danish law, citing minimal risk, low-risk topics, no sensitive data, and the project’s classification as quality development. The study was additionally submitted to the Danish Data Protection Agency (No. 20202000-229), and it was included in Region Southern Denmark’s register of research projects (No. 21/38124). Participants and HCPs were provided written and verbal information about the study, in compliance with relevant ethical standards. 45
Results
Seven workshops were conducted. Data from each workshop consisting of audio files, photographs, illustrations, and notes written by the participants were collected. The photographs, graphics, and notes were categorized by topic. After each workshop, OAH performed the initial analysis and verified with the research team. Reflectivity in the data analysis was facilitated by the research team’s discussion of their reflections. Below, parts of the content from across the complete dataset are presented, complemented with illustrative pictures.
Participant characteristics
Table 1 shows the characteristics of the participants and their participation. The average age of the AWE participants in the workshops was 18 years.
Workshop 1: Generating ideas to inform a solution
The initial workshop explored the findings from Phase 1,24,35 (Figure 3), to support the idea of the iterative process of PD. Two groups elaborated on ideas and topics relevant to the final solution. The critique stage identifies frustrations stemming from people’s lived experiences, releasing energy for creative thinking in the fantasy stage, where participants explore utopian ideas for potential solutions. Suspending reality in this stage fosters creative and imaginative thinking by allowing participants to express their hopes and dreams. In the fantasy stage, the participants were asked to build a model using creativity in any way they imagined. At the end of Workshop 1, participants presented three of their numerous ideas in plenary: (1) “The Bridge,” (2) “The Knowledge Giraffe,” and (3) “No Rules App” (Figure 4). The three ideas are presented in Table 2. In collaboration with the participants and based on a vote for the essential areas to continue with, the three creative ideas were chosen to be refined and actualized in Workshop 2: the implementation stage. The three creative ideas to work with in Workshop 2 (the Implementation Phase). The image at the top right contains the following Danish text: “No rules; receive a message about what you can and can't do; if you could call the HCP with questions; possibly a personal physician.” Content of the three creative ideas from Workshop 1, highlighted content incorporated in the final solution.

Workshop 2: Refining and actualizing ideas and solutions
In the implementation stage, participants apply pragmatic thinking to their visionary, utopian ideas, exploring and planning how to transform them into achievable changes, either fully or partially. Hence, we aimed to clarify our direction, convey a good impression of the content in a prototype, and provide an initial version of a potential solution or intervention. Three groups discussed and elaborated on the ideas “The Bridge,” “The Knowledge Giraffe,” and “No Rules App” (Figure 4 and Table 2). Significant discussions took place during the idea development stage, with one group’s concept, “The Bridge,” serving as the starting point for the final solution. As one from the group elaborated on the drawing (Picture 2). “It could be bridge-building (transition between pediatric and adult healthcare) where children and adults walk hand in hand. It could be the Great Belt Bridge, which also has a tunnel. Come over and pick the patient up, or come over and visit with open arms. A doctor and perhaps the young person’s parents are in the back of the drawing, running for something that is needed, letting go, standing, waiting, and waving. There are many different roads and bridges to choose from here. Epilepsy is so many different things; you can’t just say this is the best way. What we need is something completely different that others need.” (Mother to AWE) “The Bridge” - Illustration of the main idea for further development. The image features two Danish words: Barn (meaning ‘child’) and Voksen (meaning ‘adult’).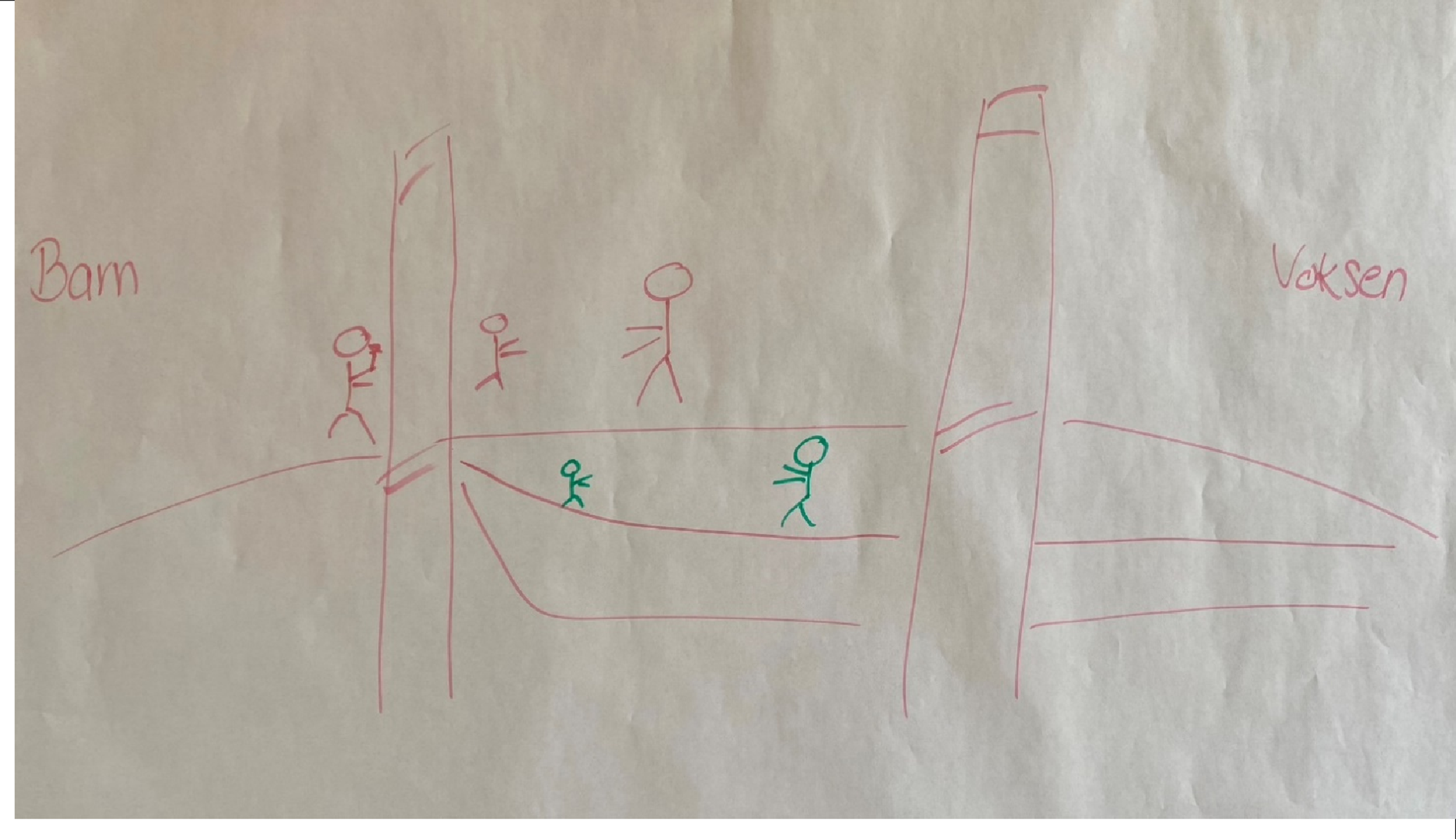
“The Bridge” reflects on and incorporates many of the suggestions from “The Knowledge Giraffe,” focusing on how we connect, communicate, and collaborate between pediatric and adult healthcare via “The Bridge.” This is a conceptual bridge and restructured organization for AWEs, where HCPs assist the transition. All three solutions were considered, and given that “The Bridge” could address most needs, the research team and participants agreed to proceed with its development, incorporating aspects of “The Knowledge Giraffe,” Thus, the Joint Transition Clinic concept was proposed, integrating many of the aspirations and ideas from Workshops 1 and 2. The Joint Transition Clinic unites families and nurses from pediatric and adult departments.
Workshop 3–7: “Laboratory test” - developing the joint transition clinic with HCPs
Based on the experiences and findings from the first two workshops, we developed a new concept for the patient transition process: the Joint Transition Clinic. The previous workshops highlighted the need for improved collaboration between the pediatric and adult departments to enhance knowledge sharing, align expectations, and better meet the needs of AWEs earlier. Three nurses, along with the first author, developed the organization of the new patient pathway and workflow related to the intervention. At workshops 3–7, features and their possible content in the Joint Transition Clinic were discussed based on the findings from the first two workshops. The features, including the joint agenda and the person-centered conversation tool “Inspiration list - what can you talk to a nurse about?” (Figure 5), were designed to support the need for information and communication, providing an opportunity to involve the AWE on their terms. The features guided the consultation on expectations, security, independence, and getting to know the young person. The new patient pathway is centered around the patient, aiming to ensure consistency, meet expectations, and provide security and satisfaction. It offers transitional consultations with active user participation, addressing individual needs, aligning expectations, ensuring security, and maintaining continuity. This patient-centric approach is the key to the proposed improvements. The new patient pathway was suitable for clinical practice, as it was developed by those who would use it (Figure 6). Table 3 provides an overview of the features of the joint transition clinic that have been developed, along with their potential impact on identified needs. Inspiration list - what can you talk to a nurse about?. Schematic representation of the existing and new patient pathways. The features of the Joint Transition Clinic and its impact on identified needs and wishes.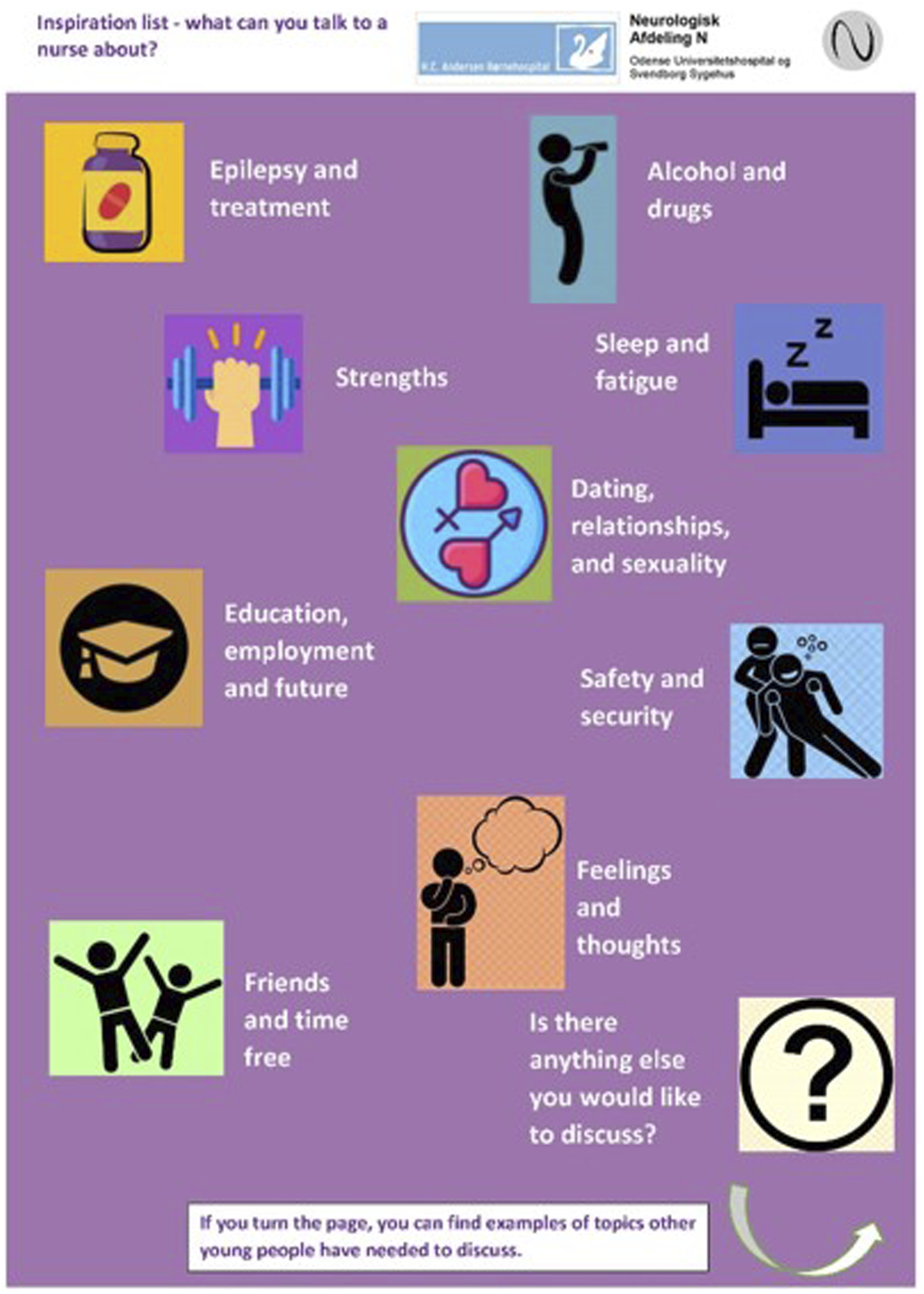


Discussion
A Joint Transition Clinic and a structured follow-up workflow were developed to address a previously identified gap in clinical practice, meeting the needs of adolescents with epilepsy as they transition from pediatric to adult healthcare. This initiative was undertaken in close collaboration with patients, their families, healthcare professionals, and researchers through a participatory design process. User involvement is the core of PD and was essential to our study. Kanstrup et al. 46 emphasize the significance of user involvement, finding that, as key actors, patients can provide original designs that combine everyday living with medical solutions in a way that designers could not have achieved by themselves. This was similar to our study. Furthermore, PD provided AWEs and HCPs with a democratic say in the final product and facilitated mutual learning for all involved. The “Joint Transition Clinic” was designed to facilitate a more patient-centered approach, adaptable to clinical practice, that accommodates AWE’s requests to be seen as individuals, not illnesses.
Adding an extra transition consultation in the Joint Transition Clinic (Figure 6) may have significant cost-effectiveness implications. However, economic analyses of various transition-related programs emphasize that the upfront costs associated with implementing these programs are outweighed by long-term benefits. 47 Structured transition interventions are likely to be cost-effective, leading to improved health outcomes and reduced costs associated with emergency visits and hospital admissions.48,49 However, future research should explore the economic challenges and benefits, as these factors are crucial for decision-makers when considering implementation and ongoing operations.
Although transition clinics for epilepsy have been developed around the world and are viewed as essential to the effective transfer of care, the implementation remains highly variable. 50 Research shows that most practical models for organizing transition care, e.g., transition clinics, educational programs, skills training, transition coordinators, and enhanced follow-up,51–54 have been developed and evaluated, focusing on the effectiveness of health outcomes and the process of passing along appropriate medical information but to a lesser extent tailored to individual needs.55–57 Transition clinics are available for several chronic conditions such as diabetes, 58 heart disease, 59 or juvenile idiopathic arthritis. 56 The challenges faced by AWEs are similarly identified in this study, including the need for holistic approaches that address both medical and psychosocial aspects of care. However, transition clinics tailored to AWEs’ needs, co-created by them, are lacking. Thus, the co-production of this study provided a unique opportunity to explore, learn, and understand the practice as experienced by users, collaboratively searching for new ways to ensure a smooth transition by involving AWEs, parents, nurses, and physicians. User involvement is central to participatory design and has been crucial to our study. The participants experienced valuable mutual learning throughout the development process. Recognizing that not all needs can be met in collaborative studies, the design process continuously focused on bridging communication between AWEs, parents, and HCPs, supported by an iterative PD approach in a search for the best possible joint solution. 29
In a previous study, we identified that AWEs seek understanding, acceptance, and autonomy in managing their epilepsy and transitioning to adult care. 24 Their experiences highlight the importance of holistic support and effective communication in healthcare settings. Fostering the recognition of AWEs as individuals with distinct personalities, needs, and capabilities requires a concerted effort from HCPs. The person-centered conversation tool: “Inspiration list - what can you talk to a nurse about?” was designed to support the need for information/communication and provide an opportunity to involve the AWE on their own terms.
Conducting a PD study requires considerable commitment and effort. Involving users consumed a lot of time, both for the participants and the research team. It was difficult to recruit young patients undergoing treatment for a chronic condition, the challenges of living with epilepsy, and busy HCPs. However, the input from users provided valuable knowledge and was crucial for refining the features of the Joint Transition Clinic and the new patient pathway for clinical practice. In addition, involving users from the clinical practice where the Joint Transition Clinic will be based was important. User involvement in the PD process significantly changed participants’ mindsets. The research team and HCPs learned about patients’ resources and motivation to engage in their treatment and care, while patients gained insight into the HCPs’ professional considerations. The research team relied on HCPs to understand clinical practice. The diverse contributions from all participants were crucial in developing a functional solution that met users’ needs and had a potentially significant impact on them.
Strengths and limitations
A strength of this study was the development of an evidence-based and patient-focused practical solution that spanned multiple departments and disciplines. The development process was iterative, incorporating reflexivity and researcher triangulation. 60 Our study demonstrated how to successfully involve the users in co-designing and developing a solution in the patient pathway.
Limitations include the fact that this single-center study was conducted in a local Danish clinical setting, which raises a note of caution regarding transferability. Furthermore, the relatively low number of participants in the workshops may limit the generalizability to other settings. Limited user participation is a well-known challenge in PD, which can impact the outcomes of workshop-developed designs. 31 Although this may present a limitation in terms of validity, the rich and nuanced data gathered during phase 124,35 was essential in ensuring that all users had a say.
Conclusion
Findings from the seven workshops, informed by the phase 1 needs assessment, guided the design and development of the Joint Transition Clinic, an organizational solution featuring tailored consultations to enhance AWEs’ engagement, preparedness, and sense of acknowledgment. Using a PD approach fostered mutual learning, enabling collaboration with AWEs and key stakeholders to develop a mutually acceptable model for transitioning from pediatric to adult healthcare. Hence, the PD approach effectively created a solution that addresses patient needs while ensuring AWEs and their parents had a voice in its development.
Implications
The pilot test of the Joint Transition Clinic (Phase 3) was conducted from January to May 2024. The experiences of both patients and HCPs will be evaluated through field interviews, video recordings, and focus groups. Based on the evaluation, it must be decided whether the solution should be fully implemented in clinical practice.
Footnotes
Acknowledgments
The authors thank all participating adolescents, parents, and HCPs for their time and insights and for sharing their experiences. The authors confirm that they have read the Journal’s position on issues in ethical publication and affirm that this report is consistent with those guidelines. For English editing, we thank Anthony C. Smith.
Ethical considerations
The Scientific Ethics Committee assessed the study, which granted an exemption from a thorough assessment based on Danish legislation. The study was additionally submitted to the Danish Data Protection Agency with the reference number 20202000-229, and it was included in Region Southern Denmark’s register of research projects with the identification number 21/38124.
Consent to participate
Written informed consent was obtained from all participants.
Author contributions
Ole Abildgaard Hansen: Writing – review & editing, Writing – original draft, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Malene Kaas Larsen: Writing – review & editing, Writing – original draft, Methodology, Investigation, Formal analysis, Data curation, Conceptualization, Supervision. Christoph P. Beier: Writing – review & editing. Anthony C. Smith: Writing – review & editing. Jane Clemensen: Writing – review & editing, Writing – original draft, Methodology, Investigation, Formal analysis, Data curation, Conceptualization, Supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available upon reasonable request.