
Abstract
Introduction
There is currently a lot of demand for healthcare systems around the world to lower costs, increase and improve service efficiency, and increase access while maintaining or even raising the quality of healthcare services offered. 1 This demand could be satisfied with the analysis of the hospital data to understand its operational status quo and to make fact-based decisions. Hence, the collection, storage and processing of hospital’ s data are of importance. Hospitals’ data is huge and varied in format. Thus, the acceptance and successful application of health information systems and technology are essential to the success of the healthcare sector which is a significant social and economic component of contemporary societies.2–4 The health information system and IT applications in hospitals are claimed to make hospitals smarter. Business intelligence (BI) as a kind of information system has grown in importance as a field of study for both researchers and practitioners due to the critical role that data plays in aiding organizational improvement. 5 By using data, statistical and quantitative analysis, explanatory and predictive models, and fact-based management to inform decisions and actions, BI is defined by Davenport and Harris 6 as a collection of tools to collect, store and process data to provide a precise understanding of corporate performance. Hence, BI could be used to create smartness for hospitals. The last 10 years have seen tremendous advancements in the field of business intelligence. 7 Chen, Chiang and Storey 5 have noted that BI holds promise for the healthcare industry. It is well known that BI may help healthcare firms with better patient care and results, efficient use of human resources, increased process efficiency, and cost savings. 8 BI can assist healthcare organizations to achieve better performance and advance the continuum from intuitive to precision medicine.9,10 By giving hospitals strategies for developing tailored data, enhancing medical safety and quality control, optimizing medical procedures, and enhancing smart hospital administration, BI applications can lead to a higher level of smartness in hospitals. These enhancements aid in achieving goals for the quality of health services. 11
A definition of smartness concerning IT-enabled technologies used in healthcare systems is necessary for a meaningful discussion about smart hospitals. From “not smart at all” to “unscripted/partially scripted invention”, there are five categories of intelligence. According to Mettler and Vimarlund, 12 the complexity of the clinical component and the multiplicity of stakeholders make it difficult to integrate BI systems to create smarter hospitals. In truth, there is no comprehensive framework for the development of BI that is available to medical institutions. 13 The problems with the current BI frameworks are emphasized, especially when it comes to how well they work in a complicated field like healthcare. The current BI frameworks are inadequate to meet the needs of healthcare industry. 14 Thus, domain-specific BI frameworks for assessing smartness are important, especially for evaluating the smartness of hospitals. To facilitate processes of expansion and continual improvement, it is crucial to monitor and evaluate the smart levels of BI-based solutions in hospitals. 10
The world is currently concentrating on the 4.0 Industrial Revolution and digital transformation. Clinicians and the public in Vietnam are generally optimistic about the potential of digital technology. 15 The Vietnam Ministry of Health has released new digital health policies and guidelines in conjunction with the development of national health databases like electronic health records (EHRs). 16 However, most hospitals in Vietnam have only partially embraced telemedicine, eHealth, and electronic medical records. 17 Moreover, there is a lack of a framework for evaluating the smartness of hospitals, which is necessary for ensuring the success of digital transformation of the healthcare industry in Vietnam. Therefore, more research is needed to guide the implementation of smart hospital models in Vietnam.
BI application in healthcare industry is limited, despite its promising application and benefits. 18 Due to the complexity of the healthcare industry, domain-specific BI frameworks for hospital smartness evaluation are still in shortage. There hasn’t been much research done on how to effectively apply a BI solution in this field. 8 More precisely, there are no complete models available to guide practitioners in setting priorities for creating effective BI solutions.5,10 Hospitals find it challenging to assess their existing problems and guide future development toward a smarter organization since there is a lack of a BI-based assessment framework, particularly for emerging markets like Vietnam. Therefore, the goal of this study is to create a BI-based framework to evaluate hospitals’ levels of smartness and to make managerial recommendations for hospital managers to increase their smartness based on the framework’s validity regarding multi-case assessment.
The remaining sections of the paper are structured as follows: section 2 presents the theoretical foundation, section 3 outlines the research method, section 4 summarizes the findings from the BI-based framework’s multi-case, section 5 suggests the management implications, and section 6 concludes the study.
Literature review
Smart levels of hospitals
According to Gomez-Sacristan et al., 19 a smart hospital is a technologically advanced, highly linked hospital that operates on tablets. Systems that employ IoT and mobile internet to connect people, documents, and organizations involved in the healthcare industry as well as access information, manage, and intelligently respond to patient requirements are examples of smart hospitals. 20 The term “smart hospital” is used in this paper to refer to a model of comprehensive healthcare that can best meet the needs of healthcare organizations, businesses, and patients, 21 using technology to access information, and connect people, 22 materials, and related organizations.20,23 This model of healthcare can also help to increase clinical effectiveness, lower costs, share responsibility, and improve safety. 19 Hospital ‘smartness’ is different from ‘readiness’ and is more important in a fast-changing environment. While ‘smartness’ refers to the capability of hospitals to utilize advanced technologies for better decision-making and efficiency, ‘readiness’ typically concerns the preparedness of an organization to adopt and implement new technologies.
A system’s or an organization’s level of smartness can be divided into five categories, according to Alter 24 : Not smart at all; Scripted execution; Formulaic adaptation; Creative adaptation; Unscripted or partially scripted invention. In this research, an assessment system for smart hospitals with 5 smart levels by using the methodology of Alter 24 is established.
Business intelligence (BI) as a cornerstone for smart hospitals
The factors of business intelligence
Factors of business intelligence.

The relationship between factors of business intelligence and smart hospital
Today, a variety of medical gadgets, 34 biomedical tools, and healthcare resources, including mobile devices with biometric sensors, are stored in numerous information systems in hospitals. 35 Dash et al. 35 claim that analyzing those data can reveal information on procedures, engineering, medicine, and other healthcare innovation areas. To optimize service quality while lowering costs, smart hospitals require electronic healthcare applications. 36 To increase their productivity and smartness, healthcare firms are attempting to adopt techniques like BI. 37 In fact, for effective hospital management, BI system improvement in hospitals should be a part of the plan of all departments. To track medical performance and enable quick and precise decision-making, it is crucial to develop BI for all levels of hospital management. 10 The development of smart hospitals needs data analysis, data visualization, and interface design based on user requirements. According to several studies,38,39 efficient BI applications have resulted in cost savings and greater productivity. In the case of BI application in healthcare, if successfully implemented, BI gives hospitals a practical method for growing and continuously enhancing their smartness. 10 This will also enable them to respond to changes rapidly, modify their plans, and, most importantly, build more advanced and smarter hospitals. As such, previous studies have shown a positive relationship between the factors of BI and the development of smart hospitals. In other words, building a smart hospital requires solid foundations of BI. Therefore, in this study, the assessment of the smart levels for hospitals will be made based on the factors of BI.
Previous assessment frameworks
Previous assessment frameworks for the healthcare industry.

Based on Table 2, recent frameworks for assessing healthcare systems have not focused on measuring the smart levels of hospitals, instead, they mostly assess the readiness or maturity of IT systems adoption. To the best of our knowledge, there is a shortage of frameworks for assessing smart levels of hospitals. As mentioned in the above review, the BI dimensions are the cornerstone of developing a smart hospital. Thus, it is necessary to develop a framework based on BI dimensions to assess the smart levels of hospitals. The smart framework plays an important role in suggesting recommendations for enhancing the smart level and improving the efficiency of hospitals in the era of IT advances.
Besides, this study’s BI-based framework also follows the FAIR principles. Specifically, the five factors of BI (Technology, Data and Process, Function, Diffusion, and Organization) are applied to assess the hospital’s smartness under FAIR principles. The two factors “Technology” and “Data and Process” are the critical measurements to assess hospitals’ smart levels, ensuring that they facilitate digital data to be findable, accessible, interoperable, and reusable. In the meantime, the other BI factors (Function, Diffusion, and Organization) are used to assess the smartness of hospitals applying FAIR data to improve their strategic and operational performance.
Research method
This research is based on Design Science methodology,
43
which focuses on the development of artifacts with the explicit intention of improving the functional performance of the artifact. The main purpose of this research is to develop a BI-based framework for assessing smart levels of hospitals. The method for this research is a combination of literature review, pilot test, and multi-case study. The research process is presented in Figure 1. Research process description.
In accordance with the research objective, the research method is composed of three phases. For the first phase, the systematic literature review is conducted to find out previous frameworks with the measurement scale for evaluating the smart levels in general, and for the smart hospital. These are analyzed to identify the gaps in the assessment scale for evaluating smart levels of hospitals. Then, an assessment scale for evaluating the smart levels of hospitals is proposed. A systematic literature review is a strategy that gathers prior studies that address the same subjects as the keywords. The major features and critical points of these studies are then identified through analysis to gain a general understanding of the state-of-the-art of subjects and research gaps. Based on this analysis of their contents, the ideas for a more thorough framework and assessment scale are derived. The process of the systematic literature review is based on PICOC44,45 and presented in Figure 2. Literature review process.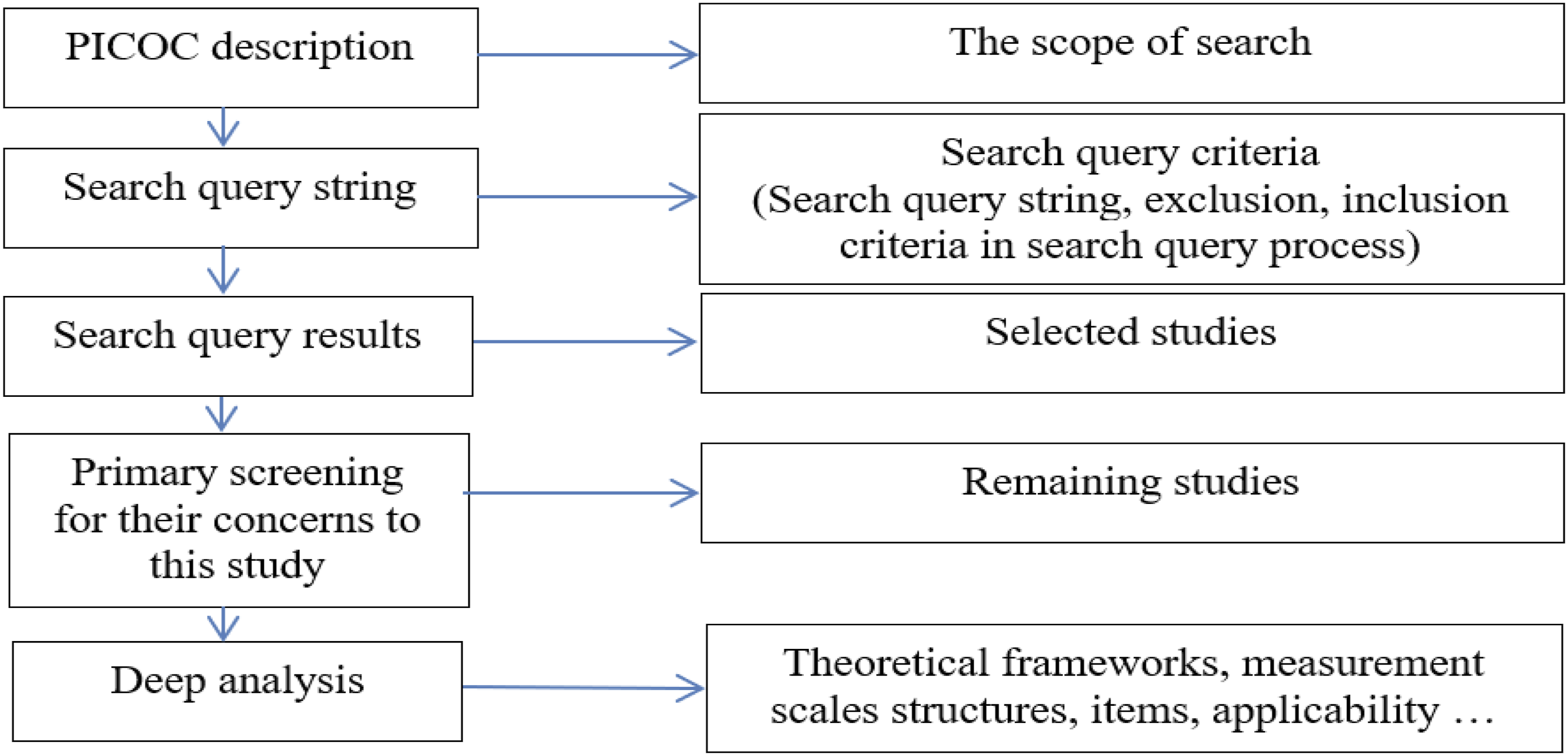
PICOC refers to Population, Intervention, Comparison, Outcome, and Context. PICOC description will help to define the scope of the search process. From the PICOC, the keywords for search are identified and the search query string is composed with Boolean connectors (AND, OR). Exclusion and inclusion criteria for article selection are also stated. Then, the search query process is started with the search query string and the criteria to select suitable articles. The selected articles are screened primarily for their contents associated with the objectives of this study; otherwise, they are deleted. The remaining articles are read and deeply analyzed to find out gaps to propose new study issues. In this study, the main topic is the smart hospital measurement scale.
The search query string is composed of the keywords such as (“Hospital management” OR “smart hospital management”) AND (“IT technologies” OR “information system” OR “business intelligence” OR “hospital information system”) AND (“Information system maturity” OR “information system success” OR “smartness measurement scale”), and related keywords. The search query process is limited to English articles having at least two keywords in the title, abstract, or keywords. The chosen period of articles is from 2005 to 2023 because the Forth Industrial Revolution is believed to start in 2005. The remaining articles are further analyzed for their objectives, theoretical frameworks, assessment scales, and applicability. The selected database is the SCOPUS/ISI, which is suitable for this topic because it is the integration of management and information field and requires a broad database with multiple disciplinary articles.
Then, the evaluation of the proposed assessment scale is conducted by a pilot test. To do so, a workshop is organized with related experts (hospital managers, IT department heads of the hospitals, and IT providers) who are decisive people to establish the IT system for the smart hospital implementation. In the workshop, these experts state different perspectives on the smart hospital (management, operation, and technology) and judge the suitability of the proposed scale. Based on the pilot test, a revision is made to get the final version of the assessment scale. Finally, the final assessment scale is tested for its applicability with a multi-case study, which is conducted in several hospitals. The details of these phases are presented in the next section.
Research results
BI-based framework for assessing the smart levels of hospitals
Based on Alter
24
and Gastaldi et al.
10
(Table 1), a framework for assessing the smart levels of hospitals is proposed. The assessment framework, which consists of five groups of BI factors divided into 27 elements, is built in accordance with five levels of smartness. To evaluate the proposed assessment scale, a workshop was organized to deeply discuss the structure, contents, and wordings of the scale. The criteria to select the participants included: (i) hospital managers having more than 10-year experience at hospitals implementing IT systems to become smart, (ii) IT providers with software provision of any kind for at least three different hospitals, and (iii) IT department heads from the hospitals having the selected managers. There were seven hospital managers, 8 IT providers, and 5 IT division heads joining the workshop. Two weeks before the workshop date, the participants received a letter presenting the assessment scale and the objective of the workshop. Some wording was suggested for adjustment. Finally, all participants came to the final version of the BI-based framework with the assessment scale (Appendix 1
Prior research in the healthcare industry has established the significance of the Hospital Information System (HIS) in overseeing organizational procedures to accomplish healthcare goals, specifically in relation to person-enabled healthcare, predictive analytics, workforce and governance, and interoperability, all of which have a significant influence on the health and wellness of patients and populations. However, different HIS structures and technology result in diverse approaches to achieving these goals. 46 In order to evaluate the maturity levels and provide guidance for developing HIS to raise them, the Healthcare Information and Management Systems Society (HIMSS) framework has been designed.47,48 Our proposed framework is intended to complement HIMSS by offering an additional method for evaluating the healthcare systems’ maturity using smartness levels. The framework centers on the hospitals’ capacity to utilize IT to automate their procedures. As a result, several components of our proposed framework are strongly related to HIMSS elements: Patient-enabled health is demonstrated by factors 2.1, 3.1, 3.2, 4.3, 4.5, and 4.6; predictive analytics is expressed by factors 1.1, 1.2, 1.3, 1.4, 2.1, 2.5, 2.7, 3.2, 4.6, 5.4, 5.5, 5.6, and 5.7; governance and workforce are covered by factors 3.1, 4.4, 4.5, and 4.6; and interoperability is related to factors 2.1, 2.5, 3.2, 5.4, and 5.7. In addition to the HIMSS components, our proposed framework also incorporates organizational aspects (such as budget and smart strategy) and technical variables (such as establishing technological standards, integration, report formats, and automation) to sustain the IT systems.
Applicability of the BI-based assessment framework for smart hospitals
Structure of the interview sample.

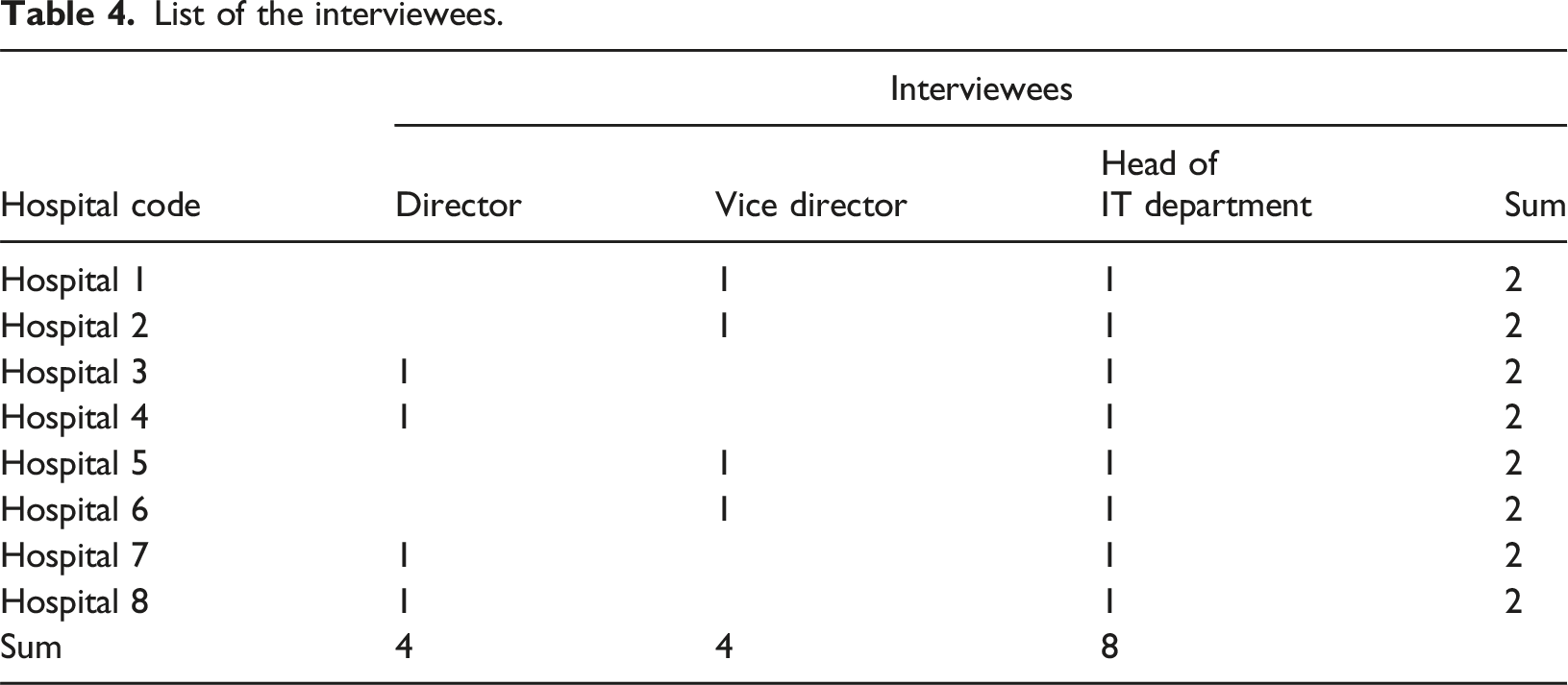
List of the interviewees.
Results of smart levels of hospitals in the sample.

As shown in Table 5, overall, the data-process dimension (4.2) is at the greatest level for the sample’s hospitals, while the technology dimension (3.9) is in second place. The development of Health Level 7 (HL7) in recent years for all hospitals and the current implementation of the Electronic Medical Record (EMR) at Grade 1 Hospitals may all be attributed to the Ministry of Health’s demands for the development of HIS. The general hospitals develop IT system technologies more than the specialized hospitals because they have more activities, processes, and complicated management with high workloads (4.1 vs. 3.1). As a result, the general hospitals have a greater level of technological dimension than the specialized ones. However, the technological dimension’s overall score (only 3.9) falls short of reaching a level higher than 4. This is because IT solution providers’ IT technology varies, and it takes longer for hospitals to deploy these IT systems. HIS, PACS, RIS, LIS, and EMR are among the IT applications used in hospitals where most IT solution providers in the city are not very proficient. They employ many technologies, and some of them implement the findings of their research and clinical trials in hospitals.
At the levels of function dimension (3.5) and diffusion dimension (3.6), these average values are the lowest. This demonstrates that management does not fully support hospital IT systems and that neither the management nor the medical staff makes full use of them. The function dimension is similarly at the lowest level for the foreign-invested hospital (hospital 7, 2.5), despite its IT system being practically completely completed. This finding demonstrates that IT technologies are not necessary for administrative tasks to be supported by hospital managers. At the function dimension, general hospitals score higher than specialized hospitals (3.5 vs. 3.1). This can be explained by the fact that general hospitals require more sophisticated, and high workload management activities than specialized hospitals. Because of this, the managers of these hospitals require more IT system support than the managers of specialized hospitals, and they also need more demanding IT systems to develop the function dimension. The specialized hospitals, therefore, have a higher degree of the data-process dimension (4.1 vs. 4.0). In a similar vein, general hospitals with more complicated operational procedures find it difficult to support all their employees and patients in the utilization of IT systems, and their operational procedures are not fully developed to support all hospital operations. Because of this, general hospitals’ diffusion level is lower than that of specialized hospitals (3.0 vs. 3.3). The specialized ones benefit from advantageous conditions for investing in IT systems and for training IT employees, users, and system administrators. They, therefore, have a better level of organization (3.9) than the average one (3.7). Besides, based on the analysis of the 5 factors of the assessment scale, the organization and diffusion factors are considered very important (high distance) to distinguish between the smart and non-smart groups. Therefore, improving these two factors can be helpful in improving the smartness of hospitals.
As shown in Table 5, Hospital 4 (public grade 1) and Hospital 8 (public grade 2) are the two hospitals with the greatest levels across all dimensions. It becomes clear from the interviews with the managers of these hospitals that they think more strategically than the other managers and focus on how to use IT systems to give them data and information for management. They are eager to pick up new skills and advance the capacity of IT workers and systems. This is proved by high levels at the function dimension (4.5 and 5.0) and results in high levels at the remaining dimensions. These findings support the notion that hospital administrators’ managerial outlooks play a key role in the growth of smartness in healthcare systems.
As shown in Figure 3, hospitals three and five need to improve only the diffusion and the organization dimension respectively to level 3, then, these hospitals will achieve the smart level at 3. Moreover, the improvement of these factors should be balanced between two groups: (1) technological group (technology, function, and data and process), and (2) social group (organization, and diffusion). Most of the hospitals in the sample focus too much on the technological group. So, they should rebalance the investment to focus more on the social group to improve the smart level in practice.
49
By using the framework with the assessment scale, hospitals can recognize their status and easily build a roadmap to improve their smart levels. These results prove the applicability of the framework in measuring hospitals’ smart levels. After discussing with hospitals’ managers in the sample, the framework was realized as a helpful tool to improve their digitalization process. Radar chart of smart levels of hospitals.
Discussions
The BI-based framework with an assessment scale to evaluate the smart levels of hospitals includes various cutting-edge features. According to the social-technical system theory, the development of smart hospitals should prioritize both the social (people utilizing and impacted by the system) and technical aspects. Our framework assesses how smart hospitals are based on those aspects and a five-level scale. Most previous studies have concentrated on IT applications (IoT, AI, telemedicine, etc.), whereas the assessment scale developed for this study also considers function, diffusion, and organization in addition to technology, data, and process. This makes it easier for the application of the information system (IS) to be accepted by the stakeholders and to provide organizational benefits. 30 The quality of the information and procedures in hospitals is not a major problem for the previous research, even though they are focused on ITs.29,30 Our framework, which includes a broad range of areas of IS success, 29 including the technology, the smart level, staff support, patient contacts, and efficacy, is expanded to incorporate the quality of information and processes to fill this gap. The assessment scale for smart levels is dynamic rather than static. As a result, the scale might be able to adapt to technological advancements. Additionally, the scale does not reflect the level of technology utilized to create the information system; rather, it assesses how smart the hospital is, which is a result of its internal information systems. Consequently, the smart scale works well and effectively over time.
Recommendations for key stakeholders to build smart hospital.
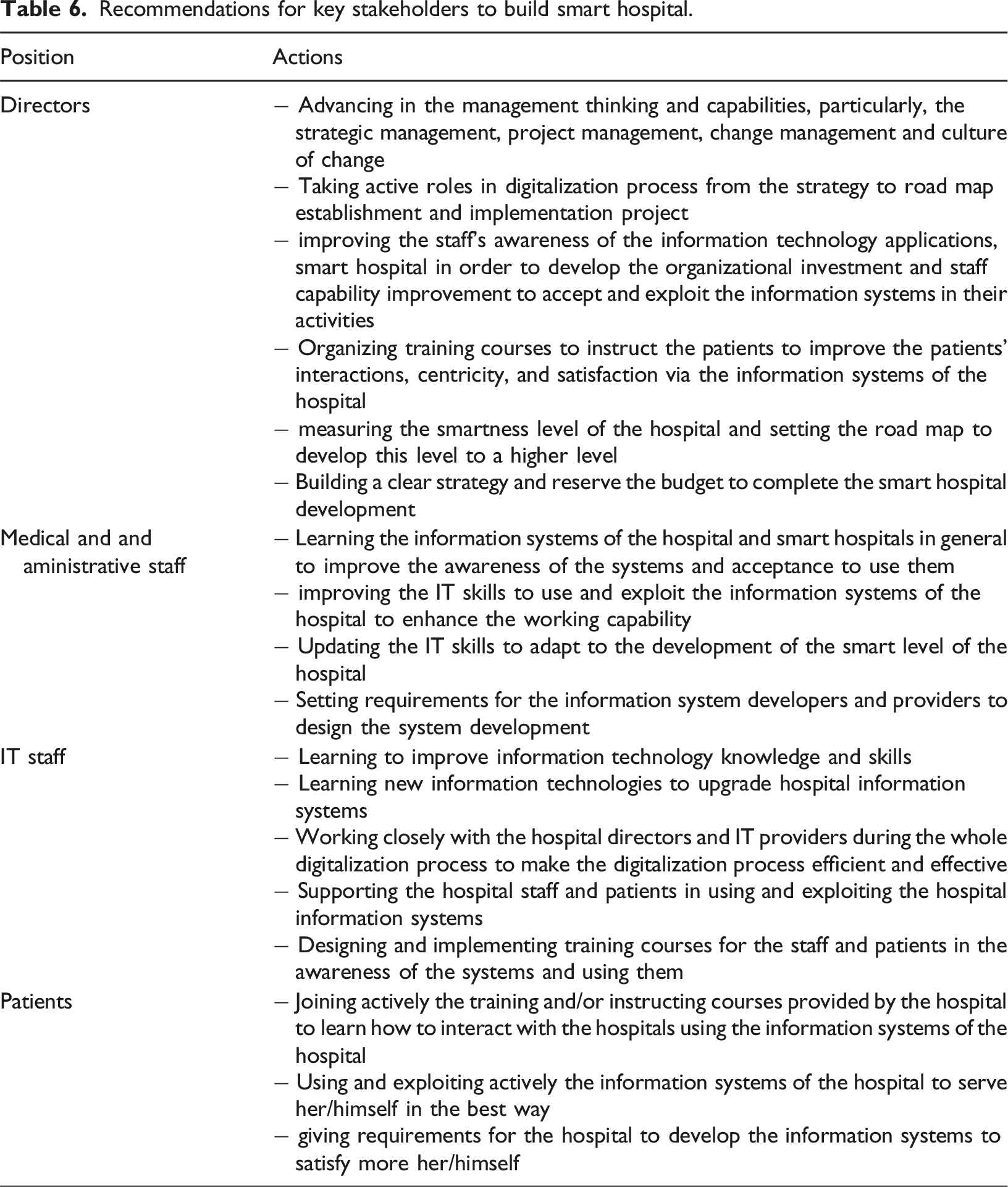
However, there are some implementation barriers for the above solutions, such as budget constraints, staff resistance, and technology integration issues. Therefore, the hospital managers should have an incremental strategy for improving the smartness of their hospitals. For example, based on BI-framework evaluation, the hospital should develop a roadmap for implementing its smartness. The roadmap should include short-term and long-term plan for improving their IT infrastructure, training users (internal and external), and integrating various functions and features of BI systems. Management supports and collaboration between IT staff and business functions should also be important elements for ensuring the success of the implementation plan.
Conclusions
The development of smart hospitals is urgently required to boost patient-centricity, medical quality, and hospital administration, as well as solve current problems of cost increase, waiting time for patients, and heavy workload for hospitals. Hospitals can implement different models to become smart hospitals. However, many hospitals place a greater emphasis on information technology applications than they do on hospital activity management. As a result, the development of the hospital information system has not adequately supported the management activities, and the hospital staff has not fully accepted and exploited it. Additionally, because there is a shortage of an assessment framework for evaluating smart levels, hospitals are unable to create a roadmap for developing their smartness effectively and systematically. The goal of this study is, therefore, to develop a BI-based framework for assessing the smart levels of hospitals to support them for improvement.
By systematic literature review, this study has found the gap in constructing the assessment scale for the evaluation of smart hospitals. Then, a comprehensive BI-based framework that includes five aspects of function, technology, diffusion, organization, and data and processes with 5 smart levels was proposed. The scale is assured of its validity and applicability by the pilot test and multiple-case studies. The results of a multiple-case study approve the applicability of the framework since it can explain the status quo of the hospitals. From then, some recommendations for hospitals are suggested to improve their smart levels.
However, there are some limitations of this research, such as the small sample size, a shortage of interviews with hospital suppliers and IT providers, etc. The sample collected in Vietnam has limited the possibility to generalize the results. The technological aspect of the framework may need to be revised and updated if there is a new technological revolution in the future. Further research can focus on the following topics: validating the assessment scale with a larger sample size; or studying the roles of hospital suppliers and IT providers to improve their smart levels. The proposed framework may be suitable for application in Vietnam and some countries with similar conditions. The further validation of the scale in other countries could also be a future research direction.
Footnotes
Acknowledgements
This research is funded by Vietnam National University - Ho Chi Minh City (VNU-HCM) under grant number DS 2022-20-08. We would like to thank Ho Chi Minh City University of Technology (HCMUT), VNU-HCM, and hospitals in the sample for the support of their time and facilities for this study.
Ethical approval
This study received ethical approval from the School of Medicine – Vietnam National University Ho Chi Minh City IRB (approval 8/QD-IRB-VN01.017) on Month 09, 2022.
Authors’ contributions
Conceptualization, M.C.T., P.L.L., Q.T.P. and V.T.N.; methodology, Q.T.P. and V.T.N.; validation, P.L.L., Q.T.P. and V.T.N.; formal analysis, M.C.T., P.L.L., Q.T.P. and V.T.N.; investigation, M.C.T., P.L.L., and V.T.N.; writing—original draft preparation, P.L.L. and V.T.N.; writing—review and editing, P.L.L., Q.T.P. and V.T.N.; supervision, M.C.T. All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is funded by VNU-HCM under grant number DS 2022-20-08
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Appendix
BI-based assessment framework for smart hospitals.
No.
Smart levels
Level 1: Not smart at all
Level 2: Scripted execution
Level 3: Formulaic adaptation
Level 4: Creative adaptation
Level 5: Unscripted or partially scripted invention
1.0 functions:
1.1
Goal definition
Hospital defines the goal for annual performance of more than 50% of activities based on the hospital-wide annual data
Hospital defines the goal for quarterly performance of more than 50% of activities based on the quarterly reports of each faculty/ department
Hospital defines the goal for monthly performance of more than 50% of activities based on the monthly reports of each faculty/ department
Hospital defines the goal for weekly performance of more than 50% of activities based on the weekly/daily reports of each faculty/ department
Hospital defines the goal and all activities the trend for daily performance of faculty/department based on the daily data of each process of each faculty/ department
1.2
Measurements
Hospital measures the annual performance by hand (not automatic) of some main activities based on hospital-wide data and annual report, such as: reception rate, medication quality, financial report, equipment usage, etc.
Hospital measures the quarterly performance by hand (not automatic) of some main activities based on quarterly data and report of faculty/ department, such as: reception rate, medication quality, financial report, equipment usage, etc.
Hospital measures the monthly performance automatically of some main activities based on monthly data and report of faculty/ department, such as: reception rate, service quality, customer satisfaction, equipment usage, human resources, balance sheet, investment and development, etc.
Hospital measures the weekly performance automatically of some main activities based on weekly/ daily data and report of each process of faculty/ department, such as: reception rate, service quality, customer satisfaction, equipment usage, human resources, balance sheet, investment and development, etc.
Hospital measures the daily performance and realizes the trends automatically/online of all activities based on daily data and report of each process of faculty/ department, such as: reception rate, service quality, customer, equipment usage, human resources, balance sheet, investment and development, etc.
1.3
Gap analysis
Every year, hospital by hand (not automatic) the distance between the real result and goal based on common data of the hospital and annual report on gap analysis
Every quarter, hospital analysis by hand (not automatic) the distance between the real result and goal based on data of each/ department and previous reports on gap analysis
Every month, hospital automatically the distance between the real result and goal based on data of each faculty/ department and previous month reports on gap analysis, and visualize the gap analysis results
Every week, hospital analysis automatically/ online the distance between the real result and goal based on data of each process of faculty/ department and previous weekly reports on gap analysis, and visualize the gap results
Hospital automatically/ online the distance between the real result and goal based on real-time data of each process of faculty/ department, and visualize the gap analysis results in an easy-to-understand form, and predict the trend on gap
1.4
Decision making
Hospital makes decision (without the support of IT) based on common data of the hospital and yearly updated reports
Hospital makes decision (without the support of IT) based on data of faculty/ department and quarterly-updated reports
Hospital makes decision based on OLAP report, data of each process/ event of each faculty/ department and monthly-updated reports
Hospital makes decision weekly based on OLAP report, data of each process/ event of each faculty/ department and daily/weekly-updated reports
Hospital makes decision based on real-time data of each process/ event of each faculty/ department and daily-updated reports/ trends
2.0 Technology:
2.1
Smart architecture
The hospital has full internal management processes, computerized, some processes of interaction with the external partners are computerized, some key processes are integrated online
2.2
Reports
Static reports (tables, tables, etc.) are made by hand and printed on paper
Static reports (including basic calculations, tables, tables, graphs, etc.) are done manually and are transferred in digital form
Static reports (including basic calculations, statistics, documents, tables, graphs, etc.), are performed automatically, always ready to be transferred and retrieved automatically
Dynamic reports (for different data sets, the report will change accordingly) with basic calculations, statistical analysis is done automatically and always ready to be transferred and retrieved automatically
Dynamic reports, structure, report content can be changed according to user needs automatically and be always ready to be transferred and retrieved automatically
2.3
User graphic interface
No interface
Have an interface at the local level
Hospital sets up website which can be accessed from personal computers
Hospital sets up website which can be accessed from personal computers or smartphones
Hospital sets up website which can be accessed from personal computers or smartphones
2.4
User profile
Hospital does not record user profiles in digital form
Hospital records user profiles as files in the local computers
Hospital records user profiles in digital form in centralized database
Hospital records user records in digital form and has user classifications (according to users, purposes of use, commonly used functions, etc.)
Hospital builds IT tools to identify and support external users depending on the users, purposes of use, commonly used functions, etc. to increase convenience and reduce system penetration time
2.5
Technology integration
Hospital has not yet applied smart solution tools (technology 4.0) to perform work and interact with the outsiders. All are done by hand
Hospital has not yet applied smart solution tools (technology 4.0) to perform work and interact with the outsiders. All are done manually. Data from internal medical devices are stored internally and cannot be transferred. No data received from external medical devices
The hospital adopts smart solutions tools (technology 4.0 such as IoT, cloud, etc.) to perform part of the internal work and some interaction with the outsiders
Medical data from internal medical devices is integrated, circulated internally and transmitted to external partners
Data from external medical devices are received, integrated and circulated inside the hospitalHospital adopts smart solutions tools (technology 4.0 such as IoT, cloud computing, big data, etc.) to carry out all internal work and all external interactions. Medical data from internal medical devices is integrated, circulated internally and transmitted to external partners
Data from external medical devices are received, integrated and circulated inside the hospitalHospital adopts new smart solutions tools (integrating 4.0 IoT technologies, big data, AI, etc.) to carry out all the work and interactions with the outside. The new smart solution tools are fully integrated with existing smart solutions tools. Medical data from internal medical devices is integrated, circulated internally and transmitted to external partners
Data from external medical devices is received, integrated and circulated inside the hospital
2.6
Standards
Hospital has not applied IT, so there is no standard for smart solution tools to perform work and interact with the outsiders
Hospital applies IT at a simple level, and does not yet apply standards for smart solution tools to perform work and interact with the outsiders
Hospital adopts the standard for a few smart solution tools to perform work and interact with the outsiders
Hospital applies the standard for all smart solution tools to perform work and interact with the outsiders
Hospital adopts a new standard for a number of new smart solution tools to perform work and interact with the outsiders
2.7
Data update
Data are updated at the hospital level and are updated annually
Data are updated at departmental level and updated quarterly
Data are updated at departmental level and updated monthly
Data are updated at process level and updated weekly
Data are updated at the process level and updated online in real time
3.0 Diffusion :
3.1
Accessing users
Hospital IT system does not support any tool for doctors, nurses, and administrative staff to work. No mean for patients, customers, vendors to contact with the hospital
Hospital IT system supports tools for less than 50% of doctors, nurses, and administrative staff to work. Tools for less than 25% of patients, customers, vendors to contact with the hospital
Hospital IT system supports tools for 50%-70% of doctors, nurses, and administrative staff to work. Tools for 25%-50% of patients, customers, vendors to contact with the hospital
Hospital IT system supports tools for 70%-80% of doctors, nurses, and administrative staff to work. Tools for 50%-75% of patients, customers, vendors to contact with the hospital
Hospital IT system supports tools for more than 80% of doctors, nurses, and administrative staff to work. Tools for more than 75% of patients, customers, vendors to contact with the hospital
3.2
Process coverage
Hospital IT system does not support management functions (goal definition, measurement, gap analysis, decision making) and business processes/ medication processes of faculty/ department
Hospital IT system supports some of management functions (goal definition, measurement, gap analysis, decision making) and business processes/ medication processes of several faculties/ departments. IT system supports interaction functions with customers, patients, such as: medication registration, meeting schedule, personal profile. Users’ data are stored in file format
Hospital IT system supports some of management functions (goal definition, measurement, gap analysis, decision making) and business processes/ medication processes of several faculties/ departments. IT system supports all online interaction functions with patients, customers, and vendors. Users’ data and trace files are stored in database
Hospital IT system supports all of management functions (goal definition, measurement, gap analysis, decision making) and all business processes/ medication processes of all faculties/ departments. IT system supports all online interaction functions automatically with patients, customers, and vendors. Users’ data and trace files are stored in an integrated database
Hospital IT system supports all of management functions (goal definition, measurement, gap analysis, decision making) and all business processes/ medication processes of all faculties/ departments. IT system supports all online interaction functions automatically in the real-time manner with patients, customers, and vendors. Users’ data and trace files are stored in an integrated database
4.0 Organization :
4.1
Smart strategy
Hospital does not focus on smart hospital strategy development
Hospital develops strategies for each department in the smart direction
Smart strategies of all faculties and departments are integrated into the general strategy development of the hospital
Smart strategies guide change management across departments and hospital-wide
Hospital has the ability to creatively analyse conditions or information to refine smart strategies
4.2
Smart budget
Hospital has no funds for smart development
Hospital uses available guidelines to build a budget for smart development
Hospital uses existing facilities to increase funding for smart development
Hospital has the ability to creatively analyse conditions or information to increase funding for smart development
Hospital has the ability to come up with new ways to increase funding for smart development
4.3
Organizational coverage
Hospital has no intrinsic resources for smart development
Hospital has some intrinsic resources for its development but these resources are not specifically dedicated to smart development
Hospital has a number of specialized intrinsic resources for smart development
Hospital forms a specialized unit in charge of smart development and leads the changes towards smartness
The specialized unit in charge of smart development for hospital is capable of self-analysing and assessing the development of the technology, patient and customer needs to propose changes in management, operation and provision of smart health care services
4.4
IT staff capabilities
No IT staff
Hospital IT staff only has basic IT technical capacity, not yet equipped to deploy 4.0 technologies for smart hospital
Hospital IT staff is capable of operating and maintaining 4.0 technologies and has applied some 4.0 technologies to meet the needs of smart hospital
Hospital IT staff is qualified to self-deploy, operate, and maintain 4.0 technologies for smart hospital to meet the hospital’s requirements
Hospital IT staff has the ability to identify new needs as well as build and deploy 4.0 technology solutions to meet needs for smart hospital
4.5
User capabilities
Heads of Departments are not capable of using smart tools and solutions to do work and create reports.
Managers and doctors are not capable of using smart tools and solutions to do the job and generate reports. Patients, customers, and partners of the hospital are not capable of using smart tools and solutions to interact with the hospitalHeads of Departments are only capable of using basic smart tools and solutions to perform tasks and create static reports that only administrators and doctors can use. Simple smart tools and solutions are used to do the job and generate static reports patients, customers, and partners of the hospital are only capable of using simple smart tools and solutions to interact with the hospital
Heads of Departments have the ability to use more complex smart tools and solutions to do most of the work, create and manage dynamic reports. Competent management staff and doctors use more complex smart tools and solutions to do most of the work, create and manage dynamic reports. Patient, customer, and partner are capable of using complex smart tools and solutions to interact with the hospital
Heads of Departments have the ability to use more complex smart tools and solutions to perform the entire job, create and manage dynamic reports, and competent management staff and doctors can use more complex smart tools and solutions to do all the work, create and manage dynamic reports. Patients, customers, partners have the ability to use complex smart tools and solutions to fully interact with the hospital
Heads of Departments and Faculty have the competence to use the tools and solutions of Technology 4.0 to analyse work outcomes and identify necessary improvements to perform work better. Management staff and doctors are competent to use the tools and solutions of technology 4.0 to analyse the results of the work, identify the necessary improvements to perform the work better. Patients, clients, and partners are able to identify the new requirements that hospitals need to meet with the support of tools and smart solutions
4.6
Competence improvement
Hospital does not have a program to improve the IT capacity of its staff
Hospital has a training program to improve IT capacity for staff to use some basic software and hospital’s IT system
Hospital has a training program to improve IT capacity for staff to use some professional software for data processing and use the hospital IT system. The hospital has drafted a manual instruction for patients and external partners to interact with the hospital through the IT system
Hospital has a training program to improve IT capacity for staff to use some professional software. Basic analysis is supported by professional data processing software, and 4.0 technology tools and system.
The hospital has identified the requirements of patients and partners to adjust the IT system and makes them easier to interact with the hospitalHospital has a training program to improve IT capacity for staff to use professional software. In-depth analysis is supported by professional data processing software as well as 4.0 tools and systems. The hospital has identified the requirements of patients and partners to adjust the IT system and makes them easier to interact with the hospital
4.7
Partner coordination
Hospital does not have mechanisms to coordinate and cooperate with tool and solution providers for smart development
Hospital coordinates with suppliers to build smart-oriented workflows, process, database, etc.
Hospital coordinates with suppliers to deploy smart tools and solutions
Hospital works with suppliers to improve smart tools and solutions and solve problems arising during the use of these tools and solutions
Hospital coordinates with suppliers to analyse and improve the performance of the IT system and upgrades the IT system capacity to meet the new requirements
5.0 Data and process:
5.1
Process capturing
Hospital does not conduct any activity for capturing and standardizing processes
Hospital uses available instructions for presenting the common processes
Hospital uses available forms and private rules for capturing and standardizing important processes
Hospital creatively uses available conditions and information for capturing and standardizing medication processes and operation processes
Hospital can create new processes for supporting creative solutions. Hospital captures and standardizes medication processes and operation processes based on new technologies
5.2
Process performance analysis
Hospital does not conduct any activity for analysing the performance of current processes
Hospital uses available instructions and basic tools for analysing the performance of repetitive processes
Hospital uses available supports and specific analysis tools for analysing the performance of important processes
Hospital can take advantages of new technologies and use information creatively for analysing the performance of medication processes
Hospital can create new and smart solutions based on new technologies to support for analysing the performance of medication processes
5.3
Process improvement
Hospital does not conduct any activity for improving the performance of current processes
Hospital uses process analysis results for improving the performance of repetitive processes
Hospital uses process analysis results and internal networks for continuously improving the performance of important processes and implementing the process change
Hospital can take advantages of new technologies and use information creatively for improving the performance of medication and operation processes and implementing the change for a better performance
Hospital can create new and smart solutions based on new technologies to support for analysing and improving the performance of medication and operation processes and implementing the change for a better performance
5.4
Data accumulation
Hospital does not integrate database of various hospital information systems automatically
Hospital integrates some databases of hospital information systems based on available guidelines
Hospital integrates various databases of hospital information systems on the cloud platform based on available conditions/ systems
Hospital integrates various databases of information systems on the cloud platform creatively (based on specific conditions/ systems)
Hospital integrates various databases of information systems in real-time manner on the cloud platform using modern technologies (IoT, cloud computing, wearable devices, etc.)
5.5
Data exploration
Hospital does not have any reporting system based on information system automatically
Hospital exploits data and reports generated from information systems based on available guidelines
Hospital exploits online data and reports generated from information systems based on available conditions/ systems
Hospital exploits online data and reports generated from hospital information systems creatively (based on specific conditions/ systems)
Hospital exploits real-time data and reports generated from smart hospital information systems on the cloud platform using modern technologies (BI, Data mining, AI, KMS, etc.)
5.6
Data quality
Hospital does not have any control system for providing the quality of input and output data of the information system
Hospital monitors and controls traditionally the quality of input and output data of faculties/ departments based on quarterly updated data
Hospital monitors and controls online the quality of input and output data of all faculties/ departments automatically (based on statistics)
Hospital monitors and controls online the quality of input and output data of all faculties/ departments automatically (based on statistics). Using data analysis tools for controlling data quality
Hospital monitors and controls in real-time manner the quality of input and output data of all faculties/ departments automatically (based on statistics). Using data analysis tools, such as: visualization, simulation, forecasting, etc., for realizing and analysing the causes of data trend and distribution
5.7
Functional integration
Hospital does not integrate operation processes and data for supporting the collaborative work between faculties/ departments
Hospital integrates business processes and data for supporting the collaborative work between internal medication group, quality group, and administrative group
Hospital integrates business processes and data for supporting the online collaborative work between internal medication group, quality group, and administrative group, and between them (basic ERP system)
Hospital fully integrates business processes and data for supporting the online collaborative work between internal medication group, quality group, and administrative group, and between them (full ERP system)
Hospital fully integrates business processes and data in real-time manner for supporting the online collaborative work between internal medication group, quality group, and administrative group, and between them (full ERP system integrated with outside partners in real-time manner)