
Abstract
Background
During the hospital-to-home transition, stroke survivors and their caregivers face a significant lack of support and information which impacts their psychosocial recovery. We aimed to co-design a program combining individual support by a trained case-manager (dedicated professional providing individual support) and an online information platform to address needs of stroke survivors and caregivers.
Methods
A two-step methodology was used. The first step followed a “user-centered design” approach during four workshops with stroke survivors, caregivers, and healthcare professionals to develop the platform and define the case-manager profile. The second step was a usability test of the platform following a Think Aloud method with patients and caregivers. The workshops and interviews were analyzed following a qualitative thematic analysis. The analysis of Think Aloud interviews was based on User Experience Honeycomb framework by Morville.
Results
Eight participants attended the workshops: two patients, two caregivers, three nurses, and a general practitioner. Activities, training, and skills of the case-manager were defined according to stroke survivors and caregivers needs. Name, graphics, navigation, and content of the platform were developed with the participants, a developer and a graphic designer. The usability of the platform was tested with 5 patients and 5 caregivers. The Think Aloud confirmed satisfaction with graphics and content but a need for improvement regarding the navigability. An update of the platform was conducted in order to answer the needs expressed by participants.
Conclusion
We developed, with a participatory approach, a patient-centered transition program, which will be evaluated in a randomized controlled trial.
Introduction
According to the Global Burden of Diseases stroke is a leading cause of disability. 1 The incidence of stroke is increasing among young people with an estimation of 25% of stroke occurring in people younger than 65 y.o. 2 Due to the improvement of acute care management, the prognosis of stroke is improving alongside an increase in the prevalence of invisible disabilities (ID) among stroke survivors (SS), a longer life expectancy with post-stroke disability, and new needs arising to younger age obligations (family organization, children education, returning to work). The ID may be caused by a physical or mental condition that impacts the individual's ability to satisfy basic social and personal needs without being perceived by others. 3 The invisible disabilities caused by stroke include, alteration in sensorial, cognitive, and psychic functions such as fatigue, anxiety, or depression.4,5 ID will therefore have an impact on the lives of SS by affecting their psychosocial competencies 6 and subsequently creating limitations in their activities and/or restrictions on social participation. Participation is defined by the International Classification of Functioning (ICF) as a person's involvement in a real-life situation or as “the lived experience” of people in the actual context in which they live (e.g. taking part in family activities).7,8 It is known that people with post-stroke ID have a lower life satisfaction and capacity to adopt self-management behaviors than the general population. 9 Self-management is defined by Bandura as the ability “to monitor their health habits, set themselves short-term goals, and report the changes they are making” (e.g. for sedentary lifestyle, to set up a daily walking time and monitor the reaching of this objective). 10 Moreover, one-third of stroke survivors suffered from apathy characterized by a loss of motivation which impairs their capacity to self-manage their recovery. 11 This might be increased by a lack of information and support regarding the ID of stroke, that are often not anticipated before hospital discharge.
The hospital-to-home transitional period is a key step in the recovery of SS and their informal caregivers (ICgs). 12 Hospitalization and the first months at home following stroke are a difficult and complex period.13,14 Indeed, returning home with unanswered questions is a source of stress and anxiety for SS and their ICgs, 15 and it is not possible to anticipate at hospital all issues that the SS and their ICgs will face when back home.16,17 It is estimated that half of SS suffer from fatigue, 18 30% from post-stroke depression,19,20 24% from post-stroke anxiety21,22 and 30% to 50% of young SS do not return to work after stroke. 23 On the other hand, ICgs are also prone to depression and anxiety, which increase the burden they feel.24,25 During this period SS and ICgs are looking for a validated individualized information, which evolves over time according to their needs.26–29 When SS returns home, the main priority is to obtain information about the stroke, then over time, needs evolve towards managing the SS emotions and behavior, and then the caregiver's needs. 12 In the long term, the needs expressed by SS concern activities of daily living, social participation, mobility aids, home adaptation, housing, financial assistance, rehabilitation, information, and transport. 30 Chen et al. identified three key factors to enable hospital-to-home transitional care which are: partnership approach to individualize transitional care, being prepared to navigate between health and social services and self-management abilities. 15 The factors described by Chen et al. are aligned with the tasks and skills of case managers. Case management involves providing an individual support by a dedicated professional (i.e. the case manager) to assess, plan, and coordinate the care of patients with complex needs. 31 It is a common approach in chronic diseases31–33; however, it has never been used in the context of stroke in France. Case-management is effective in chronic diseases to ensure patients have access to all the resources they could benefit from, improve quality of life and promote rehabilitation.34–36 This support could help SS to adapt to their new situation and promote self-management. 37
In addition to a follow-up with a case-manager, access to online resources about stroke could provide complementary information to support psychosocial recovery. 38 This kind of intervention, combining access to online resources and personalized support, could be of interest in a psychosocial recovery approach, improving social participation and self-management of SS.39–42 However, actual interventions developed to improve post-stroke transitional care mainly focused on functional rehabilitation. These interventions do not use a global perspective integrating psychosocial aspects and considering impact on informal caregivers.
Based on existing literature and previous studies on patients and caregivers needs,43,44 the aims of this study are to develop with a participatory approach a patient-centered transition program called Navistroke, combining an access to an online information platform and a personalized support from case-manager, and to test its usability. This study is part of a larger project, a randomized controlled trial called Navistroke 45 (NCT03956160).
Methods
To achieve this aim, we conducted a participatory research following guidelines of the “user-centered design” (UCD) approach. 46 This approach involves including the product's/program end-users in every stage of its development. In our study end users were stroke survivors, their informal caregivers and healthcare professionals. Our approach followed two steps: #1 Designing the components of the Navistroke program combining case-management and access to an online information and resources platform by conducting co-design workshops and #2 Testing the usability of the platform by conducting semi-structured interview following a Think aloud method.47,48
Theoretical underpinning of the intervention
In the field of health behavior change, a large number of theories aim to promote self-management in chronic diseases. We based our intervention on the International Classification of Functioning, Disability, and Health (ICF) and on the social cognitive theory from Bandura.7,10,49 The ICF considers several dimensions in the functioning (body function, activities, participation, and environment), our intervention's first goal is to improve SS social participation and largely include their environmental factors, notably social factors. We also used the Bandura social cognitive theory to support SS and empower them in their psychosocial recovery process. Bandura's theory describes 4 processes involved in promoting self-management: self-monitoring (observing and recording one's behavior), self-evaluation (comparing one's performance), self-reaction (modifying one's behavior in response to performance evaluation), and self-efficacy (believing in one's ability to achieve one's goals). It is the most widely used in interventions aimed at improving self-management of chronic diseases32,50
Co-design workshops
Participants
Stroke survivors and informal caregivers were recruited during stroke center follow-up visits of Hospices Civils de Lyon. Health professionals were recruited from the stroke center of the Hospices Civils de Lyon, the Rhône stroke care network, or the lists of healthcare professionals with agreement to deliver post-stroke driving authorization.
Data collection
The codesign phase included four workshops facilitated by MD and MM on a semi-structured approach similar to focus group facilitation. Workshops 1 to 3 were 2 hours 30 minutes long and the 4th workshop was 2 hours long. The first and second workshops were dedicated to case-manager profile definition through several activities (a stroke pathway timeline to describe poststroke difficulties from stroke onset to the discharge home, and the various medical and social services needed to help the recovery once they have returned home, case-manager tasks and functions to face these difficulties, case-manager ID card: name, training, missions, skills, knowledge, and patient contact details). To help participants in their reflections, the concept of case-management was defined and discussed with them, providing examples of the use of this method in other chronic diseases. 51 At the end of the 2nd workshop, a first outline of the information platform was also presented to the participants (Figure 1). Finally, the third and fourth workshops were dedicated solely to the platform, and focused on its content and form, its strengths and limitations, and the adaptations to be made as a result. During these workshops, the platform's graphic designer presented the mock-ups to the participants. The workshop facilitation guide (annex 2) was based on literature review about existing post-stroke programs focusing on psychosocial rehabilitation and SS/ICg needs after stroke.44,52 The methodology followed an iterative process, the facilitation guide evolved after each workshop.
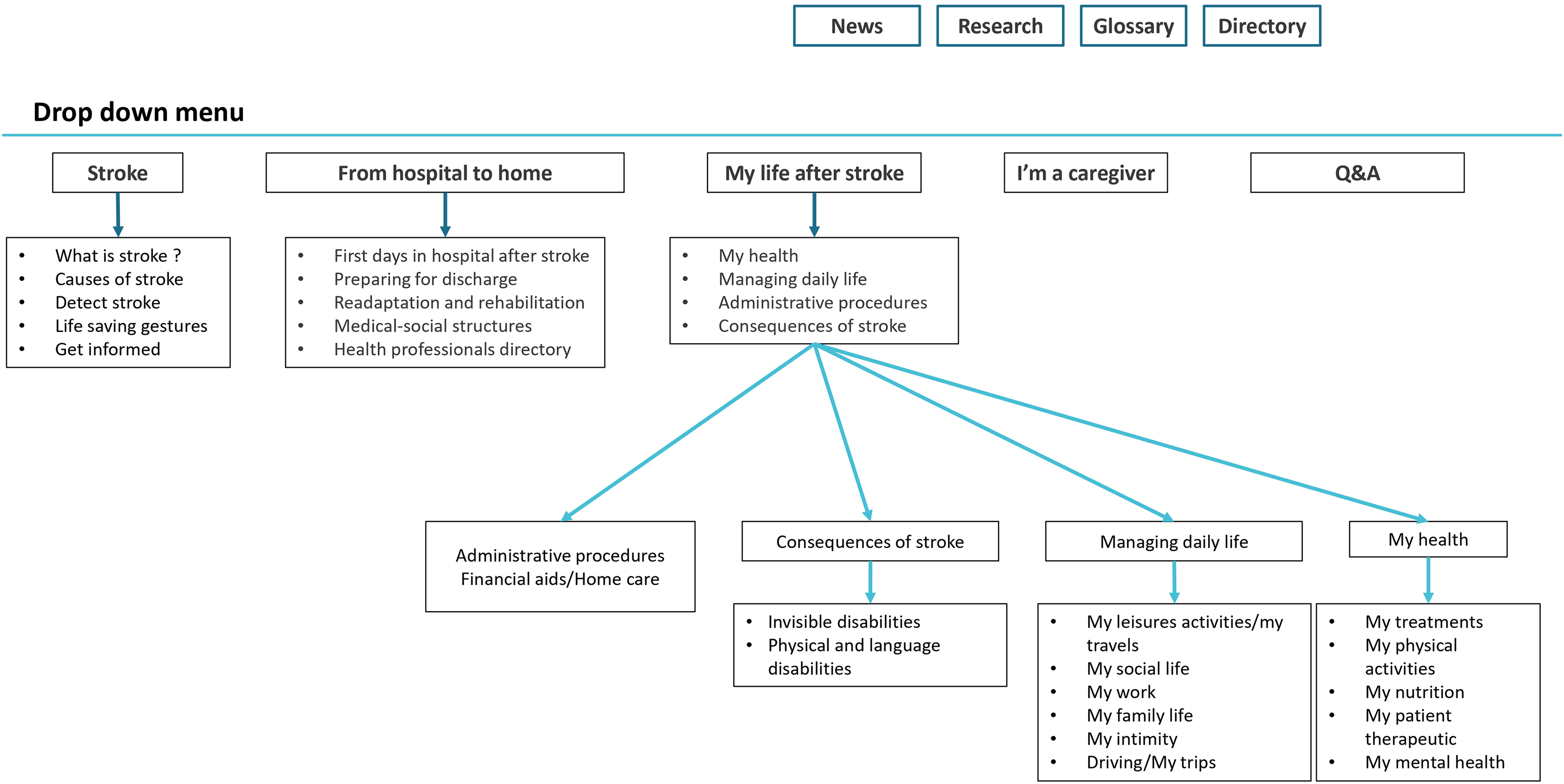
First draft of the graphical organization of the platform proposed to participants in workshop 2.
Data analysis
The analysis was based on audio recordings of the workshops, observation notes, and animation materials. A thematic content analysis following the approach proposed by Bardin 53 was carried out using NVIVO software (Nvivo QSR International). 54 The analysis grid was based on the themes of the interview grid, enriched during the analysis of emerging themes and sub-themes. The data from different sources (workshops, observational notes taken during the workshops and group dynamics) were analyzed to get an understanding of participants needs and expectations towards the intervention and to produce materials for the intervention (case-manager profile, tasks, and platform content).
Usability testing
The second stage of the study evaluated the usability of the information platform developed during the workshops through Think Aloud interviews. The usability is defined by the ISO 9241-11:2018 as “extent to which a system, product or service can be used by specified users to achieve specified goals with effectiveness, efficiency and satisfaction in a specified context of use.” 55
Participants
The participants in the second phase of the study were independent of the workshop participants and did not take part in the co-design workshops. Stroke survivors and their informal caregivers were recruited from two different places: #1 stroke center follow-up visits of Hospices Civils de Lyon, and #2 among participants of a post-stroke rehabilitation program. We also contacted SS and ICgs among participants in previous stroke studies conducted by our unit who had agreed to be contacted for future studies. To be included participants had to be SS or ICg of a stroke survivor, being older than 18 years old, being able to come at the workshop site, and live at home in the Rhône department.
Methods and data collection
The Think Aloud method consists of verbalizing the resolution of a task or a problem. 48 This method was initially developed to understand the cognitive process involved in solving a problem/task, it is frequently used in the usability testing process. 47 In our study, we aimed to understand the experience of the users when they first connect to the platform.
For this second part of the study, the interview guide was based on the User Experience Honeycomb (UX H) framework from Peter Morville. 56 The UX H is divided into 7 parts: #1Useful, #2Usable, #3 Findable, #4 Credible, #5 Accessible, #6 Desirable and #7 Valuable. Due to the context in which the interviews were conducted—that is, experimental tasks on the platform, dedicated link to access the platform, and presentation by the research team, the Findable, Credible, and Valuable part of the framework was not assessed. The guide was divided into three parts: #1 Participants were asked about their difficulties and the solutions used to overcome them, #2 Participants had to complete a list of 9 tasks and verbalize the resolution of the tasks and #3 to conclude the interview participants were ask how to improve the platform. The interview guide is available in annex 2. The lists of tasks target similar dimensions between SS and ICgs allowing the research team to triangulate the data, and some questions were specific to the profile of the interviewee (e.g. for ICgs we asked them to find a training to communicate with the SS in case of aphasia) (Table 1).
Detail of task by stroke survivors and informal caregivers.

Data analysis
The interviews were audio-recorded and the navigation on the platform was screen-recorded. All interviews were transcribed anonymously (SS for stroke survivors and ICg for Informal Caregivers followed by the number of the interview, e.g. the fourth interview of an SS was anonymized “SS 4”) and a deductive and inductive thematic content analysis was carried out. The deductive part was guided by the UX H framework. We investigated the perceived usefulness, accessibility, and desirability of the platform and its content through the participants’ speeches while they were using it. The usability of the platform was determined through the Think Aloud task resolution process. The different sources of data (interviews and notes taken during the interview) and populations (patients and caregivers) were triangulated. The transcript was encoded by MD and MM.
Ethical issues and approval
The study was approved by the Medical Ethical Review Board of the Hospices Civils de Lyon (N°20-93) Informed consent was obtained for all participants. Only researchers involved in the data analysis had access to the data. The authors used the COREQ guidelines to adequately report the results. 57
Results
Co-design workshops
Workshops were conducted between February and June 2022. Participants were stroke survivors (n = 2), informal caregivers (n = 2), and health professionals (n = 4). The two SS presented invisible disabilities (emotional disorder and aphasia for the first, fatigue for the second). One of the two ICgs was accompanying his wife, who had suffered a stroke and was also taking part in the workshops, and the second ICgs was there independently of his relative (who had communication disorders following his stroke). Among health professionals’ participants, 3 were nurses implicated in stroke pathway, 1 of them was a representative of the stroke network of the Rhône and the last one was a general practitioner (GP) accredited for the post-stroke driving license recovery process.
The number of participants changed over time due to organizational constraints (workshop 1: n = 8, workshop 2: n = 7, workshop 3: n = 4, workshop 4: n = 3); at least 1 SS or ICgs representative was present at each workshop.
Difficulties encountered in the stroke pathway—workshop 1
The first workshop was dedicated to discuss the difficulties encountered by participants in the stroke pathway. Three themes and eight subthemes were identified (Figure 2).
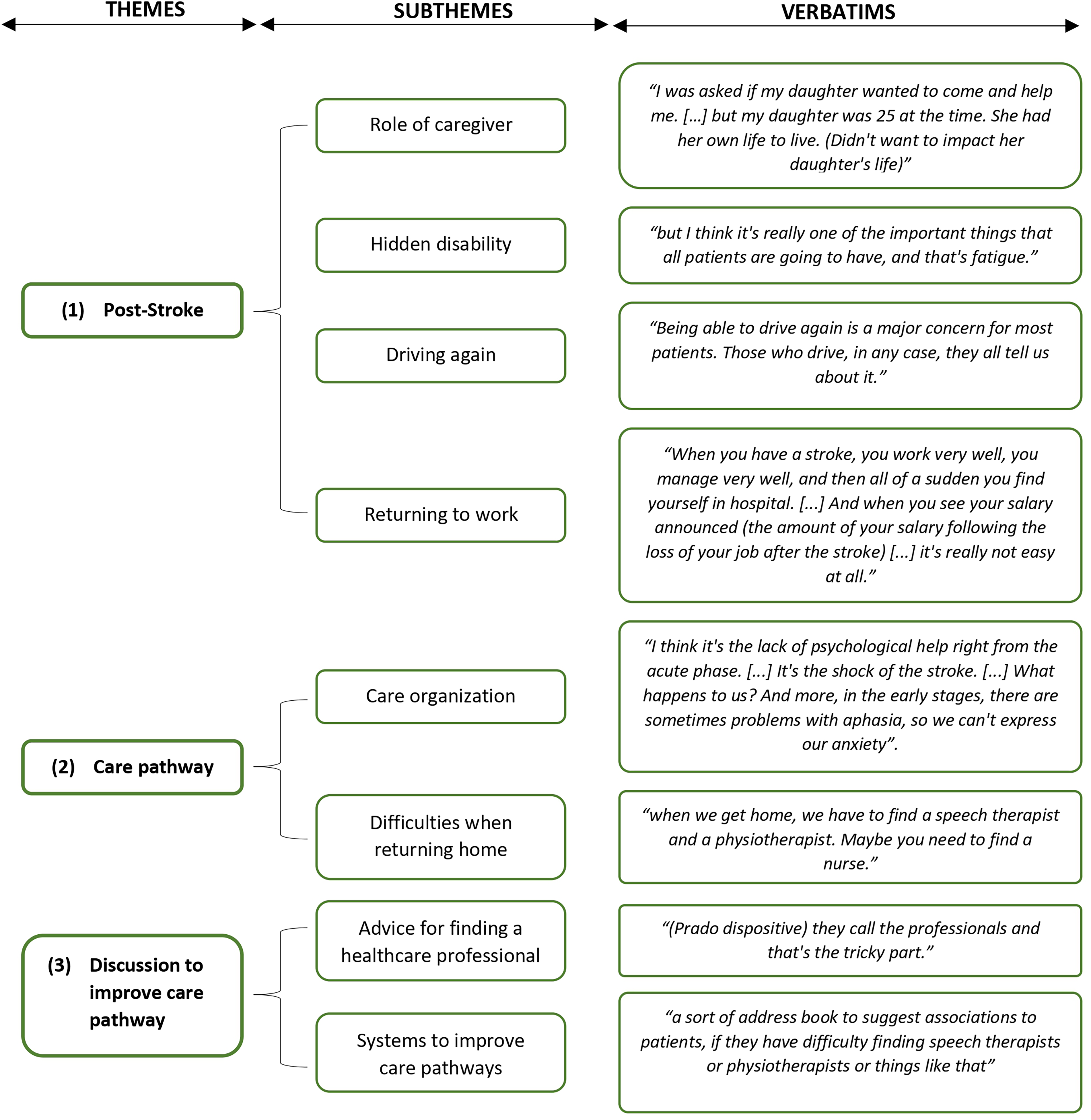
Thematic map of the identification of needs. First workshop.
The results of Workshop 1 led to reflection on the intervention components planned by the research team, and were the subject of the three following workshops.
The case-manager—workshops 1 and 2
Participants discussed case-manager profile, abilities, and skills. Firstly, the case-manager has to be knowledgeable; participants specified he/she must be familiar or trained on stroke, sequelae, and medico-social services organization. Secondly, he/she also has to have strong psychosocial skills. This includes listening and communication skills, adaptation, and dynamism, in order to be able to adapt and react to the needs of SS and ICgs. Participants felt it was important for case managers to be trained to recognize and adapt to ID. Aphasia was cited as an example by mentioning that the case-manager needs to be trained on how to communicate with aphasic patients.
Participants described the following tasks for the case-manager (CM): orientation, referral, and setting up an individualized pathway that consider the needs of SS and their ICgs, proposing appropriate solutions and adapt the pathway to the evolution of their need over time. Health professionals also mentioned that CM should be able to link primary care to hospital care. It was mentioned that in order to promote self-management and empower SS, the CM could orientate SS and ICgs through the healthcare system but without organizing the appointment for them, since the SS/ICgs have to conduct action by themselves. For example, CM might recommend to contact a health or social professional explain the reasons and help to identify the professional but the SS/ICg would have to program the visit.
Regarding case-manager's methods, participants agreed that the CM should be able to contact SS and their ICgs in a variety of ways (telephone, videoconference, emails, or on-site appointment), as well as making home visits at the patients’ request. Participants agreed that the first contact should take place during hospitalization and that four appointments should be scheduled systematically 7 days, 1 month, 3 months, and 6 months after the patient's return home.
The name “case-manager” appeared too complex for participants and not representative, “the term case-manager is too reminiscent of financial aspect of the management (…) it doesn’t make sense.” Moreover, the notions of guidance and advice were mentioned several times, leading participants to name the case-manager, “post-stroke companion.”
The information and resources platform—workshops 2 to 4
The research team designed the first platform outline and contents following the thematic content analysis from the first workshop, and presented it to participants in a graphical way (Figure 1).
The first time the platform organization was presented to participants, it was divided into five parts corresponding to four main tabs: #1 Stroke; #2 From hospital to home, #3 My life after stroke, #4 I’m a caregiver, and a Q&A section. Modifications were made during the co-design process. The Q&A was removed due to feasibility concerns, since we were not able to dedicate a professional to the facilitation and moderation of an online forum. The four main tabs were validated by the workshops’ participants, and thus maintained identical with some minor adjustments on the content in the #1 “Stroke” and #2 “From hospital to home” tabs. Professionals expressed reservations about the “healthcare professional dictionary” section, they feared that SS may experience a feeling of failure if they contacted healthcare professionals on their own—they emphasized the importance of the CM to support patients to identify and reach healthcare professionals.
The content of the fourth tab dedicated to ICgs (Figure 2) was created with the participants, who emphasized the importance of addressing the psychological aspects of caregiving, listing existing caregivers’ associations and support/training programs available for ICgs. Four sub-sections were developed: #1 administrative procedures, #2 health, #3 training, and #4 testimonials.
Alongside these four main tabs, additional tabs were developed: directory, news, and glossary. During the workshops, participants mentioned numerous references and resources, which led to the creation of an additional tab called “media library,” in which are referenced books on stroke and testimonial videos developed for the project.
Content and visuals of the platform were presented to participants during workshops. Participants recommended that text content be shortened and proofread by experts (healthcare professionals specializing in stroke). The organization of the platform and the graphical charter were discussed with workshop participants in each workshop with a graphic designer and a developer and then integrated in the platform. The process led to the first validated version of the platform (Figure 3(a) and (b)).
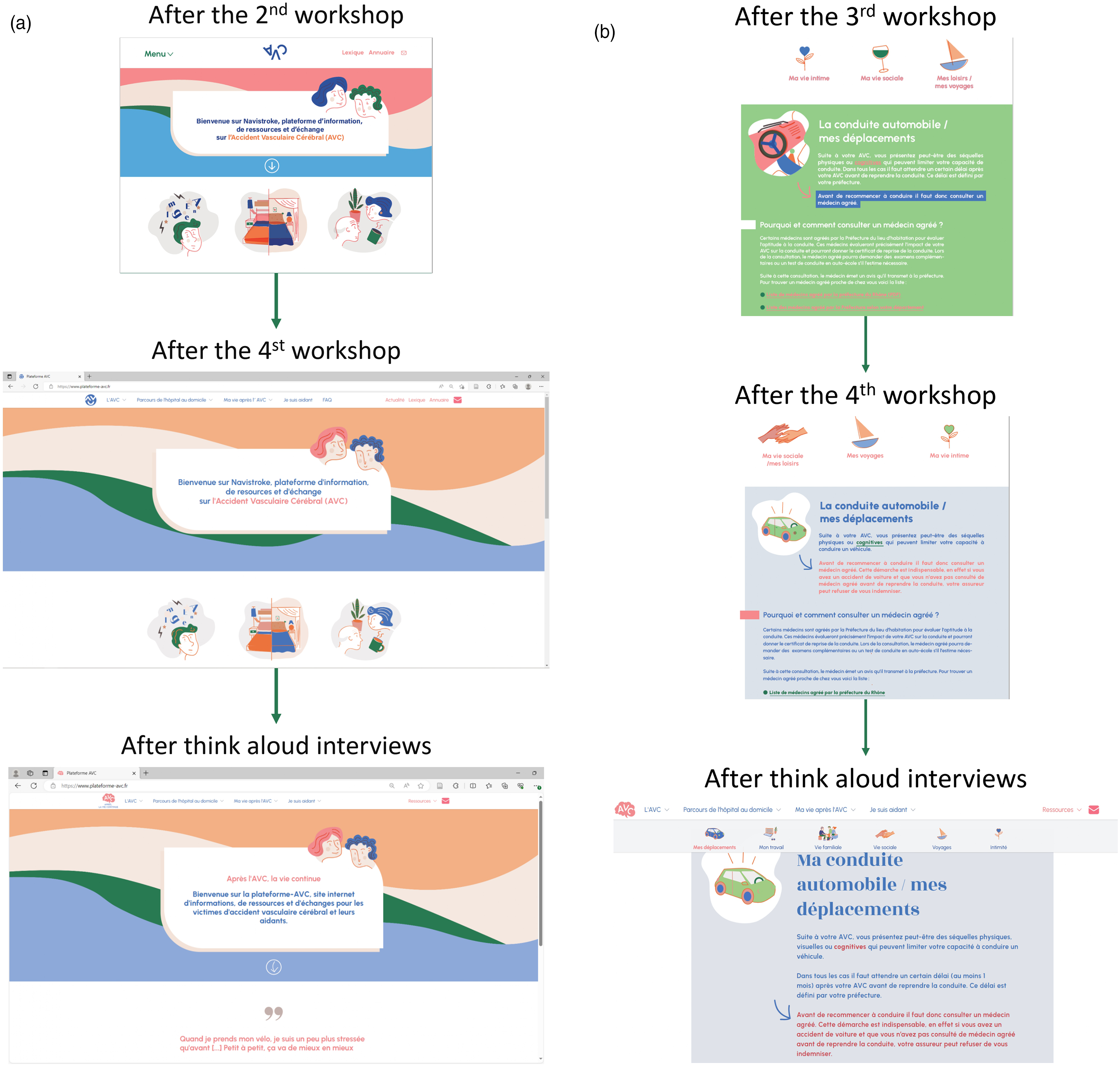
(a) Evolution of the home page during the co-design process. (b) Evolution of the “my life after stroke” page during the co-design process.
Usability testing
A total of 10 cognitive interviews were conducted between December 2022 and January 2023 to obtain feedback regarding the use of the platform. On average interviews lasted 66.9 min. Among the participants, 6 were men and the average age was 61.5 y.o (51.6 y.o for SS and 71.4 y.o for ICgs) (Table 2). All the SS had at least one ID, including fatigue, concentration, or communication disorders. All five SS were employed before the stroke and four were still employed after the stroke, the other one being unemployed due to the sequelae of his stroke (Aphasia). Of the ICgs, one was employed and four were retired. None of the participants were aware of any other stroke-related websites, although one ICgs mentioned looking for information on the hospital website following his wife's stroke.
Descriptive characteristics of think aloud interview participants.

For caregivers, type of stroke of their relative.
Useful (UX H)
Participants identified with the platform's content, in particular content related to post-stroke sequelae, particularly fatigue, speech disorders, or emotional disorders, and content relating to the adaptation of everyday life, notably the resumption of driving. For instance, regarding fatigue: SS 4 “And so, fatigue […] I didn’t perceive it right afterwards. And now that I'm back at work, it's something that's obvious. So, I like it when it comes first (about the organization of the ‘Consequences of stroke’ tab)”; or driving: SS 5 “that's something I've been looking into (information on post-stroke driving), actually about driving since I had to get my license revalidated.” Regarding getting back to work participant mentioned the lack of information on the platform related to the specific work positions or status, SS 4 “well for public administration, there are specific formalities that aren't exactly the same as for private sector employees” or SS 2 “Well, I didn't just do half-time, I did a progressive half-time […] it's true that there's a lack of information for non-salaried (self-employed) people.” Finally, two participants outlined that the content dedicated to ICgs was useful for them or their relatives: SS 5 “Understanding the sequela of a person who has suffered a stroke. [..] how to cooperate with the medical world. Because, even though we're well cared for, there are a lot of things we don't know.”
Usable (UX H)
The usability was evaluated through a task resolution process and the results are presented in Table 3.
Think aloud task-solving results by thematic of the tasks.

SS: stroke survivor; ICg: informal caregiver.
Tasks relating to the use of the directory and dictionary on healthcare professionals encountered respectively six and five failures. Participants had difficulties in identifying the directory 3 they failed to find it and abandoned. 3 Five participants also failed to find information on the role of the speech therapist. Participants mentioned that the directory and health professionals dictionary were not visible enough: ICg 5 “It's important to have a directory to find an address quickly. I would have put it a little more apparent.” Finally, all participants succeeded in locating the social and financial assistance for disability form on the site but encountered difficulties in locating it, using several paths to access it. The form had no dedicated section on the platform.
Accessibility (UX H)
Ergonomics: The platform seemed easy to handle at first use. Several participants approved the hierarchy of information and the way in which content had been categorized between the four main tabs, SS 4 for “there's certainly been a lot of thought, a lot of reflection, reflection behind all the heading, the presentation and it shows,” SS 5 “So there, effectively, the info is easily accessible.”
Readability of the text: Language level, length of sentences, paragraphs were approved by participants SS 1 “It's not all paving stones, it's adapted to people with attention problems who won't read for long.” Despite positive feedbacks regarding the accessibility of the platform, some content remained difficult to understand or use, such as the administrative procedures sections which were difficult to understand as they contain a lot of acronyms, ICg 1 “What's ‘CESU’?”; ICg 2 “First you need to know what the ‘MDPH’ file is.” SS 3, who suffers from aphasia raised the complexity of the definitions given in the section dedicated to speech disorders: “Complicated, but I understand.” Participants also found it challenging to identify where you are on the platform. To overcome this problem, they suggested that sub-tab or hierarchies (breadcrumb trails) appear at certain points on the page, SS 1 “I was thinking of a sub-menu for the headings you've put in, because I'm thinking, if I'm in the shoes of someone who had a stroke and has attention problems, or who's already having trouble reading 3 pages, or who has problems like that, it might be complicated for them to have to navigate everywhere.” Finally, 4 out of 10 participants mentioned that they would have appreciated a search bar to access the information on the site directly, rather than having to navigate through the various tabs.
Desirable (UX H)
Three out of 10 participants recommended to bright-up colors, SS 2 “I’d like to see a bit more color, I think. Because the red, the blue, it's a bit sad.” Finally, two participants mentioned that the directory's position in the taskbar was not sufficiently visible.
At the end of the interviews the platform was updated to meet patients’ expectations (Figure 3(a) and (b)).
Discussion
We used a two-step co-design approach to develop the Navistroke program which combines a case-management support and access to an internet information platform to support stroke survivors and their informal caregivers to improve their self-management skills and social participation. We involved the project's stakeholders at every stage of the program development. End-users (stroke survivors and informal caregivers) worked hand in hand with the research team, the medical team, the developer, and the graphic designer of the platform to develop a program that met their expectations.
The needs and difficulties expressed by participants regarding psychosocial issues and navigating the healthcare pathway during the workshops and interviews confirmed and reinforced the relevance of the program. Currently, the majority of post-stroke programs do not place psychosocial recovery at the forefront,58,59 while this represents a priority to patients and their caregivers.12,26,29 This translates into a limited number of programs improving quality of life and psychosocial recovery of stroke survivors,38,60 or reducing caregiver burden. 61 A similar intervention combining case-management and access to online resources by Reeves et al. reported an improvement in global physical recovery and patient activation at 3 months,62,63 but it did not significantly improve psychosocial recovery and it did not provide the longer-term evaluation. 51 We expect the two components of the Navistroke program (platform combined with case management) to improve the self-management of SS and ICgs, 15 to resume their activities, and eventually improve their social participation.43,44,64 To achieve its goals, the Navistroke program was developed to act on the 4 processes described in Bandura's social cognitive theory 49 (Figure 4). Consequently, the components of the program were developed with the aim of improving SS self-monitoring and self-reaction skills with regard to their stroke consequences. In this way, the online platform will be complementary to the “case management” component of the program.

Navistroke transition program description through Bandura's theory.
Online resources are promising to provide SS and ICgs support, reassurance, information, and social support notably to manage post-stroke depression.39,42 The main priority expressed by SS during the hospital-to-home transition period was the need to have a validated and individualized information. 12 The User-centered process allowed us to directly discuss and define with end-users the content and the information to provide on the platform to ensure that it met their needs at different moments of the stroke pathway. This has led us to rethink the structure of the platform and how it complements the case manager, and to add specific sections on definitions, caregivers’ needs and existing support programs. Since it has been shown that sharing experiences with peers who have gone through the same experience can have a positive impact on psychosocial recovery,65,66 video testimonials and contacts from patient associations will be made available. However, while direct interaction between SS/ICgs through an online forum or questions/answers has been mentioned, participants acknowledge the low feasibility of moderating discussions on such a forum, leading to the abandonment of this functionality. Indeed, non-moderated forums might be beneficial but also face the risk of negative spirals for vulnerable patients that may induce a deleterious effect on the patient's psychosocial recovery. 65
Complementary to the information and resources provided by the platform, the CM will offer personalized support to stroke survivors and their caregivers. In this way, he/she may use positive reinforcement or motivational interviewing techniques 67 to help the SS monitor their progress and reinforce their sense of efficacy. Besides, the CM will also address ICgs concerns, help them to cope with the situation, to organize their day-to-day lives with the SS and find adequate support. Case-management is commonly used in chronic diseases, with common components, such as regular phone calls combined with in-person visits; ensuring therapy adherence; and training on self-management skills. 34 A systematic review highlighted that case-management had a significant impact on reducing anxiety and depression in chronic diseases. 34 We therefore hypothesize that this effect would also be found in post-stroke case-management intervention.
The strength of this project is the process used to develop the program based on scientific evidence and experiential knowledge of stroke survivors and informal caregivers to ensure its relevance. The program has been designed to ensure that whatever their sequelae (apathy, anxiety, language disorders…), it adapts to their needs over time and accompanies them toward autonomy and psychosocial recovery. Indeed, to our knowledge, there are no transition programs focused on stroke survivors that have been entirely co-designed with them and that target psychosocial recovery in France. Our project has also some limitations, firstly, we had difficulties to maintain participation during all the workshops generating an attrition bias. However, only one definitive dropout was registered, while other non-attendances were due to last minute personal impediment. These are frequent issues in participatory and qualitative approaches, when asking a group of participants to attend several sessions. 68 However, the second step of the co-design process enabled us to enlarge the panel of patients/caregivers and ensure that the platform was designed according to the needs of a more diverse population. Secondly, the use of qualitative methods in the present study does not make it possible with the limited sample size to get a representative sample of the stroke survivors’ population that will use the program. To limit this bias, we worked with various profiles of stroke survivors with an identified ID, informal caregivers of stroke survivors with an ID, and healthcare professionals involved in stroke management at various levels. However, the aim of this study was to include the perspective of participants with lived experience of stroke during the design phase of the intervention. A perspective of this project is also to test the feasibility of this program in a pilot randomized controlled trial including a larger and representative sample size of SS and their ICgs entering the transition phase between hospital and home and during the 6 months following this transition. This pilot trial will explore the relevance and effects of the program and identify its barriers and facilitators for SS, ICgs, and the CM, as well as the implementation of the program in daily practices.
Conclusions
In this study, a participatory co-design method was used to develop a post-stroke transitional program that meets the needs of stroke survivors and their informal caregivers. This process allowed us to better conceptualize how components of the program might overcome difficulties encountered by stroke survivors and their caregivers during the stroke journey. This program will be implemented in a feasibility study. As this program includes the arrival of a new stakeholder in the post-stroke care, the case manager, it will be essential to investigate the implementation of this program in the current stroke care pathway.
Footnotes
Acknowledgments
We would like to thank the study participants for their involvement in the various stages of the Navistroke program co-construction process. The research team would also like to thank Clément Enjolras, web developer, and Mélanie Lefeuvre, graphic designer, for their work on developing the platform.
Contributorship
MD and JH conceptualized the original draft of the manuscript. MD, MM, JH, OH, AT, and AMS designed the protocol of the study. MD and MM developed the interview guides, conducted and analyzed the workshops and interviews. MD, MM, and LD recruited the participants. MM, OH, AT, AMS, and LD critically reviewed and revised the manuscript and made appropriate edits or changes.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The medical ethical review board of Hospices Civils de Lyon approved this study (REC number: 20-93).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was partly funded by the Abbvie Santé & Perspectives endowment fund.
Guarantor
Pr. Haesebaert Julie