
Abstract
Introduction: Information and Communication Technology (ICT) with emphasis on Electronic Health Records (EHR) is growing steadily in most developing countries including Ghana. This is considered the impetus for achieving quality service delivery. The study is intended to evaluate the implementation and utilization of health information systems in health care delivery. Methodology: A descriptive cross-sectional study was conducted to achieve the study objective. The target population included health professionals from diverse settings who interact with Electronic Health Records, the District Health Information and Management System (DHIMS-2). The data collection approach relied on close and open-ended questionnaires, observations, and focus group discussions. The proportionate stratified and simple random sampling techniques were used to obtain a representative group of healthcare professionals. Descriptive statistics was used to analyze user satisfaction, benefits, and challenges of EHR/DHIMS-2. Moreover, Pearson correlation and linear regression analysis were used to analyze the Technology Acceptance Model for the end users. Results: The study revealed that perceived ease of use and usefulness could be significantly predicted to influence end-users’ attitude towards technology adoption. The results show significant association between the combined effects of attitude and usefulness on acceptance. Conclusion: Implementing EHR and DHIMS-2 within the confines of developing nations is recommended.
Keywords
Introduction
The application of ICT is not a new phenomenon across many healthcare settings. ICTs with emphasis on Electronic Health Records (EHR) represent the bedrock of service provision in the prevention, diagnosis, and management of various disease conditions in the healthcare industry. An Electronic Health Record is a systemized collection of patient information in a digitized format. With the needed support in EHR applications through the right policy framework; institutions, resources, and stakeholders will recognize EHR resources as enablers for end-users to improve quality service delivery.1,2
EHR optimizes the overall quality of care, reduces healthcare and administrative costs, and enhance the privacy, confidentiality, and security of health information. 3 Notwithstanding, EHR also enables patients to better manage their conditions and encourages information exchange among clinicians for effective and efficient health care delivery. 4 A health information system (HIS) is regarded as an “integrated effort to collect, process, report and use health information and knowledge to influence policy making, programmed action and research”. 5 Computerized information systems especially EHR are anticipated to improve legibility, lessen healthcare medical misadventures, and shrink costs in order to achieve robust healthcare. 6
Nonetheless, its implementation and the overall integration of such a feat are overwhelmed with many challenges. The flaws encompass issues pertaining to the inherent characteristics and health information system’s structure to the concerns arising from HIS and communication technology and its implementers. 7
By conducting evaluation studies, we assess quality, acceptance, and usefulness, create insight for improvement, and discriminate between different options, and refine our future development strategies.
In the quest to roll out the National e-Health Strategy, the policy framework focuses on four main issues which include: a regulatory framework for health and information management, capacity building for wider application for e-health solutions in the health sector, increased coverage and bridging the equity gap in utilizing ICT and its applications and finally achieving paperless based records in decision making. 8 The policy statement reflects the nation’s total commitment to transforming Ghana into an information-rich knowledge-based society and economy to ensure that Ghana and its people fully participate in the information age and enjoy the social, cultural, and economic benefits of the emerging information revolution.
Context of the study
Health Informatics in Ghana is at the infant stage and the Ghana Health Service (GHS) report shows that it is incumbent to restructure how data is captured to meeting patients’ needs and other consumers. 9 Healthcare regulators including the Ministry of Health and Ghana Health Service bemoaned having separate, disparate, and redundant data flows and therefore the need to have this addressed. According to GHS, 10 obtaining routine service data (useful data) from all health facilities across Ghana has been the most single immediate challenge of the health sector and this has led to delays in information dissemination regarding healthcare planning and health financing posing a challenge to health administrators. This culminates in a lack of strong interventions by the Ghana Health Service in attending to emergencies, critical situations, outbreaks, and making the necessary budget.
The magnitude of the challenges informed the conduction of evaluation studies into the health information system implementation and utilization in the healthcare delivery as no research studies have been carried out in this arena. This it is believed could influence a nationwide adoption and implementation of such projects considering the fact that one could learn from facilities that have fully implemented EHR systems. To achieve the objective of this study, the study seeks to address the following research questions;
Literature review
In response to the current demand for ICT in care delivery, there has been an introduction of a nationwide electronic health project involving District Health Information and Management Systems (DHIMS-2). 11 Even though the Ghana e-health strategy has been launched, its adoption and implementation are faced with inherent challenges. A scan through e-health projects in Ghana revealed about 23 projects at different stages of implementation. 12
Examples of health information systems and how they are used to deliver healthcare
Electronic health Record (EHR)
“ It is an automated system for keeping patients’ health records that is consistent with nationally accepted interoperability standards which are formed, controlled, and thoroughly assessed by certified clinicians and other healthcare professionals in multiple healthcare settings”. 13 Electronic Health Records also facilitate and improve clinicians’ task and reduce the time spent on patients, minimize the disappointments associated with clumsy manual tracking and transferal of prevailing segmented records.
The district Health Information and Management Systems (DHIMS-2)
DHIMS-2 which is established on District Health Information System (DHIS-2) framework is a free open-source software being utilized around the globe. The system is intended to collect, transcribe, transmit, and compile data where information (in the form of text and statistics) is captured by the system. The utopian usability goals for health information system evaluation focus on the following usability principles; learnability, efficiency, rate of errors, memorability, and user satisfaction. 14
The benefits of using Health Information systems
The use of computerized information systems guarantees and offers numerous benefits to healthcare practitioners in the care industry. 15 These benefits encompass issues related to efficiency, accuracy, quality care, information availability, and management care.
Efficiency
Health information systems can increase the facility’s productivity as well as activities that improve efficiency and time consciousness thereby enhancing quality healthcare delivery.
Accuracy
Alerting systems and reminders of clinical decision support systems reduce medication errors and other allergic drug reactions are easily flagged off for improved safe use and drug administration thereby enhancing monitoring of quality service delivery.
Quality of care
Computerized health information system improves user satisfaction, and patient throughput, and promotes better health outcomes. Ease of use concerning the system enhances staff skills especially clinicians as patients’ waiting time improve considerably.
Availability of information
Health information systems make information readily accessible and also provide appropriate as well as comprehensive information by service providers in the care process. Electronic Health Record makes clinical information readily available and accessible in a more comprehensible format.
Management of care
Utilizing computerized systems in the health sector enhances data quality through payments and billings for patients, promoting medical education, ICT skills, and policy decisions, and supporting clinical health services research. 16
The barriers facing the implementation of Health Information systems
Health information system implementation is normally fraught with challenges even though implementing ICT applications offers numerous benefits to the healthcare industry. 17
System failure
Systems shut down and power fluctuations during the care process affects the entire health information usage, as patients’ records and other information are lost, it also affect patients’ waiting time.
Cost
The cost involved in implementing Electronic Health Records may not be the same in terms of the prevailing environmental conditions and performance. Moreover, the additional costs required for maintenance and system sustainability may obstruct its full integration and functionality.
Confidentiality, security, and privacy concerns
This is regarded as a daunting barrier that undermines full functionality pertaining to the implemented systems. Issues of accountability regarding health information systems utilization and data security should provide concurrency control services that promote user and vendor satisfaction. Patients’ information protection and confidentiality also raise some questions. 17 Data security is very essential and failure to protect the system compromises integration processes.
Inefficiency
Inefficiency is also a predicting factor that affects the smooth running of the health information system adoption and acceptance by healthcare professionals. There is no proper interoperability that supports health information systems due to a lack of cost-effective ICT applications usage. 18
Changes in work process
Clinicians and other healthcare professionals will have to adapt to changes in the work environment and this may affect the organizational structure and the system functionality. The changes in the work process will affect traditional routine practice among healthcare providers. 18
Acceptance of Health Information systems
It is established that issues concerning the success or failure of information systems implementations generally hinge on user acceptance.
19
Figure 1 shows the Technology Acceptance Model, a theory that predicts user acceptance of information system. The technology acceptance model (TAM). Source: Adapted from the theory of technology acceptance model (TAM).
20
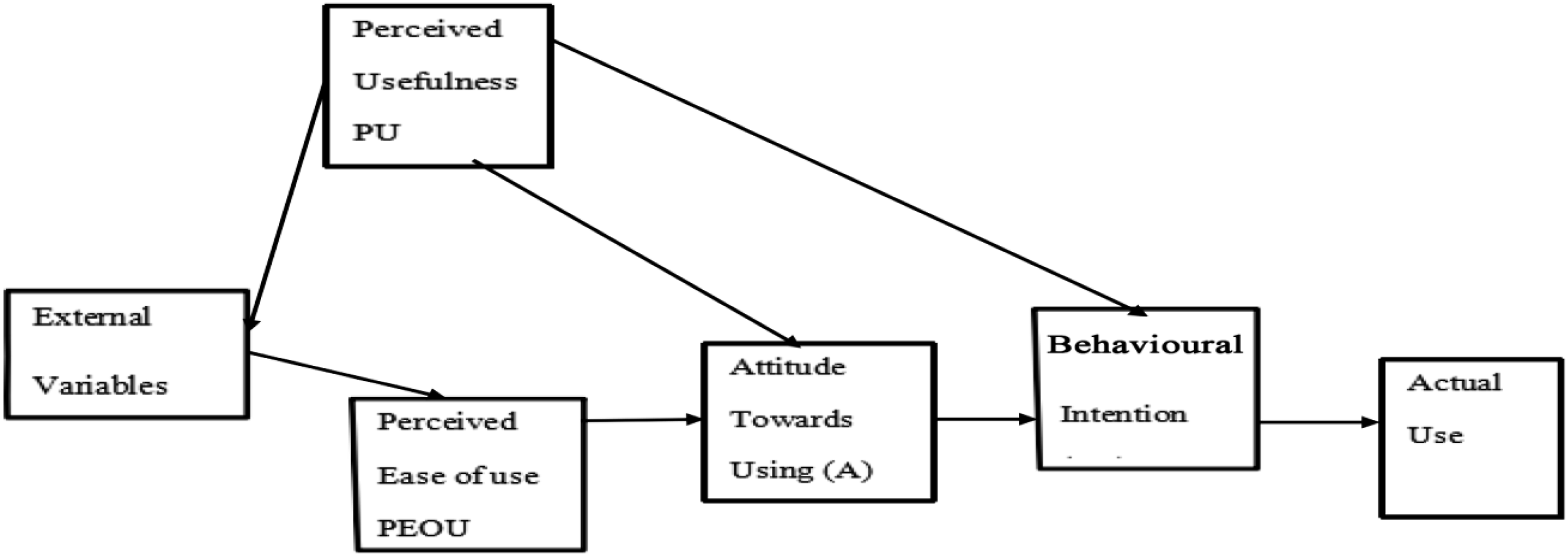
Perceived ease of use (PEOU)
Perceived Usefulness and PEOU could make predictions about IT systems users’ acceptance behaviors and the lack of acceptance relating to health information technology hinges largely on the nature or inherent characteristics pertaining to the clinician. 21
Behavioral beliefs/intention
Is a prevailing attitude influencing one’s behavior that produces the outcome or behavior in question and normative beliefs refer to the perceived behavioral norms we associate with behavior. 22 The Theory of Reasoned Action is also a theory that describes human behavior under the control of voluntary action from the social psychology context. 23 This theory has largely been applied and implemented effectively in analyzing and explaining one’s actions notably in a variety of ways. Nutbeam and Harris asserted that workers use technology because it has been incorporated into their work as an enabler that enhances work performance and would otherwise not use it. 24 Nutbeam and Harris defined Perceived Usefulness (PU) as the acceptance of a system by a user with the intent of improving job performance. 24 The construct (TAM) was modeled to compare usability and acceptance of the implemented system from the end users’ perspectives.
Methodology
Study design
A descriptive cross-sectional study was conducted to achieve the research objectives. This research design was suitable for obtaining relevant information and describing and identifying factors in relation to the use of health information systems including EHR/DHIMS-2. The research was purely qualitative and quantitative (mixed approach). The amalgamation of the mixed method approach facilitates triangulation with a vivid account of the problem statement, hence strengthens the study’s conclusion. 25 The qualitative research analysis really focused on the thematic areas of the study. The study realizes this charge, by discussing some relevant issues relating to the central thesis. Narrative analysis was used to analyze content from various sources such as interviews, and observations from the survey.
Target population
The target population of interest was a diverse group of healthcare professionals and users of the implemented EHR and DHIMS-2.
Inclusion criteria
i. Participants with more than 6 months of experience with the utilization of both EHR/DHIMS-2 in the district.
The exclusion criteria
i. Participants who had not spent more than 6 months before the data collection.
Sampling size and sampling techniques
The distribution of respondents by department.
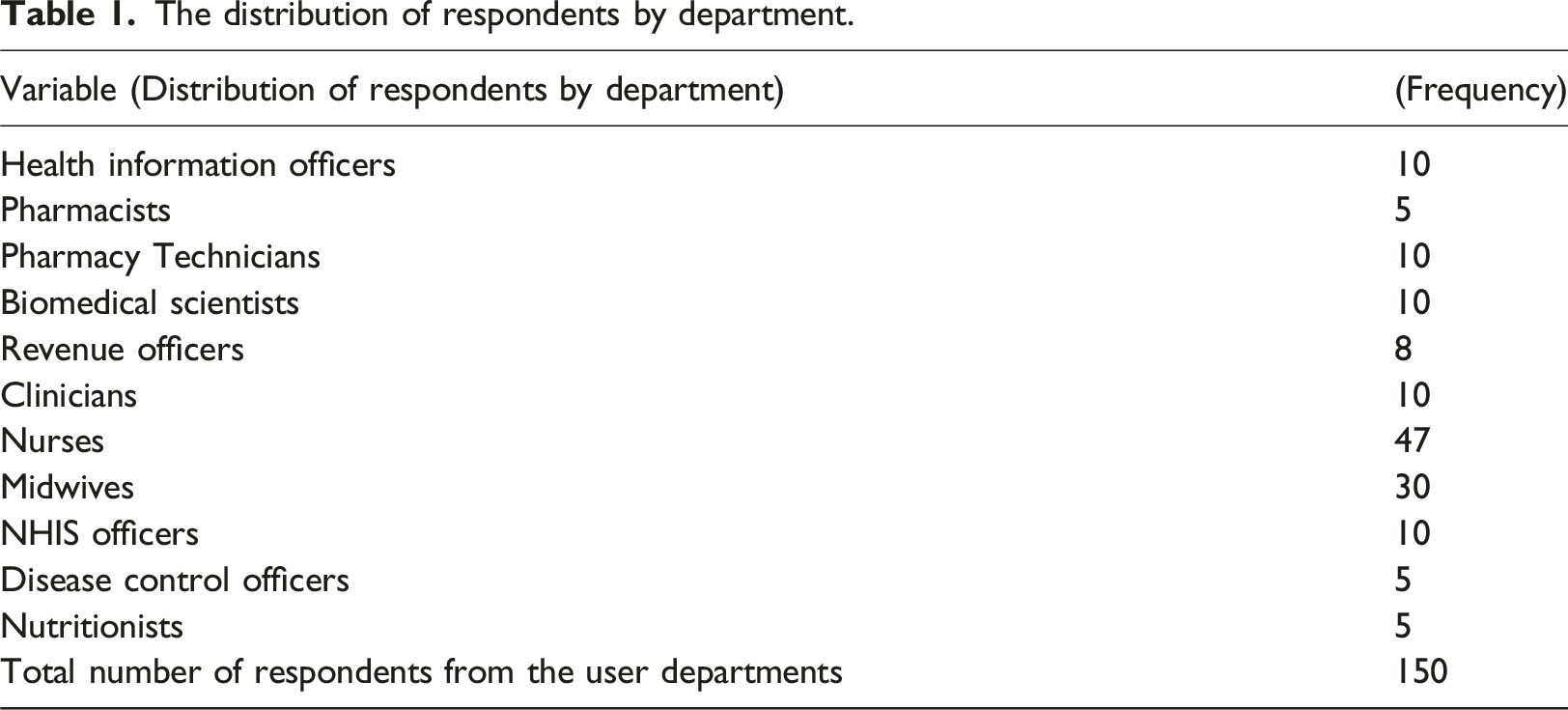
Stratification was used as one of the probability methods because it is more efficient than other methods when a population has certain groups with the same characteristics but these characteristics differ among the groups. The employees were stratified as much as possible due to the shift system in the various user departments.
Based on this, a sample size (n) of 150 was calculated with a 95% confidence level using mathematical formulas suggested by. 26
as;
The sample size was distributed among the district’s healthcare facilities, which were further apportioned to each sampled respondent, as shown in Table 1.
Pre-testing the instrument
Fifteen questions were pre-tested in the IT department and the District Health Insurance office for end-users and administrators of the system to check the validity and standard of the questions. Therefore, all concerns raised during the pre-test were reviewed by experts in health information systems management, who discussed queries with the researchers and the necessary corrections were made for the final set of questions.
Data collection tools and techniques
Self-administered questionnaires (open-ended), interviews and focus group discussion instruments contained scales to measure the various constructs depicted in the study variables. The five-point Likert scale was used to quantify and measure the different views of respondents by assigning values to arbitrary assessment which includes; strongly disagree, disagree, neutral, agree, and strongly agree. A descriptive study being qualitative was carried out using focused group discussions (FGDs). A total of 4 focus group interactions were held. The selected participants were twenty (20) in number per five groups’ representations. The content analysis and the outcome of the discussion were coded.
The interview guide focused on the system administrators of the implemented health information system. It sought views from the IT department and the facility heads in the district.
Data analysis
Statistical techniques were used in this research for the data analysis. Data was compiled, sorted, edited, and coded. Application software such as Microsoft Excel and Statistical Package for Social Science (SPSS) version 18 was used to analyze the questionnaire. Analysis of linear regression to establish the difference across the variables under the study was also measured. Pearson’s correlation was used to establish the relationship between perceived ease of use, perceived usefulness, and attitude toward using and actual system usage. A multiple regression analysis was then conducted to determine the contribution of perceived ease of use, perceived usefulness, and attitude toward using on the dependent variable (actual system usage).
Ethical consideration
Formal permission was sought from the heads of District Health Directorate and the hospital management team. The in-charges in the various units served as contact persons to help the researchers to identify the individuals. Verbal consent was sought from the respondents before the questionnaires were administered.
Results
The results and discussion of study findings are presented with a descriptive analysis of the sample using cross-tabulations. Pearson’s correlation and regression analysis were also used to perform the inferential analysis of the data.
Demographic Characteristics of Respondents.
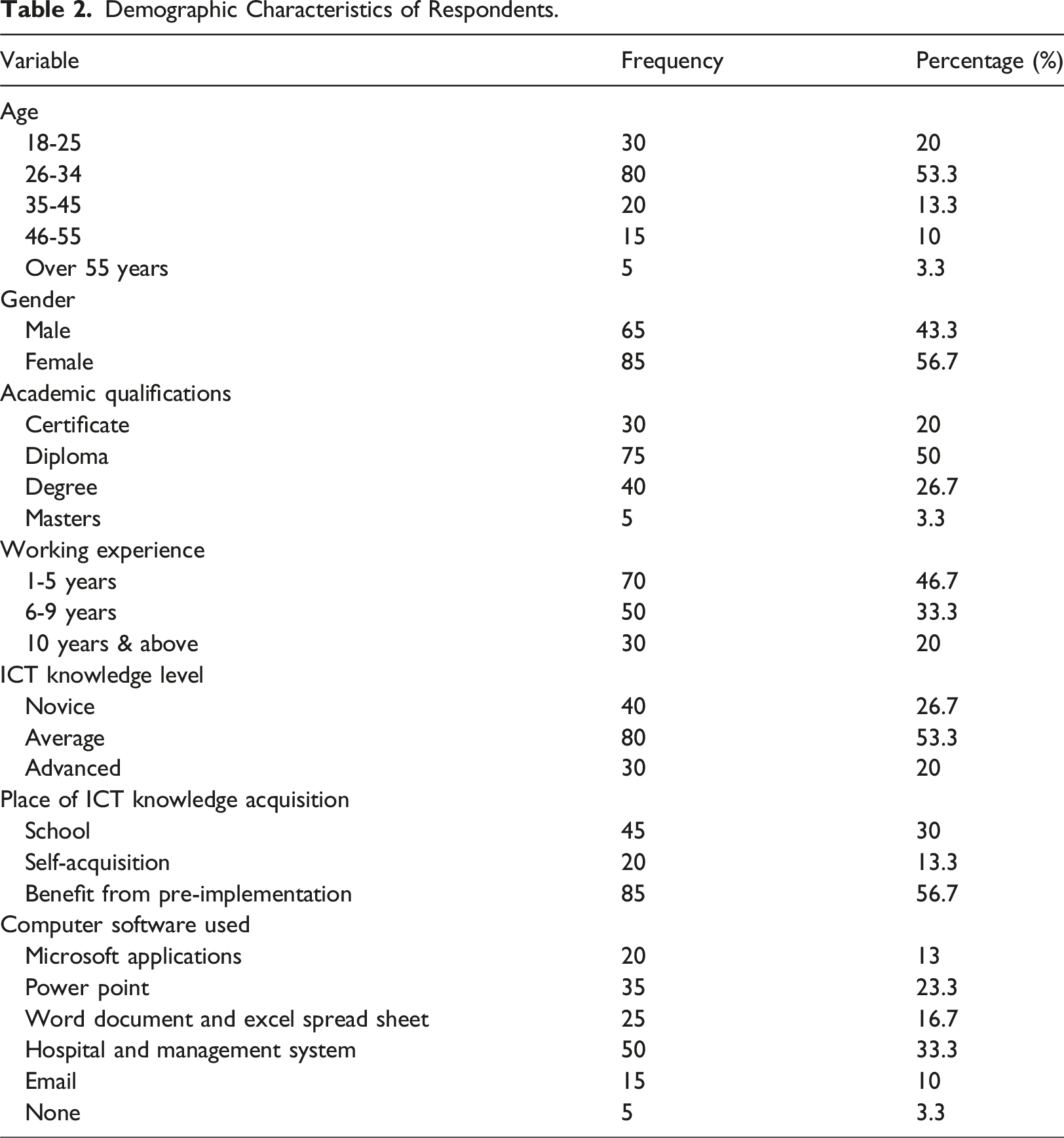
The table represents the number of respondents and their level of academic qualifications. The analysis indicates that 75 (50.0%) represented the highest percentage with a Diploma certificate of 75 (50.0%), followed by Bachelor’s Degree holders 40 (26.7%) and 30 (20%) with Certificates in health-related courses. Moreover, 5 (3.3%) are the least with a Master’s Degree qualification. These results indicate that the majority of the healthcare professionals in the selected hospitals have a minimum of a diploma and a first degree respectively.
The majority of the respondents 70 (44.6%) had worked for a period spanning from one to 5 years whereas 50 (33.3%) had worked for more than 6 years followed by 30 (20.0%) with more than ten years of work experience as shown in the Table 2.
On the respondents’ IT knowledge and mode of knowledge acquisition, the majority of the users 53.3% ( 80) rated their Information Technology (IT) literacy level as average, (40) 26.7% as novice, and 30 (20.0%) with appreciable level of IT knowledge (Advanced). Staff representing 45 (30%) acquired their IT knowledge through formal training from their respective training schools whereas others 20 (13.3%) confidently pointed out personal effort (self-acquisition). Again, a significant proportion 85 (56.7%) had also benefited from the pre-implementation training even though some felt the training was inadequate.
The Software Applications in which the respondents claimed to have acquired their training included the following; Microsoft Access (13.3%), PowerPoint (23.3%), Word and Excel (16.7%), 33.3%, 10% and 3.3% through Hospital Administration and Management Systems (HAMS)/DHIMS solution, email and non-applicable responses respectively.
Some of the respondent’s definition of EHR is given below: ➢ Electronic Health Records are defined as the means of recording patients’ information with the help of a computer. ➢ It is also defined as being the system that has replaced the paper-based/manual way of record keeping. ➢ It is a system of keeping hospital health information so that patients’ data can be easily traced with the aid of a computer.
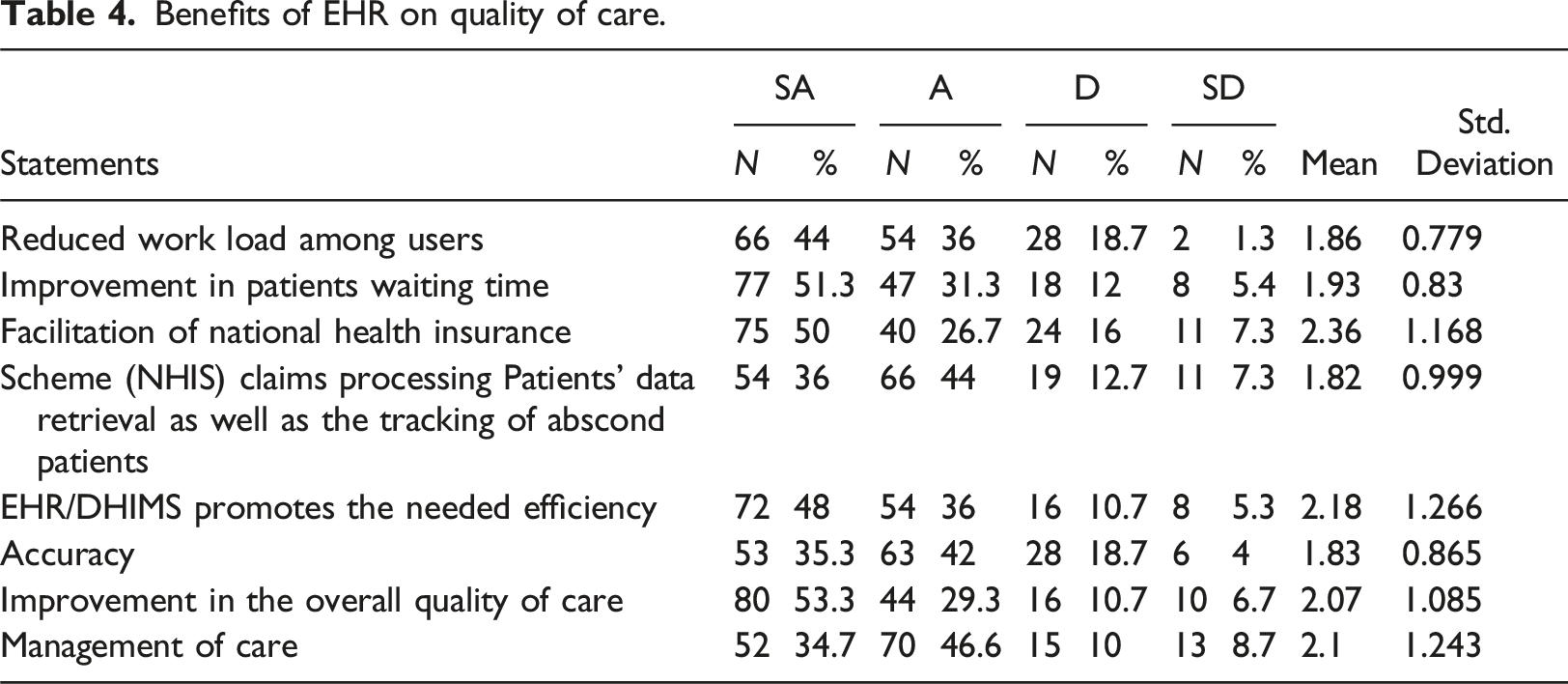
Benefits of EHR on quality of care
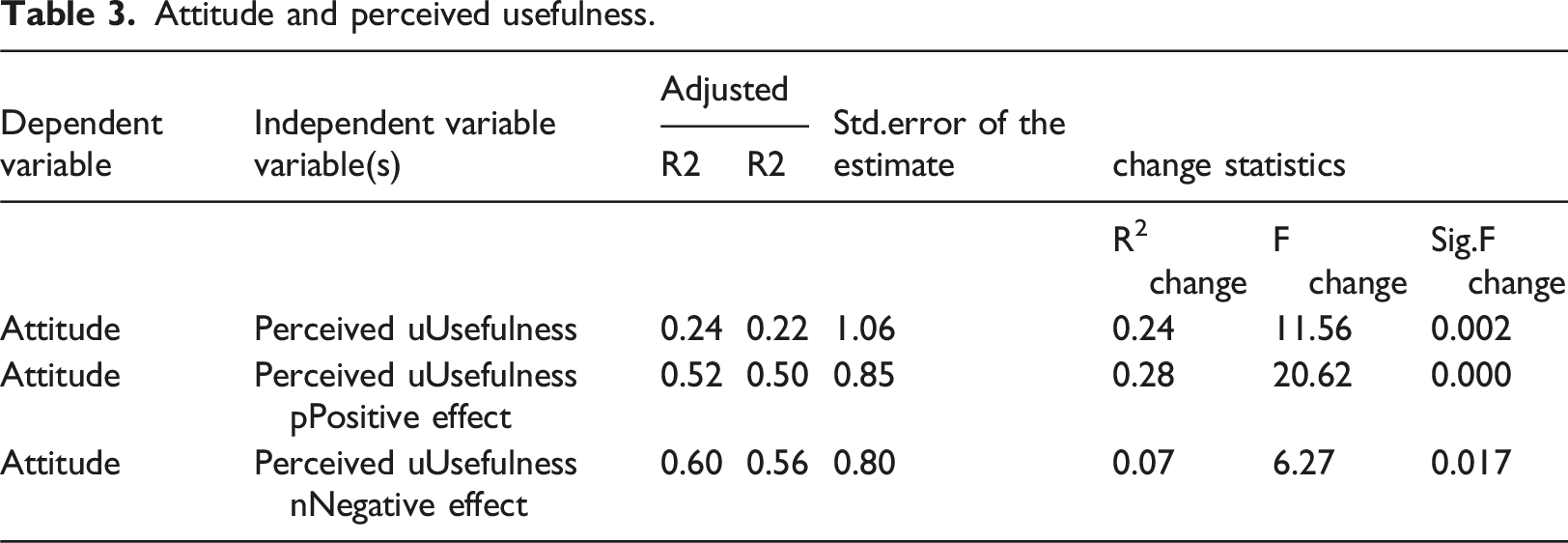
Attitude and perceived usefulness.
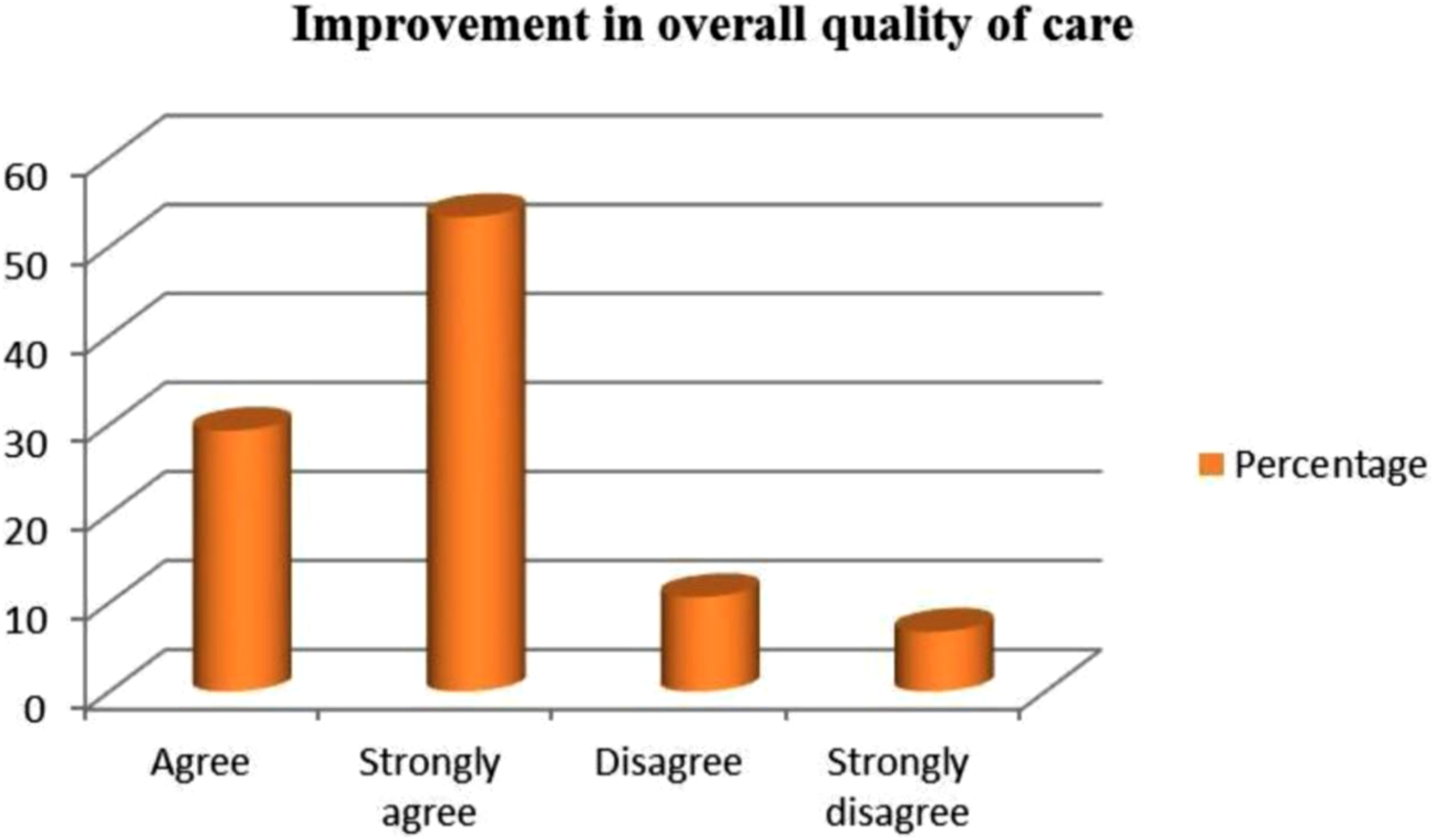
On the benefits of health information systems on quality service delivery, Table 3 shows that with a mean value greater or equal to 2.5, majority of the respondents strongly agreed to the following statement about EHR/DHIMS: (1.86) believed that there has been considerable reduction in the workload than using paper-based work, (2.36) Health Information System promote the facilitation of National Health Insurance Scheme (NHIS) claims processing and the provision of the needed efficiency, (2.18) and (2.07) improvement in the overall quality of care offered to patients. The study reports that 120 (80.0%) strongly agreed and agreed that EHR/DHIMS-2 reduces workload compared to paper-based work whereas 30 (20.0%) disagreed and strongly disagreed with the above assertion.
Benefits of EHR on quality of care.
The respondents asserted the implemented systems have improved their work and assigned some reasons to substantiate their claims; ‘’….. Information (medical histories) about patients is easily accessible to the clinicians and other healthcare professionals’’.
…. ‘’It has saved patients’ waiting time, reduced patients’ missing folders, improved data collection, facilitated dispensing of prescribed medications and monthly reports as well as reduced workload ’’
‘‘’…provides easy access of laboratory request from clinicians’’ (Respondent XXIX).
This shows that users’ perception about the overall functionality of the adopted system is quite encouraging but there is more room for improvement.
Notwithstanding the numerous benefits of the implemented system, some of the respondents bemoaned poor network concerns which makes working with the system difficult. One respondent mentioned,
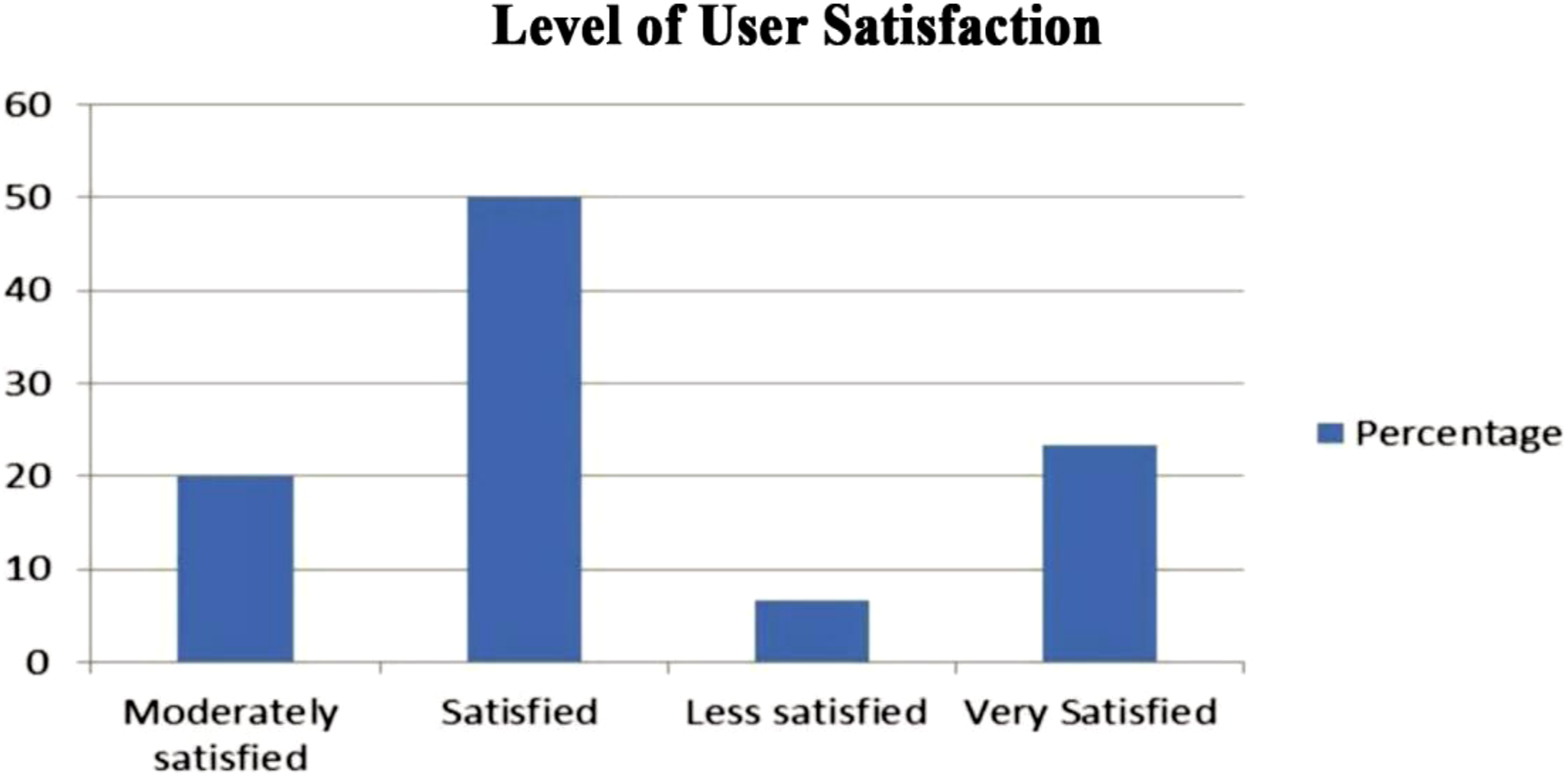
“The system is sometimes not working. There are often breaks in connections especially when there is rain or sometimes when the cables come into contact with water which makes it impossible for me to prepare patient bills” (Respondent XXVI) (Figures 2–4). Respondents Knowledge level of ICT. ICT improves the overall quality of care. Respondents level of User satisfaction with EHR/DHIMS-2.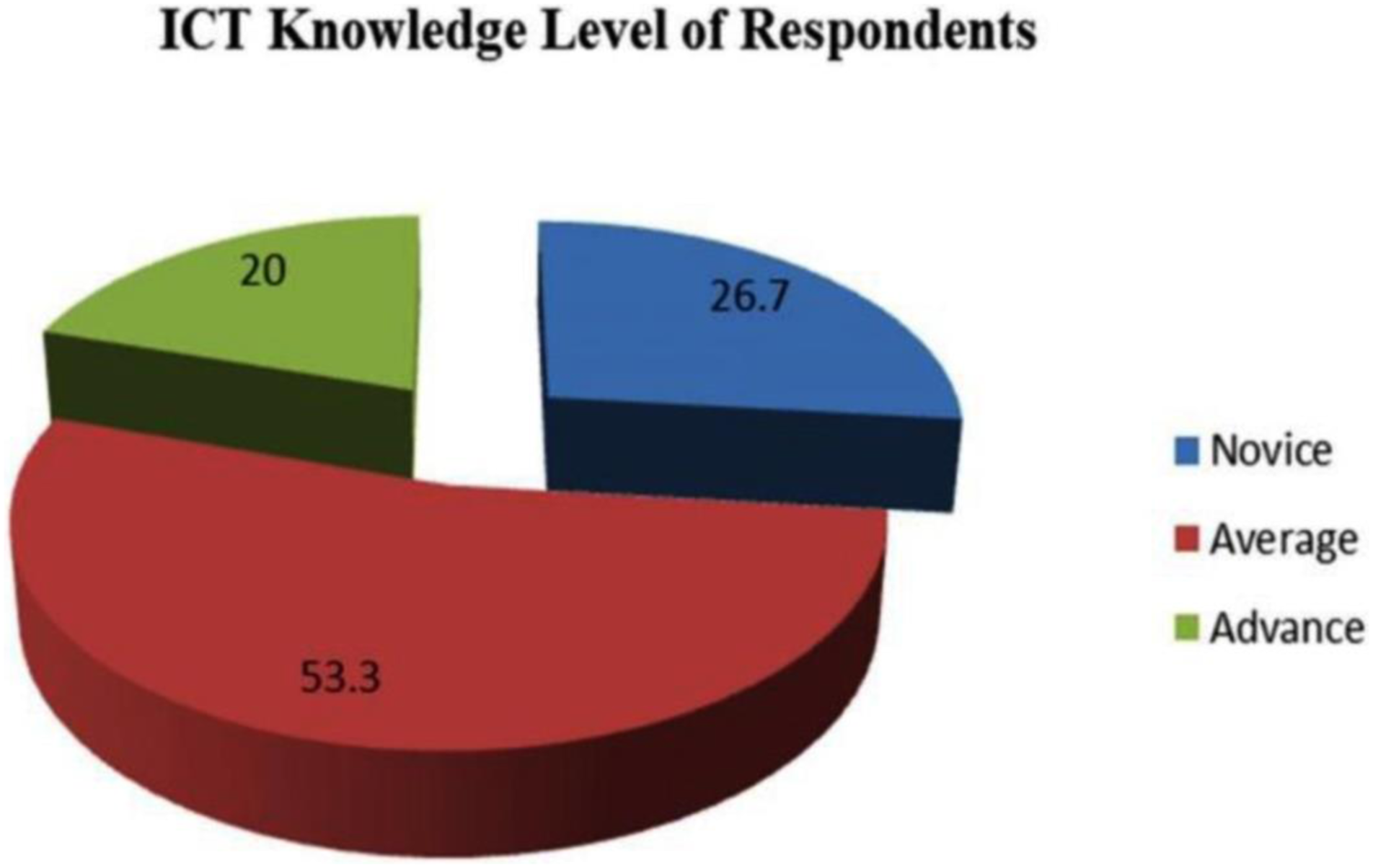
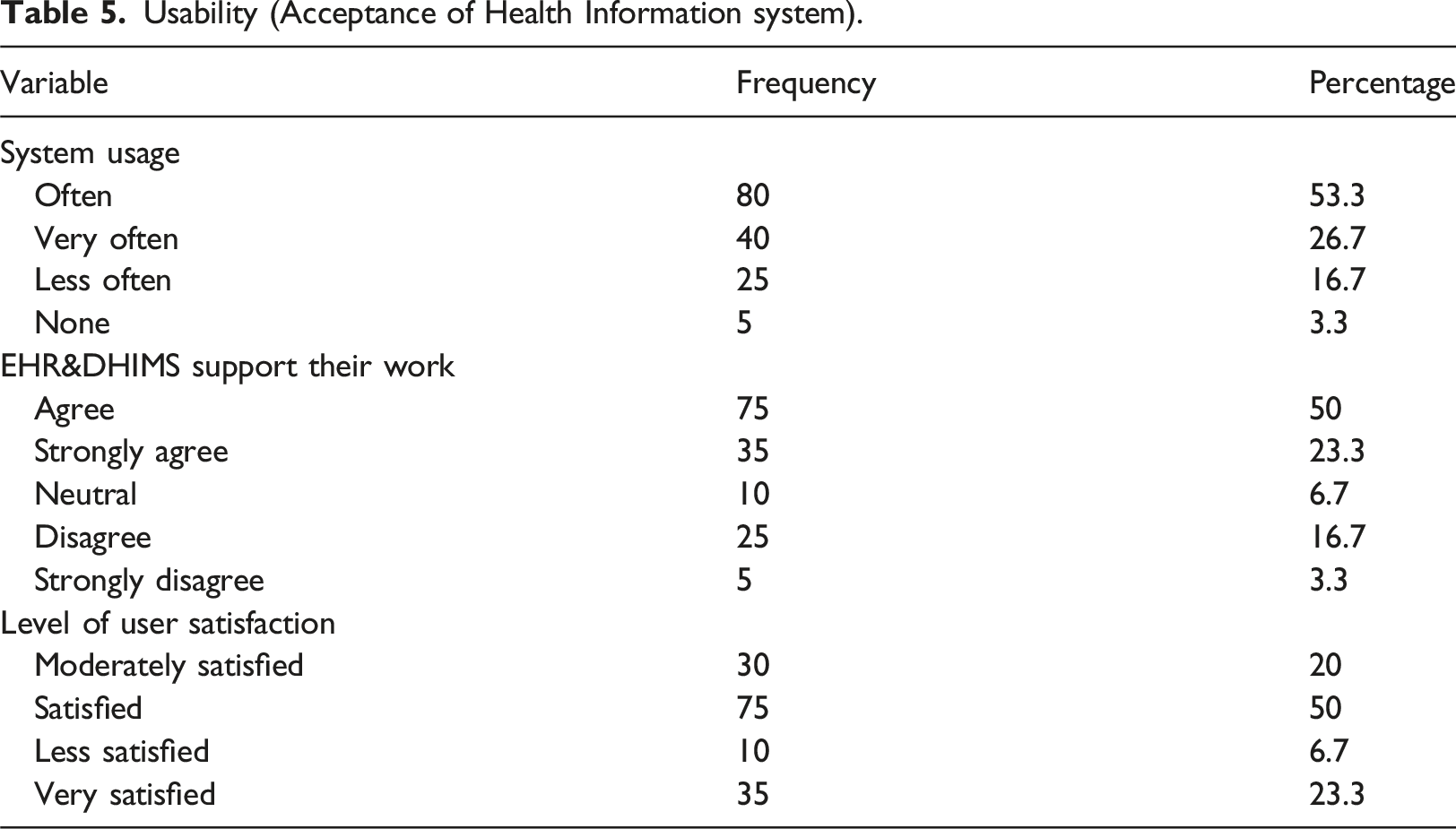
Usability (Acceptance of Health Information System)
The majority representing 75 (50.0%) out of the 150 respondents admitted that both EHR and DHIMS-2 support their work while 35 (23.3%) strongly agreed. However, 10 (6.7%) were neutral in their assessment of the system. Contrary to the overall impact of the adopted system, 25 (6.7%) disagreed whereas 5 (3.3) strongly disagreed.
Concerning the frequency of the system usage, the respondents had divergent views. Only 40 (26.7%) indicated that they used both systems (EHR and DHIMS-2) ‘very often’ twenty-five (16.7%) do ‘not use it often’. The remaining 80 (53.3%) specified that they ‘often’ use both the EHR and DHIMS-2 and 5 (3.3%) shirked from answering the question.
Usability (Acceptance of Health Information system).
Respondents view on perceived ease of use and usefulness
The first three hypotheses of this study examine whether TAM’s predictions apply to healthcare information systems. These hypotheses assert that intention to use is influenced by usefulness and attitude, usefulness is influenced by ease of use, and attitude is influenced by both ease of use and usefulness.
The results show a significant association between the combined effects of attitude and usefulness on acceptance. That is, 61% (R2 = 0.61) of variance in intention to use is explained by users’ attitude and belief that the system is useful. These results found that attitude and usefulness have a large effect size (f2 = 1.54) on intention to use. Effect size represents “the degree to which the phenomenon is present in the population” and is considered large if its value exceeds 0.33. 27 Thus, these results not only support H1a and H1b but also show that usefulness and attitude have a substantial effect on acceptance.
Contrary to TAM’s prediction, the result showed only a significant path between usefulness and attitude but not between ease of use and attitude. These results support H3b but not H3a. The extended model was tested by examining the impact of positive and negative effects on mindset.
Respondents’ view on Perceived Ease of Use and Usefulness.
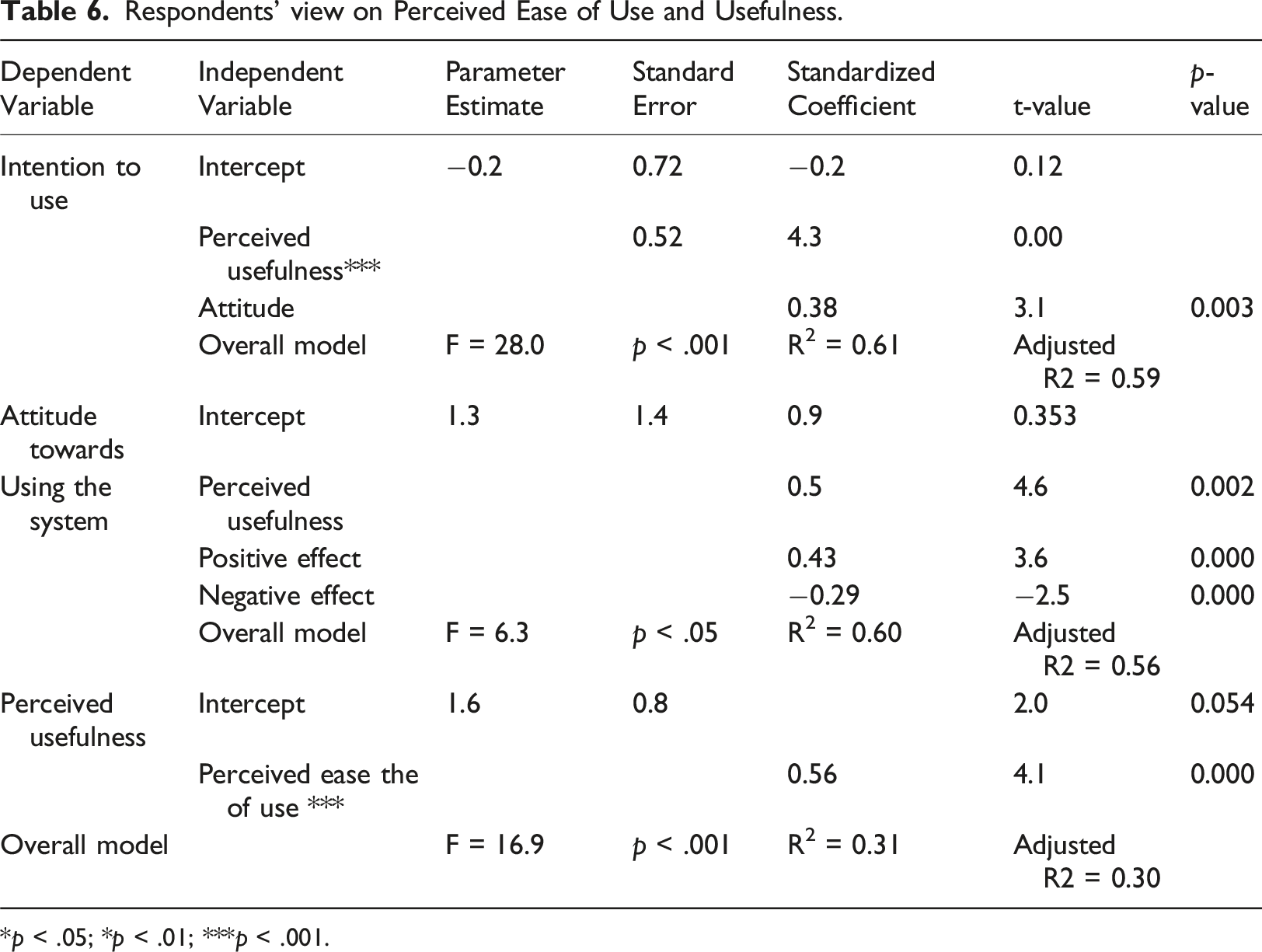
*p < .05; *p < .01; ***p < .001.
To ensure that there were no issues due to multicollinearity, tolerance and variance inflation factor (VIF) values for the data were calculated. The tolerance values were all within the 0.9 to 1.0 range which is well above the suggested lower limit of 0.10 and the VIF values were all close to 1.0, which was below the acceptable threshold of 10. 27
Confidence interval for coefficients PUSE, positive and negative affect.

Relationship between variables
Relationship between perceived usefulness, perceived ease of use and user acceptance.
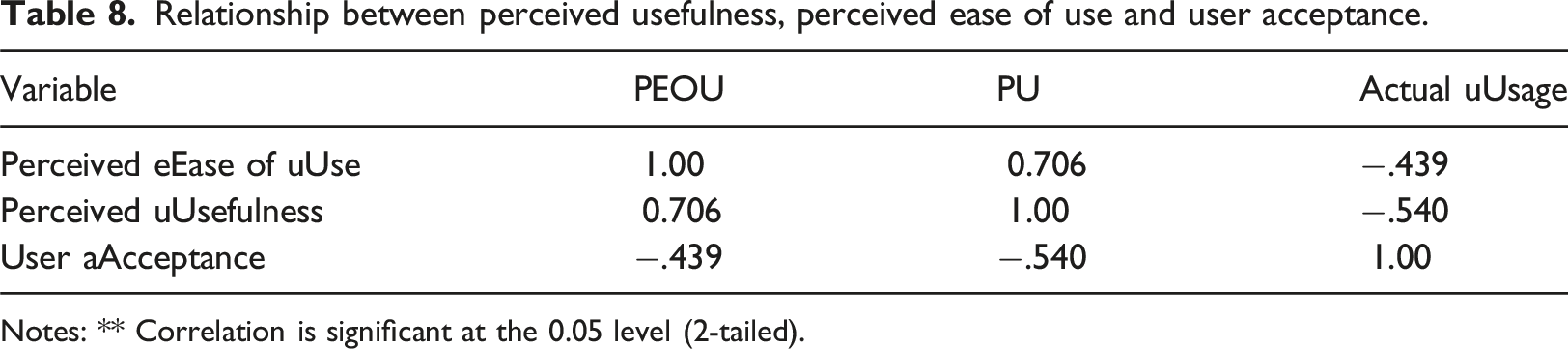
Notes: ** Correlation is significant at the 0.05 level (2-tailed).
The results were as follows: • strong positive correlation between PU and PEOU, r = 0.706, n = 106, p < 0.01, with high PU associated with high PEOU • strong negative correlation between PU and actual usage of HIS, r = −0.540, n = 106, p < 0.01, as PU decreases user acceptance of HIS increases • moderate negative correlation between actual HIS usage and PEOU, r = −0.439, n = 106, p < 0.01, as PEOU decreases user acceptance of HIS increases.
Multiple Linear Regression Standard multiple linear regression, α = 0.05 (two-tailed), was used to examine the relationship between PU, PEOU, and user acceptance of HIS. The independent variables were PU and PEOU. The dependent variable was user acceptance of HIS. The null hypothesis was there is no statistically significant relationship between (a) PU, (b) PEOU, and (c) user acceptance of HIS. The alternative hypothesis revealed a statistically significant relationship between (a) PU, (b) PEOU, and (c) user acceptance of HIS. Preliminary analyses were conducted to ascertain whether the assumptions of multicollinearity, outliers, normality, linearity, homoscedasticity, and independence of residuals were met but no serious violations were noted. The model as a whole could predict user acceptance significantly, F (2, 103) = 21.903, p < 0.000, R 2 = 0.298. The R2 (0.298) value indicated approximately 29.8% of variations in user acceptance is accounted for by the linear combination of the predictor variables (PU and PEOU). In the final model, PU and PEOU were statistically significant with PU (t = −3.947, p = 0.000, β = −0.460) accounting for a higher contribution to the model than PEOU (t = −0.977, p = 0.000, β = −0.114). The final predictive equation was: User Acceptance = 6.326 −0.460(PU) −0.114(PEOU). This shows that changes in the independent variable are associated with changes in the dependent variable hence, perceived usefulness, perceived ease of use, and user acceptance are statistically significant.
Discussion
The research attempted to make an inquest into users’ satisfaction with the newly implemented software. From the findings, 93.3% of the respondents overwhelmingly were either satisfied, or moderately satisfied and others claimed they were not satisfied. This gives credence to the fact that users were generally satisfied with the system. This assertion is in agreement with earlier studies by, 28 who indicated that the entries and retrieval of health-related data from the systems significantly encourage usability and users’ satisfaction. The identified myriad benefits associated with the system albeit some inherent challenges that affected the implementation process included, reduced workload among users, improvement in patients waiting time, facilitation of National Health Insurance Scheme (NHIS) claims processing, patients’ data retrieval as well as the tracking of abscond patients, promoting the needed efficiency and improvement in the overall quality of care. This is in Tandem with a study by Safran 15 who reported that the use of computerized information systems guarantees and offers numerous benefits to healthcare practitioners in the care industry.
Despite the myriad benefits associated with the implemented EHR/DHIMS-2 in the district, the inherent challenges that gainsay the operationalization of the system cannot be overlooked. The challenges from the respondents’ perception included; poor computer network concerns, unstable power supply, inadequate training, and increased work tasks. This assertion is in congruence with a study by Bra et al., 29 who opined that researchers have indicated that the daunting challenges associated with implemented EHR systems are peculiar to developing countries as a result of many contributing determinants. 29 The above findings are consistent with similar studies carried out by 30 in Ghana. The findings revealed that the IT infrastructure in most Ghanaian hospitals is woefully inadequate to contain the full functionality of electronic health records systems. The facility lacks proper Internet infrastructure and in most cases when there is availability of Internet connectivity, the network is most at times slow. This is also consistent with a study by De Heer-Menlah who disclosed that the charge for Internet access is also exorbitant as the situation in most Sub-Saharan African countries. The poorer countries without good telecommunication infrastructure are those that pay high prices for Internet access, for example $33.75 per month in Ghana. 31
As hypothesized, the results found that users’ attitude toward a healthcare information system has an important role in their acceptance behavior. This further supports the choice of TAM as the base model in our study.
Perceive usefulness and ease of use have significant positive influence on end-users acceptance and utilization of the system. Specifically, the results indicate that users’ positive affect and their perception of the usefulness of the system have almost the same influence on their attitudes toward the system, which in turn has a significant influence on their acceptance behavior. This is in support of the Technology Acceptance Model by 21 and 27 When the end-users feel the implemented system is easy to use, they assume it will be beneficial to their daily routines. 21 Therefore perceived ease of use and usefulness could be significantly predicted to influence end-users’ attitudes toward consumption.
Study limitations
Even though the respondents had used computers before, not all were very computer literate and comfortable with the new technology which may affect their perceptions of it. Less experienced users may find the technology difficult to use and less enjoyable, which may lead to negative attitudes.
Conclusion
Generally, the respondents indicated their satisfaction with the implemented system. The EHR was acceptable as could be seen from the frequency of system usage, support to their work, and the reduced errors and workload albeit inherent challenges among others. This study provided insights into the factors influencing user acceptance of HIS and revealed that users’ attitude toward a healthcare information system has an important role in their acceptance behavior. It is also recommended that the Health Ministry and Ghana Health Service should ensure comprehensive research on health information systems especially the EHR and DHIMS-2 to critically examine specific implementation policies and the effect on such systems within the confines of developing nations, particularly in Ghana.
Footnotes
Acknowledgements
‘’We acknowledge the support and guidance provided by the healthcare and academic communities that contributed to the successful completion of this study’’
Author Contributions
Corresponding Author: Kennedy Addo (
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.